

Multidimensional Results and Reflections on CAR-T: The Italian Evidence
 , , , , , and
, , , , , and
Abstract
:1. Introduction
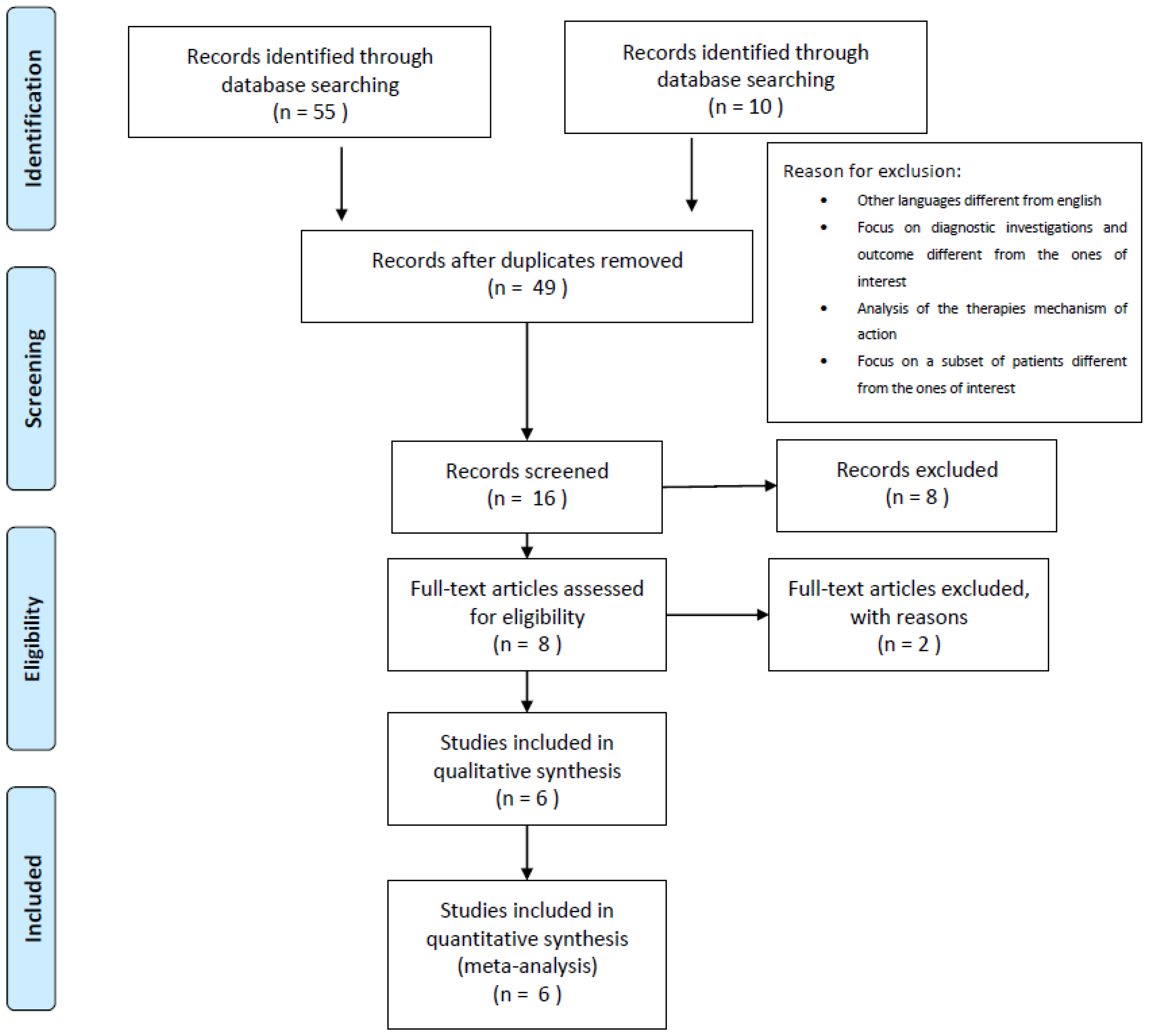
2. Materials and Methods
- (i)
- P (population): Patients affected by diffuse large B-cell lymphoma (DLBCL) in third-line therapy.
- (ii)
- I (intervention): CAR T-cell therapy.
- (iii)
- C (comparator): Chemotherapy—immunotherapy, Best Alternative Care, also defined as Best Salvage Care [5].
- (iv)
- O (outcome): Efficacy (OS and progression-free survival, PFS), safety (neurological adverse events and cytokine release syndrome), and related management costs.
- The cost of CAR-T therapy for the two drugs approved by the Italian Medicines Agency (AIFA) and currently used in the Italian market, for which AIFA have established “the payment by results mechanism” (i.e., the reimbursement of drug is related to the health results achieved), was referred to. For tisagenlecleucel, an initial payment equal to 30% is due at the infusion phase, whereas the remaining payment is due on the achievement of a successful and effective patient outcome (in particular, 35% at 6 months and 35% at 12 months). In contrast, a 50% reimbursement is due for axicabtagene ciloleucel at 6 months on achieving a successful and effective patient outcome. The remaining value is then reimbursed at 9 and 12 months, for 40% and 10% shares, respectively.
- The difference in the costs of CAR-T cells also emerged in the conservation phase. Tisagenlecleucel required a cryopreservation process, carried out by the hospital, while the collection and delivery costs related to the management of axicabtagene ciloleucel are supported by the manufacturer.
- CAR T-cell administration requires hospitalization of the patient. The economic evaluation considered the cost of hospitalization per day as EUR 1,875, and an overall length of stay equal to 15 days on average (analyzing gathered data, in line with literature evidence), for the management of patient monitoring and the infusion phase of the protocol for CAR-T treatment.
- BSC treatments, considered alternative therapeutic options, comprised the most common salvage therapy, excluding experimental protocols. In this specific setting, the most used therapeutic strategies are R-DHAX (rituximab, dexamethasone, cytarabine and oxaliplatin), R-GDP (rituximab, gemcitabine, dexamethasone, cisplatin, or carboplatin) and rituximab-bendamustine.
- Home palliative care and hospice care were included in the economic evaluation of BSC treatment.
3. Results
3.1. Results from the Literature Review
3.2. Results from the Economic Evaluation
3.3. Results from the Organizational Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freedman, A.; Friedberg, J. Patient Education: Diffuse Large B Cell Lymphoma in Adults (Beyond the Basics); Mac Master University: Hamilton, ON, Canada, 2022. [Google Scholar]
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2021, 384, 842–858. [Google Scholar] [CrossRef]
- Susanibar-Adaniya, S.; Barta, S.K. Update on Diffuse large B cell lymphoma: A review of current data and potential applications on risk stratification and management. Am. J. Hematol. 2021, 96, 617–629. [Google Scholar] [CrossRef]
- Dahi, P.B.; Moskowitz, C.H.; Giralt, S.A.; Lazarus, H.M. Novel agents may positively impact chemotherapy and transplantation in subsets of diffuse large B-cell lymphoma. Expert Rev. Hematol. 2019, 12, 407–418. [Google Scholar] [CrossRef]
- Crump, M.; Neelapu, S.S.; Farooq, U.; Van Den Neste, E.; Kuruvilla, J.; Westin, J.; Link, B.K.; Hay, A.; Cerhan, J.R.; Zhu, L.; et al. Outcomes in refractory diffuse large B-cell lymphoma: Results from the international SCHOLAR-1 study. Blood 2017, 130, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Sarkozy, C.; Sehn, L.H. Management of relapsed/refractory DLBCL. Best Pract. Res. Clin. Haematol. 2018, 31, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Kockenderfer, J.; Dudley, M.E.; Kassim, S.H.; Somerville, R.P.T.; Carpenter, R.O.; Stetler-Stevenson, M.; Yang, J.C.; Phan, G.Q.; Hughes, M.S.; Sherry, R.M.; et al. Chemotherapy-Refractory Diffuse Large B-Cell Lymphoma and Indolent B-Cell Malignancies Can Be Effectively Treated With Autologous T Cells Expressing an Anti-CD19 Chimeric Antigen Receptor. J. Clin. Oncol. 2015, 33, 540–549. [Google Scholar] [CrossRef] [Green Version]
- June, C.H.; Sadelain, M. Chimeric antigen receptor therapy. N. Engl. J. Med. 2018, 379, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): A multicentre seamless design study. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Charrot, S.; Hallam, S. CAR-T Cells: Future Perspectives. Hemasphere 2019, 3, e188. [Google Scholar] [CrossRef] [PubMed]
- Makita, S.; Imaizumi, K.; Kurosawa, S.; Tobinai, K. Chimeric antigen receptor T-cell therapy for B-cell non-Hodgkin lymphoma: Opportunities and challenges. Drugs Context 2019, 8, 212567. [Google Scholar] [CrossRef]
- Lyman, G.H.; Nguyen, A.; Snyder, S.; Gitlin, M.; Chung, K.C. Economic Evaluation of Chimeric Antigen Receptor T-Cell Therapy by Site of Care Among Patients with Relapsed or Refractory Large B-Cell Lymphoma. JAMA Netw. Open 2020, 3, e202072. [Google Scholar] [CrossRef]
- Heine, R.; Thielen, F.W.; Koopmanschap, M.; Kersten, M.J.; Einsele, H.; Jaeger, U.; Sonneveld, P.; Sierra, J.; Smand, C.; Uyl-de Groot, C.A. Health Economic Aspects of Chimeric Antigen Receptor T-cell Therapies for Haematological Cancers: Present and Future. Hemasphere 2021, 5, e524. [Google Scholar] [CrossRef]
- Kron, F.; Franz, J.; Kron, A.; Hallek, M. Ökonomie und Management bei der CAR-T-Zell-Therapie: Status quo und Ausblick [Economics and management of CAR T-cell therapy: Status quo and future perspectives]. Internist 2021, 62, 620–626. [Google Scholar] [CrossRef]
- Raimond, V.; Kaltenbach, E.; Adam, C.; Lazzarotto, S.; Le Galès, C.; Perrier, L.; Wittwer, J. Challenges raised by the economic evaluation of CAR-T-cell therapies. The review by the French National Authority for Health. Bull. Cancer 2021, 108, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Pagani, R.; Porazzi, E.; Manzini, R.; Lazzarotti, V.; Lettieri, E.; Foglia, E.; Ferrario, L.; Garagiola, E.; Masella, C. Assessing Innovative Healthcare Technologies in Hospitals: Lessons Learnt from an Empirical Experiment. In Proceedings of the RnD Management Conference, Pisa, Italy, 23–26 June 2015. [Google Scholar]
- Ghorashian, S.; Malard, F.; Yüksel, M.K.; Mauff, K.; Hoogenboom, J.D.; Urbano-Ispizua, A.; Kuball, J.; de la Camara, R.; Ljungman, P.; Ruggeri, A.; et al. Defining the impact of SARS-CoV-2 on delivery of CAR T-cell therapy in Europe: A retrospective survey from the CTIWP of the EBMT. Bone Marrow Transpl. 2022, 57, 299–301. [Google Scholar] [CrossRef]
- Hu, Y.; Yin, E.T.S.; Yang, Y.; Wu, H.; Wei, G.; Su, J.; Cui, Q.; Jin, A.; Yang, L.; Fu, S.; et al. CAR T-cell treatment during the COVID-19 pandemic: Management strategies and challenges. Curr. Res. Transl. Med. 2020, 68, 111–118. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for peer-reviewed journals: Secrets of the trade. J. Chiropratic. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernardo, W.M.; Nobre, M.R.; Jatene, F.B. Evidence based clinical practice. Part II—Searching evidence databases [Article in Portuguese]. Rev. Assoc. Med. Bras. 2004, 50, 104–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EUNetHTA. The HTA Core Model, Version 3.0. Available online: https://www.eunethta.eu/hta-core-model/ (accessed on 13 November 2022).
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improv searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carrol, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Kaplan, R.S. Activity-based systems: Measuring the costs of resource usage. Account. Horiz. 1992, 6, 1–13. [Google Scholar]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, S.D.; Mauskopf, J.A.; Augustovski, F.; Jaime Caro, J.; Lee, K.M.; Minchin, M.; Orlewska, E.; Penna, P.; Rodriguez Barrios, J.M.; Shau, W.Y. Budget impact analysis-principles of good practice: Report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health 2014, 17, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitzinger, J. Qualitative research: Introducing focus groups. BMJ 1995, 311, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Berg, B. Qualitative Research Methods for the Social Sciences; Allyn & Bacon: Boston, MA, USA, 2009; pp. 101–157. [Google Scholar]
- Jansen, H. The Logic of Qualitative Survey Research and its Position in the Field of Social Research Methods. Forum Qual. Soz./Forum Qual. Soc. Res. 2010, 11. [Google Scholar] [CrossRef]
- Locke, F.L.; Neelapu, S.S.; Bartlett, N.L.; Siddiqi, T.; Chavez, J.C.; Hosing, C.M.; Ghobadi, A.; Budde, L.E.; Bot, A.; Rossi, J.M.; et al. Phase 1 Results of ZUMA-1: A Multicenter Study of KTE-C19 Anti-CD19 CAR T Cell Therapy in Refractory Aggressive Lymphoma. Mol. Ther. 2017, 25, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Chavez, J.C.; Bachmeier, C.; Kharfan-Dabaja, M.A. CAR T-cell therapy for B-cell lymphomas: Clinical trial results of available products. Ther. Adv. Hematol. 2019, 10, 2040620719841581. [Google Scholar] [CrossRef] [Green Version]
- Arcari, A.; Chiappella, A.; Spina, M.; Zanlari, L.; Bernuzzi, P.; Valenti, V.; Tani, M.; Marasca, R.; Cabras, M.G.; Zambello, R.; et al. Safety and efficacy of rituximab plus bendamustine in relapsed or refractory diffuse large B-cell lymphoma patients: An Italian retrospective multicenter study. Leuk Lymphoma 2016, 57, 1823–1830. [Google Scholar] [CrossRef] [PubMed]
- Barton, S.; Hawkes, E.A.; Cunningham, D.; Peckitt, C.; Chua, S.; Wotherspoon, A.; Attygalle, A.; Horwich, A.; Potter, M.; Ethell, M.; et al. Rituximab, Gemcitabine, Cisplatin and Methylprednisolone (R-GEM-P) is an effective regimen in relapsed diffuse large B-cell lymphoma. Eur. J. Haematol. 2015, 94, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ribera Santasusana, J.M.; de Andrés Saldaña, A.; García-Muñoz, N.; Gostkorzewicz, J.; Martínez Llinàs, D.; Díaz de Heredia, C. Cost-Effectiveness Analysis of Tisagenlecleucel in the Treatment of Relapsed or Refractory B-Cell Acute Lymphoblastic Leukaemia in Children and Young Adults in Spain. Clin. Outcomes Res. 2020, 12, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Petrou, P. Is it a Chimera? A systematic review of the economic evaluations of CAR-T cell therapy. Expert Rev. Pharm. Outcomes Res. 2019, 19, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Foglia, E.; Garagiola, E.; Ferrario, L.; Ladisa, V.; Scorza, A.; Rambaldi, A.; Cairoli, R.; Medaglia, M.; Sammassimo, S.; Omodeo Salè, E.; et al. New insights from CAR-T: An economic and organizational perspective. Value Health 2020, 23 (Suppl. 2), S430. [Google Scholar] [CrossRef]
- Croce, D.; Foglia, E.; Garagiola, E. Capitolo 2: Definizione della tariffa di rimborso del percorso CAR-T: Evidenze economiche e di sostenibilità. In CAR-T Innovazione, Valore e Sostenibilità Della Terapia, I Quaderni di Medicina, Il Sole 24 Ore; Cosentino, R., Ed.; Siemens Healthineers: Erlangen, Germany, 2021; p. 11. Available online: https://www.siemens-healthineers.com/it/news-and-events/quaderno-digitale-sole-24 (accessed on 16 February 2023).
- Borgert, R. Improving outcomes and mitigating costs associated with CAR T-cell therapy. Am. J. Manag. Care 2021, 27 (Suppl. 13), S253–S261. [Google Scholar]
- Fiorenza, S.; Ritchie, D.S.; Ramsey, S.D.; Turtle, C.J.; Roth, J.A. Value and affordability of CAR T-cell therapy in the United States. Bone Marrow Transpl. 2020, 55, 1706–1715. [Google Scholar] [CrossRef]
- Lin, J.K.; Muffly, L.S.; Spinner, M.A.; Barnes, J.I.; Owens, D.K.; Goldhaber-Fiebert, J.D. Cost Effectiveness of Chimeric Antigen Receptor T-Cell Therapy in Multiply Relapsed or Refractory Adult Large B-Cell Lymphoma. J. Clin. Oncol. 2019, 37, 2105–2119. [Google Scholar] [CrossRef]


{kind=link}
| CAR-T | BSC | |||||
|---|---|---|---|---|---|---|
| Chavez et al. (2019) [34] | Locke et al. (2017) [33] | Neelapu et al. (2017) [9] | Barton et al. (2014) [36] | Crump et al. (2017) [5] | Arcari et al. (2016) [35] | |
| Overall Survival (12 months) | 49% | 59% | 67% | 50% | 28% | 10.8 months |
| Progression-Free Survival (12 months) | 66% | 44% | 42% | 28% | - | 8.8 months |
| Adverse Event Incidence Rates | Reference | Economic Evaluation of the Adverse Events [EUR] | |
|---|---|---|---|
| Cytokine Release Syndrome | |||
| Pyrexia | 86% | Locke et al., 2017 [33] | EUR 232.97 |
| Hypotension | 71% | Locke et al., 2017 [33] | EUR 963.00 |
| Tachycardia | 43% | Locke et al., 2017 [33] | EUR 124.59 |
| Acute kidney injury | 29% | Locke et al., 2017 [33] | EUR 5167.40 |
| Cardiac failure | 14% | Locke et al., 2017 [33] | EUR 4700.00 |
| Metabolic acidosis | 14% | Locke et al., 2017 [33] | EUR 774.97 |
| Hyponatremia | 14% | Locke et al., 2017 [33] | EUR 774.97 |
| Dyspnea | 21% | Locke et al., 2017 [33] | EUR 1484.00 |
| Infection | 14% | Locke et al., 2017 [33] | EUR 447.97 |
| Immune effector cell-associated neurotoxicity syndrome | |||
| Headache | 14% | Locke et al., 2017 [33] | EUR 20.07 |
| Hypoxia | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Encephalopathy | 37% | Locke et al., 2017 [33] | EUR 2077.00 |
| Tremor | 31% | Locke et al., 2017 [33] | EUR 709.38 |
| Agitation | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Aphasia | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Delirium | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Dizziness | 14% | Locke et al., 2017 [33] | EUR 113.31 |
| Hallucination | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Restlessness | 14% | Locke et al., 2017 [33] | EUR 709.38 |
| Nausea | 58% | Locke et al., 2017 [33] | EUR 296.28 |
| Vomiting | 34% | Locke et al., 2017 [33] | EUR 52.74 |
| Constipation | 30% | Locke et al., 2017 [33] | EUR 153.96 |
| Confused state | 27% | Locke et al., 2017 [33] | EUR 709.38 |
| Haematological events | |||
| Anemia | 68% | Neelapu et al., 2017 [9] | EUR 23,625.51 |
| Thrombocytopenia | 35% | Neelapu et al., 2017 [9] | |
| Decreased neutrophil count | 33% | Locke et al., 2017 [33] | |
| Decreased platelet count | 30% | Locke et al., 2017 [33] | |
| Increased alanine aminotransferase | 20% | Locke et al., 2017 [33] | |
| Decreased lymphocyte count | 20% | Locke et al., 2017 [33] | |
| Leucopenia | 19% | Locke et al., 2017 [33] | |
| Adverse Event Incidence Rates | Reference | Economic Evaluation of the Adverse Events [EUR] | |
|---|---|---|---|
| Neutropenia | 60% 64% | Arcari et al., 2016 [35] Barton et al., 2015 [36] | EUR 1678.90 |
| Anemia | 45% | Arcari et al., 2016 [35] | EUR 7320.93 |
| Thrombocytopenia | 29% 69% | Arcari et al., 2016 [35] Barton et al., 2015 [36] | EUR 1349.00 |
| Infection | 27% | Arcari et al., 2016 [35] | EUR 447.97 |
| Nausea | 25% | Arcari et al., 2016 [35] | EUR 106.74 |
| Anorexia | 18% | Arcari et al., 2016 [35] | EUR 22.50 |
| Fatigue | 5% | Arcari et al., 2016 [35] | EUR 22.50 |
| Diarrhea | 4% | Arcari et al., 2016 [35] | EUR 153.96 |
| Maculopapular rash | 9% | Arcari et al., 2016 [35] | EUR 132.12 |
| Dehydration | 4% | Arcari et al., 2016 [35] | EUR 22.50 |
| Squamous cell carcinoma of the skin | 4% | Arcari et al., 2016 [35] | EUR 204.33 |
| Process Mapping and Economic Evaluation of CAR-T Treatment | Mean Cost per Patient [EUR] |
|---|---|
| Procedures and controls cryo-conservation | 361.00 EUR |
| CAR-T therapy | 232,772.55 EUR |
| PET (Positron-Emission Tomography) | 1081.86 EUR |
| Lymphodepleting chemotherapy | 650.58 EUR |
| Lymphocyte collection + CAR-T infusion + observation in hospital | 27,185.91 EUR |
| Neurotoxicity and cytokine release toxicity and Tocilizumab use | 41,580.50 EUR |
| Total with CAR-T treatment | 303,632.40 EUR |
| Total without CAR-T treatment costs | 71,220.84 EUR |
| Process Mapping and Economic Evaluation of BSC Treatment | Mean Cost per Patient [EUR] |
| PET (Positron-Emission Tomography) | EUR 1081.86 |
| Lymphodepleting chemotherapy | EUR 1971.26 |
| Salvage chemotherapy | EUR 17,500.00 |
| Adverse events | EUR 5176.28 |
| Hospitalization in hospice and home palliative care (on average 20 days) | EUR 3682.00 |
| Total BSC treatment | EUR 29,558.41 |
| I year | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 12,453,917.20 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 53,769,548.98 EUR | 332% | |
| Innovative Scenario 2 (individuals over 26 years old) | 49,350,521.33 EUR | 296% | |
| II year | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 12,310,871.42 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 52,561,627.69 EUR | 327% | |
| Innovative Scenario 2 (individuals over 26 years old) | 49,374,005.83 EUR | 301% | |
| III year | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 12,253,833.80 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 52,318,055.43 EUR | 327% | |
| Innovative Scenario 2 (individuals over 26 years old) | 49,145,289.79 EUR | 301% | |
| Total | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 37,018,621.41 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 158,649,230.60 EUR | 329% | |
| Innovative Scenario 2 (individuals over 26 years old) | 147,869,815.38 EUR | 299% |
| I year | Scenario | Overall Costsfor the Italian Cohort | Differences |
| Baseline Scenario | 12,453,917.20 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 15,430,415.83 EUR | 24% | |
| Innovative Scenario 2 (individuals over 26 years old) | 14,162,273.97 EUR | 14% | |
| II year | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 12,310,871.42 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 15,083,774.89 EUR | 23% | |
| Innovative Scenario 2 (individuals over 26 years old) | 14,169,012.11 EUR | 15% | |
| III year | Scenario | Overall Costs for the Italian Cohort | Differences |
| Baseline Scenario | 12,253,833.80 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 15,013,875.49 EUR | 23% | |
| Innovative Scenario 2 (individuals over 26 years old) | 14,103,377.75 EUR | 15% | |
| Total | Scenario | Overall costs for the Italian cohort | Differences |
| Baseline Scenario | 37,018,621.41 EUR | ||
| Innovative Scenario 1 (individuals over 18 years old) | 45,528,064.62 EUR | 23% | |
| Innovative Scenario 2 (individuals over 26 years old) | 42,434,662.82 EUR | 15% |
| Organizational Investment | Unit Number [Minimum] | Unit Number [Maximum] | Typology of Investment | h Min | h Max | Euro/h | Euro/unit | Organizational Investment [Minimum] | Organizational Investment [Maximum] |
|---|---|---|---|---|---|---|---|---|---|
| Additional Staff | 0 | 1 | Nurse | EUR 39,398.40 | EUR - | EUR 39,398.40 | |||
| Training Course | 20 | 25 | Clinician | 6 | 10 | EUR 39.60 | EUR 4752.00 | EUR 9900.00 | |
| 20 | 25 | Nurse | 6 | 10 | EUR 21.60 | EUR 2592.00 | EUR 5400.00 | ||
| 2 | 2 | Pharmacist | 6 | 10 | EUR 34.20 | EUR 410.40 | EUR 410.40 | ||
| 2 | 4 | Laboratory Experts | 6 | 10 | EUR 21.60 | EUR 259.20 | EUR 864.00 | ||
| 2 | 4 | Biologist | 6 | 10 | EUR 21.60 | EUR 259.20 | EUR 864.00 | ||
| Hospital Meeting | 20 | 25 | Clinician | 4 | 24 | EUR 39.60 | EUR 3168.00 | EUR 23,760.00 | |
| 20 | 25 | Nurse | 4 | 24 | EUR 21.60 | EUR 1728.00 | EUR 12,960.00 | ||
| 2 | 2 | Pharmacist | 4 | 24 | EUR 34.20 | EUR 273.60 | EUR 1641.6 | ||
| 2 | 4 | Laboratory Experts | 2 | 4 | EUR 21.60 | EUR 86.40 | EUR 345.60 | ||
| 2 | 4 | Biologist | 2 | 4 | EUR 21.60 | EUR 86.40 | EUR 345.60 | ||
| Patient and Caregiver education | 3 | 4 | Clinician | 1 | 2 | EUR 39.60 | EUR 118.80 | EUR 316.80 | |
| 2 | 4 | Nurses | 1 | 2 | EUR 21.60 | EUR 43.20 | EUR 172.80 | ||
| Additional Furniture | 0 | 1 | Hospital Beds | EUR 296.00 | EUR - | EUR 296.00 | |||
| Additional Equipment | 1 | 3 | Multi-parameter patient monitors | EUR 2091.43 | EUR 2091.43 | EUR 6274.29 | |||
| Total costs | EUR 15,868.63 | EUR 102,949.49 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foglia, E.; Garagiola, E.; Ladisa, V.; Rambaldi, A.; Cairoli, R.; Sammassimo, S.; Salè, E.O.; Zinzani, P.L.; Esposti, M.; Alberti, L.; et al. Multidimensional Results and Reflections on CAR-T: The Italian Evidence. Int. J. Environ. Res. Public Health 2023, 20, 3830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053830
Foglia E, Garagiola E, Ladisa V, Rambaldi A, Cairoli R, Sammassimo S, Salè EO, Zinzani PL, Esposti M, Alberti L, et al. Multidimensional Results and Reflections on CAR-T: The Italian Evidence. International Journal of Environmental Research and Public Health. 2023; 20(5):3830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053830
Chicago/Turabian StyleFoglia, Emanuela, Elisabetta Garagiola, Vito Ladisa, Alessandro Rambaldi, Roberto Cairoli, Simona Sammassimo, Emanuela Omodeo Salè, Pier Luigi Zinzani, Marco Esposti, Luisa Alberti, and et al. 2023. "Multidimensional Results and Reflections on CAR-T: The Italian Evidence" International Journal of Environmental Research and Public Health 20, no. 5: 3830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053830