
Therapeutic Effects of Metaverse Rehabilitation for Cerebral Palsy: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Assumptions
2.3. Experimental Procedure
2.3.1. GMFM 66
2.3.2. Cardiopulmonary Function
2.3.3. FIM
2.3.4. Pediatric QOL
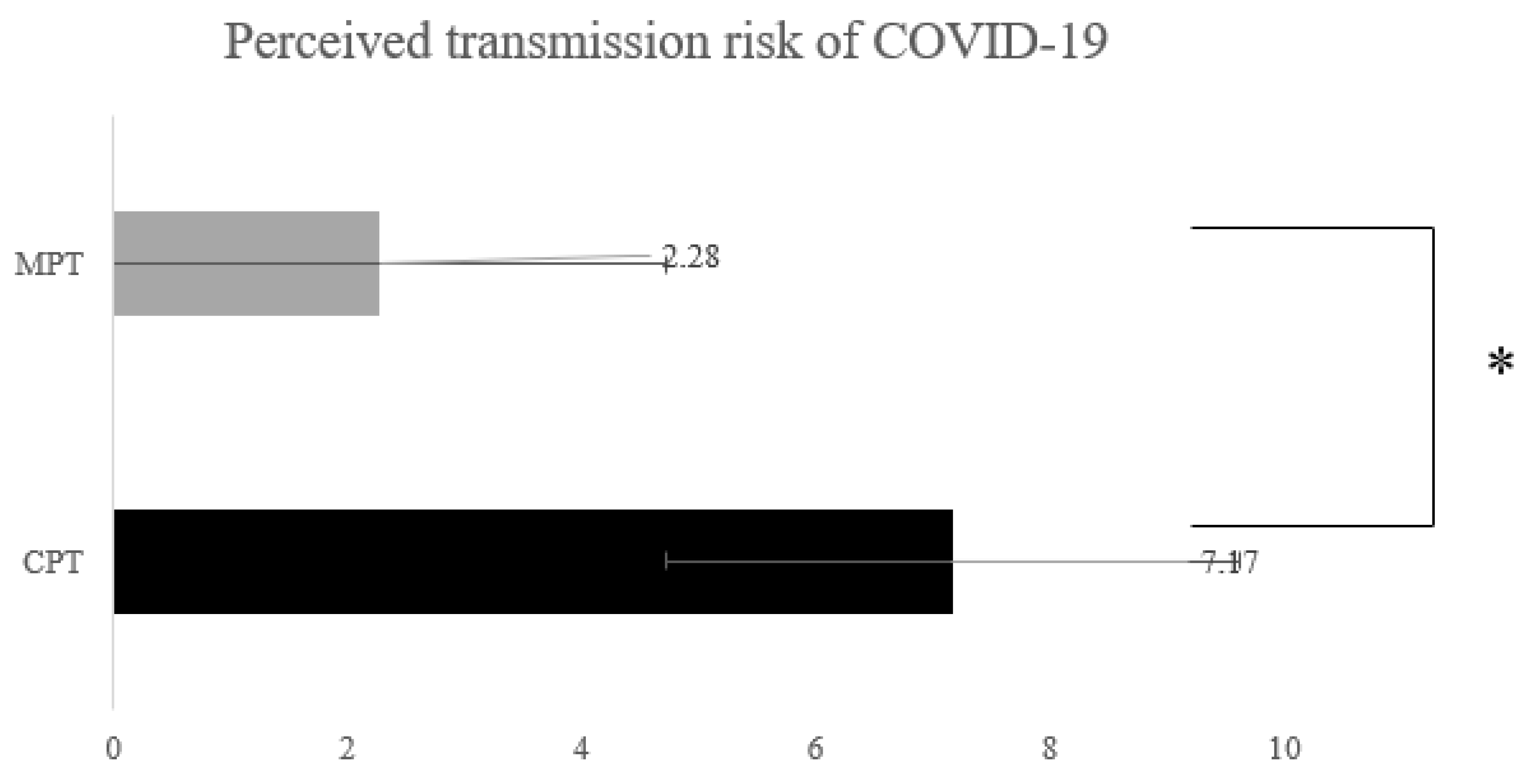
2.3.5. Perceived Risk of COVID-19 Transmission
2.4. Intervention
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients (N = 26)
3.2. Clinical Outcome Measurements
3.2.1. GMFM
3.2.2. Cardiopulmonary Function
3.2.3. FIM and QOL
3.3. Perceived Risk of COVID-19 Transmission
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blair, E.; Cans, C. The definition of cerebral palsy. In Cerebral Palsy; Springer: Cham, Switzerland, 2018; pp. 13–17. [Google Scholar]
- Eggink, H.; Kremer, D.; Brouwer, O.F.; Contarino, M.F.; van Egmond, M.E.; Elema, A.; Folmer, K.; van Hoorn, J.F.; van de Pol, L.A.; Roelfsema, V. Spasticity, dyskinesia and ataxia in cerebral palsy: Are we sure we can differentiate them? Eur. J. Paediatr. Neurol. 2017, 21, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Armand, S.; Decoulon, G.; Bonnefoy-Mazure, A. Gait analysis in children with cerebral palsy. EFORT Open Rev. 2016, 1, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.; Sakzewski, L.; Whittingham, K.; Wotherspoon, J.; Chatfield, M.D.; Ware, R.S.; Boyd, R.N. Development of social functioning in children with cerebral palsy: A longitudinal study. Dev. Med. Child Neurol. 2022, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- James, S.; Ziviani, J.; Boyd, R. A systematic review of activities of daily living measures for children and adolescents with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 233–244. [Google Scholar] [CrossRef]
- Sugimoto, D.; Rabatin, A.E.; Shea, J.E.; Parmeter, B.; Shore, B.J.; Stracciolini, A. Attitudes and Behaviors of Physical Activity in Children with Cerebral Palsy: Findings from PLAY Questionnaire. Children 2022, 9, 968. [Google Scholar] [CrossRef]
- Nelson, K.B.; Grether, J.K. Causes of cerebral palsy. Curr. Opin. Pediatr. 1999, 11, 487–491. [Google Scholar] [CrossRef]
- Zanon, M.A.; Pacheco, R.L.; Latorraca, C.d.O.C.; Martimbianco, A.L.C.; Pachito, D.V.; Riera, R. Neurodevelopmental treatment (Bobath) for children with cerebral palsy: A systematic review. J. Child Neurol. 2019, 34, 679–686. [Google Scholar] [CrossRef]
- Song, J.-W.; Zhang, C.; Fan, X.; Meng, F.-P.; Xu, Z.; Xia, P.; Cao, W.-J.; Yang, T.; Dai, X.-P.; Wang, S.-Y. Immunological and inflammatory profiles in mild and severe cases of COVID-19. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Dantas, L.O.; Barreto, R.P.G.; Ferreira, C.H.J. Digital physical therapy in the COVID-19 pandemic. Braz. J. Phys. Ther. 2020, 24, 381. [Google Scholar] [CrossRef]
- Crebbin, K.; Grisbrook, T.; Elliott, C.; Thornton, A. The Use of Serious Gaming to Improve Sensorimotor Function and Motivation in People with Cerebral Palsy: A Systematic Review. Games Health J. 2022, 11. Epub ahead of print. [Google Scholar] [CrossRef]
- Chung, E.J.; Lee, B.-H. The effects of flipped learning on learning motivation and attitudes in a class of college physical therapy students. J. Probl. Based Learn. 2018, 5, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Nadarzynski, T.; Miles, O.; Cowie, A.; Ridge, D. Acceptability of artificial intelligence (AI)-led chatbot services in healthcare: A mixed-methods study. Digit. Health 2019, 5, 2055207619871808. [Google Scholar] [CrossRef] [PubMed]
- Te Velde, A.; Morgan, C. Gross Motor Function Measure (GMFM-66 & GMFM-88) User’s Manual, Book Review. Pediatr. Phys. Ther. 2022, 34, 88–89. [Google Scholar]
- Wei, S.; Su-Juan, W.; Yuan-Gui, L.; Hong, Y.; Xiu-Juan, X.; Xiao-Mei, S. Reliability and validity of the GMFM-66 in 0-to 3-year-old children with cerebral palsy. Am. J. Phys. Med. Rehabil. 2006, 85, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Ritchie, C. Rating of perceived exertion (RPE). J. Physiother. 2012, 58, 62. [Google Scholar] [CrossRef] [Green Version]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Kidd, D.; Stewart, G.; Baldry, J.; Johnson, J.; Rossiter, D.; Petruckevitch, A.; Thompson, A. The Functional Independence Measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 10–14. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL™: Measurement model for the pediatric quality of life inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL™* 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul. Pediatr. 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Desai, A.D.; Zhou, C.; Stanford, S.; Haaland, W.; Varni, J.W.; Mangione-Smith, R.M. Validity and responsiveness of the pediatric quality of life inventory (PedsQL) 4.0 generic core scales in the pediatric inpatient setting. JAMA Pediatr. 2014, 168, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.H.; Park, C.; You, J.H. Minimal Contact Robotic Stroke Rehabilitation on Risk of COVID-19, Work Efficiency and Sensorimotor Function. Healthcare 2022, 10, 691. [Google Scholar] [CrossRef] [PubMed]
- Cabezas-López, M.; Bernabéu-Brotóns, E. The effects of Bobath therapy on children with cerebral palsy: A systematic review. Int. J. Ther. Rehabil. 2022, 29, 1–11. [Google Scholar] [CrossRef]
- Mbada, C.E.; Olaoye, M.I.; Dada, O.O.; Ayanniyi, O.; Johnson, O.E.; Odole, A.C.; Ishaya, G.P.; Omole, O.J.; Makinde, M.O. Comparative efficacy of clinic-based and telerehabilitation application of Mckenzie therapy in chronic low-back pain. Int. J. Telerehabilitation 2019, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, D.L. Home Program Instruction Sheets for Infants and Young Children; Therapy Skill Builders: Tucson, AZ, USA, 1987. [Google Scholar]
- Zhang, R.; Cao, S. Real-time human motion behavior detection via CNN using mmWave radar. IEEE Sens. Lett. 2018, 3, 1–4. [Google Scholar] [CrossRef]
- Wu, Z.; Zhao, S.; Peng, Y.; He, X.; Zhao, X.; Huang, K.; Wu, X.; Fan, W.; Li, F.; Chen, M. Studies on different CNN algorithms for face skin disease classification based on clinical images. IEEE Access 2019, 7, 66505–66511. [Google Scholar] [CrossRef]
- Kidziński, Ł.; Yang, B.; Hicks, J.L.; Rajagopal, A.; Delp, S.L.; Schwartz, M.H. Deep neural networks enable quantitative movement analysis using single-camera videos. Nat. Commun. 2020, 11, 4054. [Google Scholar] [CrossRef]
- Oh, W.; An, Y.; Min, S.; Park, C. Comparative Effectiveness of Artificial Intelligence-Based Interactive Home Exercise Applications in Adolescents with Obesity. Sensors 2022, 22, 7352. [Google Scholar] [CrossRef]
- Arnoni, J.L.B.; Pavao, S.L.; dos Santos Silva, F.P.; Rocha, N.A.C.F. Effects of virtual reality in body oscillation and motor performance of children with cerebral palsy: A preliminary randomized controlled clinical trial. Complement. Ther. Clin. Pract. 2019, 35, 189–194. [Google Scholar] [CrossRef]
- Jung, Y.G.; Chang, H.J.; Jo, E.S.; Kim, D.H. The Effect of a Horse-Riding Simulator with Virtual Reality on Gross Motor Function and Body Composition of Children with Cerebral Palsy: Preliminary Study. Sensors 2022, 22, 2903. [Google Scholar] [CrossRef]
- Luna-Oliva, L.; Ortiz-Gutiérrez, R.M.; Cano-de la Cuerda, R.; Piédrola, R.M.; Alguacil-Diego, I.M.; Sánchez-Camarero, C.; Martínez Culebras Mdel, C. Kinect Xbox 360 as a therapeutic modality for children with cerebral palsy in a school environment: A preliminary study. NeuroRehabilitation 2013, 33, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Chuang, T.Y.; Sung, W.H.; Chang, H.A.; Wang, R.Y. Effect of a virtual reality-enhanced exercise protocol after coronary artery bypass grafting. Phys. Ther. 2006, 86, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Cacau, L.d.A.P.; Oliveira, G.U.; Maynard, L.G.; Araújo Filho, A.A.d.; Silva, W.M.d., Jr.; Cerqueria Neto, M.L.; Antoniolli, A.R.; Santana-Filho, V.J. The use of the virtual reality as intervention tool in the postoperative of cardiac surgery. Braz. J. Cardiovasc. Surg. 2013, 28, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.-F.; Tsai, P.-Y.; Sung, W.-H.; Lin, C.-Y.; Chuang, T.-Y. The comparisons of heart rate variability and perceived exertion during simulated cycling with various viewing devices. Presence 2008, 17, 575–583. [Google Scholar] [CrossRef]
- McGrady, A.; McGinnis, R.; Badenhop, D.; Bentle, M.; Rajput, M. Effects of depression and anxiety on adherence to cardiac rehabilitation. J. Cardiopulm. Rehabil. Prev. 2009, 29, 358–364. [Google Scholar] [CrossRef]
- Tachibana, K.; Kikuchi, K.; Sugimoto, M.; Osuda, K.; Iwashiro, Y.; Arihara, A.; Okawa, A. Virtual Reality Simulation for Minimally Invasive Coronary Artery Bypass Grafting With Aortic No-Touch Total Arterial Grafting Technique. Innovations 2022, 17, 430–437. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CPT a Group (n = 13) | MPT b Group (n = 13) | p-Value | |
|---|---|---|---|
| Sex (male/female) | 6/7 | 6/7 | 1.00 |
| Age (years) | 16.15 ± 3.16 | 17.43 ± 2.88 | 0.36 |
| Body height (cm) | 133.17 ± 21.41 | 140.21 ± 18.11 | 0.14 |
| Body mass (kg) | 38.44 ± 16.08 | 42.56 ± 20.37 | 0.10 |
| c CP classification | |||
| Spastic/ataxic | 10/3 | 11/2 | 0.64 |
| CPT b | MPT c | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Pre Test | Post Test | Pre Test | Post Test | Time Effect | Between Groups | Time × Group Interaction | |
| GMFM a | 68.13 ± 18.27 | 72.66 ± 20.17 | 70.16 ± 11.37 | 75.01 ± 18.16 | 0.001 * | 0.21 | 0.48 |
| CPT c | MPT d | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Pre Test | Post Test | Pre Test | Post Test | Time Effect | Between Groups | Time × Group Interaction | |
| HR a | 78.16 ± 4.88 | 79.14 ± 3.17 | 74.84 ± 5.12 | 81.44 ± 4.11 | 0.03 * | 0.17 | 0.001 * |
| BRPE b | 11.14 ±0.88 | 10.88 ±1.43 | 12.26 ±1.10 | 10.13 ±0.75 | 0.001 * | 0.03 * | 0.02 * |
| CPT c | MPT d | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Pre Test | Post Test | Pre Test | Post Test | Time Effect | Between Groups | Time × Group Interaction | |
| FIM a | 17.88 ± 8.33 | 18.21 ± 6.42 | 16.79 ± 9.77 | 18.33 ± 11.21 | 0.17 | 0.33 | 0.18 |
| QOL b | 56.21 ± 17.44 | 53.19 ± 14.66 | 54.88 ± 16.71 | 52.67 ± 15.85 | 0.09 | 0.51 | 0.30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, I.; An, Y.; Min, S.; Park, C. Therapeutic Effects of Metaverse Rehabilitation for Cerebral Palsy: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021578
Moon I, An Y, Min S, Park C. Therapeutic Effects of Metaverse Rehabilitation for Cerebral Palsy: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(2):1578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021578
Chicago/Turabian StyleMoon, Ilyoung, Yeongsang An, Seunghwa Min, and Chanhee Park. 2023. "Therapeutic Effects of Metaverse Rehabilitation for Cerebral Palsy: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 2: 1578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021578