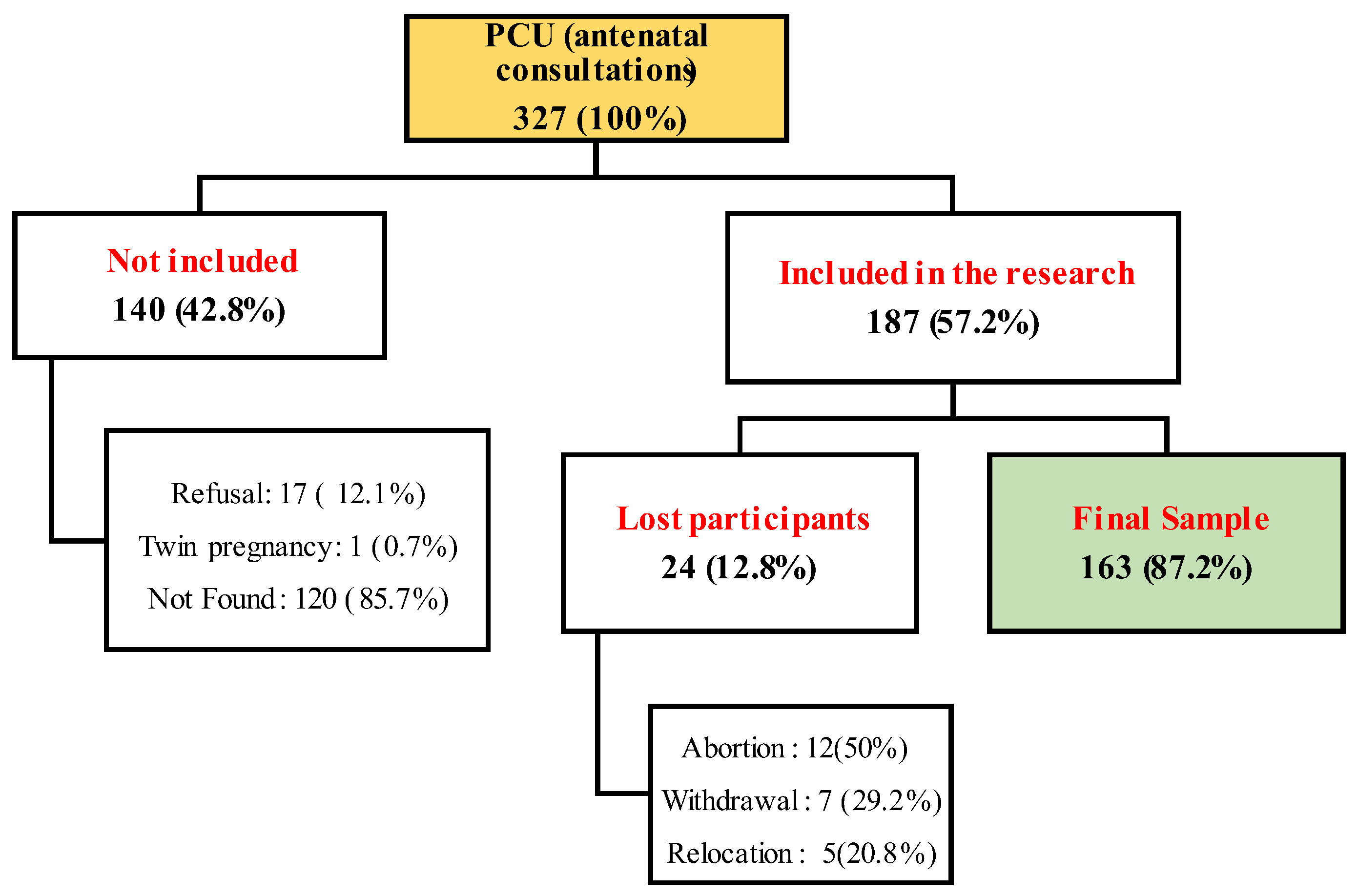
In this exploratory study, we investigated the exposure to Pb, Cd, As, and Mn in biological samples (blood, hair, and toenails) of 163 pregnant women residing in two municipalities in the Recôncavo Baiano, Brazil. The exposure level to As was very low, with 98% of the participants having AsH below the method’s LOD. However, 4.3 and 5.1% of the participants had biomarkers above the recommended reference values for Mn and Pb. We found a worrying situation regarding exposure to Cd, given that 22.2 to 61.1% of the pregnant women had high levels depending on the reference value considered. This work demonstrates the importance and urgency of implementing, as in developed countries, biomonitoring strategies in the general population, especially in those of vulnerable groups such as pregnant women and children living in impoverished regions. The low SES, domestic waste burning, passive smoking, being multiparous, and having renovated the house were some of the determinant factors of the high levels of Mn, Pb, and Cd in this population.
4.1. Lead
Considering the environmental sample, the median RtPb (13.0 µg/m
2/30 days) was much lower than the reference (431 µg/m
2) suggested by the US Agency for Environmental Protection [
43]. As our methodology considered the duration (30 days) of dust deposition, we estimated for the period of gestation the range of exposure of our study population, using the minimum and maximum range found (0.57 to 89.9 µg/m
2/30 days). The results (5.13 to 802.71 µg/m
2 for nine months) showed a probable situation of risk for these pregnant women.
Compared with another study carried out with school-age children in the municipality of Aratuípe, in a community producing Pb glazed ceramics (Maragogipinho district, Bahia, Brazil) [
19], the median level observed was lower than that found in the exposed (169 μg/m
2/30 days) or control (56.7 μg/m
2/30 days) group. In the case of other published works that used a methodology similar to this study, our average RtPb was identical to that found in homes (17 μg/m
2/30 days) in Germany [
44] or daycare centers in Sydney, Australia (22 μg/m
2/30 days) [
45]. This finding also corroborates with some of the reported geometric means of RtPb (between 19 and 63 μg/m
2/30 days) in elementary schools in Simões Filho, Bahia, Brazil [
5].
PbB levels have been associated significantly with RtPb, as observed in several studies [
19,
45,
46], showing evidence of the contribution of this matrix to human exposure. Although we found no correlation between RtPb and PbB, this possibility should be considered, as demonstrated by Ohtsu et al. [
47].
The median (range) 0.95 (0.05–16.4) µg/dL of PbB was lower than the CDC recent reference value (3.5 µg/dL) [
40,
48]. Nonetheless, some participants presented a risky situation for themselves and their fetus, such as the participants with PbB levels above the reference value [
40,
42]. Also, considering only the limited number of pregnant women (
n = 9) in the Maragogipinho district included in this research, the situation seems more worrying, since the median and mean PbB (3.07 and 1.9 μg/dL, respectively) were twofold higher than those found in the whole study population. It is essential to point out that these limits were not indicated as levels below which there are no toxic effects for humans, the pregnant woman, and the fetus [
15,
40,
49].
In other studies, reporting exposure to low levels of Pb, the median found here was lower than the findings by Silver et al. [
50], by La-Llave-León et al. [
51], and Guy et al., [
52] with a median (interquartile range) of 3.74 µg/dL (3.05–5.20). Despite the low level of PbB found by Guy et al. [
52] in Benin, contrary to our investigation, almost half of the participants had PbB above the new CDC reference value. Few studies with pregnant women have reported levels lower than or similar to ours, such as Ohtsu et al. [
47] in Japan, Wang et al. [
53] and Perkins et al., ([
54], in the USA). Despite this low level of PbB, Perkins et al. [
54] reported the adverse effects of Pb on anthropometric outcomes in children born to pregnant women in their cohort. Some research has shown the negative CNS impacts of prenatal exposure to low levels of Pb in children. For example, Silver et al. [
50] demonstrated an association of low levels of PbB with delayed maturation of the auditory and visual systems in neonates (with an average of two days of age), while Jedrychowski et al. [
55] reported their association with low neurocognitive performance in a six-month-old baby.
Despite sufficient evidence in the literature on the relationship between socioeconomic factors and Pb exposure, only multiparity was associated with PbB levels above the median. The lack of relationship with other factors was also reported in other studies; for example, Ohtsu et al. [
47] Taylor et al. [
15] and Guy et al. [
52] also found no association between PbB levels with factors such as exposure to cigarette smoking, SES, and the presence of peeling paint in the house. The low level of exposure, in addition to the absence of a specific exposure source, except for residents in Maragogipinho, maybe the reason, as reported by Taylor et al. [
15].
Although only a significant influence of multiparity on PbB levels was detected, it is relevant to highlight the possible influences of some socioeconomic and environmental covariates. Passive smoking had a median PbB 1.28 times higher (1.02 vs. 0.80 µg/dL; p = 0.786) compared to those not exposed to cigarette smoke. Pregnant women from lower SES or education levels had higher medians when compared to another category of the same variable considered. In addition, considering only homes with peeling paint (n = 67), pregnant women who reported having a lot or moderate amount of peeling paint in their home had a median PbB (1.35 vs. 0.73 µg/dL; p = 0.24) 1.85 times higher than those with a little peeled amount. Taking into account the toxicity of Pb for the pregnant woman and the fetus and the existence of evidence in the literature, we suggest considering these factors in eventual awareness sessions for participants in our cohort and decision-makers in the respective municipalities.
4.2. Manganese
Few participants presented values of the Mn biomarkers above the reference values [
38,
39]. Ward et al. [
39], suggested 4.14 µg/g as a cutoff point to distinguish welders exposed to Mn fumes from the control group of their study. Therefore, it is essential to consider that the reference values for these Mn biomarkers are also not related to the threshold compatible with the beneficial or deleterious effects of Mn. For the time being, there is little data on these matrices used as biomarkers either in the general population or in pregnant women [
2,
56,
57]. Studies in populations with low levels are therefore essential to contribute to the correct definition of these reference values concerning possible effects; our cohort study has the final objective of estimating the impact of these exposures on children’s neurodevelopment at 12 months.
Considering studies carried out with pregnant women, Mora et al. [
58], found a geometric mean of 1.8 µg/g in pregnant women’s hair in Costa Rica, while Rodrigues et al. [
36], reported medians of 27.1 and 34.7 µg/g, respectively, in Pabna and Sirajdikhan (in Bangladesh). The difference is that these studies were conducted in areas close to sources of exposure (such as plantations using pesticides and drinking water from highly contaminated artesian wells), which could explain these levels above ours. Other studies carried out in children (15.2 µg/g) and in non-pregnant women (4.4 µg/g) in areas close to a ferromanganese alloy plant in Brazil also reported levels well above the ones reported here [
3,
4]. Even in the control group of their research, Menezes-Filho et al. [
3] reported a median (1.76 µg/g) 8.8 times higher than those in this study. Regarding the evaluation of Mn in toenails, Signes-Pastor et al. [
57] found in pregnant women a median (range) of 0.34 (0.17–0.72) µg/g, two times lower than that reported in this study. Our findings do not corroborate with those of Rodrigues et al. [
36], probably due to the high levels of exposure.
Three factors associated with higher levels of Mn mainly stood out in the MLR: SES, waste burning, and passive exposure to cigarette smoke. However, most publications were carried out in populations with high exposure and mainly considered correlations or univariate analyzes [
56], which makes comparisons difficult. Despite using hair and nails as matrices to estimate exposure to Mn, Viana et al. [
4], found no correlation between Mn exposure and cigarette smoking or waste burning. Although Tasker et al. [
10] used blood as a matrix in their investigation, the authors reported a relationship between second hand cigarette smoking and blood Mn levels (MnB) in the second trimester. Still, their finding was contrary to ours (lower levels of MnB in smokers). Contrary to our findings, Viana et al. [
4] reported significantly higher median levels of MnH in individuals with less education.
Co-exposure to Pb and Mn: Of the metals evaluated, only Pb and Mn (PbB and MnTn) showed a correlation in their exposure dynamics. As the matrices (toenails and blood) do not suggest exposure simultaneously (7 to 12 months and 1-month window for toenails and blood [
4,
57], respectively), we suggest that this relationship is spurious and not related to any biological mechanism absorption of these metals.
4.3. Cadmium
CdB level is a biomarker of recent exposure to Cd, in addition to being a good proxy for chronic exposure to low levels; that is, even in a population not occupationally exposed, it is possible to find worrying levels [
59,
60]. The CdB values found in our study population point to a situation contrary to our expectations.
Mean and median values in this study exceeded CdB levels in workers and populations living close to areas with a source of exposure. Ferron et al. [
6] reported in recycling sorting workers from São Paulo an arithmetic mean (0.47 μg/L) and median (0.44 μg/L) lower than our values (respectively, 0.81 and 0.55 µg/L). The control group of this study presented an average value 6.7 times lower than ours. Also worrying was the maximum value (7.61 μg/L), which is well above what was found by Ferron et al. [
6] (2020) and Naka et al., [
61]. In non-pregnant women residing in the industrial zone of the state of Amazonas [
61], the authors also found a similar average (0.46 μg/L) while the control group presented a value (0.22 μg/L) 2.5 times lower.
Some studies conducted with general populations outside Brazil reported similar situations to ours. For example, Garner and Levallois [
35] in Canada reported a geometric mean of 0.43 μg/L in non-pregnant women, similar to Sakellari et al. [
62] in Greece and Johntson et al. [
60] from the USA. According to the authors [
35,
60], cigarette smoking may be the leading cause of the higher level of Cd. Indeed, as expected, passive exposure to cigarette smoke was significantly associated with a fourfold higher chance of having levels above 1 μg/L. Active smoking before pregnancy did not show a significant relationship with high levels of CdB, given the small number of observations. Passive cigarette smoking exposure is a relevant source of contamination of a multitude of compounds, which raises the importance of the shared responsibility of all residents in a home for the health of the pregnant woman and her fetus. Besides the pregnant woman stopping smoking, the other house residents would have to do the same or avoiding smoking indoors. Active or passive smoking status was self-reported by participants; the fact of not having evaluated cotinine, a biomarker of exposure to nicotine [
60] may be a limitation of our study. Nevertheless, pregnancy is often a reason that leads many women to stop smoking or reduce their habit.
House renovation (or painting) was another determining factor that increased the likelihood of having CdB levels above 1 or 0.6 μg/L. We suggest that the type of paint used during the renovation could explain this finding. In fact, during our visits to the participants’ homes, we noticed the reforms or changes in the residences to adjust for the arrival of the baby. Some works have shown the possibility of finding high levels of cadmium and other metals in paint pigments or building and renovation materials [
63,
64]. Other possible sources of exposure to Cd could be living close to or inside workshops or production units of palm oil, soap (some participants), or even a diet rich in shellfish or animal viscera. We have visited pregnant women whose homes were located in these environments. Regarding diet, data on food frequency is being processed.
None of the sociodemographic variables (SES, age, education, income, municipality) and the fact of not being primiparous were not associated with an increase in CdB above the reference values. Contrary to what was expected with alcohol consumption [
35,
60,
65], no association was detected, probably because pregnant women stopped drinking when they were aware of their pregnancy.

 ,
, 

{kind=link}