
Hope-Based Program for Portuguese Outpatients with Advanced Chronic Illness in a Community Setting: A Randomized Control Trial


Abstract
:1. Introduction
2. Materials and Methods
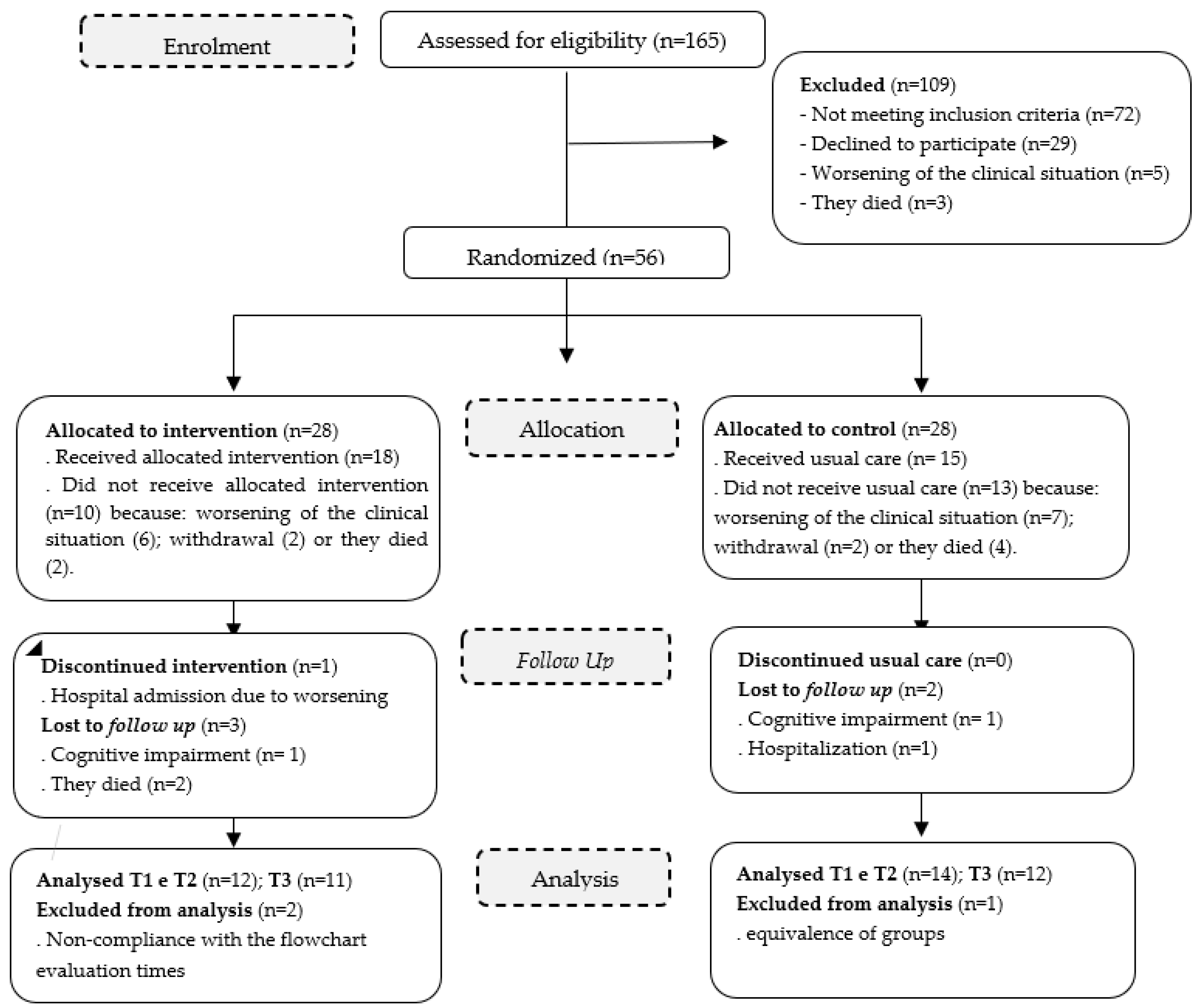
2.1. Study Design
2.2. Setting and Participants
2.2.1. Eligibility Criteria
2.2.2. Random Assignment
2.3. Intervention—Hope Promotion Program (HPP)
2.4. Sample Size
2.5. Outcome Variables and Measurements
2.6. Data Collection Procedure
2.7. Analysis
2.8. Ethical Issues
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Relationship between Hope, Comfort and QoL in the Sample
3.3. Effect of Intervention
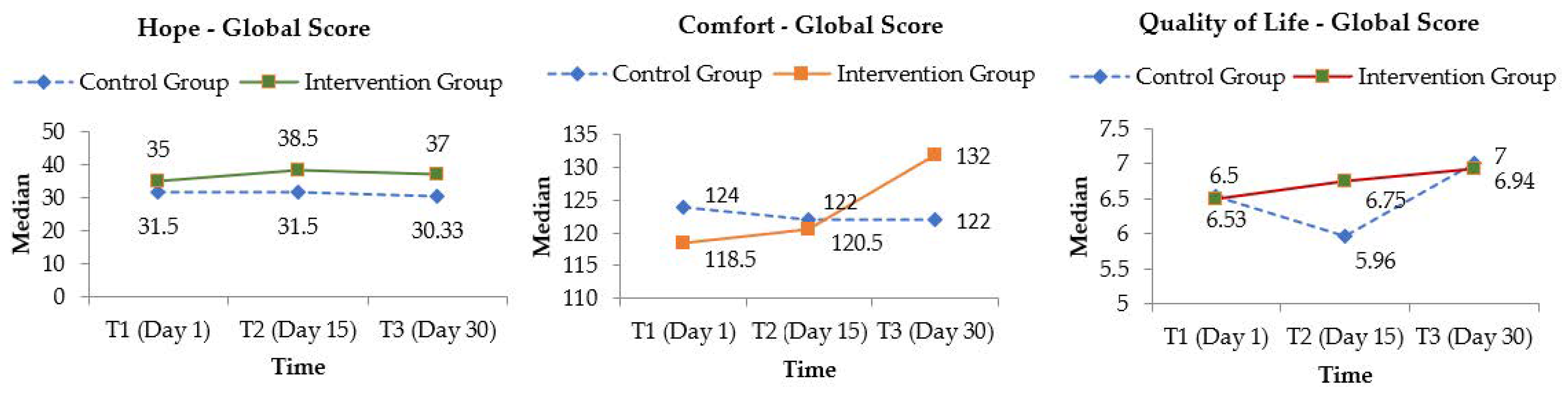
3.3.1. Primary Outcome
3.3.2. Secondary Outcomes
4. Discussion
4.1. Study Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, P.; de Graaf, S.; Hillen, M. The inherent tensions and ambiguities of hope: Towards a post-formal analysis of experiences of advanced-cancer patients. Health 2015, 19, 207–225. [Google Scholar] [CrossRef] [Green Version]
- Broadhurst, K.; Harrington, A. A mixed-method thematic review: The importance of hope to the dying patient. J. Adv. Nurs. 2016, 72, 18–32. [Google Scholar] [CrossRef]
- Duggleby, W.; Cooper, D.; Nekolaichuk, C.; Cottrell, L.; Swindle, J.; Barkway, K. The psychosocial experiences of older palliative patients while participating in a Living with Hope Program. Palliat. Support. Care 2016, 14, 672–679. [Google Scholar] [CrossRef]
- Laranjeira, C.; Dixe, M.A.; Semeão, I.; Rijo, S.; Faria, C.; Querido, A. “Keeping the Light On”: A Qualitative Study on Hope Perceptions at the End of Life in Portuguese Family Dyads. Int. J. Environ. Res. Public Health 2022, 19, 1561. [Google Scholar] [CrossRef] [PubMed]
- Wrigley, A. Hope, Dying and Solidarity. Ethic. Theory Moral Prac. 2019, 22, 187–204. [Google Scholar] [CrossRef] [Green Version]
- Kirby, E.; Broom, A.; MacArtney, J.; Lewis, S.; Good, P. Hopeful dying? The meanings and practice of hope in palliative care family meetings. Soc. Sci. Med. 2021, 291, 114471. [Google Scholar] [CrossRef] [PubMed]
- Eliott, J.; Olver, I. Hope, life, and death: A qualitative analysis of dying cancer patients’ talk about hope. Death Stud. 2009, 33, 609–638. [Google Scholar] [CrossRef]
- Olsman, E. Hope in Health Care: A Synthesis of Review Studies. In Historical and Multidisciplinary Perspectives on Hope, 1st ed.; van den Heuvel, S.C., Ed.; Springer: Cham, Switzerland, 2020; pp. 197–214. [Google Scholar]
- Duggleby, W.; Wright, K. The hope of professional caregivers caring for persons at the end of life. J. Hosp. Palliat. Nurs. 2007, 9, 42–49. [Google Scholar] [CrossRef]
- Rustøen, T. Hope: A Health Promotion Resource. In Health Promotion in Health Care—Vital Theories and Research, 1st ed.; Haugan, G., Eriksson, M., Eds.; Springer: Cham, Switzerland, 2021; pp. 61–70. [Google Scholar]
- Cotter, N.; Foxwell, A. The Meaning of Hope in the Dying. In Textbook of Palliative Nursing, 5th ed.; Ferrel, B.N., Coyle, J.P., Eds.; University Press: Oxford, UK, 2015; pp. 513–529. [Google Scholar]
- Laranjeira, C.A.; Querido, A.; Charepe, Z.B.; Dixe, M. Hope-based interventions in chronic disease: An integrative review in the light of Nightingale. Rev. Bras. Enferm. 2020, 73 (Suppl. 5), e20200283. [Google Scholar] [CrossRef]
- Badr, H. Psychosocial Interventions for Patients With Advanced Cancer and Their Families. Am. J. Lifestyle Med. 2014, 10, 53–63. [Google Scholar] [CrossRef]
- Chan, K.; Wong, F.K.; Lee, P.H. A Brief Hope Intervention to Increase Hope Level and Improve Well-Being in Rehabilitating Cancer Patients: A Feasibility Test. SAGE Open Nurs. 2019, 5, 2377960819844381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Blanckenburg, P.; Leppin, N. Psychological interventions in palliative care. Curr. Opin. Psychiatry 2018, 31, 389–395. [Google Scholar] [CrossRef]
- Hall, S.; Goddard, C.; Opio, D.; Speck, P.W.; Martin, P.; Higginson, I.J. A novel approach to enhancing hope in patients with advanced cancer: A randomised phase II trial of dignity therapy. BMJ Support. Palliat. Care 2011, 1, 315–321. [Google Scholar] [CrossRef]
- Salamanca-Balen, N.; Merluzzi, T.V.; Chen, M. The effectiveness of hope-fostering interventions in palliative care: A systematic review and meta-analysis. Palliat. Med. 2021, 35, 710–728. [Google Scholar] [CrossRef]
- López, J.; Serrano, M.I.; Giménez, I.; Noriega, C. Forgiveness Interventions for Older Adults: A Review. J. Clin. Med. 2021, 10, 1866. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, J.; Hu, X. The effectiveness of dignity therapy on hope, quality of life, anxiety, and depression in cancer patients: A meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2022, 132, 104273. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Morita, T.; Akechi, T.; Okamoto, T. Japanese Task Force for Spiritual Care. Efficacy of short-term life-review interviews on the spiritual well-being of terminally ill cancer patients. J. Pain Symptom Manag. 2010, 39, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Guy, M.P.; Higginson, I.J.; Amesbury, B.D. The effect of palliative daycare on hope: A comparison of daycare patients with two control groups. J. Palliat. Care 2011, 27, 216–223. [Google Scholar] [CrossRef]
- Duggleby, W. Living with Hope Program. In Hospice Palliative Home Care and Bereavement Support; Holtslander, L., Peacock, S., Bally, J., Eds.; Springer: Cham, Switzerland, 2019; pp. 161–167. [Google Scholar] [CrossRef]
- Li, P.; Guo, Y.J.; Tang, Q.; Yang, L. Effectiveness of nursing intervention for increasing hope in patients with cancer: A meta-analysis. Rev. Lat. Am. De Enferm. 2018, 26, e2937. [Google Scholar] [CrossRef]
- Doe, M.J. Conceptual Foreknowings: An Integrative Review of Hope. Nurs. Sci. Q. 2020, 33, 55–64. [Google Scholar] [CrossRef]
- National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for Quality Palliative Care, 4th ed.; National Consensus Project for Quality Palliative Care: Pittsburgh, PA, USA, 2018; Available online: https://www.nationalcoalitionhpc.org/wp-content/uploads/2018/10/NCHPC-NCPGuidelines_4thED_web_FINAL.pdf (accessed on 10 September 2022).
- Wensley, C.; Botti, M.; McKillop, A.; Merry, A.F. Maximising comfort: How do patients describe the care that matters? A two-stage qualitative descriptive study to develop a quality improvement framework for comfort-related care in inpatient settings. BMJ Open 2020, 10, e033336. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G.; Consolidated Standards of Reporting Trials Group. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santana, I.; Duro, D.; Lemos, R.; Costa, V.; Pereira, M.; Simões, M.R.; Freitas, S. Mini-Mental State Examination: Avaliação dos Novos Dados Normativos no Rastreio e Diagnóstico do Défice Cognitivo [Mini-Mental State Examination: Screening and Diagnosis of Cognitive Decline, Using New Normative Data]. Acta Med. Port. 2016, 29, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fradique, E. Efetividade da Intervenção Multidisciplinar em Cuidados Paliativos. Effectiveness of Multidisciplinary Intervention in Palliative Care. Master’s Thesis, University of Lisbon, Lisbon, Portugal, 2010. [Google Scholar]
- Kim, D.; Kim, H.; Thorne, S. An Intervention Model to Help Clients to Seek Their Own Hope Experiences: The Narrative Communication Model of Hope Seeking Intervention. Korean J. Hosp. Palliat. Care 2017, 20, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Farran, C.J.; Herth, K.A.; Popovich, J.M. Hope and Hopelessness: Critical Clinical Constructs; Sage Publications: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Duggleby, W.D.; Williams, A.M. Living with hope: Developing a psychosocial supportive program for rural women caregivers of persons with advanced cancer. BMC Palliat. Care 2010, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Dahodwala, M.; Geransar, R.; Babion, J.; de Grood, J.; Sargious, P. The impact of the use of video-based educational interventions on patient outcomes in hospital settings: A scoping review. Patient Educ. Couns. 2018, 101, 2116–2124. [Google Scholar] [CrossRef]
- Querido, A.; Laranjeira, C.; Dixe, M.; Figueiredo, M.; Marques, R.; Charepe, Z. A promoção da esperança nas transições de saúde-doença: Contributos para a Ação [Promoting hope in health-illness transitions: Contributions to Action]. In O Cuidado Centrado no Cliente: Da Apreciação à Intervenção de Enfermagem; Eunice, H., Ed.; Lusodidata/Sabooks Editora: Lisboa, Portugal, 2021; pp. 187–202. [Google Scholar]
- Klainin-Yobas, P.; Oo, W.N.; Suzanne Yew, P.Y.; Lau, Y. Effects of relaxation interventions on depression and anxiety among older adults: A systematic review. Aging Ment. Health 2015, 19, 1043–1055. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef]
- Viana, A.; Querido, A.; Dixe, M.A.; Barbosa, A. Avaliação da esperança em cuidados Paliativos [Evaluation of hope in palliative care]. Int. J. Educ. Psychol. 2010, 2, 607–616. [Google Scholar]
- Querido, A. A Promoção da Esperança em Fim de Vida—Avaliação da Efetividade de um Programa de Intervenção em Pessoas com Doença Crónica Avançada e Progressiva. The Promotion of Hope at the End of Life—Evaluation of the Effectiveness of an Intervention Program for People with Advanced and Progressive Chronic Illness. Doctoral Thesis, UCP, Lisboa, Portugal, 2013; p. 312. [Google Scholar]
- Kolcaba, K.Y. Comfort Theory and Practice; Springer: New York, NY, USA, 2003. [Google Scholar]
- Duarte, A.C.; Querido, A.I.; Dixe, M.A. Validação transcultural da “McGill Quality of Life Questionnaire”—Qualidade de vida em doentes em cuidados intensivos [Cross-cultural validation of the “McGill Quality of Life Questionnaire”—Quality of life in intensive care patients]. Int. J. Educ. Psychol. 2010, 4, 437–448. [Google Scholar]
- Cohen, S.R.; Mount, B.M.; Bruera, E.; Provost, M.; Rowe, J.; Tong, K. Validity of the McGill Quality of Life Questionnaire in the palliative care setting: A multi-centre Canadian study demonstrating the importance of the existential domain. Palliat. Med. 1997, 11, 3–20. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herth, K. Development and Implementation of a Hope Intervention Program. Oncol. Nurs. Forum. 2001, 28, 1009–1017. [Google Scholar] [PubMed]
- Duggleby, W.D.; Degner, L.; Williams, A.; Wright, K.; Cooper, D.; Popkin, D.; Holtslander, L. Living with Hope: Initial Evaluation of a Psychosocial Hope Intervention for Older Palliative Home Care Patients. J. Pain Symptom Manag. 2007, 33, 247–257. [Google Scholar] [CrossRef]
- Ostherr, K.; Killoran, P.; Shegog, R.; Bruera, E. Death in the Digital Age: A Systematic Review of Information and Communication Technologies in End-of-Life Care. J. Palliat. Med. 2016, 19, 408–420. [Google Scholar] [CrossRef] [Green Version]
- Warnock-Parkes, E.; Wild, J.; Stott, R.; Grey, N.; Ehlers, A.; Clark, D.M. Seeing Is Believing: Using Video Feedback in Cognitive Therapy for Social Anxiety Disorder. Cogn. Behav. Pract. 2017, 24, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.; Verplanken, B.; Skevington, S.M. Cross cultural application of the WHOQOL-SRPB in the Chinese community with diverse spiritual affiliations. Soc. Indic. Res. 2017, 132, 291–312. [Google Scholar] [CrossRef]
- Laranjeira, C.; Querido, A. Hope and Optimism as an Opportunity to Improve the “Positive Mental Health” Demand. Front. Psychol. 2022, 13, 827320. [Google Scholar] [CrossRef]
- Sawatzky, R.; Porterfield, P.; Lee, J.; Dixon, D.; Lounsbury, K.; Pesut, B.; Roberts, D.; Tayler, C.; Voth, J.; Stajduhar, K. Conceptual foundations of a palliative approach: A knowledge synthesis. BMC Palliat. Care 2016, 15, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, A.; Parola, V.; Sandgren, A.; Fernandes, O.; Kolcaba, K.; Apóstolo, J. The Effects of Guided Imagery on Comfort in Palliative Care. J. Hosp. Palliat. Nurs. 2018, 20, 392–399. [Google Scholar] [CrossRef]
- Butcher, H.; Bulechek, G.; Dochterman, J.; Wagner, C. Nursing Interventions Classification (NIC), 7th ed.; Mosby: New York, NY, USA, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Evaluation Time Points | T1 (Baseline) | RANDOMIZATION | Intervention | T2 (15 Days after) | T3 (after 1 Month) |
| Protocol measure and assessment instruments | (1) demographics (gender, age, marital status and social status); (2) clinical characteristics (medical diagnosis, functional status, presence of medical symptoms like pain, fatigue or depression); (3) Herth Hope Index [HHI]; (4) McGill Quality of Life Questionnaire [MQoL]; (5) Hospice Comfort Questionnaire [HCQ]. | IG *—Hope Promotion Program (HPP) CG **—Standard palliative care | HHI, MQoL and HCQ | HHI, MQoL and HCQ |
| Variables | Intervention Group (n = 12) | Control Group (n = 15) | ||
|---|---|---|---|---|
| Age (years) Mean ± (SD) | 60.17 (10.83) | 60.00 (11.98) | ||
| n | % | n | % | |
| Sex (female) | 8 | 29.63 | 7 | 25.93 |
| Married | 10 | 37.04 | 12 | 44.44 |
| Education (Primary education) | 7 | 25.93 | 11 | 40.74 |
| Lives with relatives | 11 | 18.52 | 13 | 26.53 |
| Functional status (Karnofsky Performance Scale) | ||||
| From 60 to 70 | 0 | 0 | 3 | 11.54 |
| From 80 to 100 | 12 | 46.15 | 11 | 42.31 |
| Pain | ||||
| Yes | 2 | 7.41 | 7 | 25.93 |
| No | 10 | 37.04 | 8 | 29.63 |
| Fatigue | ||||
| Yes | 11 | 40.74 | 11 | 40.74 |
| No | 1 | 3.70 | 4 | 14.81 |
| Depression | ||||
| Yes | 5 | 18.52 | 6 | 22.22 |
| No | 7 | 25.93 | 9 | 33.33 |
| Intervention Group n = 12 | Control Group n = 14 | U Mann-Whitney (One Tailed p) | ||||
|---|---|---|---|---|---|---|
| M | SD | M | SD | U | (p) | |
| HHI | 34.166 | 3.243 | 31.571 | 3.715 | 49.50 | 0.074 |
| Hope—Fator 1 | 3.527 | 0.399 | 3.226 | 0.456 | 50.50 | 0.082 |
| Hope—Fator 2 | 3.250 | 0.399 | 3.053 | 0.356 | 59.00 | 0.186 |
| MQoL | 6.817 | 1.366 | 6.527 | 1.583 | 79.00 | 0.797 |
| Physical QoL (Quality of Life) | 5.667 | 2.568 | 5.287 | 2.536 | 78.00 | 0.757 |
| Psychological symptoms | 5.459 | 2.215 | 5.571 | 2.588 | 79.00 | 0.797 |
| Existential QoL | 8.056 | 1.413 | 7.595 | 1.956 | 71.50 | 0.520 |
| Support | 8.125 | 1.932 | 7.714 | 1.729 | 69.00 | 0.436 |
| HCQ | 118.500 | 16.473 | 123.500 | 15.022 | 68.00 | 0.410 |
| Relief | 3.541 | 0.719 | 3.750 | 0.667 | 68.50 | 0.425 |
| Ease | 5.120 | 0.794 | 5.261 | 0.980 | 71.50 | 0.518 |
| Transcendence | 5.286 | 0.857 | 5.520 | 0.414 | 75.00 | 0.641 |
| Evolution of Hope | IG * n = 12 | CG† n = 14 | |||
| Z | p (one tailed p) | Z | p (one tailed p) | ||
| Total hope score | |||||
| T1/T2 | −1.536 | 0.042 | −0.539 | 0.295 | |
| T2/T3 | −0.089 | 0.464 | −0.299 | 0.382 | |
| T1/T3 | −1.841 | 0.033 | −0.819 | 0.206 | |
| Factor 1—Temporality, trust and interconnection | |||||
| T1/T2 | −0.669 | 0.251 | −0.402 | 0.344 | |
| T2/T3 | −0.777 | 0.218 | −0.843 | 0.199 | |
| T1/T3 | −1.730 | 0.042 | −0.827 | 0.204 | |
| Factor 2—Positive interior disposition and expectations | |||||
| T1/T2 | −2.146 | 0.016 | −0.707 | 0.240 | |
| T2/T3 | −1.026 | 0.152 | −0.287 | 0.387 | |
| T1/T3 | −1.327 | 0.092 | −0.499 | 0.309 | |
| Evolution of comfort | IG * n = 12 | CG † n = 14 | |||
| Z | p (one tailed p) | Z | p (one tailed p) | ||
| Total comfort score | T1/T2 | −0.445 | 0.328 | −1.203 | 0.114 |
| T2/T3 | −2.668 | 0.004 | −0.358 | 0.360 | |
| T1/T3 | −2.091 | 0.018 | −1.203 | 0.114 | |
| Relief | T1/T2 | −1.296 | 0.097 | −1.506 | 0.060 |
| T2/T3 | −2.538 | 0.005 | −0.059 | 0.476 | |
| T1/T3 | −2.268 | 0.011 | −0.748 | 0.227 | |
| Ease | T1/T2 | 0.000 | 0.500 | −1.692 | 0.045 |
| T2/T3 | −1.589 | 0.056 | −0.351 | 0.363 | |
| T1/T3 | −0.920 | 0.178 | −2.463 | 0.007 | |
| Transcendence | T1/T2 | −0.461 | 0.322 | −2.228 | 0.013 |
| T2/T3 | −1.972 | 0.024 | −0.632 | 0.263 | |
| T1/T3 | −1.643 | 0.050 | −2.834 | 0.002 | |
| Physical context | T1/T2 | −0.713 | 0.238 | −0.223 | 0.412 |
| T2/T3 | −1.793 | 0.036 | −0.238 | 0.406 | |
| T1/T3 | −1.382 | 0.083 | −0.870 | 0.192 | |
| Psychospiritual context | T1/T2 | −1.694 | 0.045 | −0.908 | 0.162 |
| T2/T3 | −2.233 | 0.013 | −0.920 | 0.178 | |
| T1/T3 | −2.807 | 0.025 | −0.051 | 0.479 | |
| Environmental context | T1/T2 | −0.530 | 0.298 | −1.823 | 0.034 |
| T2/T3 | −2.388 | 0.085 | −1.279 | 0.100 | |
| T1/T3 | −1.625 | 0.052 | −0.687 | 0.246 | |
| Sociocultural context | T1/T2 | −1.126 | 0.130 | −1.260 | 0.104 |
| T2/T3 | −0.566 | 0.285 | −0.140 | 0.444 | |
| T1/T3 | −0.313 | 0.377 | −0.938 | 0.174 | |
| Evolution of QoL (Quality of Life) | IG * n = 12 | CG † n = 14 | |||
| Z | p (one tailed p) | Z | p (one tailed p) | ||
| Total QoL score | T1/T2 | −0.353 | 0.362 | −1.570 | 0.058 |
| T2/T3 | −0.490 | 0.312 | −1.531 | 0.063 | |
| T1/T3 | −0.000 | 0.500 | −0.903 | 0.183 | |
| Physical QoL | T1/T2 | −1.493 | 0.067 | −2.169 | 0.015 |
| T2/T3 | −2.201 | 0.014 | −2.826 | 0.002 | |
| T1/T3 | −1.112 | 0.133 | −0.890 | 0.377 | |
| Psychological Symptoms | T1/T2 | −1.380 | 0.084 | −0.311 | 0.377 |
| T2/T3 | −1.068 | 0.142 | −1.290 | 0.098 | |
| T1/T3 | −0.223 | 0.412 | −0.471 | 0.319 | |
| Existential well-being | T1/T2 | −0.178 | 0.429 | −0.102 | 0.459 |
| T2/T3 | −0.624 | 0.266 | −2.613 | 0.004 | |
| T1/T3 | −1.122 | 0.131 | −2.229 | 0.013 | |
| Support | T1/T2 | −0.422 | 0.336 | −0.823 | 0.205 |
| T2/T3 | −0.703 | 0.241 | −1.513 | 0.065 | |
| T1/T3 | −0.060 | 0.475 | −0.060 | 0.475 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Querido, A.; Laranjeira, C. Hope-Based Program for Portuguese Outpatients with Advanced Chronic Illness in a Community Setting: A Randomized Control Trial. Int. J. Environ. Res. Public Health 2023, 20, 1566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021566
Querido A, Laranjeira C. Hope-Based Program for Portuguese Outpatients with Advanced Chronic Illness in a Community Setting: A Randomized Control Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):1566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021566
Chicago/Turabian StyleQuerido, Ana, and Carlos Laranjeira. 2023. "Hope-Based Program for Portuguese Outpatients with Advanced Chronic Illness in a Community Setting: A Randomized Control Trial" International Journal of Environmental Research and Public Health 20, no. 2: 1566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021566