
Evaluating the Effects of Capacity Building Initiatives and Primary Care Networks in Singapore: Outcome Harvesting of System Changes to Chronic Disease Care Delivery

Abstract
:1. Introduction
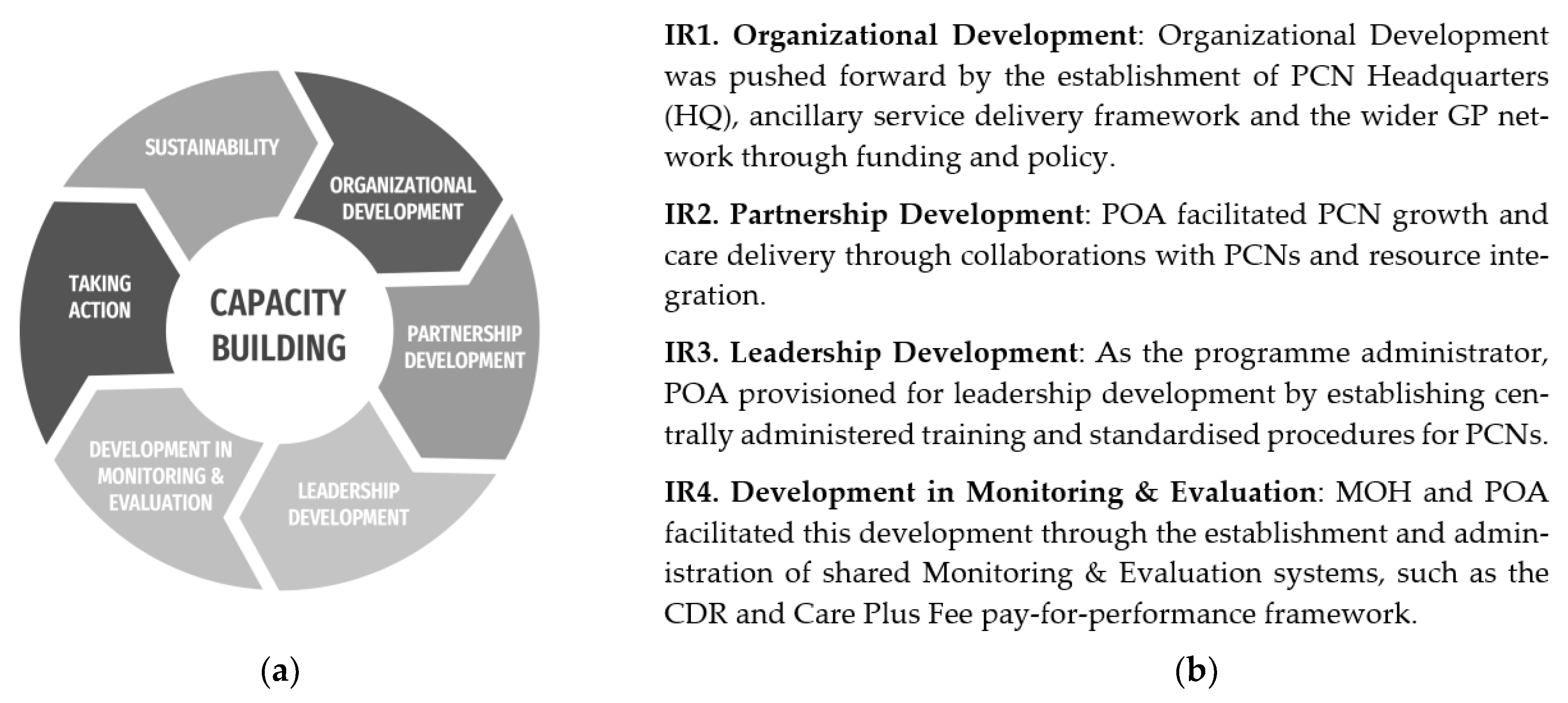
1.1. Conceptual Model
1.2. Aims and Research Questions
- What are the observed PCN outcomes that have resulted from the capacity building initiatives of the programme?
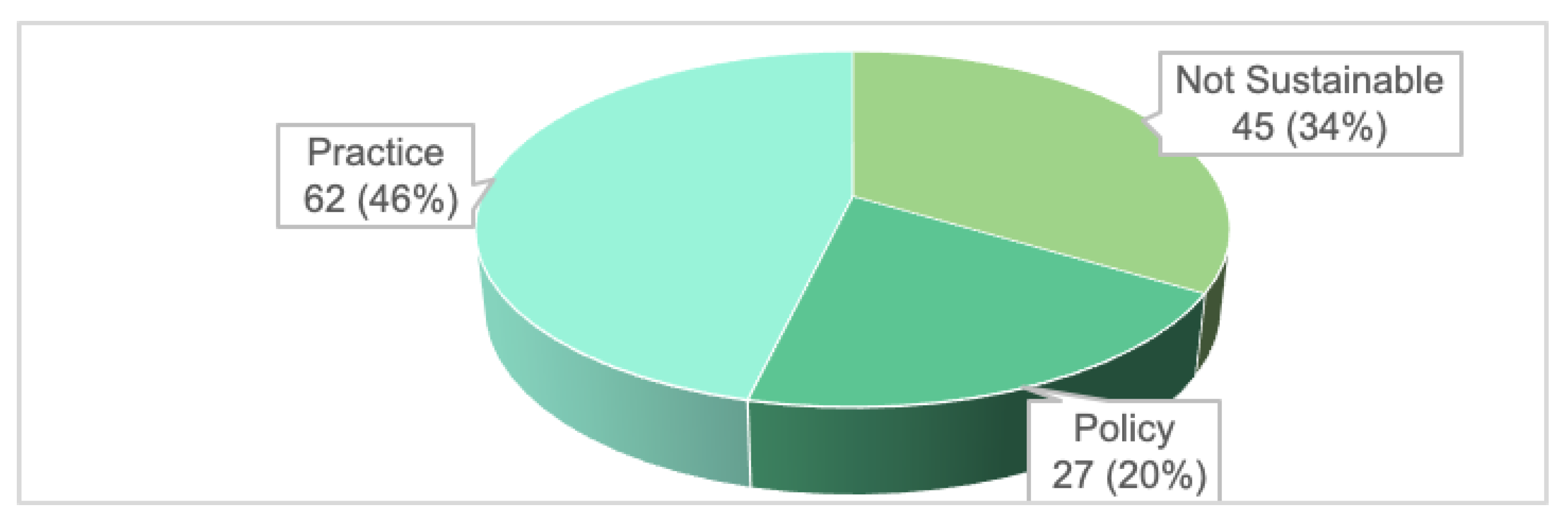
- How sustainable are the outcomes that have been initiated by participation in the PCN?
2. Methods
2.1. Methodology Overview
2.2. Ethical Procedures
2.3. Participant Profile
3. Results
3.1. Question 1: What Are the Observed PCN Outcomes That Have Resulted from the Capacity Building Initiatives of the Programme?
3.1.1. IR1 Organisational Development: Establishment of PCN HQ, Ancillary Services and the Wider GP Network through Funding and Policy
3.1.2. IR2 Partnership Development: PCN Growth through Collaborations and Resource Integration
3.1.3. IR3 Leadership Development: Establishment of Standardised Procedures and Training
3.1.4. IR4 Development in Monitoring and Evaluation: Establishment and Administration of Shared Monitoring and Evaluation Systems
3.2. Question 2: How Sustainable Are the Outcomes That Have Been Initiated by Participation in the PCN?
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A. Breakdown of Charted Data into Tabular Format

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
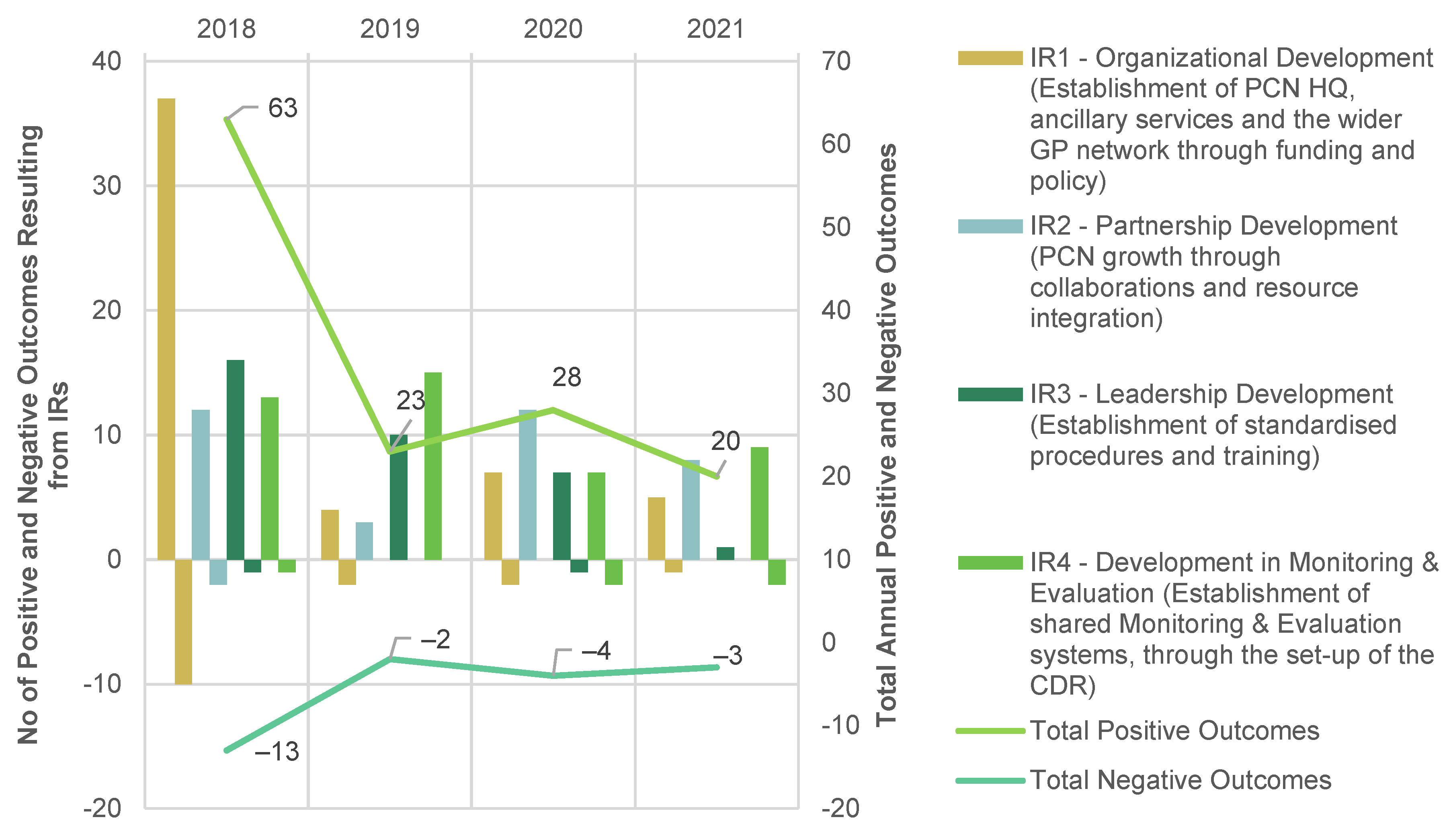
| Year | Total (+) | Total (−) | IR1 (+) | IR1 (−) | IR2 (+) | IR2 (−) | IR3 (+) | IR3 (−) | IR4 (+) | IR4 (−) |
|---|---|---|---|---|---|---|---|---|---|---|
| 2018 | 63 | −13 | 37 | −10 | 12 | −2 | 16 | −1 | 13 | −1 |
| 2019 | 23 | −2 | 4 | −2 | 3 | 0 | 10 | 0 | 15 | 0 |
| 2020 | 28 | −4 | 7 | −2 | 12 | 0 | 7 | −1 | 7 | −2 |
| 2021 | 20 | −3 | 5 | −1 | 8 | 0 | 1 | 0 | 9 | −2 |
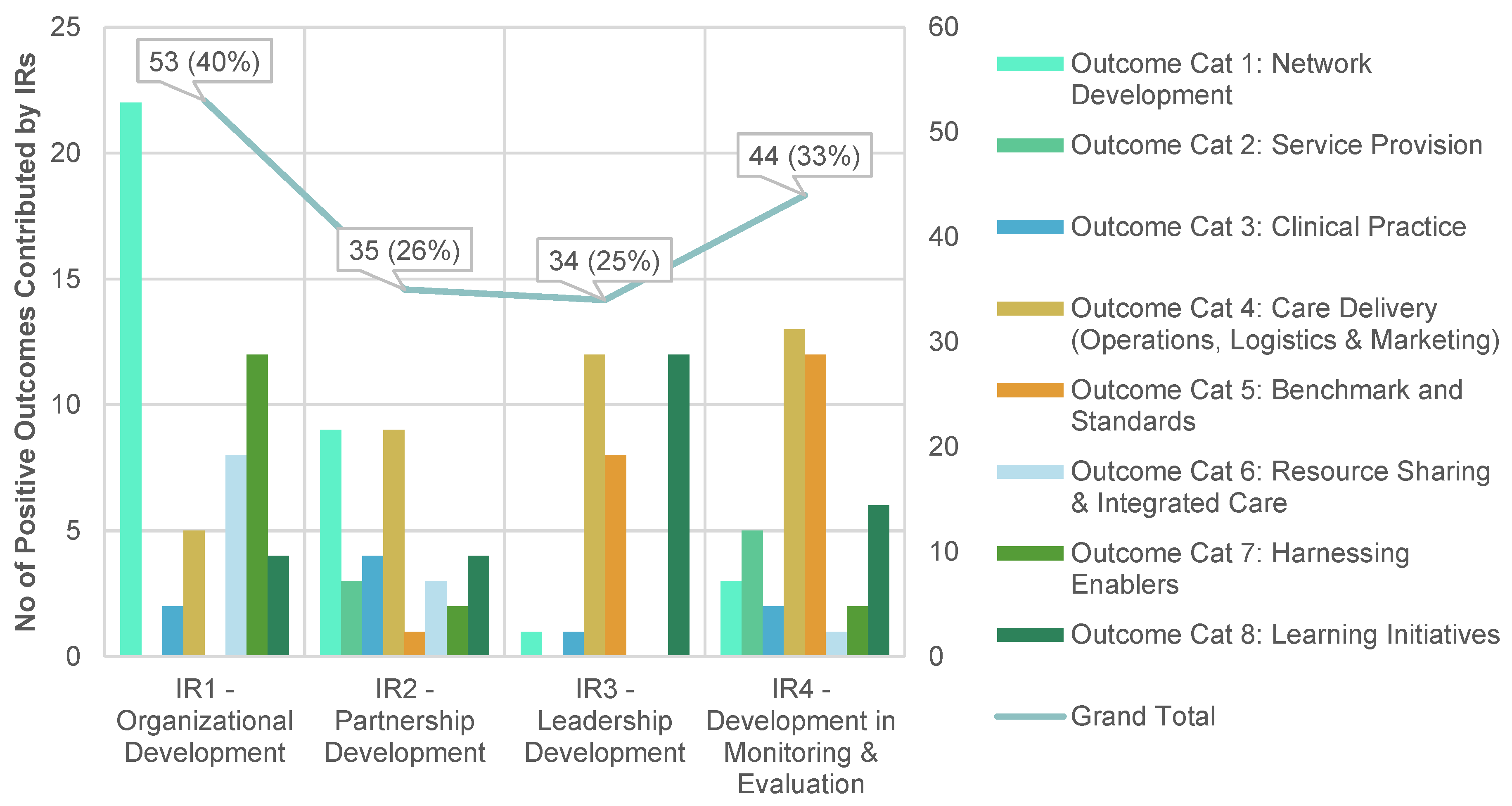
| IRs | Cat 1 | Cat 2 | Cat 3 | Cat 4 | Cat 5 | Cat 6 | Cat 7 | Cat 8 | Grand Total |
|---|---|---|---|---|---|---|---|---|---|
| IR1 | 22 | 0 | 2 | 5 | 0 | 8 | 12 | 4 | 53 |
| IR2 | 9 | 3 | 4 | 9 | 1 | 3 | 2 | 4 | 35 |
| IR3 | 1 | 0 | 1 | 12 | 8 | 0 | 0 | 12 | 34 |
| IR4 | 3 | 5 | 2 | 13 | 12 | 1 | 2 | 6 | 44 |
| IRs | Cat 1 | Cat 2 | Cat 4 | Cat 5 | Cat 6 | Grand Total |
|---|---|---|---|---|---|---|
| IR1 | 3 | 4 | 1 | 0 | 7 | 15 |
| IR2 | 1 | 0 | 1 | 0 | 0 | 2 |
| IR3 | 0 | 0 | 2 | 0 | 0 | 2 |
| IR4 | 1 | 0 | 2 | 2 | 0 | 5 |
Appendix B. Grouped Outcomes
| Outcome Category | Key Outcomes Sub-Category | Grouped Outcomes | S/N of Individual Outcome (N = Total) |
|---|---|---|---|
| Category 1: Network Development | Governance, resource allocation and involvement of parent organisation |
| 4, 5, 6, 25, 71, 72 (N = 6) |
| 15, 17 (N = 2) | ||
| 14 (N = 1) | ||
| GP onboarding, engagement and cohesion building |
| 13, 19, 25, 26(N = 4) | |
| 8 (N = 1) | ||
| 1, 2, 3, 9, 10, 11, 17, 20, 21, 27, 40, 57, 75, 78, 109, 142, 147 (N = 17) | ||
| 16, 95 (N = 2) | ||
| Corporate governance |
| 56, 66 (N = 2) | |
| Pre-existing network and infrastructure |
| 19, 37, 71, 124, 127 (N = 5) | |
| GP engagement |
| 12 (N = 1) | |
| Limited Resource Allocation |
| 5 (N = 1) | |
| Cluster Catchment Policy |
| 24, 32, 39 (N = 3) | |
| Category 2: Service Provision | Models of Ancillary Service Delivery |
| 18, 29, 30, 31, 33, 36, 37, 62, 74, 76 (N = 10) |
| 30, 107, 114 (N = 3) | ||
| 18, 29, 36(N = 3) | ||
| 82 (N = 1) | ||
| Ground-up Initiatives |
| 110 (N = 1) | |
| 35, 41, 47, 130 (N = 4) | ||
| Financial Access |
| 34 (N = 1) | |
| Internal referral system |
| 38 (N = 1) | |
| Category 3: Clinical Practice | Mental Health Care Initiatives |
| 41, 42, 44, 46, 50, 55, 116, 130, 147, 152 (N = 10) |
| Secondary screening |
| 43, 45 (N = 2) | |
| Clinical Audits |
| 49 (N = 1) | |
| Category 4: Care Delivery (Operations, Logistics, Marketing) | One-Stop Ancillary Services |
| 18, 30, 31, 52, 59, 62, 80 (N = 7) |
| Nurse Counselling (NC) |
| 53, 54, 58, 69, 124 (N = 5) | |
| Administrative support |
| 10, 30, 57, 75, 77, 85 (N = 6) | |
| Platform for COVID initiatives |
| 51, 60, 61, 79, 81 (N = 5) | |
| Ancillary service delivery |
| 52 (N = 1) | |
| COVID impact on chronic disease management |
| 61 (N = 1) | |
| Limited Resources for ancillary service delivery |
| 70 (N = 1) | |
| Category 5: Benchmarks and Standards | Data Management (data collection, transfer, maintaining data integrity and analysis) |
| 64, 77, 92(N = 3) |
| 87, 89, 96 (N = 3) | ||
| 112, 125, 127, 128, 129(N = 5) | ||
| 96 (N = 1) | ||
| 118, 123 (N = 2) | ||
| 98 (N = 1) | ||
| Gap Analysis and Quality Improvements |
| 75, 85, 86, 88, 91, 93, 95, 99, 139, 149 (N = 10) | |
| 48, 91, 93, 95, 96 (N = 5) | ||
| Data Presentation & Dissemination |
| 94, 96, 135 (N = 3) | |
| Process Indicators |
| 90 (N = 1) | |
| Pay-for-Performance framework |
| 97 (N = 1) | |
| Administrative burden of CDR |
| 2 (N = 1) | |
| Category 6: Resource Sharing and Integrated Care | Right-siting |
| 67, 68, 105 (N = 3) |
| GP+ Co-operative |
| 102, 115 (N = 2) | |
| Medication Access |
| 55, 84 (N = 2) | |
| Right-siting |
| 63, 104 (N = 2) | |
| 68, 100, 101, 103, 106, 113 (N = 6) | ||
| 108 (N = 1) | ||
| Category 7: Harnessing Enablers | EMR adoption |
| 121 (N = 1) |
| Patient Engagement Apps |
| 122, 126 (N = 2) | |
| Pay-for-Performance framework |
| 119 (N = 1) | |
| Category 8: Learning initiatives | Collaborative learning |
| 133, 136, 140, 144, 148, 150, 151 (N = 7) |
| 138 (N = 1) | ||
| Training |
| 131, 132, 134, 137, 141, 146(N = 6) | |
| 143 (N = 1) |
References
- Ministry of Health. Population and Vital Statistics. Available online: https://www.moh.gov.sg/resources-statistics/singapore-health-facts/population-and-vital-statistics (accessed on 13 May 2022).
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef]
- The Straits Times. Shifting Focus to Preventive Care Is Difficult But Right Thing To Do: PM Lee. Available online: https://www.straitstimes.com/singapore/shifting-healthcare-focus-to-preventive-care-is-difficult-but-right-thing-to-do-says-pm-lee (accessed on 24 April 2022).
- Tan, C.C.; Lam, C.S.P.; Matchar, D.B.; Zee, Y.K.; Wong, J.E.L. Singapore’s health-care system: Key features, challenges, and shifts. Lancet 2021, 398, 1091–1104. [Google Scholar] [CrossRef]
- Khoo, H.S.; Lim, Y.W.; Vrijhoef, H.J.M. Primary healthcare system and practice characteristics in Singapore. Asia Pac. Fam. Med. 2014, 13, 8. [Google Scholar] [CrossRef] [Green Version]
- Nurjono, M.; Shrestha, P.; Ang, I.Y.H.; Shiraz, F.; Eh, K.X.; Toh, S.E.S.; Vrijhoef, H.J.M. Shifting care from hospital to community, a strategy to integrate care in Singapore: Process evaluation of implementation fidelity. BMC Health Serv. Res. 2020, 20, 452. [Google Scholar] [CrossRef] [PubMed]
- Satkunanantham, K.; Lee, C.E. Singapore’s Health Care System: What 50 Years Have Achieved; World Scientific: Singapore, 2016; pp. 203–218. [Google Scholar]
- Ministry of Health. Primary Healthcare Services. Available online: https://www.moh.gov.sg/home/our-healthcare-system/healthcare-services-and-facilities/primary-healthcare-services (accessed on 17 June 2022).
- Lim, J. Myth or Magic: The Singapore Healthcare System; Select Publishing: Singapore, 2013; pp. 233–236. [Google Scholar]
- Chow, W.L.; Wang, V.W.; Low, Y.S.; Tse, D.W.; Lim, J.F. Factors that influence the choice of seeking treatment at polyclinics. Singap. Med. J. 2012, 53, 109–115. [Google Scholar]
- Ministry of Health. Primary Care Survey Report 2014. Available online: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/reports/moh-primary-care-survey-2014-report.pdf (accessed on 28 May 2022).
- Ministry of Health. Primary Care Networks. Available online: https://www.moh.gov.sg/home/our-healthcare-system/healthcare-services-and-facilities/primary-care-networks (accessed on 13 May 2022).
- Liow, Y.; Young, D.; Stavdal, A.; Valderas, J.M. From Astana to Singapore: Primary Health Care is key to the long-term success of Singapore’s health system. Ann. Acad. Med. Singap. 2022, 51, 528–530. [Google Scholar] [CrossRef]
- Cumming, J. Integrated care in New Zealand. Int. J. Integr. Care 2011, 11, e138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levesque, J.-F.; Strumpf, E.; Coyle, N.; Hutchison, B. Primary health care in Canada: Systems in motion. Milbank Q. 2011, 89, 256–288. [Google Scholar] [CrossRef] [Green Version]
- Center for Innovative Education Solutions. Capacity Building Model. Available online: https://www.innovativeedsolutions.org (accessed on 1 November 2022).
- Bauer, M.S.; Kirchner, J. Implementation science: What is it and why should I care? J. Psychiatry Res. 2020, 283, 112376. [Google Scholar] [CrossRef]
- Agency of Integrated Care. Healthier SG. Available online: https://www.aic.sg/about-us/Pages/Initiatives/Healthier-SG.aspx (accessed on 16 May 2022).
- Gurman, T.A.; Awangtang, G.; Leslie, L.T. Evaluating Capacity Strengthening for Social and Behaviour Change Communication through Outcome Harvesting. J. Dev. Commun. 2018, 29, 45–61. [Google Scholar]
- Selvaraj, K. Outcome Harvesting. 2020. Available online: https://evaluatingadvocacy.org/doc/Outcome-harvesting.pdf (accessed on 15 May 2022).
- Wilson-Grau, R.; Britt, H. Outcome Harvesting. 2013. Available online: https://outcomeharvesting.net/outcome-harvesting-brief/ (accessed on 15 May 2022).
- Ministry of Health. White Paper on Healthier SG. Ministry of Health (MOH): 2022. Available online: https://file.go.gov.sg/healthiersg-whitepaper-pdf.pdf (accessed on 21 September 2022).
- Chua, L.K.L.; Chong, C.K.; Wee, H.-l.; Tham, T.Y. Primary care network (PCN) as a model of care for GP chronic disease management. Singap. Fam. Physician 2015, 41, 61–64. [Google Scholar]
- Milat, A.J.; King, L.; Bauman, A.E.; Redman, S. The concept of scalability: Increasing the scale and potential adoption of health promotion interventions into policy and practice. Health Promot. Int. 2013, 28, 285–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooley, L.; Kohl, R. Scaling up—From Vision to Large-Scale Change: A Management Framework for Practitioners, 3rd ed.; Management Systems International: Washington, DC, USA, 2016. [Google Scholar]
- The Straits Times. What It Takes to Arrive at a Healthier Singapore: Teo Yik Ying. Available online: https://www.straitstimes.com/opinion/what-it-takes-to-arrive-at-a-healthier-singapore (accessed on 20 October 2022).
- Levengood, T.W.; Peng, Y.; Xiong, K.Z.; Song, Z.; Elder, R.; Ali, M.K.; Chin, M.H.; Allweiss, P.; Hunter, C.M.; Becenti, A. Team-Based Care to Improve Diabetes Management: A Community Guide Meta-analysis. Am. J. Prev. Med. 2019, 57, e17–e26. [Google Scholar] [CrossRef] [PubMed]
- Boston Consulting Group. Capitation for Population Health: A Great Start But What’s Next? Available online: https://www.theedgesingapore.com/views/healthcare/capitation-population-health-great-start-whats-next (accessed on 24 March 2022).
- Boston Consulting Group. Successful Transition to Capitation Models—Is Data & Analytics the Secret Sauce? Available online: https://www.theedgesingapore.com/views/healthcare/successful-transition-capitation-models--data-analytics-secret-sauce (accessed on 31 March 2022).
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health. Speech by Minister for Health, Mr Ong Ye Kung, at the MOH Work Plan Seminar, 2 June 2022. Available online: https://www.moh.gov.sg/news-highlights/details/speech-by-minister-for-health-mr-ong-ye-kung-at-the-moh-work-plan-seminar-2022-2-june-2022 (accessed on 3 June 2022).
- Surendran, S.; Foo, C.; Tam, C.H.; Ho, E.Q.Y.; Matchar, D.B.; Car, J.; Koh, G.C.H. The Missed Opportunity of Patient-Centered Medical Homes to Thrive in an Asian Context. Int. J. Environ. Res. Public Health 2021, 18, 1817. [Google Scholar] [CrossRef] [PubMed]
- Ngoh, S.; Tang, W.E.; Chng, E.; Chong, P.N. Comment on Surendran et al. The Missed Opportunity of Patient-Centered Medical Homes to Thrive in an Asian Context. Int. J. Environ. Res. Public Health 2021, 18, 1817. Int. J. Environ. Res. Public Health 2022, 19, 4683. [Google Scholar] [CrossRef]
- Surendran, S.; Foo, C.; Tam, C.H.; Ho, E.Q.Y.; Matchar, D.B.; Car, J.; Koh, G.C.H. Reply to Ngoh et al. Comment on “Surendran et al. The Missed Opportunity of Patient-Centered Medical Homes to Thrive in an Asian Context. Int. J. Environ. Res. Public Health 2022, 18, 1817”. Int. J. Environ. Res. Public Health 2022, 19, 4686. [Google Scholar] [CrossRef]
- Today. MOH to Look Into Concerns of Price Gap between Drugs at Polyclinics and Private GPs as Part of Healthier SG Push. Available online: https://www.todayonline.com/singapore/moh-examine-price-gap-medicine-gp-polyclinic-1900861 (accessed on 18 May 2022).
- Bearden, T.; Ratcliffe, H.L.; Sugarman, J.R.; Bitton, A.; Anaman, L.A.; Buckle, G.; Cham, M.; Quan, D.C.W.; Ismail, F.; Jargalsaikhan, B. Empanelment: A foundational component of primary health care. Gates Open Res. 2019, 3, 1654. [Google Scholar] [CrossRef]
- Chong, P.-N.; Tang, W.E. Transforming primary care—The way forward with the TEAMS2 approach. Fam. Pract. 2018, 36, 369–370. [Google Scholar] [CrossRef]
- Foo, C.D.; Surendran, S.; Jimenez, G.; Ansah, J.P.; Matchar, D.B.; Koh, G.C.H. Primary Care Networks and Starfield’s 4Cs: A Case for Enhanced Chronic Disease Management. Int. J. Environ. Res. Public Health 2021, 18, 2926. [Google Scholar] [CrossRef]
- Foo, C.D.; Surendran, S.; Tam, C.H.; Ho, E.; Matchar, D.B.; Car, J.; Koh, G.C.H. Perceived facilitators and barriers to chronic disease management in primary care networks of Singapore: A qualitative study. BMJ Open 2021, 11, e046010. [Google Scholar] [CrossRef] [PubMed]
- Surendran, S.; Foo, C.; Matchar, D.B.; Ansah, J.P.; Car, J.; Koh, G.C.H. Developing integration among stakeholders in the primary care networks of Singapore: A qualitative study. BMC Health Serv. Res. 2022, 22, 782. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, A.T.H.; Koh, G.C.-H.; Fong, N.P.; Lim, J.F.Y.; Hildon, Z.J.-L. Evaluating the Effects of Capacity Building Initiatives and Primary Care Networks in Singapore: Outcome Harvesting of System Changes to Chronic Disease Care Delivery. Int. J. Environ. Res. Public Health 2023, 20, 2192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032192
Chen ATH, Koh GC-H, Fong NP, Lim JFY, Hildon ZJ-L. Evaluating the Effects of Capacity Building Initiatives and Primary Care Networks in Singapore: Outcome Harvesting of System Changes to Chronic Disease Care Delivery. International Journal of Environmental Research and Public Health. 2023; 20(3):2192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032192
Chicago/Turabian StyleChen, Andrew Teik Hong, Gerald Choon-Huat Koh, Ngan Phoon Fong, Jeremy Fung Yen Lim, and Zoe Jane-Lara Hildon. 2023. "Evaluating the Effects of Capacity Building Initiatives and Primary Care Networks in Singapore: Outcome Harvesting of System Changes to Chronic Disease Care Delivery" International Journal of Environmental Research and Public Health 20, no. 3: 2192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032192