
The Relationship between Physical Activity and Mental Depression in Older Adults during the Prevention and Control of COVID-19: A Mixed Model with Mediating and Moderating Effects


Abstract
:1. Introduction
1.1. Physical Activity and Mental Depression
1.2. Mediation of Self-Efficacy
1.3. Moderation of Social Support
2. Materials and Methods
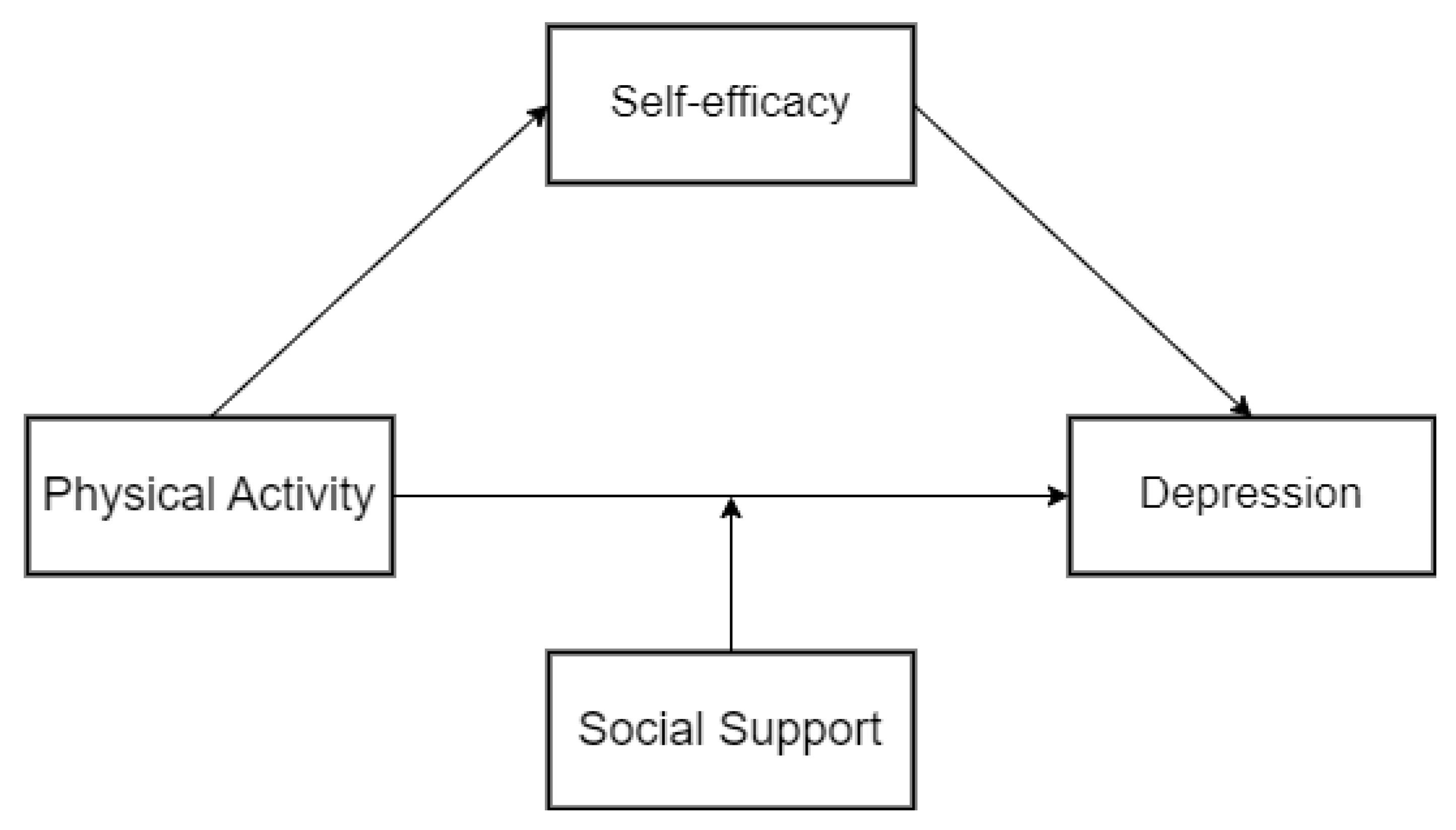
2.1. Hypotheses and Conceptual Model
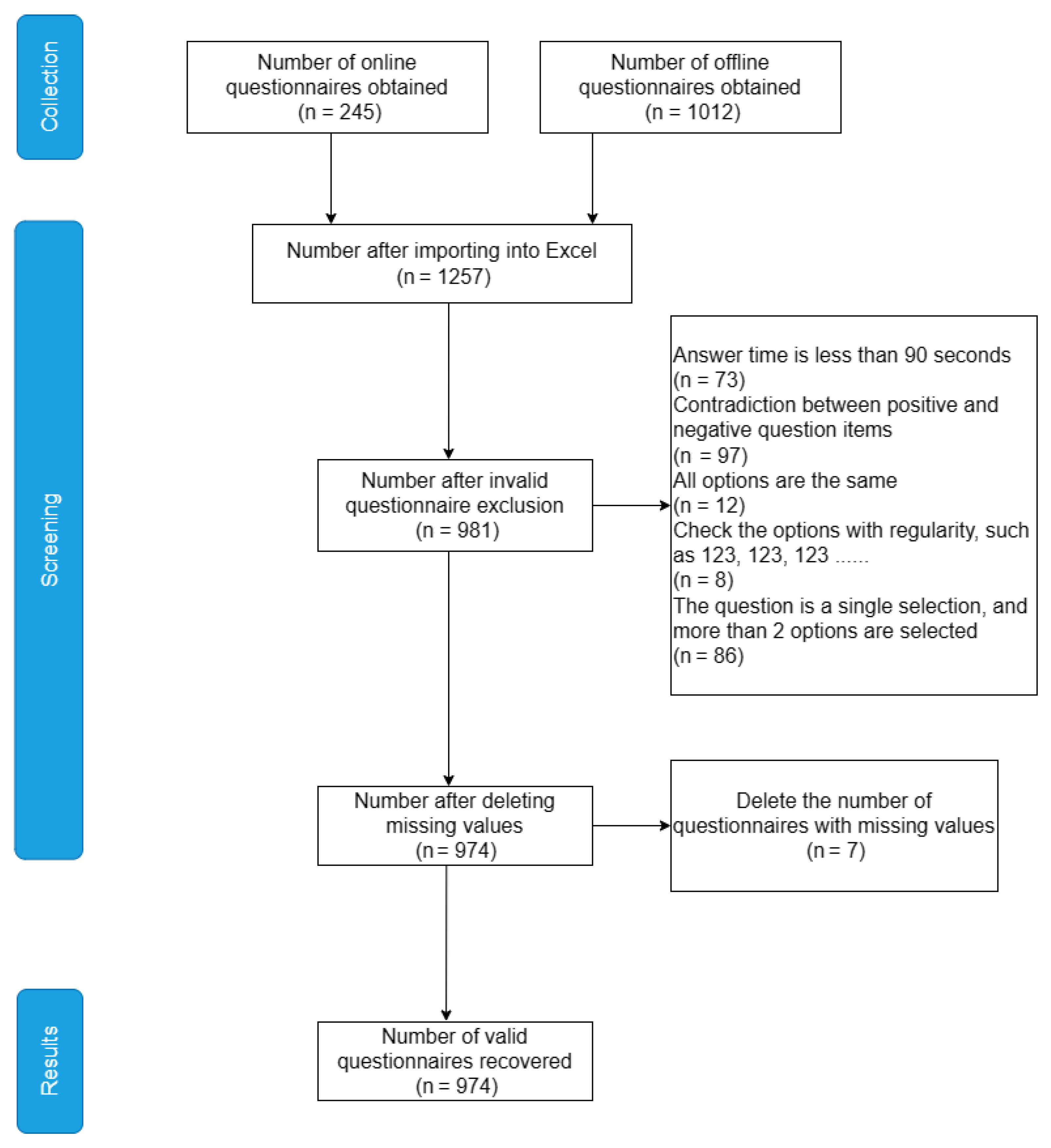
2.2. Participants and Procedures
2.3. Control Variables
2.4. Measurements
2.4.1. Physical Activity
2.4.2. Mental Depression
2.4.3. Self-Efficacy
2.4.4. Social Support
2.5. Statistical Analysis
3. Results
3.1. Analysis of the Sample Situation
3.2. Reliability and Validity Tests
3.3. Descriptive Statistics and Correlation Analysis
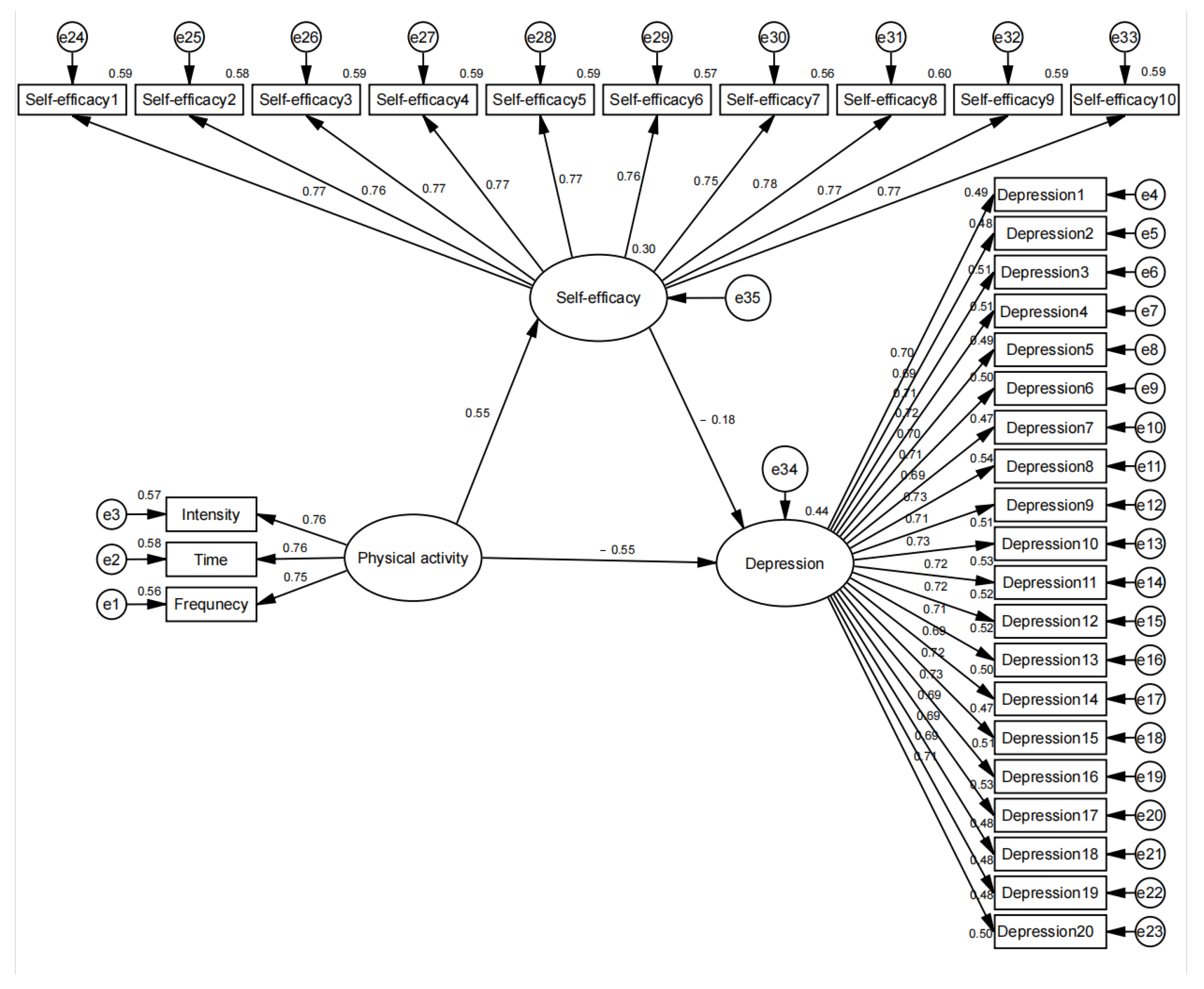
3.4. Mediating Analysis
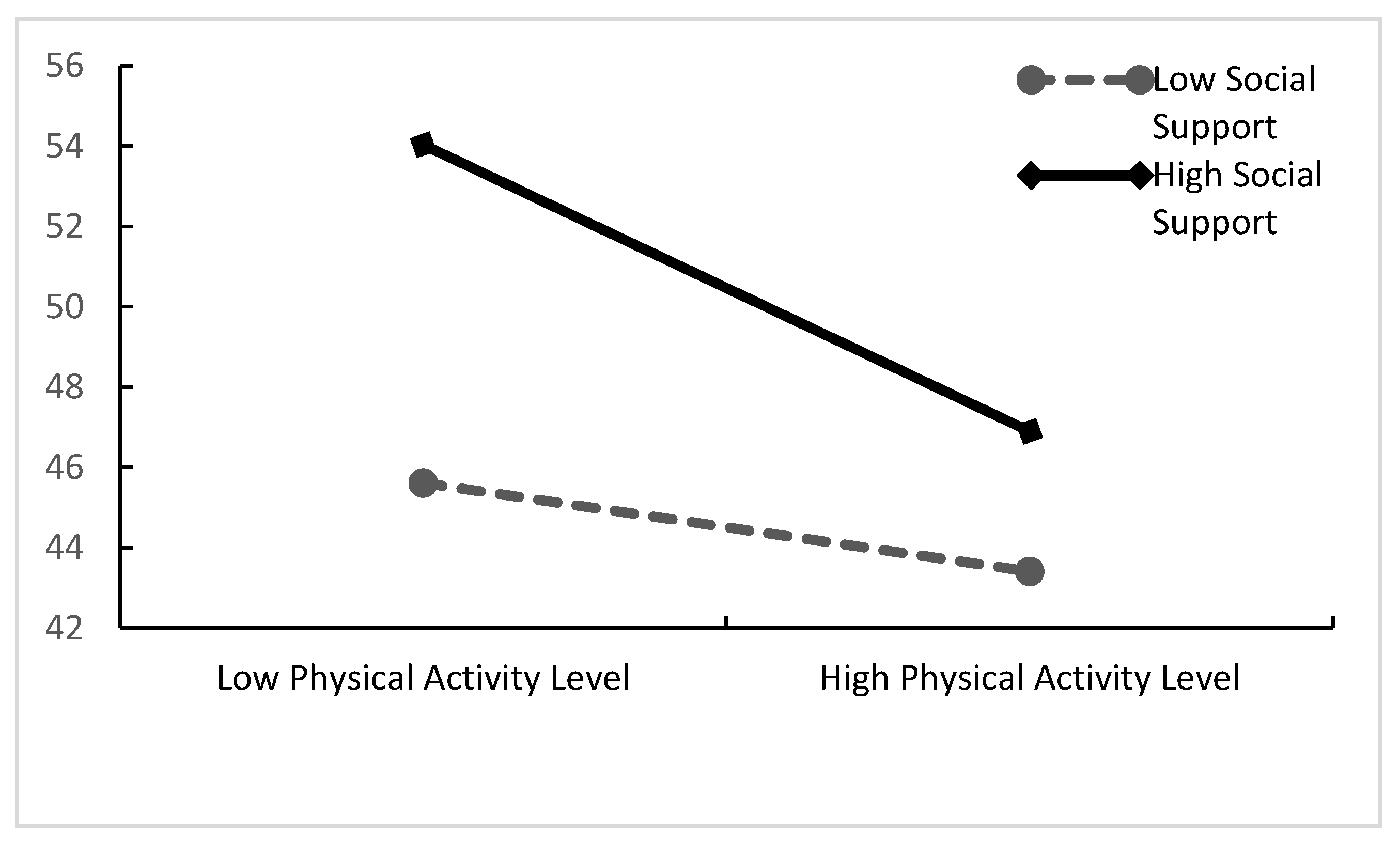
3.5. Moderating Analysis
4. Discussion
4.1. Physical Activity and Psychological Depression in Older Adults
4.2. Mediating Effect of Self-Efficacy
4.3. Moderating Effect of Social Support
4.4. Contributions
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. COVID-19 Public Health Emergency of International Concern (PHEIC) Global Research and Innovation Forum. Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum (accessed on 13 October 2022).
- Lee, K.; Jeong, G.C.; Yim, J. Consideration of the Psychological and Mental Health of the Elderly during COVID-19: A Theoretical Review. Int. J. Environ. Res. Public Health 2020, 17, 8098. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- AKİ, Ö.E. COVID-19 pandemic and the mental health of elderly. Turk. J. Geriatr./Türk Geriatr. Derg. 2020, 23, 291–298. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D.; WHO. The global Burden of Disease: A comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020: Summary; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Dinas, P.C.; Koutedakis, Y.; Flouris, A.D. Effects of exercise and physical activity on depression. Ir. J. Med. Sci. 2011, 180, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Delle Fave, A.; Bassi, M.; Boccaletti, E.S.; Roncaglione, C.; Bernardelli, G.; Mari, D. Promoting Well-Being in Old Age: The Psychological Benefits of Two Training Programs of Adapted Physical Activity. Front. Psychol. 2018, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Howard, E.P. Physical Activity and Positive Psychological Well-Being Attributes Among U.S. Latino Older Adults. J. Gerontol. Nurs. 2019, 45, 44–56. [Google Scholar] [CrossRef]
- Rejeski, W.J.; Mihalko, S.L. Physical activity and quality of life in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Tang, Y.; Jennings, G.; Zhao, B.; Zhu, F.; Ma, X. Physical activity and subjective well-being of older adults during COVID-19 prevention and control normalization: Mediating role of outdoor exercise environment and regulating role of exercise form. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, M.A.; Dakkalirad, A.; Saedi, F.; Shahnavazi, A.; Kordi, M.; Ahmadipour, M.; Dehghan, M. Depression and Self-Efficacy Among Iranian Children During the Prevalence of COVID-19 Disease. Front. Pediatr. 2022, 10, 888712. [Google Scholar] [CrossRef]
- Wu, Y.; Shao, J.; Zhang, D.; Wang, Y.; Wang, S.; Wang, Z.; Qu, Y.; Gu, J. Pathways from self-disclosure to medical coping strategy among adolescents with moderate and major depression during the COVID-19 pandemic: A mediation of self-efficacy. Front. Psychiatry 2022, 13, 976386. [Google Scholar] [CrossRef]
- Xiong, H.; Yi, S.; Lin, Y. The Psychological Status and Self-Efficacy of Nurses During COVID-19 Outbreak: A Cross-Sectional Survey. Inquiry 2020, 57, 46958020957114. [Google Scholar] [CrossRef]
- Mo, P.K.H.; Fong, V.W.I.; Song, B.; Di, J.; Wang, Q.; Wang, L. Association of Perceived Threat, Negative Emotions, and Self-Efficacy With Mental Health and Personal Protective Behavior Among Chinese Pregnant Women During the COVID-19 Pandemic: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e24053. [Google Scholar] [CrossRef] [PubMed]
- Kok, R.M.; Reynolds, C.F., 3rd. Management of Depression in Older Adults: A Review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef]
- Mishra, R.; Park, C.; York, M.K.; Kunik, M.E.; Wung, S.F.; Naik, A.D.; Najafi, B. Decrease in Mobility during the COVID-19 Pandemic and Its Association with Increase in Depression among Older Adults: A Longitudinal Remote Mobility Monitoring Using a Wearable Sensor. Sensors 2021, 21, 3090. [Google Scholar] [CrossRef]
- Teixeira, C.M.; Vasconcelos-Raposo, J.; Fernandes, H.M.; Brustad, R.J. Physical Activity, Depression and Anxiety Among the Elderly. Soc. Indic. Res. 2013, 113, 307–318. [Google Scholar] [CrossRef]
- O’Connor, P.J.; Aenchbacher, L.E.; Dishman, R.K. Physical Activity and Depression in the Elderly. J. Aging Phys. Act. 1993, 1, 34–58. [Google Scholar] [CrossRef]
- Lee, H.; Lee, J.A.; Brar, J.S.; Rush, E.B.; Jolley, C.J. Physical activity and depressive symptoms in older adults. Geriatr. Nurs. 2014, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Iwasa, H.; Kumagai, S.; Suzuki, T.; Awata, S.; Yoshida, H. Longitudinal association between habitual physical activity and depressive symptoms in older people. Psychiatry Clin. Neurosci. 2015, 69, 686–692. [Google Scholar] [CrossRef]
- Mata, J.; Thompson, R.J.; Jaeggi, S.M.; Buschkuehl, M.; Jonides, J.; Gotlib, I.H. Walk on the bright side: Physical activity and affect in major depressive disorder. J. Abnorm. Psychol. 2012, 121, 297–308. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C.; American College of Sports, M.; American Heart, A. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [Green Version]
- Uher, R.; Perlis, R.H.; Henigsberg, N.; Zobel, A.; Rietschel, M.; Mors, O.; Hauser, J.; Dernovsek, M.Z.; Souery, D.; Bajs, M.; et al. Depression symptom dimensions as predictors of antidepressant treatment outcome: Replicable evidence for interest-activity symptoms. Psychol. Med. 2012, 42, 967–980. [Google Scholar] [CrossRef]
- Walker, J.G.; Mackinnon, A.J.; Batterham, P.; Jorm, A.F.; Hickie, I.; McCarthy, A.; Fenech, M.; Christensen, H. Mental health literacy, folic acid and vitamin B12, and physical activity for the prevention of depression in older adults: Randomised controlled trial. Br. J. Psychiatry 2010, 197, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Fair, J.M.; Haskell, W.L.; Varady, A.N.; Iribarren, C.; Hlatky, M.A.; Go, A.S.; Fortmann, S.P. Validation of the Stanford Brief Activity Survey: Examining psychological factors and physical activity levels in older adults. J. Phys. Act. Health 2010, 7, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Bowe, A.K.; Owens, M.; Codd, M.B.; Lawlor, B.A.; Glynn, R.W. Physical activity and mental health in an Irish population. Ir. J. Med. Sci. 2019, 188, 625–631. [Google Scholar] [CrossRef]
- Ren, K.; Liu, X.; Feng, Y.; Li, C.; Sun, D.; Qiu, K. The Relationship between Physical Activity and Academic Procrastination in Chinese College Students: The Mediating Role of Self-Efficacy. Int. J. Environ. Res. Public Health 2021, 18, 11468. [Google Scholar] [CrossRef] [PubMed]
- Reigal, R.E.; Moral-Campillo, L.; Morillo-Baro, J.P.; Juarez-Ruiz de Mier, R.; Hernandez-Mendo, A.; Morales-Sanchez, V. Physical Exercise, Fitness, Cognitive Functioning, and Psychosocial Variables in an Adolescent Sample. Int. J. Environ. Res. Public Health 2020, 17, 1100. [Google Scholar] [CrossRef] [PubMed]
- Sowle, A.J.; Francis, S.L.; Margrett, J.A.; Shelley, M.C.; Franke, W.D. A Community-Based Exergaming Physical Activity Program Improves Readiness-to-Change and Self-Efficacy Among Rural-Residing Older Adults. J. Aging Phys. Act. 2017, 25, 432–437. [Google Scholar] [CrossRef]
- Tikac, G.; Unal, A.; Altug, F. Regular exercise improves the levels of self-efficacy, self-esteem and body awareness of young adults. J. Sports Med. Phys. Fit. 2022, 62, 157–161. [Google Scholar] [CrossRef]
- Pu, J.; Hou, H.P.; Ma, R.Y. Direct and Indirect Effects of Self-efficacy on Depression: The Mediating Role of Dispositional Optimism. Curr. Psychol. 2017, 36, 410–416. [Google Scholar] [CrossRef]
- Chao, C.Y.; Lemieux, C.; Restellini, S.; Afif, W.; Bitton, A.; Lakatos, P.L.; Wild, G.; Bessissow, T. Maladaptive coping, low self-efficacy and disease activity are associated with poorer patient-reported outcomes in inflammatory bowel disease. Saudi J. Gastroenterol. 2019, 25, 159–166. [Google Scholar] [CrossRef]
- Wu, S.F.; Huang, Y.C.; Lee, M.C.; Wang, T.J.; Tung, H.H.; Wu, M.P. Self-efficacy, self-care behavior, anxiety, and depression in Taiwanese with type 2 diabetes: A cross-sectional survey. Nurs. Health Sci. 2013, 15, 213–219. [Google Scholar] [CrossRef]
- Wang, L.; Luo, J.; Li, Y.; Zhou, Y.; Wang, W. Social support, anxiety, and depression in patients with prostate cancer: Complete mediation of self-efficacy. Support Care Cancer 2022, 30, 6851–6856. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Qiu, N.; Chen, C.; Wang, D.; Zhang, G.; Zhai, L. Self-Efficacy and Depression in Boxers: A Mediation Model. Front. Psychiatry 2020, 11, 00791. [Google Scholar] [CrossRef] [PubMed]
- Harandi, T.F.; Taghinasab, M.M.; Nayeri, T.D. The correlation of social support with mental health: A meta-analysis. Electron. Physician 2017, 9, 5212–5222. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cai, L.; Qian, J.; Peng, J. Social support moderates stress effects on depression. Int. J. Ment. Health Syst. 2014, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- DuPertuis, L.L.; Aldwin, C.M.; Bosse, R. Does the source of support matter for different health outcomes? Findings from the Normative Aging Study. J. Aging Health 2001, 13, 494–510. [Google Scholar] [CrossRef]
- da Silva, I.C.; Azevedo, M.R.; Goncalves, H. Leisure-time physical activity and social support among Brazilian adults. J. Phys. Act. Health 2013, 10, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, G.; Cheng, L.A.; Melo, E.N.; de Farias Junior, J.C. Physical activity and social support in adolescents: A systematic review. Health Educ. Res. 2014, 29, 822–839. [Google Scholar] [CrossRef]
- Liang, D. Stress levels of students in higher education and their relationship with physical activity. Chin. J. Ment. Health 1994, 8, 5–6. [Google Scholar]
- Zhang, J.; Wu, Z.; Fang, G.; Li, J.; Han, B.; Chen, Z. Establishment of a national urban norm for the Flow Survey Center Depression Scale. Chin. J. Ment. Health 2010, 24, 139–143. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. J. Weinman S. Wright M. Johnston Meas. Health Psychol. A User’s Portfolio. Causal Control. Beliefs 2012, 35, 37. [Google Scholar] [CrossRef]
- Xiao, S. Theoretical foundations and research applications of the Social Support Rating Scale. J. Clin. Psychiatry 1994, 4, 98–100. [Google Scholar]
- Davison, A.C.; Hinkley, D.V. Bootstrap Methods and Their Application; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; Sage: New York, NY, USA, 1991. [Google Scholar]
- Chengdu Municipal Health Commission. The Latest Version! «The Guide to Prevention and Control of New Coronary Pneumonia Epidemic in Sichuan Province (Sixth Edition)» Is Here. Available online: http://cdwjw.chengdu.gov.cn/cdwjw/c135633/2022-07/09/content_2d0093e5a6304e549e2f1ef36f6744ca.shtml (accessed on 3 January 2023).
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Zhao, X.S.; Lynch, J.G.; Chen, Q.M. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Moore, K.A.; Babyak, M.A.; Wood, C.E.; Napolitano, M.A.; Khatri, P.; Craighead, W.E.; Herman, S.; Krishnan, R.; Blumenthal, J.A. The Association between Physical Activity and Depression in Older Depressed Adults. J. Aging Phys. Act. 1999, 7, 55–61. [Google Scholar] [CrossRef]
- Kritz-Silverstein, D.; Barrett-Connor, E.; Corbeau, C. Cross-sectional and prospective study of exercise and depressed mood in the elderly: The Rancho Bernardo study. Am. J. Epidemiol. 2001, 153, 596–603. [Google Scholar] [CrossRef]
- Lindwall, M.; Larsman, P.; Hagger, M.S. The reciprocal relationship between physical activity and depression in older European adults: A prospective cross-lagged panel design using SHARE data. Health Psychol. 2011, 30, 453–462. [Google Scholar] [CrossRef]
- Baran, J.; Kalandyk-Osinko, K.; Baran, R. Does Prenatal Physical Activity Affect the Occurrence of Postnatal Anxiety and Depression? Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 2284. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Rutland-Lawes, J.; Wallinheimo, A.S.; Evans, S.L. Risk factors for depression during the COVID-19 pandemic: A longitudinal study in middle-aged and older adults. BJPsych. Open 2021, 7, e161. [Google Scholar] [CrossRef]
- de Oliveira, L.; Souza, E.C.; Rodrigues, R.A.S.; Fett, C.A.; Piva, A.B. The effects of physical activity on anxiety, depression, and quality of life in elderly people living in the community. Trends Psychiatry Psychother. 2019, 41, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.R.; Park, J.H.; Park, H.Y. Analysis of Factors Affecting Depression in Older Adults in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 9887. [Google Scholar] [CrossRef]
- Zhang, S.; Xiang, K.; Li, S.; Pan, H.F. Physical activity and depression in older adults: The knowns and unknowns. Psychiatry Res. 2021, 297, 113738. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.; Thibodeaux, L.; Jiang, L.; Francis, K.; Hochhalter, A. Fit & strong! Promotes physical activity and well-being in older cancer survivors. Front. Public Health 2014, 2, 171. [Google Scholar] [CrossRef]
- Luberto, C.M.; Coey, C.A.; Davis, R.B.; Wayne, P.M.; Crute, S.; Yeh, G.Y. Exploring correlates of improved depression symptoms and quality of life following tai chi exercise for patients with heart failure. ESC Heart Fail. 2020, 7, 4206–4212. [Google Scholar] [CrossRef]
- White, K.; Kendrick, T.; Yardley, L. Change in self-esteem, self-efficacy and the mood dimensions of depression as potential mediators of the physical activity and depression relationship: Exploring the temporal relation of change. Ment. Health Phys. Act. 2009, 2, 44–52. [Google Scholar] [CrossRef]
- Barbour, K.A.; Blumenthal, J.A. Exercise training and depression in older adults. Neurobiol. Aging 2005, 26 (Suppl. 1), 119–123. [Google Scholar] [CrossRef]
- Singh, N.A.; Clements, K.M.; Singh, M.A. The efficacy of exercise as a long-term antidepressant in elderly subjects: A randomized, controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M497–M504. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef]
- Zach, S.; Fernandez-Rio, J.; Zeev, A.; Ophir, M.; Eilat-Adar, S. Physical activity, resilience, emotions, moods, and weight control, during the COVID-19 global crisis. Isr. J. Health Policy Res. 2021, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Gyasi, R.M. Social support, physical activity and psychological distress among community-dwelling older Ghanaians. Arch. Gerontol. Geriatr. 2019, 81, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Lage, A.; Carrapatoso, S.; Sampaio de Queiroz Neto, E.; Gomes, S.; Soares-Miranda, L.; Bohn, L. Associations Between Depressive Symptoms and Physical Activity Intensity in an Older Adult Population During COVID-19 Lockdown. Front. Psychol. 2021, 12, 644106. [Google Scholar] [CrossRef] [PubMed]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2020, 18, 210. [Google Scholar] [CrossRef]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Alston, M.; Guo, W. The influence of social support on loneliness and depression among older elderly people in China: Coping styles as mediators. J. Community Psychol. 2019, 47, 1235–1245. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 490 | 50.308 |
| Female | 484 | 49.692 |
| Age | ||
| 60–64 | 303 | 31.109 |
| 65–69 | 274 | 28.131 |
| 70–74 | 229 | 23.511 |
| 75–79 | 94 | 9.651 |
| ≥80 | 74 | 7.598 |
| Education Level | ||
| No schooling | 174 | 17.864 |
| Primary school | 261 | 26.797 |
| Middle school | 206 | 21.15 |
| High school or technical secondary school | 167 | 17.146 |
| College (including higher vocational education) | 72 | 7.392 |
| Bachelor degree | 50 | 5.133 |
| Graduate and higher | 44 | 4.517 |
| Income (USD) | ||
| <2000 | 253 | 25.975 |
| 2000–3000 | 292 | 29.979 |
| 3000–4000 | 156 | 16.016 |
| 4000–5000 | 175 | 17.967 |
| >5000 | 98 | 10.062 |
| Health condition | ||
| Very Good | 438 | 44.969 |
| Good | 146 | 14.99 |
| Poor | 341 | 35.01 |
| Bad | 49 | 5.031 |
| Physical Activity | ||
| Low exercise levels | 422 | 43.326 |
| Moderate exercise levels | 302 | 31.006 |
| High exercise levels | 250 | 25.667 |
| Mental Depression | ||
| No depression | 394 | 40.452 |
| Suspected depression | 66 | 6.776 |
| Some degree of depression | 514 | 52.772 |
| Self-Efficacy | ||
| Low self-efficacy | 374 | 38.398 |
| Moderate self-efficacy | 346 | 35.524 |
| High self-efficacy | 254 | 26.078 |
| Social Support | ||
| Low social support | 152 | 15.606 |
| Moderate social support | 635 | 65.195 |
| High social support | 187 | 19.199 |
| Dimension | Items | Parameters of Significant Test | SMC | CR | AVE | |||
|---|---|---|---|---|---|---|---|---|
| Estimate | S.E. | C.R. | p-Value | |||||
| PA | Frequency | 0.746 | 0.019 | 39.263 | *** | 0.557 | 0.798 | 0.568 |
| Time | 0.764 | 0.019 | 40.211 | *** | 0.584 | |||
| Intensity | 0.750 | 0.018 | 41.667 | *** | 0.562 | |||
| Depression | Depression1 | 0.700 | 0.015 | 46.667 | *** | 0.490 | 0.952 | 0.501 |
| Depression2 | 0.693 | 0.015 | 46.200 | *** | 0.480 | |||
| Depression3 | 0.713 | 0.015 | 47.533 | *** | 0.508 | |||
| Depression4 | 0.716 | 0.015 | 47.733 | *** | 0.512 | |||
| Depression5 | 0.700 | 0.014 | 50.000 | *** | 0.489 | |||
| Depression6 | 0.707 | 0.014 | 50.500 | *** | 0.500 | |||
| Depression7 | 0.688 | 0.015 | 45.867 | *** | 0.473 | |||
| Depression8 | 0.732 | 0.014 | 52.286 | *** | 0.535 | |||
| Depression9 | 0.714 | 0.014 | 51.000 | *** | 0.510 | |||
| Depression10 | 0.726 | 0.014 | 51.857 | *** | 0.527 | |||
| Depression 11 | 0.718 | 0.014 | 51.286 | *** | 0.515 | |||
| Depression 12 | 0.720 | 0.015 | 48.000 | *** | 0.518 | |||
| Depression 13 | 0.705 | 0.016 | 44.063 | *** | 0.497 | |||
| Depression 14 | 0.689 | 0.016 | 43.063 | *** | 0.474 | |||
| Depression 15 | 0.715 | 0.014 | 51.071 | *** | 0.511 | |||
| Depression 16 | 0.729 | 0.013 | 56.077 | *** | 0.532 | |||
| Depression 17 | 0.689 | 0.014 | 49.214 | *** | 0.475 | |||
| Depression 18 | 0.695 | 0.015 | 46.333 | *** | 0.483 | |||
| Depression 19 | 0.693 | 0.015 | 46.200 | *** | 0.480 | |||
| Depression 20 | 0.707 | 0.015 | 47.133 | *** | 0.500 | |||
| SE | SE1 | 0.769 | 0.012 | 64.083 | *** | 0.591 | 0.934 | 0.585 |
| SE2 | 0.761 | 0.013 | 58.538 | *** | 0.579 | |||
| SE3 | 0.768 | 0.012 | 64.000 | *** | 0.589 | |||
| SE4 | 0.767 | 0.013 | 59.000 | *** | 0.588 | |||
| SE5 | 0.770 | 0.012 | 64.167 | *** | 0.593 | |||
| SE6 | 0.756 | 0.013 | 58.154 | *** | 0.571 | |||
| SE7 | 0.750 | 0.014 | 53.571 | *** | 0.562 | |||
| SE8 | 0.776 | 0.012 | 64.667 | *** | 0.603 | |||
| SE9 | 0.765 | 0.013 | 58.846 | *** | 0.586 | |||
| SE10 | 0.765 | 0.012 | 63.750 | *** | 0.585 | |||
| SS | US | 0.859 | 0.016 | 53.688 | *** | 0.738 | 0.843 | 0.646 |
| SUS | 0.882 | 0.019 | 46.421 | *** | 0.779 | |||
| OS | 0.649 | 0.022 | 29.500 | *** | 0.421 | |||
| χ2 | df | χ2/df | P | GFI | AGFI | CFI | NFI | IFI | RMSEA | |
|---|---|---|---|---|---|---|---|---|---|---|
| Model | 730.005 | 588 | 1.242 | 0.000 | 0.960 | 0.955 | 0.993 | 0.964 | 0.993 | 0.016 |
| Variable | M | S.D. | PA | Depression | SE | SS |
|---|---|---|---|---|---|---|
| PA | 29.24 | 22.702 | 0.753 | |||
| Depression | 42.98 | 13.156 | −0.649 *** | 0.708 | ||
| SE | 24.57 | 7.392 | 0.551 *** | −0.485 *** | 0.765 | |
| SS | 34.06 | 10.376 | 0.233 *** | −0.081 *** | 0.199 *** | 0.804 |
| χ2 | df | χ2/df | P | GFI | AGFI | CFI | NFI | IFI | RMSEA | |
|---|---|---|---|---|---|---|---|---|---|---|
| Model | 571.176 | 492 | 1.161 | 0.008 | 0.966 | 0.961 | 0.998 | 0.969 | 0.996 | 0.013 |
| Path | Estimate | S.E. | Z | Bootstrapping | ||||
|---|---|---|---|---|---|---|---|---|
| Bias-Corrected | Percentile | |||||||
| Lower | Upper | Lower | Upper | |||||
| Indirect effect | PA → SE → Depression | −0.101 | 0.023 | −4.391 | −0.149 | −0.058 | −0.147 | −0.057 |
| Direct effect | PA → Depression | −0.548 | 0.046 | −11.913 | −0.638 | −0.461 | −0.638 | −0.461 |
| Total effect | PA → Depression | −0.649 | 0.034 | −19.088 | −0.716 | −0.583 | −0.714 | −0.581 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| β | T | β | T | β | T | |
| Constants | - | 24.306 ** | - | 24.289 ** | - | 25.725 ** |
| Gender | 0.006 | 0.23 | 0.009 | 0.318 | 0.015 | 0.552 |
| Age | −0.014 | −0.494 | −0.015 | −0.563 | −0.02 | −0.775 |
| Education | 0.016 | 0.585 | 0.017 | 0.618 | 0.016 | 0.604 |
| Income | −0.027 | −0.965 | −0.027 | −0.981 | −0.04 | −1.515 |
| Health condition | −0.013 | −0.464 | −0.011 | −0.39 | 0.001 | 0.034 |
| PA | −0.519 | −18.866 ** | −0.537 | −18.803 ** | −0.449 | −15.442 ** |
| SS | 0.067 | 2.331 * | 0.074 | 2.618 ** | ||
| PA×SS | −0.258 | −9.144 ** | ||||
| R2 | 0.27 | 0.274 | 0.332 | |||
| Adjusted R2 | 0.266 | 0.269 | 0.327 | |||
| F-value | F (6967) = 56.690, p = 0.000 | F (7966) = 52.174, p = 0.000 | F (8965) = 60.008, p = 0.000 | |||
| ΔR2 | 0.27 | 0.004 | 0.058 | |||
| ΔF value | F (6967) = 56.690, p = 0.000 | F (1966) = 5.435, p = 0.020 | F (1965) = 83.613, p = 0.000 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, G.; Wang, C.; Ma, X. The Relationship between Physical Activity and Mental Depression in Older Adults during the Prevention and Control of COVID-19: A Mixed Model with Mediating and Moderating Effects. Int. J. Environ. Res. Public Health 2023, 20, 3225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043225
Xiong G, Wang C, Ma X. The Relationship between Physical Activity and Mental Depression in Older Adults during the Prevention and Control of COVID-19: A Mixed Model with Mediating and Moderating Effects. International Journal of Environmental Research and Public Health. 2023; 20(4):3225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043225
Chicago/Turabian StyleXiong, Guoyan, Caixia Wang, and Xiujie Ma. 2023. "The Relationship between Physical Activity and Mental Depression in Older Adults during the Prevention and Control of COVID-19: A Mixed Model with Mediating and Moderating Effects" International Journal of Environmental Research and Public Health 20, no. 4: 3225. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043225