
The Effect of Community-Based Exercise on Health Outcomes for Indigenous Peoples with Type 2 Diabetes: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
- Participants/populationIndigenous adults 18 years of age or older participate in community-based exercise programmes intended to prevent or manage type 2 diabetes.
- Intervention(s), exposure(s)Community-based group exercise programmes are intended to prevent or manage type 2 diabetes.
- Comparator(s)/controlParticipants who receive usual care. Those who do not receive community-based group exercise programmes intended to prevent or manage type 2 diabetes.
- Main outcome(s)Pre and post-health outcomes using behavioural, clinical, or psychosocial measures. Primary outcomes of interest include glycaemic control (measured by HbA1c), body mass index (BMI), waist circumference, physical fitness measures, functional capacity, and psychosocial outcomes, e.g., quality of life (QOL).
- Additional outcome(s)Clinician-type, clinician experience, setting of intervention, mode of delivery, and level of adherence to the intervention.
2.3. Inclusion-Exclusion Criteria
2.4. Study Selection
2.5. Outcome Measures
2.6. Quality Appraisal
2.6.1. Mixed Methods Appraisal Tool (MMAT)
2.6.2. Community Engagement Tool (CET)
2.7. Data Extraction
2.8. Data Synthesis
3. Results
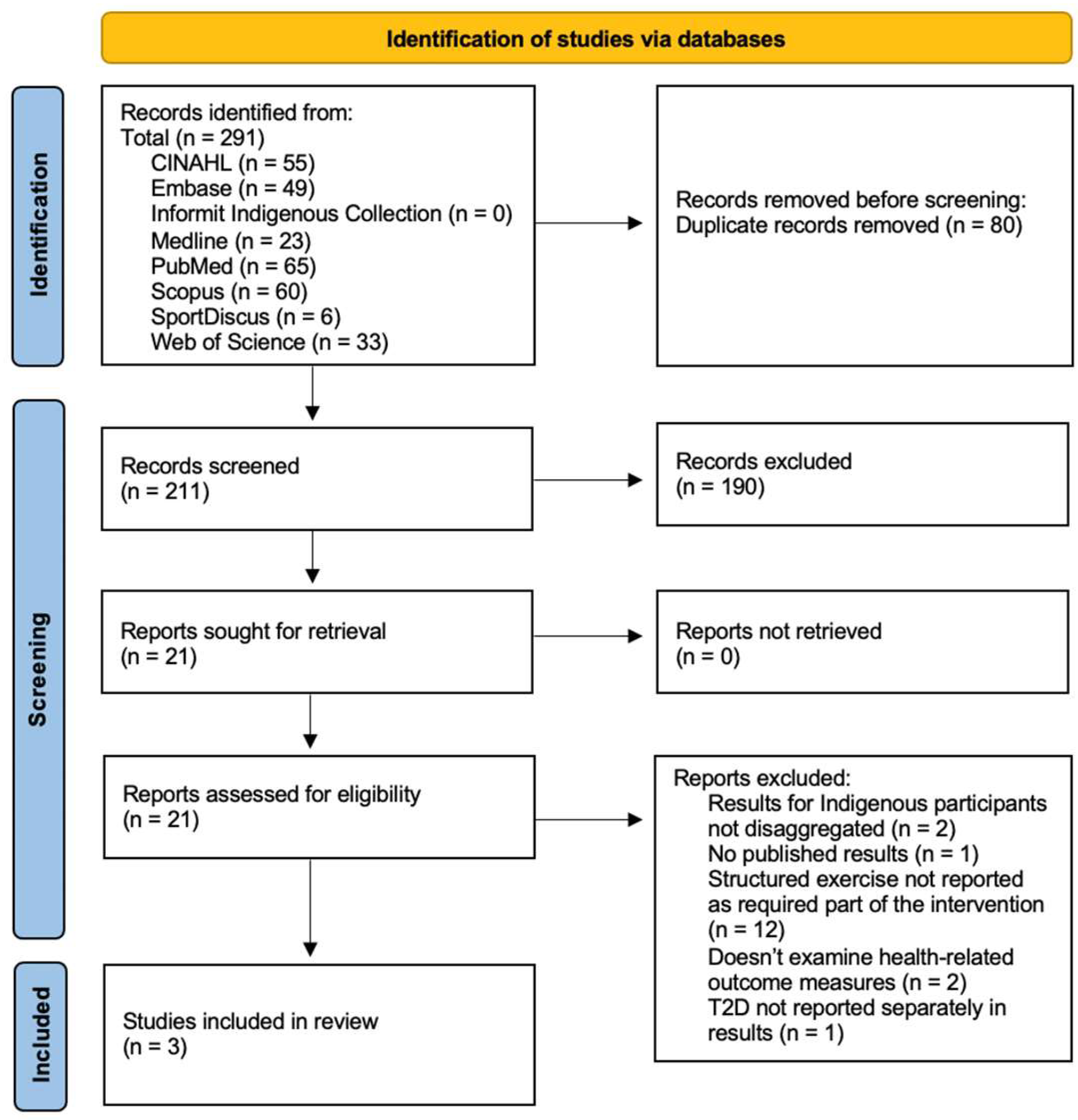
3.1. Study Selection
3.2. Quality Appraisal
3.3. Study Characteristics
3.4. Outcome of Interventions
3.4.1. Biomedical Outcomes
3.4.2. Psychosocial Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Axelsson, P.; Kukutai, T.; Kippen, R. The field of Indigenous health and the role of colonisation and history. J. Popul. Res. 2016, 33, 1–7. [Google Scholar] [CrossRef]
- Burrow, S.; Ride, K. Review of diabetes among Aboriginal and Torres Strait Islander people. Aust. Indig. Health 2016. Available online: https://nla.gov.au/nla.obj-279724722/view (accessed on 27 October 2023).
- Sushames, A.; van Uffelen, J.G.; Gebel, K. Do physical activity interventions in Indigenous people in Australia and New Zealand improve activity levels and health outcomes? A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 129. [Google Scholar] [CrossRef]
- Czyzewski, K. Colonialism as a Broader Social Determinant of Health. Int. Indig. Policy J. 2011, 2. [Google Scholar] [CrossRef]
- Sherwood, J. Colonisation—It’s bad for your health: The context of Aboriginal health. Contemp. Nurse 2013, 46, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Canada Clinical Practice Guidelines Expert Committee; Crowshoe, L.; Dannenbaum, D.; Green, M.; Henderson, R.; Hayward, M.N.; Toth, E. Type 2 Diabetes and Indigenous Peoples. Can. J. Diabetes 2018, 42 (Suppl. 1), S296–S306. [Google Scholar] [CrossRef]
- United Nations. Chapter V: Health; United Nations: New York, NY, USA, 2009; pp. 156–187. [Google Scholar]
- Meyer, W.H. Indigenous Rights, Global Governance, and State Sovereignty. Human Rights Rev. 2012, 13, 327–347. [Google Scholar] [CrossRef]
- National Congress of American Indians. Tribal Nations & the United States: An Introduction. Available online: https://www.ncai.org/about-tribes (accessed on 27 October 2023).
- Sukala, W.R.; Page, R.; Rowlands, D.S.; Krebs, J.; Lys, I.; Leikis, M.; Pearce, J.; Cheema, B.S.; Sukala, W.R.; Page, R.; et al. South Pacific Islanders resist type 2 diabetes: Comparison of aerobic and resistance training. Eur. J. Appl. Physiol. 2012, 112, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Sukala, W.R.; Page, R.; Lonsdale, C.; Lys, I.; Rowlands, D.; Krebs, J.; Leikis, M.; Cheema, B.S. Exercise improves quality of life in indigenous Polynesian peoples with type 2 diabetes and visceral obesity. J. Phys. Act. Health 2013, 10, 699–707. [Google Scholar] [CrossRef]
- Shah, V.O.; Carroll, C.; Mals, R.; Ghahate, D.; Bobelu, J.; Sandy, P.; Colleran, K.; Schrader, R.; Faber, T.; Burge, M.R. A home-based educational intervention improves patient activation measures and diabetes health indicators among Zuni Indians. PloS ONE 2015, 10, e0125820. [Google Scholar] [CrossRef]
- Australian Institute of Health Welfare. Determinants of Health for Indigenous Australians; AIHW: Canberra, Australia, 2022. [Google Scholar]
- Marmot, M. Social determinants and the health of Indigenous Australians. Med. J. Aust. 2011, 194, 512–513. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Dandeneau, S.; Marshall, E.; Phillips, M.K.; Williamson, K.J. Rethinking resilience from indigenous perspectives. Can. J. Psychiatry 2011, 56, 84–91. [Google Scholar] [CrossRef]
- Usher, K.; Jackson, D.; Walker, R.; Durkin, J.; Smallwood, R.; Robinson, M.; Sampson, U.N.; Adams, I.; Porter, C.; Marriott, R. Indigenous Resilience in Australia: A Scoping Review Using a Reflective Decolonizing Collective Dialogue. Front. Public Health 2021, 9, 630601. [Google Scholar] [CrossRef]
- Kirwan, M.; Chiu, C.L.; Hay, M.; Laing, T. Community-Based Exercise and Lifestyle Program Improves Health Outcomes in Older Adults with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 6147. [Google Scholar] [CrossRef]
- Diabetes Australia. Diabetes Globally. Available online: https://www.diabetesaustralia.com.au/about-diabetes/diabetes-globally/ (accessed on 27 October 2023).
- Ministry of Health. A Portrait of Health. Key Results of the 2006/07 New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2008.
- World Health Organisation. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 28 October 2023).
- U.S. Department of Health and Human Services, I.H.S. Indian Health Disparities; HIS: Rockville, MD, USA, 2019.
- International Diabetes Federation. Type 2 Diabetes. Available online: https://www.idf.org/aboutdiabetes/type-2-diabetes.html (accessed on 27 October 2023).
- National Institute of Diabetes and Digestive and Kidney Diseases. What is Diabetes? Available online: https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes (accessed on 27 October 2023).
- Cheran, K.; Murthy, C.; Bornemann, E.A.; Kamma, H.K.; Alabbas, M.; Elashahab, M.; Abid, N.; Manaye, S.; Venugopal, S. The Growing Epidemic of Diabetes among the Indigenous Population of Canada: A Systematic Review. Cureus 2023, 15, e36173. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Australia. Type 2 Diabetes. Available online: https://www.diabetesaustralia.com.au/about-diabetes/type-2-diabetes/ (accessed on 27 October 2023).
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes—2011. Diabetes Care 2011, 34 (Suppl. 1), S11–S61. [Google Scholar] [CrossRef] [PubMed]
- Umpierre, D.; Ribeiro, P.A.B.; Kramer, C.K.; Leitão, C.B.; Zucatti, A.T.N.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical Activity Advice Only or Structured Exercise Training and Association with HbA1c Levels in Type 2 Diabetes: A Systematic Review and Meta-analysis. JAMA 2011, 305, 1790–1799. [Google Scholar] [CrossRef]
- Dasso, N.A. How is exercise different from physical activity? A concept analysis. Nurs. Forum 2019, 54, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Costigan, S.A.; Karunamuni, N.D.; Lubans, D.R. Community-based physical activity interventions for treatment of type 2 diabetes: A systematic review with meta-analysis. Front. Endocrinol. 2013, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, M.; Gwynne, K.; Laing, T.; Hay, M.; Chowdhury, N.; Chiu, C.L. Can Health Improvements from a Community-Based Exercise and Lifestyle Program for Older Adults with Type 2 Diabetes Be Maintained? A Follow up Study. Diabetology 2022, 3, 348–354. [Google Scholar] [CrossRef]
- Banna, J.; Bersamin, A. Community involvement in design, implementation and evaluation of nutrition interventions to reduce chronic diseases in indigenous populations in the U.S.: A systematic review. Int. J. Equity Health 2018, 17, 116. [Google Scholar] [CrossRef] [PubMed]
- Pressick, E.L.; Gray, M.A.; Cole, R.L.; Burkett, B.J. A systematic review on research into the effectiveness of group-based sport and exercise programs designed for Indigenous adults. J. Sci. Med. Sport 2016, 19, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- The EndNote Team. EndNote, EndNote 20; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B. Mixed methods appraisal tool (MMAT), version 2018. BMJ Open 2018, 10, 1148552. [Google Scholar]
- Christie, V.; Green, D.; Amin, J.; Pyke, C.; Littlejohn, K.; Skinner, J.; McCowen, D.; Gwynne, K. What Is the Evidence Globally for Culturally Safe Strategies to Improve Breast Cancer Outcomes for Indigenous Women in High Income Countries? A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6073. [Google Scholar] [CrossRef] [PubMed]
- Christie, V.; Amin, J.; Skinner, J.; Green, D.; Littlejohn, K.; Gwynne, K. Comparison of Study Quality as Determined by Standard Research and Community Engagement Metrics: A Pilot Study on Breast Cancer Research in Urban, Rural, and Remote Indigenous Communities. Int. J. Environ. Res. Public Health 2022, 19, 5008. [Google Scholar] [CrossRef]
- Dyck, R.; Osgood, N.; Lin, T.H.; Gao, A.; Stang, M.R. Epidemiology of diabetes mellitus among First Nations and non-First Nations adults. CMAJ 2010, 182, 249–256. [Google Scholar] [CrossRef]
- Wedekind, L.E.; Mitchell, C.M.; Andersen, C.C.; Knowler, W.C.; Hanson, R.L. Epidemiology of Type 2 Diabetes in Indigenous Communities in the United States. Curr. Diabetes Rep. 2021, 21, 47. [Google Scholar] [CrossRef]
- Batal, M.; Chan, H.M.; Fediuk, K.; Ing, A.; Berti, P.; Sadik, T.; Johnson-Down, L. Associations of health status and diabetes among First Nations Peoples living on-reserve in Canada. Can. J. Public Health 2021, 112, 154–167. [Google Scholar] [CrossRef]
- Wang, M.L.; McElfish, P.A.; Long, C.R.; Lee, M.S.; Bursac, Z.; Kozak, A.T.; Ko, L.K.; Kulik, N.; Kim Yeary, K.H.-C. BMI and related risk factors among U.S. Marshallese with diabetes and their families. Ethn. Health 2021, 26, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; McDermott, R.; Thompson, F.; Usher, K. Depression and diabetes in the remote Torres Strait Islands. Health Promot. J. Austr. 2017, 28, 59–66. [Google Scholar] [CrossRef] [PubMed]
- McElfish, P.A.; Purvis, R.S.; Esquivel, M.K.; Sinclair, K.A.; Townsend, C.; Hawley, N.L.; Haggard-Duff, L.K.; Kaholokula, J.K. Diabetes Disparities and Promising Interventions to Address Diabetes in Native Hawaiian and Pacific Islander Populations. Curr. Diabetes Rep. 2019, 19, 19. [Google Scholar] [CrossRef]
- Minges, K.E.; Zimmet, P.; Magliano, D.J.; Dunstan, D.W.; Brown, A.; Shaw, J.E. Diabetes prevalence and determinants in Indigenous Australian populations: A systematic review. Diabetes Res. Clin. Pract. 2011, 93, 139–149. [Google Scholar] [CrossRef]
- Apidechkul, T. Prevalence and factors associated with type 2 diabetes mellitus and hypertension among the hill tribe elderly populations in northern Thailand. BMC Public Health 2018, 18, 694. [Google Scholar] [CrossRef] [PubMed]
- Hare, M.J.L.; Zhao, Y.; Guthridge, S.; Burgess, P.; Barr, E.L.M.; Ellis, E.; Butler, D.; Rosser, A.; Falhammar, H.; Maple-Brown, L.J. Prevalence and incidence of diabetes among Aboriginal people in remote communities of the Northern Territory, Australia: A retrospective, longitudinal data-linkage study. BMJ Open 2022, 12, e059716. [Google Scholar] [CrossRef]
- McNamara, B.J.; Sanson-Fisher, R.; D’Este, C.; Eades, S. Type 2 diabetes in Indigenous populations: Quality of intervention research over 20 years. Prev. Med. 2011, 52, 3–9. [Google Scholar] [CrossRef]
- Sanson-Fisher, R.W.; Campbell, E.M.; Perkins, J.J.; Blunden, S.V.; Davis, B.B. Indigenous health research: A critical review of outputs over time. Med. J. Aust. 2006, 184, 502–505. [Google Scholar] [CrossRef]
- Stanley, L.R.; Swaim, R.C.; Kaholokula, J.K.a.; Kelly, K.J.; Belcourt, A.; Allen, J. The Imperative for Research to Promote Health Equity in Indigenous Communities. Prev. Sci. 2020, 21, 13–21. [Google Scholar] [CrossRef]
- Liu, H.; Huffman, M.D.; Trieu, K. The role of contextualisation in enhancing non-communicable disease programmes and policy implementation to achieve health for all. Health Res. Policy Syst. 2020, 18, 38. [Google Scholar] [CrossRef]
- Whitesell, N.R.; Mousseau, A.; Parker, M.; Rasmus, S.; Allen, J. Promising Practices for Promoting Health Equity through Rigorous Intervention Science with Indigenous Communities. Prev. Sci. 2020, 21, 5–12. [Google Scholar] [CrossRef]
- Heinrich, K.; Kurtz, B.; Patterson, M.; Crawford, D.; Barry, A. Incorporating a Sense of Community in a Group Exercise Intervention Facilitates Adherence. Health Behav. Res. 2022, 5, 1. [Google Scholar] [CrossRef]
- Sukala, W.R.; Page, R.; Cheema, B.S. Exercise training in high-risk ethnic populations with type 2 diabetes: A systematic review of clinical trials. Diabetes Res. Clin. Pract. 2012, 97, 206–216. [Google Scholar] [CrossRef]
- Newman, S.; Cheng, T.; Ghahate, D.M.; Bobelu, J.; Sandy, P.; Faber, T.; Shah, V.O. Assessing knowledge and attitudes of diabetes in Zuni Indians using a culture-centered approach. PLoS ONE 2014, 9, e99614. [Google Scholar] [CrossRef]
- Kirwan, J.P.; Sacks, J.; Nieuwoudt, S. The essential role of exercise in the management of type 2 diabetes. Cleve Clin. J. Med. 2017, 84, S15–S21. [Google Scholar] [CrossRef]
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C.; White, R.D. Physical activity/exercise and type 2 diabetes: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 1433–1438. [Google Scholar] [CrossRef]
- Farzad, N.; Majid, M.; Abbas, Y.; Haidar, N.; Akbar, A.; Naimeh Mashinchi, A.; Mitra, N.; Jalil Houshyar, G.; Vahideh, S. Effect of regular exercise training on changes in HbA1c, BMI and VO2max among patients with type 2 diabetes mellitus: An 8-year trial. BMJ Open Diabetes Res. Care 2017, 5, e000414. [Google Scholar] [CrossRef]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Nicolucci, A.; Balducci, S.; Cardelli, P.; Cavallo, S.; Fallucca, S.; Bazuro, A.; Simonelli, P.; Iacobini, C.; Zanuso, S.; Pugliese, G.; et al. Relationship of exercise volume to improvements of quality of life with supervised exercise training in patients with type 2 diabetes in a randomised controlled trial: The Italian Diabetes and Exercise Study (IDES). Diabetologia 2012, 55, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Alison, R.H.; Mark, R.E. Amount and frequency of exercise affect glycaemic control more than exercise mode or intensity. Br. J. Sports Med. 2015, 49, 1012. [Google Scholar] [CrossRef]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef]
- Jing, X.; Chen, J.; Dong, Y.; Han, D.; Zhao, H.; Wang, X.; Gao, F.; Li, C.; Cui, Z.; Liu, Y.; et al. Related factors of quality of life of type 2 diabetes patients: A systematic review and meta-analysis. Health Qual. Life Outcomes 2018, 16, 189. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M.; Tobias, M.I.; Sarfati, D.; Haslett, S.J. SF-36 health survey reliability, validity and norms for New Zealand. Aust. N. Z. J. Public Health 1999, 23, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Foliaki, S.; Pearce, N. Prevention and control of diabetes in Pacific people. BMJ 2003, 327, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.H.; Mahoney, E.R.; Stock, R.; Tusler, M. Do increases in patient activation result in improved self-management behaviors? Health Serv. Res. 2007, 42, 1443–1463. [Google Scholar] [CrossRef]
- Rask, K.J.; Ziemer, D.C.; Kohler, S.A.; Hawley, J.N.; Arinde, F.J.; Barnes, C.S. Patient activation is associated with healthy behaviors and ease in managing diabetes in an indigent population. Diabetes Educ. 2009, 35, 622–630. [Google Scholar] [CrossRef]
- Remmers, C.; Hibbard, J.; Mosen, D.M.; Wagenfield, M.; Hoye, R.E.; Jones, C. Is patient activation associated with future health outcomes and healthcare utilization among patients with diabetes? J. Ambul. Care Manag. 2009, 32, 320–327. [Google Scholar] [CrossRef]


{kind=link}
| Criteria | Sukala et al. 2012 [10] | Sukala et al. 2013 [11] | Shah et al. 2015 [12] |
|---|---|---|---|
| MMAT | |||
| Total (%) | 40% | 40% | 80% |
| Rating | Medium | Medium | High |
| CET | |||
| Issue Identified by the Community | 0 | 0 | 1 |
| Indigenous Governance | 0 | 0 | 0 |
| Capacity Building | 0 | 0 | 1 |
| Cultural Consideration in Design | 1 | 1 | 1 |
| Respecting Community Experience | 1 | 1 | 1 |
| Total/5 | 2 | 2 | 4 |
| Rating | Moderate | Moderate | Strong |
| Reference (Author, Year) | Aim | Design | Country | Indigenous Population | Program | Participants | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Included (n) | Completed (n) | Sex (%) | Age (Years) | Co-Morbidities | ||||||
| (i) Sukala et al., 2012 [10] (ii) Sukala et al., 2013 [11] | (i) To evaluate the effectiveness of two exercise modalities for improving glycosylated hemoglobin (HbA1c) and associated clinical outcomes in Polynesian adults diagnosed with type 2 diabetes and visceral obesity (ii) To evaluate the differential effect of 2, group-based exercise modalities on quality of life (QoL) in indigenous Polynesian peoples with type 2 diabetes (T2DM) and visceral obesity | Randomised parallel arm | New Zealand | Polynesian descent (self-identified): New Zealand Māori (10), Cook Islands Māori (3), Samoan (2), Fijian (1), Tokelauan (1), Tongan (1) | Resistance vs. Aerobic Exercise Intervention | n = 26 | n = 18 | F: 72% M: 28% | 49 ± 5 | Visceral Obesity |
| Shah et al., 2015 [12] | To evaluate the use of a novel chronic disease prevention approach for improving clinical outcomes and health-related quality of life in Zuni Indians with chronic disease | Prospective cohort | Zuni Pueblo, New Mexico, USA | Native American ancestry: Zuni Indians | Lifestyle Intervention: group educational classes and home-based teaching, point of care testing, and individualized exercise and nutritional programs | n = 60 | n = 60 | F: 68% M: 32% | 49.4 ± 12.0 | None Reported |
| Reference (Author, Year) | Exercise Type | Exercise Characteristics | Exercise Intensity | Exercise Volume | Length of Intervention | Intervention Compliance | Outcome | |
|---|---|---|---|---|---|---|---|---|
| Biomedical | Psychosocial | |||||||
| (i) Sukala et al., 2012 [10] (ii) Sukala et al., 2013 [11] | Resistance Exercise | Resistance: Eight exercises using machine weights targeting all the major muscle groups of the body: seated leg press, knee extension, knee flexion, chest press, lat pulldown, overhead press, biceps curl, and triceps extension | 2–3 sets of 6–8 repetitions with 1 min rest between sets and exercises. Load increased by 5% when 10 repetitions could be performed | 40–60 min per session 3 sessions per week | 16 weeks | 67 ± 18% | (i) HbA1c (%), HOMA2-IR index, McAuley index, Glucose (mmol/L), Insulin (pmol/L), C-peptide, Free fatty acids (mEq/L), Log C-reactive protein, Adiponectin, Blood Lipids (mmol/L): Total cholesterol, HDL cholesterol, LDL cholesterol, Triglycerides, Body weight (kg), BMI (kg/m2), Waist circumference (cm), Body fat (%), SBP & DBP | (ii) Quality of life: Medical Outcomes Trust Short Form-36 Health Survey (v. 1.0) (SF-36) |
| Aerobic Exercise | Aerobic: Exercises on a cycle ergometer | First 2 weeks: progression from 65% to 85% of participants heart rate reserve (HRR) Remaining program: 85% of HRR | 73 ± 19% | |||||
| Shah et al., 2015 [12] | Walking Program Aerobic Exercise | Exercise in addition to normal activity within peer groups of 4–6 individuals: walking at least 3× weekly (on their own or within CHR organised walking groups), and optional additional aerobic exercise at Zuni Health Facility | Not Reported | 150 min weekly 3× weekly (walking) | 6 months | 100% | A1c%, Glucose(mg/dL), Total Cholestrol (mg/dL), Triglyceride (mg/dL) Blood Urea Nitrogen/BUN (mg/dL), Creatinine (mg/dL), Urine Albumin-to-Creatinine ratio/UACR (mg ALB/g CR), Uric Acid (mg/dL), BMI | PAM levels: Patient Activation Measure (PAM)-short form PAM questionnaire |
| Author | Year | Group | HbA1c (%) | Glucose (mmol/L) | Total Cholesterol (mmol/L) | BMI (kg/m2) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | % Change | p Value | Pre | Post | % Change | p Value | Pre | Post | % Change | p Value | Pre | Post | % Change | p Value | |||
| Sukala et al. | 2012 [10] | RET | 10.7 ± 2.1 | 10.6 ± 2.4 | −0.1 ± 1.1 | 0.86 | 9.5 ± 3.5 | 11.4 ± 4 | 1.9 ± 3.2 | 0.17 | 4.9 ± 1.5 | 4.5 ± 1 | −0.4 ± 0.9 | 0.21 | 42.7 ± 12.1 | 42.7 ± 11.7 | 0.0 ± 1.1 | 0.91 |
| AET | 8.9 ± 1.9 | 8.8 ± 2.1 | −0.1 ± 0.6 | 0.6 | 10.2 ± 3.3 | 10.4 ± 2.9 | 0.2 ± 1.6 | 0.72 | 4.5 ± 0.4 | 4.7 ± 0.4 | 0.3 ± 0.6 | 0.22 | 45 ± 6.5 | 44.5 ± 6.9 | −0.5 ± 1.3 | 0.32 | ||
| Shah et al. | 2015 [12] | 8.12 ± 2.16 | 7.39 ± 1.6 | Not Reported | 0.001 | 8.8 ± 3.9 | 7.5 ± 2.5 | Not Reported | 0.0003 | 4.1 ± 1.0 | 3.8 ± 0.8 | Not Reported | 0.003 | 33.8 ± 8.4 | 32.4 ± 8.2 | Not Reported | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurst, L.; Kirwan, M.; Christie, V.; Cross, C.; Baylis, S.; White, L.; Gwynne, K. The Effect of Community-Based Exercise on Health Outcomes for Indigenous Peoples with Type 2 Diabetes: A Systematic Review. Int. J. Environ. Res. Public Health 2024, 21, 290. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph21030290
Hurst L, Kirwan M, Christie V, Cross C, Baylis S, White L, Gwynne K. The Effect of Community-Based Exercise on Health Outcomes for Indigenous Peoples with Type 2 Diabetes: A Systematic Review. International Journal of Environmental Research and Public Health. 2024; 21(3):290. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph21030290
Chicago/Turabian StyleHurst, Lauren, Morwenna Kirwan, Vita Christie, Cara Cross, Sam Baylis, Liam White, and Kylie Gwynne. 2024. "The Effect of Community-Based Exercise on Health Outcomes for Indigenous Peoples with Type 2 Diabetes: A Systematic Review" International Journal of Environmental Research and Public Health 21, no. 3: 290. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph21030290