
Social Isolation and Social Support Influence Health Service Utilisation and Survival after a Cardiovascular Disease Event: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Population: people living in Australia and New Zealand who had experienced a CVD event. Exclusions included intervention studies and cohorts of people with aphasia, as aphasia is not exclusively caused by a CVD event.
- (2)
- Exposure: Social health was assessed as a predictor, effect modifier, or mediator of a CVD patient’s health service utilisation or survival.
- (3)
- Outcome: CVD-related health services or survival.
- (4)
- Search: Four electronic databases from the earliest record to 21 June 2020 (Supplementary S1). References of included papers and relevant review articles were scanned for eligible papers.
- (5)
- Screening: Two independent reviewers for titles/abstracts, with discrepancies included. One reviewer for full text.
- (6)
- Data extraction: One author (R.F.P) extracted data using a pre-specified form, with a second author either independently extracting or checking data.
- (7)
- Authors were contacted when (a) the article was a conference abstract, (b) a full text could not be obtained from two university library sources, or (c) clarification or additional data were required for included papers. Authors were contacted at least twice (via email, LinkedIn, or ResearchGate).
- (8)
- Interpretation: During data extraction, papers were grouped based on their outcome/s.
3. Results
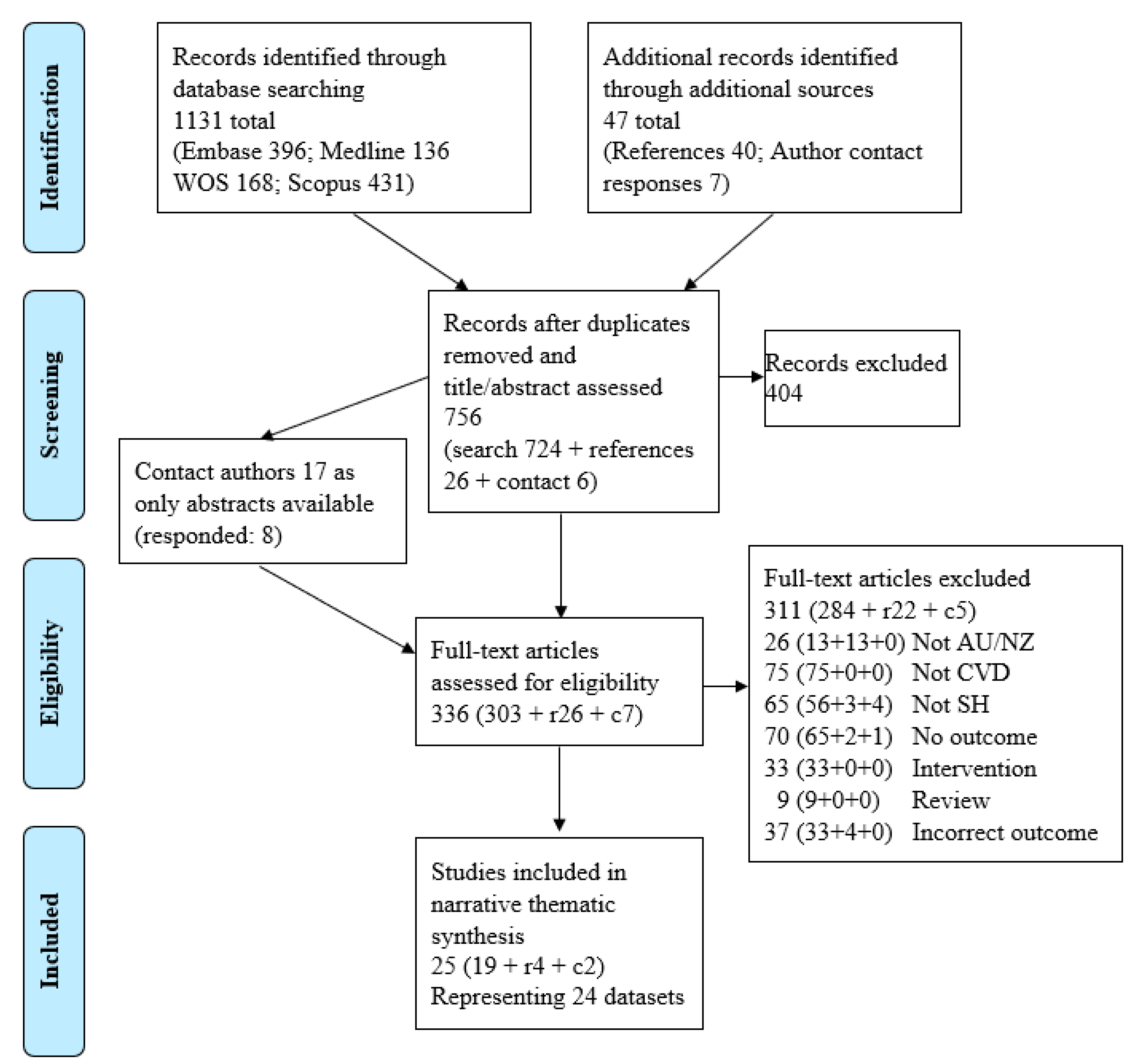
3.1. Results of the Search
3.2. Included Publications and Study Cohorts

{kind=link}
| Study ID | Sample | Eligibility and Demographics | Social Health * | Outcome | Relevant Findings |
|---|---|---|---|---|---|
| INPATIENT LENGTH OF STAY | |||||
| Turner 2010 [50] | Baseline July 2003–Jan 2006; Quant; L (6 w, 2.6 y); Au, NSW, Newcastle; n = 293–322 depending on missing data | Cardiac; rehabilitation outpatients 27.5%F; age 64.19 + 10.91 y | Marital status (n = 293; married, single, widowed, divorced or separated). Living alone (n = 322; yes or no) | Hospital length of stay, mean ~8d | Being married was associated to hospital length of stay in univariable analysis (comparator not clear, z = 2.27, p = 0.02) for all hospital stays during 2.6 y + 0.9SD follow-up but not after adjustment. No association was observed between living situation and hospital length of stay (statistics not reported). |
| Unsworth 1996 [63] | Baseline 1992; Quant; CS; Au, VIC; n = 62 (patients and consultants) | Stroke; new cerebrovascular, inpatient rehabilitation > 6 d, age ≥ 60 y; and a patient’s rehabilitation team member Patients: 52%F; age 75 y (60–90); Team: NR | Marital status (married, Single) | Rehabilitation length of stay, mean 57 d | Rehabilitation length of stay was not associated with marital status (t(58) 0.08, p = 0.9343). |
| DISCHARGE DESTINATION | |||||
| Hakkennes 2013 [52] | Baseline June 2010–Sep 2011; Quant & Qual; CS; Au, VIC; n = 89 (75 patients, 14 consultants) | Acute severe stroke; admitted (primary diagnosis), onset ≤ 3 d prior to admission, not from high-level residential care, not in intensive/palliative care on day 3 post-stroke. Assessors were clinicians responsible for assessing the suitability of patients for inpatient rehabilitation (43% consultants, 36% registrars, 21% geriatricians). No restrictions regarding qualifications or experience Patients: 49.3%F; median age 76.5 y IQR 66.0–83.0 | Living arrangement (alone, with others, supported accommodation). Qual (Social Attribute factor: Pre-morbid living situation, Patient/carer goals, Social support, Patient/carer advocating for rehabilitation) | Discharge to inpatient rehabilitation vs. not | Those accepted for rehabilitation enrolment vs. not were more likely to be living at home with others pre-stroke (Of accepted: 83.6% Home alone vs. 13.1%, Supported accommodation 3.3%, p = 0.041). (Qual) In factor analysis, Social Attributes (4 variables) accounted for 14% of the variance in allocation. An increase by 1 unit on the scale of the factor representing social attributes increased the odds of being discharged to rehabilitation by 4.402 (95%CI:1.436–13.494, p = 0.010). For those not accepted for inpatient rehabilitation, social support (median 8.2, IQR 6.7–8.5) was one of three most important items. |
| Hayward 2014 [54,55] | Baseline 2012; Quant; CS; Au, QLD; n = 21 consultants | Stroke; consultant medical officers 45.5%F; age 46.4 + 10.1 y | Factors related to social and support networks: Capacity to adapt residence for discharge, Premorbid place of residence (high-level residential care vs. other), Presence of a spouse/carer/relative and: readiness to support, ability to support, expectations for recovery, acceptance of functional prognosis/goal of rehabilitation | Perceptions of influences on discharge decision to inpatient rehabilitation vs. not | The social factors favouring the decision to admit a person with stroke to inpatient rehabilitation were capacity to adapt residence for discharge (40.9% favours, 40.9% strongly favours; total = 81.8%); presence of a spouse/carer/relative (40.9% favours, 36.4% strongly favours; total = 77.3%); spouse/carer/relative who was able to provide support (50% favours, 13.6% strongly favours; total = 63.6%); and spouse/carer/relative’s acceptance of the functional prognosis/goal of rehabilitation (50% favours, 22.7% strongly favours; total = 72.7%). The social factors disfavouring the decision to admit a person with stroke to inpatient rehabilitation were the spouse/carer/relative being ready to support (9.1% strongly disfavours, 63.6% disfavours; total = 72.7%) and have high/unrealistic expectations for recovery (68.2% strongly disfavours, 22.7 disfavours; total = 90.9%). |
| Ilett 2010 [51] | Baseline NR; Quant; CS; Au, VIC; n = 616 | Stoke (primary diagnosis); hospitalised, survivors, onset < 3 d, symptoms not resolved by day 3, not from residential care or another hospital, not admitted with another primary illness or incident 47%F; age 72.2 + 12.7 y (22–98) | Living circumstance (alone, family, supported accommodation/hostel) | Discharge destination from hospital (home, rehabilitation, nursing home) | Patients who lived with family pre-stroke were more likely to be discharged to rehabilitation than a nursing home compared to patients who lived in supported accommodation/hostel (B −1.19, p = 0.03; no association between living home alone compared to living in supported accommodation/hostel B −0.93, p = 0.11). No association was observed between pre-stroke living situation and discharge to home versus rehabilitation (with family −0.17, p = 0.79; alone −0.94, p = 0.15, compared to supported accommodation/hostel). |
| Kennedy 2012 [53] | Baseline NR; Qual; CS; Au, VIC; n = 17 physicians | Stroke; rehabilitation unit physicians Demographics NR | Qual (theme: Level of social support) | Rehabilitation admission vs. not | Social support was the second most influential patient-based factor (behind prognosis) influencing selection for rehabilitation (rating: median 2nd place, IQR: 1–3) |
| McBride 2017 [49] | Baseline July 2010–June 2015; Qual; CS; Au, SA; n = NR | Cardiac; Aboriginal patients, families, hospital staff Demographics NR | Qual (theme: Family relationships: support and loneliness) | Hospital self-discharge | “Potential reasons for [high rates of] self-discharge [by Aboriginal patients] include: competing family and community obligations; a lack of communication on the importance of staying in hospital; grief, loss and fear; loneliness and dislocation from family and community, and; perceptions of inadequate or racist treatment. Active involvement of family, community and Aboriginal staff were key in reversing patient self-discharge.” |
| Unsworth 1993 [40] | Baseline 1991; Quant; CS; Au, VIC; n = 82 consultants | Stroke; clinicians currently involved in making accommodation decisions or who had been involved in the past two years: 9 rehabilitation physicians, 16 nurses, 9 speech therapists, 19 occupational therapists, 14 physiotherapists and 15 social workers. Demographics not collected, hence NR | 3 of 15 cues: Premorbid living arrangements; Social situation, including personal and community supports; Relatives’ choice/wishes for accommodation for the client | Discharge accommodation decisions from rehabilitation (e.g., home, hostel, nursing home) | Clinicians considered that “social situation, including personal and community supports” ranked 3rd most important cue, out of 15, in patient’s discharge accommodation decisions (mean rank 4.48 ± 6.03 variance); “Premorbid living arrangements” ranked 8th (7.90 + 9.99) and “Relatives’ choice/wishes for accommodation for the client” ranked 11th (9.71 ± 6.16). |
| Unsworth 1995 [65] | Baseline 1992; Quant; CS; Au, VIC; n = 74 consultants (in 13 teams) | Stroke; clinicians in rehabilitation units 68%F; age not collected | Premorbid living arrangements and Social situation (scaled from “no emotional or physical support of either a personal or community nature to assist the patient on discharge,” through to “constant support”) considered as 2 of 8 attributes pertinent when formulating a housing recommendation | Discharge housing for 50 hypothetical patients from rehabilitation (Level 1: high dependency to Level 7: own home without supports or equipment) | After personal mobility (beta: 0.465 + 0.087SD, weight range 0.266–0.611), social situation was 2nd (beta: 0.302 + 0.111SD, weight 0.173–0.548; with personal functional skills, beta: 0.308 + 0.111SD, weight 0.124–0.468) and premorbid living arrangements was 4th (beta: 0.164 + 0.066, weight 0072–0.294) in predicting ability to make an accommodation recommendation. The contribution of social support to the decision varied between beta 0.548 and 0.148 between the 13 teams, and premorbid living varied between 0.294 and 0.069. |
| Unsworth 1996 [63] | Baseline 1992; Quant; CS; Au, VIC; n = 62 (patients and consultants) | Stroke; new cerebrovascular, inpatient rehabilitation > 6 d, age ≥ 60 y; and a patient’s rehabilitation team member Patients (n = 58): 52%F; age 75 y (60–90). Team (n = 58): Demographics NR | Marital status (Married, Single) | Discharge decisions from rehabilitation (Level 1: total assistance to Level 7: completely independent) | The team recommended and patients chose lower assisted housing if married (team: Level 5, patients Level 6; vs. single patients team: Level 3/4, t(58) 3.02, p = 0.0038; patients Level 5, t(49) 2.05, p = 0.0458). Patients saw discharge housing decisions as their own, unaware of rehabilitation team influence (correlation team recommendation vs. actual = 0.70) who generally recommended more support required. |
| Unsworth 2001 [46] | Baseline NR; Quant; CS; Au, VIC; n = 223 | Stroke (primary diagnosis); admitted using ICD-10 (World Health Organization, 1992) codes from 430 to 438 53%F; age 77.14 y (60–93) | Social interaction (measured in Adult FIMSM). Social situation, including personal and community supports. Of 24 variables assessed | Hospital discharge location (home, rehabilitation, nursing home) | Social interaction, social support and premorbid housing were 3 of 6 variables (of 24 assessed) which predicted of discharge location, after additional adjustment. Social interaction predicted discharge to rehabilitation (model 1 coefficient = 2.884, model 2 = 1.741), home (2.411, 1.368), then nursing home (1.310, 1.260). Social situation predicted discharge to home (model 2 = 0.739), rehabilitation (0.538), then nursing home (−0.721). Premorbid housing predicted discharge to home (model 2 = 1.981), rehabilitation (1.884), then home (1.016). |
| Unsworth 2003 [45] | Baseline NR (5m); Quant; CS; Au, VIC, Melbourne; n = 60 | First stroke (primary diagnosis); hospitalised, aged ≥ 60 y, rehabilitation > 6 d 52%F; age 74.7 y (60–90) | Marital status. Premorbid living arrangements. Social situation. The latter two assessed of 8 cues. | Discharge decisions from rehabilitation (Level 1: total assistance to Level 7: completely independent) | Social support was the 3rd (b = 0.201) and premorbid housing was the 4th (b = 0.136) strongest predictor of higher independent housing recommendation (behind mobility 0.299, ADL 0.248). Single participants more likely to be discharged to supported housing (levels 1–3) than married participants (t(58) = 3.018, p = 0.0038). |
| OUTPATIENT REHABILITATION ATTENDANCE | |||||
| Fernandez 2008 [64] | Baseline Aug–Nov 2005; Qual; CS; Au, NSW & ACT; n = 20 consultants | Coronary heart disease; cardiac rehabilitation coordinators Demographics NR | Qual (theme: Other individual barriers, subtheme: Low social support) | Cardiac rehabilitation attendance | “Lack of Quality Social Support: An effective system of social support is vital for the adoption of healthy behaviours. There is also evidence that involvement of partners in the rehabilitation process by engaging in risk reduction behaviours themselves is a critical factor in its effectiveness. Involvement of family in CR programs was discussed by most CR coordinators; however, they expressed that often, the family members did not actively engage in the risk modification behaviours. For example, a few coordinators indicated how the partner would smoke outside while their relative would attend CR, which demonstrated the lack of family support in engaging in risk modification behaviours.” |
| Fernandez 2008 [60] | Baseline Dec 2004–Mar 2005; Quant; CS; Au, NSW; n = 202 | CVD with successful percutaneous coronary intervention (PCI); survived 1–2 y, aged 18–80 y; not cognitively impaired; telephone contact number; hospital stay < 30 d post-PCI. Excluded: significant comorbidities; malignant disease; condition impairing cooperation in the study; transferred to a nursing home post-PCI 27%F; age 64.0 ± 11.7 y (18–80) | Marital status (living with partner vs. alone) | Cardiac rehabilitation participation | Living with a partner was the factor most strongly associated with self-reported cardiac rehabilitation participation (OR 4.05; 95%CI 1.34–12.25; p = 0.013) |
| Hagan 2007 [62] | Baseline June–Aug 2000; Qual; CS; Au, VIC, Melbourne; n = 10 | Acute myocardial infarction; survivor, first-onset, sufficient English, referred to phase 2 cardiac rehabilitation 20%F; age (31 + y) | Living arrangements (alone vs. with another person); Qual (themes: Family support, Presence of support social networks) | Cardiac rehabilitation attendance (perceived as a relevant goal) | While not statistically significant, of the patients who attended rehabilitation, all lived with another person (n = 4 of 8) compared to none who lived alone (n = 0 of 2; p = 0.3, calculated from Table 1). (Qual) Family support: “Participants in this study frequently cited the importance of family support in providing meaning in their lives and the motivation to recover and make the necessary lifestyle changes… Although consideration of family members was often part of the participant’s decision to attend a phase 2 cardiac rehabilitation program, it was also discovered that in some instances family members had little influence over their actual decision to attend. Even though these participants stated that their families were supportive of their decision, they believed that this was coincidental to their decision to attend…However, issues or problems associated with the absence of family support were seen to impact significantly on the lives of some participants. Two participants lived alone at the time of the interview, and both discussed their lack of family support at some length…” Presence of support social networks: “If a person thought that his or her life was important to others, cardiac rehabilitation was likely to be seen as a relevant goal…Living alone raised unique issues related to the need for greater social support for some participants…In contrast with the participants who lived alone and failed to attend their scheduled appointments, this participant considered that attending a phase 2 cardiac rehabilitation program was a means of gaining social support networks.” |
| Horwood 2015 [58] | Baseline NR; Quant; CS; NZ, Dunedin; n = 44 | Coronary artery disease; event >6 m and completed outpatient rehabilitation >6 m, aged > 60 y 29.5%F; age 72.7 + 6.9 y (60+) | Partner status (married/living with partner vs. not). Perceived benefits (including Social Benefits: Social standing, At ease with people, Acceptance by others, Companionship) assessed using a Multi-dimensional Outcomes Expectations for Exercise Scale (MOEES). Perceived barriers (including Social Influences: Others with heart problems don’t go, Work responsibilities, Family responsibilities) measured using Cardiac Rehabilitation Barriers Scale (CRBS) | Community-based cardiac rehabilitation attendance | No association was observed between partner status and attendance (72.7% of high attenders were married/living with partner, 75% low attenders, 70.6% non-attenders, p = 0.648). High attenders at cardiac rehabilitation reported greater perceived social benefits in social standing (high 4.3 + 0.8, low 3.2 + 1.2, non 3.2 + 1.0, p = 0.022) and at ease with people (4.3 + 0.7, 3.4 + 1.0, 3.5 + 0.9, p = 0.036) than both low and non-attenders. No association was observed between attendance and acceptance by others (4.0 + 0.6, 3.7 + 1.0, 3.3 + 0.9, p = 0.129) or companionship (4.4 + 0.7, 3.8 + 0.9, 3.7 + 1.1, p = 0.151) or social influences (Others with heart problems don’t go 1.8 + 1.4, 1.4 + 0.7, 1.9 + 1.1, p = 0.446; Work responsibilities 1.6 + 1.2, 2.3 + 1.7, 2.0 + 1.4, p = 0.567; Family responsibilities 2.0 + 1.3, 1.9 + 1.2, 1.8 + 1.3, p = 0.937). |
| Schulz 2000 [59] | Baseline Jul 1993–Dec 1996; Quant; CS; Au, VIC, Horsham; n = 79 | Acute myocardial infarction; survivor, rural 34%F; age NR | Marital status (married, all other categories). Living with a partner (yes, no) | Cardiac rehabilitation attendance | Cardiac rehabilitation attendees were more likely to be married (vs. other categories; χ2 = 8.15, p = 0.004) and living with a partner (vs. not; χ2 = 7.58, p = 0.006) than respondents who did not attend. |
| Sundararajan 2004 [38] | Baseline Jan–Dec 1998; Quant; L (not defined); Au, VIC; n = 12,821 | Acute myocardial infarction (primary diagnosis); hospitalised, coronary artery bypass grafting or percutaneous transluminal coronary angioplasty as stated in the Victorian Admitted Episodes Dataset; survived ≥30 d based on the Victorian Deaths Registry 29.9%F; age (40+) y | Marital status (Currently married, Never married, Previously married, Unknown) | The Victorian Cardiac Rehabilitation Dataset data linkage, attending ≥1 cardiac rehabilitation session | Being currently married was associated with attending cardiac rehabilitation (compared to: Never married OR 0.77, 95%CI 0.63–0.93; Previously married OR 0.77, 95%CI 0.68–0.87; Unknown OR 0.52, 95%CI 0.38–0.69) |
| Thornhill 1998 [39] | Baseline NR (recruited over 12m); Qual; CS; Au, NSW, Dubbo; n = 16 | Cardiac; hospitalised for a life-threatening cardiac episode, rural hospital 50%F; age 60 y (47–53) | Qual (theme: Important people, with subthemes: spouses, staff) | Attending cardiac rehabilitation | “Spouses were extremely important for people in both groups” (attending or non-attending cardiac rehabilitation). Partners participated in exercises, diet changes, attended rehabilitation (for attenders), and were great motivators. “Both groups of interviewees commented on two types of staff involved in their recruitment, or attempted recruitment… Interviewees, especially members of the attenders group, felt they had understood and remembered what helpful staff members said to them. Helpful staff were remembered because they chose times to see the interviewees when they ‘had some hope of understanding’ what was being said to them. Unhelpful staff were those who intimidated and confused participants.” |
| REHOSPITALISATION | |||||
| Korda 2017 [48] | Baseline Jan 2006–Apr 2009 (to Dec 2011); Quant; L (30d); Au, NSW; n = 5074 | Heart failure; hospital diagnosis (primary or additional), participating in 45 and Up Study, age ≥ 45 y, with linked data, no death before discharge, had ≥30 d of follow-up, first readmission to hospital within 30 d follow-up was not planned 42%F; age 80 ± 9.4 y, median 82 IQR 12 (45±) | Marital status (single, de facto/married). Duke Social Support Index (DSSI) 4-item social interaction subscale, range 4–12. | 30 d unplanned readmission | No association observed between marital status and 30 d unplanned readmission (aOR 0.91, 95%CI 0.78–1.05). Higher social interaction associated with lower 30 d unplanned readmission (aOR 0.95, 95%CI 0.91–0.99). |
| Turner, 2010 [50] | Baseline July 2003 to Jan 2006; Quant; L (6 w, 2.6 y); Au, NSW, Newcastle; n = 293–322 depending on missing data | Cardiac; rehabilitation outpatients 27.5%F; age 64.19 + 10.91 y | Marital status (n = 293; married, single, widowed, divorced or separated). Living alone (n = 322; yes or no) | Number of hospital admissions, mean ~2, follow-up 2.6 + 0.9SD y | No association observed between marital status or living alone with number of hospital admissions over 2.6 + 0.9SD y (univariable, statistics not reported). |
| Winefield 1982 [47] | Baseline 1980–1981; Quant; L (6–7 m); Au, SA, Adelaide; n = 29 | First myocardial infarction; hospitalised, men, age 30–65 y, English-speaking, completed psychological tests, survived 6–7 m. 0%F; age total sample: 53.53 + 8.18 y (30–65) | The Social Environment Questionnaire (SEQ) question regarding confiders in respondent. | Death, rehospitalisation | MI patients who died or were hospitalised for cardiac treatment within 6 m reported fewer confidants (n = 8, 2.88 + 2.80SD; vs. not rehospitalised and survived n = 21, confiders: 4.81 + 2.93; p = 0.06). |
| SURVIVAL | |||||
| Anderson 2004 [37] | Baseline Mar 1981–Feb 1982; Quant; L (21y); NZ, Auckland; n = 680 | Acute stroke; participating in the first Auckland Region Coronary Or Stroke (ARCOS) Study 51%F; age 71.2 ± 13.4 y | Ever married (not defined) | Survival (not defined) | No association observed between ever married and survival (92% deceased, 89% survived, X2 p = 0.37) |
| Korda 2017 [48] | Baseline Jan 2006–Apr 2009 (to Dec 2011); Quant; L (30d); Au, NSW; n = 5074 | Heart failure; hospital diagnosis (primary or additional), participating in 45 and Up Study, age ≥ 45 y, with linked data, no death before discharge, had ≥30 d of follow-up, first readmission to hospital within 30 d follow-up was not planned. 42%F; age 80 ± 9.4 y, median 82 y IQR 12 (45±) | Marital status (single, de facto/married). Duke Social Support Index (DSSI) 4-item social interaction subscale, range 4–12. | 30 d unplanned readmission | No association observed between marital status (aOR 1.06, 95%CI 0.77–1.47) or social interaction (aOR 0.97, 95%CI 0.88–1.07) and 30 d mortality. |
| Stewart 2003 [61] | Baseline Jun 1990–Dec 1992; Quant; L (baseline, median 8.1y); Au and NZ; n = 1130 | Acute myocardial infarction or hospitalized for unstable angina; survivors 3 m–3 y, age 31–75 y, enrolled in the LIPID study, a randomized placebo-controlled clinical trial of cholesterol-lowering treatment with pravastatin, and the LIPID Psychological Well-Being Substudy Gender NR; age (31–75 y) | Divorce or separation (life events scale; yes in preceding year vs. not). Social isolation (living alone and ≤4/m vs. not). Marital/family problems (life events scale; yes in preceding year vs. not). General Health Questionnaire subscale of social dysfunction. | Cardiovascular death (not defined), median follow-up 8.1 y | No association was observed between divorce/separation (aHR 0.91, 95%CI 0.28–2.89), social isolation (aHR 0.69, 95%CI 0.43–1.10), social dysfunction (aHR 0.95, 95%CI 0.59–1.54), or marital/family problems (aHR 1.02, 95%CI 0.60–1.82) and cardiovascular death over mean 8.1 y. |
| Turner, 2010 [50] | Baseline July 2003 to Jan 2006; Quant; L (6w, 2.6y); Au, NSW, Newcastle; n = 293–322 depending on missing data | Cardiac; rehabilitation outpatients 27.5%F; age 64.19 + 10.91 y | Marital status (n = 293; married, single, widowed, divorced or separated). Living alone (n = 322; yes or no) | Mortality, follow-up 2.6 + 0.9SD y (39 d–3.8 y) | No association observed between marital status or living alone with survival over 2.6 + 0.9SD y (univariable, statistics not reported). |
| Wheeler 2012 [56] | Baseline 2000–2002; Quant; L (5y); Au, SA; n = 337 | Acute myocardial infarction; hospitalised, participating in the Identifying Depression as a Comorbid Condition (IDACC) study which recruited cardiac and followed for 12 m post-discharge 26%F; age 59 + 12 y for survivors; 69 + 11 y for fatalities (23–84) | Perceived Social Support Scale (PSSS) | All-cause mortality; Cardiac mortality, 5 y | Lower social support was a predictor of 5 y all-cause mortality (survivor 5.8 + 1.2SD, death 5.4 + 1.0, p = 0.08; aHR 0.70, 95%CI 0.54–0.90 p = 0.006) and cardiac mortality (survivor 5.8 + 1.2, death 5.3 + 1.2, p = 0.12; HR 0.67,95%CI 0.49 to 0.93, p = 0.016) after adjustment. Additionally adjusting for binary depression did not alter findings (all-cause HR 0.68, 95% CI 0.50 to 0.94, p = 0.019; cardiac NR). |
| Wong 2010 [57] | Baseline July 1994–June 2004; Quant; L (10y); Au, SA; n = 753 | Chronic heart failure; hospitalised, who had echocardiograms 44.5% F; age 75.5 y | Marital status (married, widowed, separated/divorced, single). Family support/Next of kin (child or spouse vs. other) | Death linked the National Death Index, study census 30 June 2005 | “Other” relative (not spouse or child) as next of kin associated with increased survival (aHR 1.502, 95%CI 1.04–2.16, p = 0.028). Marital status not reported. |
| Winefield 1982 [47] | Baseline 1980–1981; Quant; L (6–7m); Au, SA, Adelaide; n = 29 | First myocardial infarction; hospitalised, men, age 30–65 y, English-speaking, completed psychological tests, survived 6–7 m. 0%F; age total sample: 53.53 + 8.18 y (30–65) | The Social Environment Questionnaire (SEQ) question regarding confiders in respondent. | Death, rehospitalisation | MI patients who died or were rehospitalised for cardiac treatment within 6 months reported fewer confidants (n = 8, 2.88 + 2.80SD; vs. not rehospitalised and survived n = 21, confiders: 4.81 + 2.93; p = 0.06). |
3.3. Outcomes
3.3.1. Inpatient Length of Stay
3.3.2. Discharge Destination
3.3.3. Outpatient Rehabilitation Attendance
3.3.4. Rehospitalisation
3.3.5. Survival
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Significance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Fact Sheets: Cardiovascular Diseases (CVDs) 2021. Available online: www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 5 March 2023).
- Bloom, D.E.; Cafiero, E.T.; Jané-Llopis, E.; Abrahams-Gessel, S.; Bloom, L.R.; Fathima, S.; Feigl, A.B.; Gaziano, T.; Hamandi, A.; Mowafi, M.; et al. The Global Economic Burden of Noncommunicable Diseases; World Economic Forum: Geneva, Switzerland, 2011. [Google Scholar]
- Nghiem, S.; Afoakwah, C.; Byrnes, J.; Scuffham, P. Lifetime Costs of Hospitalised Cardiovascular Disease in Australia: An Incidence-Based Estimate. Heart Lung Circ. 2021, 30, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Ronzi, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart Br. Card. Soc. 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. A J. Assoc. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Freak-Poli, R.; Ryan, J.; Neumann, J.T.; Tonkin, A.; Reid, C.M.; Woods, R.L.; Nelson, M.; Stocks, N.; Berk, M.; McNeil, J.J.; et al. Social isolation, social support and loneliness as predictors of cardiovascular disease incidence and mortality. BMC Geriatr. 2021, 21, 711. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; The National Academies Press: Washington, DC, USA, 2020; 316p. [Google Scholar]
- Freak-Poli, R.; Ryan, J.; Tran, T.; Owen, A.; Power, J.M.; Berk, M.; Stocks, N.; Gonzalez-Chica, D.; Lowthian, J.A.; Fisher, J.; et al. Social isolation, social support and loneliness as independent concepts, and their relationship with health-related quality of life among older women. Aging Ment. Health 2022, 26, 1335–1344. [Google Scholar] [CrossRef]
- Cloutier-Fisher, D.; Kobayashi, K.; Smith, A. The subjective dimension of social isolation: A qualitative investigation of older adults’ experiences in small social support networks. J. Aging Stud. 2011, 25, 407–414. [Google Scholar] [CrossRef]
- Mund, M.; Freuding, M.M.; Mobius, K.; Horn, N.; Neyer, F.J. The Stability and Change of Loneliness Across the Life Span: A Meta-Analysis of Longitudinal Studies. Pers. Soc. Psychol. Rev. 2020, 24, 24–52. [Google Scholar] [CrossRef]
- Sebri, V.; Mazzoni, D.; Triberti, S.; Pravettoni, G. The Impact of Unsupportive Social Support on the Injured Self in Breast Cancer Patients. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Hu, J.; Phyo, A.Z.Z.; Barker, F. Does social isolation, social support or loneliness influence health or well-being after a cardiovascular disease event? A narrative thematic systematic review. Health Soc. Care Community 2022, 30, e16–e38. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Phyo, A.Z.Z.; Hu, J.; Barker, S.F. Are social isolation, lack of social support or loneliness risk factors for cardiovascular disease in Australia and New Zealand? A systematic review and meta-analysis. Health Promot. J. Austr. 2022, 33 (Suppl. 1), 278–315. [Google Scholar] [CrossRef]
- Freak-Poli, R.; Wagemaker, N.; Wang, R.; Lysen, T.S.; Ikram, M.A.; Vernooij, M.W.; Dintica, C.S.; Vernooij-Dassen, M.; Melis, R.J.; Laukka, E.J.; et al. Loneliness, Not Social Support, Is Associated with Cognitive Decline and Dementia Across Two Longitudinal Population-Based Cohorts. J. Alzheimers Dis. 2022, 85, 295–308. [Google Scholar] [CrossRef]
- Hu, J.; Fitzgerald, S.M.; Owen, A.J.; Ryan, J.; Joyce, J.; Chowdhury, E.; Reid, C.M.; Britt, C.; Woods, R.L.; McNeil, J.J.; et al. Social isolation, social support, loneliness and cardiovascular disease risk factors: A cross-sectional study among older adults. Int. J. Geriatr. Psychiatry 2021, 36, 1795–1809. [Google Scholar] [CrossRef] [PubMed]
- Joyce, J.; Ryan, J.; Owen, A.; Hu, J.; Power, J.M.; Shah, R.; Woods, R.; Storey, E.; Britt, C.; Freak-Poli, R.; et al. Social isolation, social support, and loneliness and their relationship with cognitive health and dementia. Int. J. Geriatr. Psychiatry 2021, 37, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef] [PubMed]
- de Jong Gierveld, J.; van Tilburg, T.; Dykstra, P. New Ways of Theorizing and Conducting Research in the Field of Loneliness and Social Isolation. In The Cambridge Handbook of Personal Relationships; Vangelisti, A.L., Perlman, D., Eds.; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Hanratty, B. Loneliness, social isolation and social relationships: What are we measuring? A novel framework for classifying and comparing tools. BMJ Open 2016, 6, e010799. [Google Scholar] [CrossRef] [PubMed]
- Valtorta, N.K.; Moore, D.C.; Barron, L.; Stow, D.; Hanratty, B. Older Adults’ Social Relationships and Health Care Utilization: A Systematic Review. Am. J. Public Health 2018, 108, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Heidari Gorji, M.A.; Fatahian, A.; Farsavian, A. The impact of perceived and objective social isolation on hospital readmission in patients with heart failure: A systematic review and meta-analysis of observational studies. Gen. Hosp. Psychiatry 2019, 60, 27–36. [Google Scholar] [CrossRef]
- Dufour, I.; Chouinard, M.C.; Dubuc, N.; Beaudin, J.; Lafontaine, S.; Hudon, C. Factors associated with frequent use of emergency-department services in a geriatric population: A systematic review. BMC Geriatr. 2019, 19, 185. [Google Scholar] [CrossRef]
- Andrew, M.K.; Powell, C. An Approach to ‘The Social Admission’. Can. J. Gen. Intern. Med. 2015, 10, 20–22. [Google Scholar]
- Bu, F.; Zaninotto, P.; Fancourt, D. Longitudinal associations between loneliness, social isolation and cardiovascular events. Heart Br. Card. Soc. 2020, 106, 1394–1399. [Google Scholar] [CrossRef]
- Kukull, W.A.; Ganguli, M. Generalizability: The trees, the forest, and the low-hanging fruit. Neurology 2012, 78, 1886–1891. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software VHI, Melbourne, Australia. Available online: www.covidence.org (accessed on 1 September 2020).
- Bertorelli, D.; Metro South Health, Brisbane, Australian; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Gaskin, K.; St John’s Campus, University of Worcester, Henwick Grove, Worcester, UK; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Maiorana, A.; Curtin University, Chippendale, New South Wales; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Moorley, C.; London South Bank University, London, UK; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Pinyopasakul, W.; Mahidol University, Bangkok, Thailand; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Ranta, A.; University of Otago, Dunedin, New Zealand; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Von Dohren, C.; North Lakes Health Precinct, North Lakes, QLD, Australia; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Wells, S.; University of Otago, Dunedin, New Zealand; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Jacobs, D.; Cardiac Assessment Unit, Bowral & District Hospital, Bowral, New South Wales; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Anderson, C.S.; Carter, K.N.; Brownlee, W.J.; Hackett, M.L.; Broad, J.B.; Bonita, R. Very long-term outcome after stroke in Auckland, New Zealand. Stroke 2004, 35, 1920–1924. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, V.; Bunker, S.J.; Begg, S.; Marshall, R.; McBurney, H. Attendance rates and outcomes of cardiac rehabilitation in Victoria, 1998. Med. J. Aust. 2004, 180, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, M.; Stevens, J.A. Client perceptions of a rural-based cardiac rehabilitation program: A grounded theory approach. Aust. J. Rural Health 1998, 6, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Unsworth, C.A.; Thomas, S.A. Information use in discharge accommodation recommendations for stroke patients. Clin. Rehabil. 1993, 7, 181–188. [Google Scholar]
- Brock, K.; St Vincent’s Health Australia, Melbourne, Australia; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- McBride, K.; Independent medical research institute, Adelaide, Australia; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Unsworth, C.A.; Central Queensland University, Rockhampton, Australia; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Winefield, H.; The University of Adelaide, Adelaide, South Australia; Freak-Poli, R.; Monash University, Melbourne, Australia. Personal communication, 2020.
- Unsworth, C.A.; Thomas, S.A. External validation of a housing recommendation model for clients following stroke rehabilitation. Disabil. Rehabil. 2003, 25, 1208–1218. [Google Scholar] [CrossRef]
- Unsworth, C.A. Selection for rehabilitation: Acute care discharge patterns for stroke and orthopaedic patients. Int. J. Rehabil. Res. 2001, 24, 103–114. [Google Scholar] [CrossRef]
- Winefield, H.R. Male social support and recovery after myocardial infarction. Aust. J. Psychol. 1982, 34, 45–52. [Google Scholar] [CrossRef]
- Korda, R.J.; Du, W.; Day, C.; Page, K.; Macdonald, P.S.; Banks, E. Variation in readmission and mortality following hospitalisation with a diagnosis of heart failure: Prospective cohort study using linked data. BMC Health Serv. Res. 2017, 17, 1–18. [Google Scholar] [CrossRef]
- McBride, K.; Kelly, J.; Dowling, A.; Keech, W.; Brown, A. Unpacking high self-discharge rates for aboriginal cardiac patients. Heart Lung Circ. 2017, 26 (Suppl. 2), S337–S338. [Google Scholar] [CrossRef]
- Turner, A.; Phillips, L.; Hambridge, J.A.; Baker, A.L.; Bowman, J.; Colyvas, K. Clinical outcomes associated with depression, anxiety and social support among cardiac rehabilitation attendees. Aust. N. Z. J. Psychiatry 2010, 44, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Ilett, P.A.; Brock, K.A.; Graven, C.J.; Cotton, S.M. Selecting Patients for Rehabilitation After Acute Stroke: Are There Variations in Practice? Arch. Phys. Med. Rehabil. 2010, 91, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Hakkennes, S.; Brock, K.; Hill, K.; Churilov, L. Selection for inpatient rehabilitation following severe stroke: An observational study. Neurorehabilit. Neural Repair. 2012, 26, 761. [Google Scholar]
- Kennedy, G.M.; Brock, K.A.; Lunt, A.W.; Black, S.J. Factors influencing selection for rehabilitation after stroke: A questionnaire using case scenarios to investigate physician perspectives and level of agreement. Arch. Phys. Med. Rehabil. 2012, 93, 1457–1459. [Google Scholar] [CrossRef]
- Hayward, K.S.; Aitken, P.D.; Barker, R.N.; Brauer, S.G. Admission to and Continuation of Inpatient Stroke Rehabilitation in Queensland, Australia: A Survey of Factors that Contribute to the Consultant’s Decision. Brain Impair. 2014, 15, 88–98. [Google Scholar] [CrossRef]
- Hayward, K.S.; Aitkin, P.D.; Barker, R.N.; Brauer, S.G. Factors influencing the consultants’ decision to admit a stroke survivor to and then continue or cease inpatient stroke rehabilitation: A statewide survey. Int. J. Stroke 2013, 8 (Suppl. 1), 33. [Google Scholar]
- Wheeler, A.; Beltrame, J.; Tucker, G.; Air, T.; Ling, L.-H.; Schrader, G. Depression and 5-year mortality in patients with acute myocardial infarction: Analysis of the IDACC database. Aust. N. Z. J. Psychiatry 2012, 46, 669–675. [Google Scholar] [CrossRef]
- Wong, D.T.; Clark, R.A.; Dundon, B.K.; Philpott, A.; Molaee, P.; Shakib, S. Caveat anicula! Beware of quiet little old ladies: Demographic features, pharmacotherapy, readmissions and survival in a 10-year cohort of patients with heart failure and preserved systolic function. Med. J. Aust. 2010, 192, 9–13. [Google Scholar] [CrossRef]
- Horwood, H.; Williams, M.J.A.; Mandic, S. Examining Motivations and Barriers for Attending Maintenance Community-Based Cardiac Rehabilitation Using the Health-Belief Model. Heart Lung Circ. 2015, 24, 980–987. [Google Scholar] [CrossRef]
- Schulz, D.L.; McBurney, H. Factors which influence attendance at a rural Australian cardiac rehabilitation program. Coron. Health Care 2000, 4, 135–141. [Google Scholar] [CrossRef]
- Fernandez, R.S.; Salamonson, Y.; Griffiths, R.; Juergens, C.; Davidson, P. Sociodemographic predictors and reasons for participation in an outpatient cardiac rehabilitation programme following percutaneous coronary intervention. Int. J. Nurs. Pract. 2008, 14, 237–242. [Google Scholar] [CrossRef]
- Stewart, R.A.; North, F.M.; West, T.M.; Sharples, K.J.; Simes, R.J.; Colquhoun, D.M.; White, H.D.; Tonkin, A.M. Depression and cardiovascular morbidity and mortality: Cause or consequence? Eur. Heart J. 2003, 24, 2027–2037. [Google Scholar] [CrossRef]
- Hagan, N.A.; Botti, M.A.; Watts, R.J. Financial, family, and social factors impacting on cardiac rehabilitation attendance. Heart Lung J. Crit. Care 2007, 36, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Unsworth, C. Clients’ perceptions of discharge housing decisions after stroke rehabilitation. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1996, 50, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, R.S.; Davidson, P.; Griffiths, R. Cardiac rehabilitation coordinators’ perceptions of patient-related barriers to implementing cardiac evidence-based guidelines. J. Cardiovasc. Nurs. 2008, 23, 449–457. [Google Scholar] [CrossRef]
- Unsworth, C.A.; Thomas, S.A.; Greenwood, K.M. Rehabilitation team decisions on discharge housing for stroke patients. Arch. Phys. Med. Rehabil. 1995, 76, 331–340. [Google Scholar] [CrossRef]
- Petrie, K.J.; Weinman, J.; Sharpe, N.; Buckley, J. Role of patients’ view of their illness in predicting return to work and functioning after myocardial infarction: Longitudinal study. Br. Med. J. 1996, 312, 1191–1194. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australia’s Welfare 1997: Services and Assistance; AIHW: Canberra, Australia, 1997.
- Azzopardi, S.; Lee, G. Health-Related Quality of Life 2 Years After Coronary Artery Bypass Graft Surgery. J. Cardiovasc. Nurs. 2009, 24, 232–240. [Google Scholar] [CrossRef]
- White, J.H.; MacKenzie, L.; Magin, P.; Pollack, M.R.P. The occupational experience of stroke survivors in a community setting. OTJR Occup. Particip. Health 2008, 28, 160–167. [Google Scholar] [CrossRef]
- Ski, C.; O’Connell, B. Stroke: The increasing complexity of carer needs. J. Neurosci. Nurs. J. Am. Assoc. Neurosci. Nurses 2007, 39, 172–179. [Google Scholar] [CrossRef]
- Clark, M.S.; Rubenach, S.; Winsor, A. A randomized controlled trial of an education and counselling intervention for families after stroke. Clin. Rehabil. 2003, 17, 703–712. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare (AIHW). Cardiovascular Disease in Australian Women—A Snapshot of National Statistics. Cat. No. CDK 10; AIHW: Canberra, Australia, 2019.
- Darsin Singh, S.K.; Noor, A.B.; Ahmedy, F.; Abdullah, K.L.; Abidin, I.Z.; Suhaimi, A.B.; Sator, P. Exploring Social Support for Women Coping with a Cardiac Rehabilitation Programme after Acute Coronary Syndrome: A Systematic Review of Qualitative Studies. J. Rehabil. Med. 2022, 54, jrm00295. [Google Scholar] [CrossRef] [PubMed]
- Clayton, C.; Motley, C.; Sakakibara, B. Enhancing Social Support Among People with Cardiovascular Disease: A Systematic Scoping Review. Curr. Cardiol. Rep. 2019, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Jellema, S.; Wijnen, M.A.M.; Steultjens, E.M.J.; Nijhuis-van der Sanden, M.A.-O.; van der Sande, R. Valued activities and informal caregiving in stroke: A scoping review. Disabil. Rehabil. 2019, 41, 2223–2234. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freak-Poli, R.; Hu, J.; Phyo, A.Z.Z.; Barker, S.F. Social Isolation and Social Support Influence Health Service Utilisation and Survival after a Cardiovascular Disease Event: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4853. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20064853
Freak-Poli R, Hu J, Phyo AZZ, Barker SF. Social Isolation and Social Support Influence Health Service Utilisation and Survival after a Cardiovascular Disease Event: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(6):4853. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20064853
Chicago/Turabian StyleFreak-Poli, Rosanne, Jessie Hu, Aung Zaw Zaw Phyo, and S. Fiona Barker. 2023. "Social Isolation and Social Support Influence Health Service Utilisation and Survival after a Cardiovascular Disease Event: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 6: 4853. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20064853