
SPACEE Protocol: “Spiritual Care Competence” in PAlliative Care Education and PracticE: Mixed-Methods Research in the Development of Iberian Guidelines
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
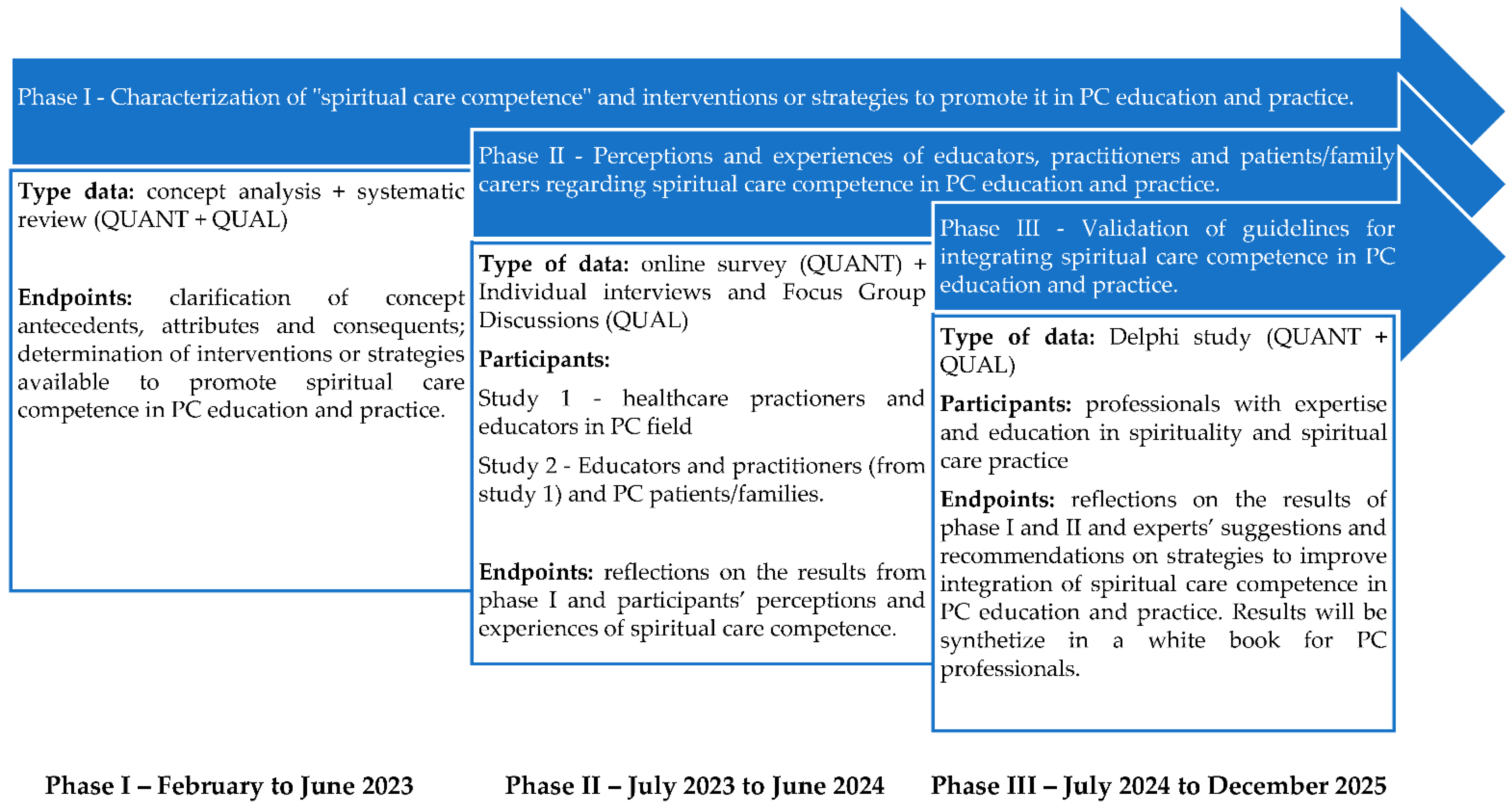
2.1. Study Overview
2.1.1. Phase I
Purpose
Procedures
- Task 1: Concept analysis on “Spiritual Care Competence” in PC.
- Task 2: Systematic review.
2.1.2. Phase II
Purpose
Procedures
- Task 3a: Methodological Pilot Study
- Task 3b: A multicenter, quantitative descriptive cross-sectional survey.
- Task 4: A multisite, descriptive, and contextual qualitative study.
2.1.3. Phase III
Purpose
Procedures
- Task 5: A multi-phase modified Delphi method
- Task 6: White Book
2.2. Ethical Considerations
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Binder, P.E. Suffering a Healthy Life—On the Existential Dimension of Health. Front. Psychol. 2022, 13, 803792. [Google Scholar] [CrossRef] [PubMed]
- Hartogh, G.D. Suffering and dying well: On the proper aim of palliative care. Med. Health Care Philos. 2017, 20, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siler, S.; Borneman, T.; Ferrell, B. Pain and Suffering. Semin. Oncol. Nurs. 2019, 35, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Rocca, E.; Anjum, R.L. Complexity, Reductionism and the Biomedical Model. In Rethinking Causality, Complexity and Evidence for the Unique Patient; Anjum, R., Copeland, S., Rocca, E., Eds.; Springer: Cham, Switzerland, 2020; pp. 75–94. [Google Scholar]
- Benito, E.; Dones, M.; Barbero, J. El acompañamiento espiritual en cuidados paliativos. Psicooncologia 2017, 13, 367–384. [Google Scholar] [CrossRef] [Green Version]
- Soto-Rubio, A.; Perez-Marin, M.; Tomas Miguel, J.; Barreto Martin, P. Emotional Distress of Patients at End-of-Life and Their Caregivers: Interrelation and Predictors. Front. Psychol. 2018, 9, 2199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Søvold, L.E.; Naslund, J.A.; Kousoulis, A.A.; Saxena, S.; Qoronfleh, M.W.; Grobler, C.; Münter, L. Prioritizing the Mental Health and Well-Being of Healthcare Workers: An Urgent Global Public Health Priority. Front. Public Health 2021, 9, 679397. [Google Scholar] [CrossRef] [PubMed]
- Dones Sánchez, M.; Bimbaum, N.C.; Barbero Gutierrez, J.; Bofill, C.; Balbuena Mora-Figueroa, P.; Benito, E. How professionals perceive spiritual care in palliative care teams in Spain? Med. Paliativa 2016, 23, 63–71. [Google Scholar] [CrossRef]
- Best, M.; Leget, C.; Goodhead, A.; Paal, P. An EAPC white paper on multi-disciplinary education for spiritual care in palliative care. BMC Palliat. Care 2020, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.F.; Paal, P.; Symons, X.; Best, M.C. The Content, Teaching Methods and Effectiveness of Spiritual Care Training for Healthcare Professionals: A Mixed-Methods Systematic Review. J. Pain Symptom Manag. 2021, 62, e261–e278. [Google Scholar] [CrossRef]
- Van Leeuwen, R.; Schep-Akkerman, A. Nurses’ perceptions of spirituality and spiritual Care in Different Health Care Settings in the Netherlands. Religions 2015, 6, 1346–1357. [Google Scholar] [CrossRef]
- Cooper, K.L.; Chang, E.; Luck, L.; Dixon, K. How Nurses Understand Spirituality and Spiritual Care: A Critical Synthesis. J. Holist. Nurs. 2020, 38, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Gijsberts, M.H.E.; Liefbroer, A.I.; Otten, R.; Olsman, E. Spiritual Care in Palliative Care: A Systematic Review of the Recent European Literature. Med. Sci. 2019, 7, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atarhim, M.A.; Lee, S.; Copnell, B. An Exploratory Study of Spirituality and Spiritual Care Among Malaysian Nurses. J. Relig. Health 2019, 58, 180–194. [Google Scholar] [CrossRef] [PubMed]
- García-Navarro, E.B.; Medina-Ortega, A.; García Navarro, S. Spirituality in Patients at the End of Life-Is It Necessary? A Qualitative Approach to the Protagonists. Int. J. Environ. Res. Public Health 2021, 19, 227. [Google Scholar] [CrossRef] [PubMed]
- Laranjeira, C.; Querido, A.; Charepe, Z.; Dixe, M.A. Hope-based interventions in chronic disease: An integrative review in the light of Nightingale. Rev. Bras. Enferm. 2020, 73 (Suppl. S5), e20200283. [Google Scholar] [CrossRef] [PubMed]
- Laranjeira, C.; Baptista Peixoto Befecadu, F.; Da Rocha Rodrigues, M.G.; Larkin, P.; Pautex, S.; Dixe, M.A.; Querido, A. Exercising Hope in Palliative Care Is Celebrating Spirituality: Lessons and Challenges in Times of Pandemic. Front. Psychol. 2022, 13, 933767. [Google Scholar] [CrossRef]
- Yildirim, J.G.; Ertem, M. Professional quality of life and perceptions of spirituality and spiritual care among nurses: Relationship and affecting factors. Perspect. Psychiatr. Care 2022, 58, 438–447. [Google Scholar] [CrossRef]
- SECPAL. Espiritualidad en Clínica Una Propuesta de Evaluación y Acompañamiento Espiritual en Cuidados Paliativos; Benito, E., Barbero, J., Dones, M., Eds.; Punto Gráfico: Madrid, Spain, 2014; Available online: https://seor.es/wp-content/uploads/Monografia-secpal.pdf (accessed on 10 November 2022).
- Best, M.; Butow, P.; Olver, I. Doctors discussing religion and spirituality: A systematic literature review. Palliat. Med. 2016, 30, 327–337. [Google Scholar] [CrossRef]
- Bar-Sela, G.; Schultz, M.J.; Elshamy, K.; Rassouli, M.; Ben-Arye, E.; Doumit, M.; Gafer, N.; Albashayreh, A.; Ghrayeb, I.; Turker, I.; et al. Training for awareness of one’s own spirituality: A key factor in overcoming barriers to the provision of spiritual care to advanced cancer patients by doctors and nurses. Palliat. Support Care 2019, 17, 345–352. [Google Scholar] [CrossRef]
- Jones, K.F.; Pryor, J.; Care-Unger, C.; Simpson, G.K. Rehabilitation health professionals’ perceptions of spirituality and spiritual care: The results of an online survey. Neuro Rehabil. 2020, 46, 17–30. [Google Scholar] [CrossRef]
- Kang, K.A.; Chun, J.; Kim, H.Y.; Kim, H.Y. Hospice palliative care nurses’ perceptions of spiritual care and their spiritual care competence: A mixed-methods study. J. Clin. Nurs. 2021, 30, 961–974. [Google Scholar] [CrossRef] [PubMed]
- Balboni, M.; Sullivan, A.; Enzinger, A.; Epstein-Peterson, Z.; Tseng, Y.; Mitchell, C.; Niska, J.; Zollfrank, A.; VanderWeele, T.; Balboni, T. Nurse and physician barriers to spiritual care provision at the end of life. J. Pain Symptom Manag. 2014, 48, 400–410. [Google Scholar] [CrossRef] [PubMed]
- McSherry, W.; Ross, L.; Attard, J.; van Leeuwen, R.; Giske, T.; Kleiven, T.; Boughey, A.; The EPICC Network. Preparing undergraduate nurses and midwives for spiritual care: Some developments in European education over the last decade. J. Study Spiritual. 2020, 10, 55–71. [Google Scholar] [CrossRef]
- Van Leeuwen, R.; Attard, J.; Ross, L.; Boughey, A.; Giske, T.; Kleiven, T.; McSherry, W. The development of a consensus-based spiritual care education standard for undergraduate nursing and midwifery students: An educational mixed methods study. J. Adv. Nurs. 2021, 77, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Rykkje, L.; Søvik, M.B.; Ross, L.; McSherry, W.; Cone, P.; Giske, T. Educational interventions and strategies for spiritual care in nursing and healthcare students and staff: A scoping review. J. Clin. Nurs. 2022, 31, 1440–1464. [Google Scholar] [CrossRef] [PubMed]
- Benito, E.; Oliver, A.; Galiana, L.; Barreto, P.; Pascual, A.; Gomis, C.; Barbero, J. Development and validation of a new tool for the assessment and spiritual care of palliative care patients. J. Pain Symptom Manag. 2014, 47, 1008–1018.e1. [Google Scholar] [CrossRef] [PubMed]
- Chahrour, W.H.; Hvidt, N.C.; Hvidt, E.A.; Viftrup, D.T. Learning to care for the spirit of dying patients: The impact of spiritual care training in a hospice-setting. BMC Palliat. Care 2021, 20, 115. [Google Scholar] [CrossRef] [PubMed]
- Guedes, A.; Carvalho, M.S.; Laranjeira, C.; Querido, A.; Charepe, Z. Hope in palliative care nursing: Concept analysis. Int. J. Palliat. Nurs. 2021, 27, 176–187. [Google Scholar] [CrossRef]
- Koper, I.; Pasman, H.R.W.; Schweitzer, B.P.M.; Kuin, A.; Onwuteaka-Philipsen, B.D. Spiritual care at the end of life in the primary care setting: Experiences from spiritual caregivers—A mixed methods study. BMC Palliat. Care 2019, 18, 98. [Google Scholar] [CrossRef] [PubMed]
- Fitch, M.I.; Bartlett, R. Patient Perspectives about Spirituality and Spiritual Care. Asia Pac. J. Oncol. Nurs. 2019, 6, 111–121. [Google Scholar] [CrossRef]
- Batstone, E.; Bailey, C.; Hallett, N. Spiritual care provision to end-of-life patients: A systematic literature review. J. Clin. Nurs. 2020, 29, 3609–3624. [Google Scholar] [CrossRef]
- Ghorbani, M.; Mohammadi, E.; Aghabozorgi, R.; Ramezani, M. Spiritual care interventions in nursing: An integrative literature review. Support. Care Cancer 2021, 29, 1165–1181. [Google Scholar] [CrossRef]
- Haufe, M.; Leget, C.; Potma, M.; Teunissen, S. How can existential or spiritual strengths be fostered in palliative care? An interpretative synthesis of recent literature. BMJ Support. Palliat. Care 2020, 371, bmjspcare-2020-002379. [Google Scholar] [CrossRef] [PubMed]
- Baldacchino, D. Spiritual Care Education of Health Care Professionals. Religions 2015, 6, 594–613. [Google Scholar] [CrossRef] [Green Version]
- Creswell, J.; Plano Clark, V. Designing and Conducting Mixed Methods Research, 3rd ed.; SAGE: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- O’Cathain, A.; Murphy, E.; Nicholl, J. Three techniques for integrating data in mixed methods studies. BMJ 2010, 341, c4587. [Google Scholar] [CrossRef]
- Paal, P.; Roser, T.; Frick, E. Developments in spiritual care education in German-speaking countries. BMC Med. Educ. 2014, 14, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, J.M. Analyzing and Conceptualizing the Theoretical Foundations of Nursing; Springer Publishing Company: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP Checklists. 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 10 November 2022).
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office, Industry Canada: Gatineau, QC, Canada, 2018.
- Creswell, J.W.; Plano Clark, V.L.; Gutmann, M.L.; Hanson, W.E. Advanced mixed methods research design. In Handbook of Mixed Methods in Social and Behavioral Research; Tashakkori, A., Teddlie, C., Eds.; SAGE: Thousand Oaks, CA, USA, 2003; pp. 209–240. [Google Scholar]
- Draucker, C.B.; Rawl, S.M.; Vode, E.; Carter-Harris, L. Integration Through Connecting in Explanatory Sequential Mixed Method Studies. West. J. Nurs. Res. 2020, 42, 1137–1147. [Google Scholar] [CrossRef]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving integration in mixed methods designs—Principles and practices. Health Serv. Res. 2013, 48 Pt 2, 2134–2156. [Google Scholar] [CrossRef] [Green Version]
- Fang, H.F.; Susanti, H.D.; Dlamini, L.P.; Miao, N.F.; Chung, M.H. Validity and reliability of the spiritual care competency scale for oncology nurses in Taiwan. BMC Palliat. Care 2022, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Abusafia, A.H.; Mamat, Z.; Rasudin, N.S.; Bakar, M.; Ismail, R. Spiritual care competence among Malaysian staff nurses. Nurse Media J. Nurs. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- International Test Commission. International Test Commission Guidelines for Translating and Adapting Tests, 2nd ed.; The International Test Commission: Hemel Hempstead, UK, 2017; Available online: http://www.intestcom.org (accessed on 10 November 2022).
- Tabachnick, B.; Fidell, L. Using Multivariate Statistics; Pearson Education Inc.: Boston, MA, USA, 2013. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Prev. Med. 2007, 45, 247–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, R.; Fisher, J. Domains of Spiritual Well-Being and Development and Validation of the Spiritual Well-Being Questionnaire. Pers. Individ. Dif. 2003, 35, 1975–1991. [Google Scholar] [CrossRef] [Green Version]
- Bugen, L. Coping: Effects of death education. Omega 1981, 11, 175–183. [Google Scholar] [CrossRef]
- McSherry, W.; Draper, P.; Kendrick, D. The construct validity of a rating scale designed to assess spirituality and spiritual care. Int. J. Nurs. Stud. 2002, 39, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R.; Tiesinga, L.J.; Middel, B.; Post, D.; Jochemsen, H. The validity and reliability of an instrument to assess nursing competencies in spiritual care. J. Clin. Nurs. 2009, 18, 2857–2869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Leeuwen, R.V.; Li, F. Psychometric properties of the Chinese version of the spiritual care competency scale in nursing practice: A methodological study. BMJ Open 2019, 9, e030497. [Google Scholar] [CrossRef]
- Sousa, F.N.; Costa, A.P.; Moreira, A. webQDA [Software]; Microio/Ludomedia: Aveiro, Portugal, 2019. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- McKenna, H.P. The Delphi technique: A worthwhile research approach for nursing? J. Adv. Nurs. 1994, 19, 1221–1225. [Google Scholar] [CrossRef] [PubMed]
- Knighting, K.; O’Brien, M.R.; Roe, B.; Gandy, R.; Lloyd-Williams, M.; Nolan, M.; Jack, B. Gaining consensus on family carer needs when caring for someone dying at home to develop the Carers’ Alert Thermometer (CAT): A modified Delphi study. J. Adv. Nurs. 2016, 72, 227–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demirsoy, N. Holistic Care Philosophy for Patient-Centered Approaches and Spirituality. In Patient-Centered Medicine; InTech: London, UK, 2017. [Google Scholar] [CrossRef]
- Vincensi, B.B. Interconnections: Spirituality, Spiritual Care, and Patient-Centered Care. Asia Pac. J. Oncol. Nurs. 2019, 6, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E. Competences in spiritual care education and training. In Oxford Textbook of Spirituality in Healthcare; Cobb, M.R., Puchalski, C.M., Rumbold, B., Eds.; Academic: Oxford, UK, 2012; pp. 435–442. [Google Scholar]


{kind=link}
| Step 1 | Two independent translators (familiar with both languages and the instrument’s aims) create two separate forward translations of the tool |
| Step 2 | Reconciliation into single translation by project leader |
| Step 3 | Back-translation into source language by two independent translators with proficiency in both languages |
| Step 4 | A panel composed of 6 experts (practitioners, educators, researchers, subject area experts, and a tool validation expert) review the process and validate the final version in the target language |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laranjeira, C.; Benito, E.; Dixe, M.A.; Dones, M.; Specos, M.; Querido, A. SPACEE Protocol: “Spiritual Care Competence” in PAlliative Care Education and PracticE: Mixed-Methods Research in the Development of Iberian Guidelines. Int. J. Environ. Res. Public Health 2023, 20, 3505. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043505
Laranjeira C, Benito E, Dixe MA, Dones M, Specos M, Querido A. SPACEE Protocol: “Spiritual Care Competence” in PAlliative Care Education and PracticE: Mixed-Methods Research in the Development of Iberian Guidelines. International Journal of Environmental Research and Public Health. 2023; 20(4):3505. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043505
Chicago/Turabian StyleLaranjeira, Carlos, Enric Benito, Maria Anjos Dixe, Monica Dones, Marcela Specos, and Ana Querido. 2023. "SPACEE Protocol: “Spiritual Care Competence” in PAlliative Care Education and PracticE: Mixed-Methods Research in the Development of Iberian Guidelines" International Journal of Environmental Research and Public Health 20, no. 4: 3505. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20043505