
Evolution of Public Health Human Papillomavirus Immunization Programs in Canada

 ,
,
Abstract
:1. Introduction
2. Methods
3. Data Analysis
4. Ethics Approval
5. Results
5.1. Evolution of Public HPV Vaccination Programs
5.2. HPV Vaccination Coverage Rates in School-Based Programs
6. Discussion
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forman, D.; De Martel, C.; Lacey, C.J.; Soerjomataram, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global Burden of Human Papillomavirus and Related Diseases. Vaccine 2012, 30, F12–F23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burd, E.M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens—Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef]
- Smith, M. HPV related cancers: Tip of a very large iceberg! J. Fam. Pract. Oncol. 2017, 29, 1. [Google Scholar]
- Saraiya, M.; Steben, M.; Watson, M.; Markowitz, L. Evolution of cervical cancer screening and prevention in United States and Canada: Implications for public health practitioners and clinicians. Prev. Med. 2013, 57, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, G.K.; Guichon, J.; Kelaher, M. Canadian school-based HPV vaccine programs and policy considerations. Vaccine 2017, 35, 5700–5707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C.; Smith, S.R. Examining Provincial HPV Vaccination Schemes in Canada: Should We Standardise the Grade of Vaccination or the Number of Doses? Int. Sch. Res. Not. 2015, 2015, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.; Baines, N.; Memon, S.; Fitzgerald, N.; Chadder, J.; Politis, C.; Nicholson, E.; Earle, C.; Bryant, H. Moving toward the elimination of cervical cancer: Modelling the health and economic benefits of increasing uptake of human papillomavirus vaccines. Curr. Oncol. 2019, 26, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, G.K.; Perez, S.; Rosberger, Z. Including males in Canadian human papillomavirus vaccination programs: A policy analysis. Can. Med. Assoc. J. 2016, 188, 881–886. [Google Scholar] [CrossRef] [Green Version]
- BC Centre for Disease Control. Immunization Uptake in Grade 6 Students; BC Centre for Disease Control: Vancouver, BC, Canada, 2018. [Google Scholar]
- Government of Saskatchewan. Vaccine Preventable Disease Monitoring Report: Human Papillomavirus, 2017; Population Health Branch: Regina, SK, Canada, 2018. [Google Scholar]
- Ontario Agency for Health Protection and Promotion (Public Health Ontario). Immunization Coverage Report for School Pupils: 2016–17 School Year; Queen’s Printer for Ontario: Toronto, ON, Canada, 2018. [Google Scholar]
- New Brunswick Department of Health. Daycare, School Entry, and School Program Immunization Report. Data for School Year 2017/18; New Brunswick Department of Health: Fredericton, NB, Canada, 2018. [Google Scholar]
- Alberta Health. Interactive Health Data Application 2019. Available online: http://www.ahw.gov.ab.ca/IHDA_Retrieval/ihdaData.do (accessed on 29 August 2019).
- Prince Edward Island Provincial Immunization Committee Chief Public Health Office. Childhood Immunization in PEI 2017. Available online: https://www.princeedwardisland.ca/sites/default/files/publications/childhoodreportfinal.pdf (accessed on 4 September 2019).
- Government of Quebec. Flash Vigie Bulletin Quebecois de Vigie, de Surveillance et D’intervention en Protection de la sante Publique; Government of Quebec: Montréal, QC, Canada, 2015; pp. 1–3. [Google Scholar]
- Prince Edward Island. Human Papillomavirus (HPV) Vaccine (Gardasil® 9) 2018. Available online: https://www.princeedwardisland.ca/en/information/health-and-wellness/human-papillomavirus-hpv-vaccine-gardasilr-9 (accessed on 4 September 2019).
- Newfoundland Labrador. Communicable Disease Report; Newfoundland Labrador Health and Community Services: St. John’s, NL, Canada, 2015. [Google Scholar]
- Canadian Partnership Against Cancer. The 2016 Cancer System Performance Report; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2016. [Google Scholar]
- Canadian Partnership Against Cancer. The 2018 Cancer System Performance Report; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2018. [Google Scholar]
- Canadian Immunization Committee. Recommendations for Human Papillomavirus Immunization Programs; Public Health Agency of Canada: Ottawa, ON, Canada, 2014. [Google Scholar]
- Prince Edward Island Population Health Assessment and Surveillance. Immunization Uptake in Grade 6—2017/18; Prince Edward Island Provincial Immunization Committee: Charlottetown, PE, Canada, 2019. [Google Scholar]
- BC Centre for Disease Control. Immunization Uptake in Grade 6 Students; BC Centre for Disease Control: Vancouver, BC, Canada, 2019; p. 20. [Google Scholar]
- New Brunswick Department of Health. Daycare, School Entry, and School Program Immunization Report. Data for School Year 2018/19; New Brunswick Department of Health: Fredericton, NB, Canada, 2019. [Google Scholar]
- Government of Quebec. Flash Vigie Bulletin Quebecois de Vigie, de Surveillance et D’intervention en Protection de la sante Publique; Government of Quebec: Montreal, QC, Canada, 2017; pp. 1–4.
- Community Health Programs Yukon Immunization Program. Yukon Immunization Program Manual; Government of Yukon, Yukon Immunization Program: Whitehorse, YT, Canada, 2019.
- BC Centre for Disease Control. Immunize BC: Progress Report: April 1, 2007–March 31, 2012; Ministry of Health: Victoria, BC, Canada, 1 April 2012.
- Alberta Health Services. Human Papillomavirus 9-Valent Vaccine Biological Page; Alberta Health Services: Calgary, AB, Canada, 2019. [Google Scholar]
- Dawar, M.; Harris, M.T.; McNeil, S.; Naci, A.B. Update on Human Papillomavirus (HPV) Vaccines. Can. Commun. Dis. Rep. 2012, 38, 1–62. [Google Scholar] [CrossRef]
- Manitoba Health. Manitoba’s Immunization Program: Vaccines Offered Free-of-Charge (Eligibility Criteria for Publicly-Funded Vaccines) 2019. Available online: http://www.manitoba.ca/health/publichealth/cdc/vaccineeligibility.html (accessed on 2 October 2019).
- BC Centre for Disease Control. Human Papillomavirus Vaccine [Bivalent (Types 16 and 18) Recombinant]: CERVARIX® 2016. Available online: http://www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Guidelines%20and%20Manuals/Epid/CD%20Manual/Chapter%202%20-%20Imms/Part4/HPV2.pdf (accessed on 29 August 2019).
- BC Centre for Disease Control. Immunize BC: Evidence-Based Immunization Information and Tools for B.C. Residents. Available online: https://immunizebc.ca/hpv (accessed on 29 August 2019).
- Nunavut Department of Health. Nunavut Immunization Manual; Nunavut Department of Health: Iqaluit, NU, Canada, 2017. [Google Scholar]
- Nova Scotia Department Health and Wellness. Publicly Funded Vaccine/Immunoglobulin Eligibility Policy 2019. Available online: https://novascotia.ca/dhw/cdpc/documents/Nova_Scotia_Vaccine_Immunoglobin_eligibility.pdf (accessed on 6 November 2019).
- Ontario Agency for Health Protection and Promotion (Public Health Ontario). Human Papillomavirus (HPV) Vaccine; Queen’s Printer for Ontario: Toronto, ON, Canada, 2017. [Google Scholar]
- Nova Scotia Department Health and Wellness. School-Based Immunization Coverage in Nova Scotia, 2016–2017; Nova Scotia Department of Health and Wellness: Halifax, NS, Canada, 2018.
- Government of Quebec. Flash Vigie Bulletin Quebecois de Vigie, de Surveillance et D’intervention en Protection de la Sante Publique; Government of Quebec: Montréal, QC, Canada, 2018; Volume 13, pp. 1–5. [Google Scholar]
- Population Health Branch. Saskatchewan Ministry of Health. Vaccine Preventable Disease Monitoring Report. Human Papillomavirus, 2017; Saskatchewan Ministry of Health: Regina, SK, Canada, 2018.
- Canadian Partnership Against Cancer. Human Papillomavirus (HPV) Vaccination. Available online: https://www.systemperformance.ca/cancer-control-domain/prevention/hpv-vaccination/#!figures (accessed on 29 August 2019).
- Steben, M.; Thompson, M.T.; Rodier, C.; Mallette, N.; Racovitan, V.; DeAngelis, F.; Stutz, M.; Rampakakis, E. A Review of the Impact and Effectiveness of the Quadrivalent Human Papillomavirus Vaccine: 10 Years of Clinical Experience in Canada. J. Obstet. Gynaecol. Can. 2018, 40, 1635–1645. [Google Scholar] [CrossRef] [Green Version]
- Rosberger, Z.; Steben, M.; Norris, T.; McFadyen, A.; Shapiro, G.K. A mixed two-dose vaccination schedule: Not enough evidence to support a policy change in Quebec. Vaccine 2019, 37, 4421. [Google Scholar] [CrossRef]
- Gilca, V.; Sauvageau, C.; Panicker, G.; De Serres, G.; Ouakki, M.; Unger, E.R. Immunogenicity and safety of a mixed vaccination schedule with one dose of nonavalent and one dose of bivalent HPV vaccine versus two doses of nonavalent vaccine—A randomized clinical trial. Vaccine 2018, 36, 7017–7024. [Google Scholar] [CrossRef] [PubMed]
- Franco, E. Quebec’s Mixed Schedule in HPV Vaccination Program—Preamble. Available online: https://www.hpvworld.com/articles/quebec-s-mixed-schedule-in-hpv-vaccination-program-preamble/ (accessed on 27 January 2021).
- Franco, E. Interview Eduardo Franco. Available online: https://www.hpvworld.com/articles/interview-eduardo-fanco/ (accessed on 27 January 2021).
- Government of Canada. Interim Guidance on Continuity of Immunization Programs during the COVID-19 Pandemic. Available online: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/interim-guidance-immunization-programs-during-covid-19-pandemic.html#a6 (accessed on 27 January 2021).
- Canadian Partnership Against Cancer. Action Plan for the Elimination of Cervical Cancer in Canada 2020–2030. Available online: https://s22438.pcdn.co/wp-content/uploads/2020/11/Elimination-cervical-cancer-action-plan-EN.pdf (accessed on 27 January 2021).
- Canadian Immunization Committee. Recommendations on a Human Papillomavirus Immunization Program; Public Health Agency of Canada: Ottawa, ON, Canada, 2007.
- Government of Canada. Vaccination Coverage Goals and Vaccine Preventable Disease Reduction Targets by 2025. 2020. Available online: https://www.canada.ca/en/public-health/services/immunization-vaccine-priorities/national-immunization-strategy/vaccination-coverage-goals-vaccine-preventable-diseases-reduction-targets-2025.html#1.2 (accessed on 27 January 2021).
- Gilbert, N.L.; Gilmour, H.; Dubé, È.; Wilson, S.E.; Laroche, J. Estimates and determinants of HPV non-vaccination and vaccine refusal in girls 12 to 14 y of age in Canada: Results from the Childhood National Immunization Coverage Survey, 2013. Hum. Vaccines Immunother. 2016, 12, 1484–1490. [Google Scholar] [CrossRef]
- Perez, S.; Tatar, O.; Gilca, V.; Shapiro, G.K.; Ogilvie, G.; Guichon, J.R.; Naz, A.; Rosberger, Z. Untangling the psychosocial predictors of HPV vaccination decision-making among parents of boys. Vaccine 2017, 35, 4713–4721. [Google Scholar] [CrossRef]
- Perez, S.; Tatar, O.; Shapiro, G.K.; Dubé, E.; Ogilvie, G.; Guichon, J.; Gilca, V.; Rosberger, Z. Psychosocial determinants of parental human papillomavirus (HPV) vaccine decision-making for sons: Methodological challenges and initial results of a pan-Canadian longitudinal study. BMC Public Health 2016, 16, 1223. [Google Scholar] [CrossRef] [Green Version]
- Tatar, O.; Shapiro, G.K.; Perez, S.; Wade, K.; Rosberger, Z. Using the precaution adoption process model to clarify human papillomavirus vaccine hesitancy in canadian parents of girls and parents of boys. Hum. Vaccines Immunother. 2019, 15, 1803–1814. [Google Scholar] [CrossRef]
- Musto, R.; Siever, J.E.; Johnston, J.C.; Seidel, J.; Rose, M.S.; McNeil, D.A. Social equity in Human Papillomavirus vaccination: A natural experiment in Calgary Canada. BMC Public Health 2013, 13, 640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guichon, J.R.; Mitchell, I.; Buffler, P.; Caplan, A. Citizen intervention in a religious ban on in-school HPV vaccine administration in Calgary, Canada. Prev. Med. 2013, 57, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Bird, Y.; Obidiya, O.; Mahmood, R.; Nwankwo, C.; Moraros, J. Human papillomavirus vaccination uptake in Canada: A systematic review and meta-analysis. Int. J. Prev. Med. 2017, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, L.E.; Tsu, V.; Deeks, S.L.; Cubie, H.; Wang, S.A.; Vicari, A.S.; Brotherton, J.M. Human Papillomavirus Vaccine Introduction—The First Five Years. Vaccine 2012, 30, F139–F148. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.-Y.; Garland, S.M. Human papillomavirus vaccination: The population impact. F1000Research 2017, 6, 866. [Google Scholar] [CrossRef] [Green Version]
- Williams, W.W.; Lu, P.-J.; O’Halloran, A.; Kim, D.K.; Grohskopf, L.A.; Pilishvili, T.; Skoff, T.H.; Nelson, N.P.; Harpaz, R.; Markowitz, L.E.; et al. Surveillance of Vaccination Coverage among Adult Populations—United States, 2015. MMWR. Surveill. Summ. 2017, 66, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.; Quach, S.; Macdonald, S.E.; Naus, M.; Deeks, S.L.; Crowcroft, N.S.; Mahmud, S.M.; Tran, D.; Kwong, J.; Tu, K.; et al. Methods used for immunization coverage assessment in Canada, a Canadian Immunization Research Network (CIRN) study. Hum. Vaccines Immunother. 2017, 13, 1928–1936. [Google Scholar] [CrossRef] [PubMed]




| Province/territory | School Grade of Vaccination | School year | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007/08 | 2008/09 | 2009/10 | 2010/11 | 2011/12 | 2012/13 | 2013/14 | 2014/15 | 2015/16 | 2016/17 | 2017/18 | 2018/19 | |||
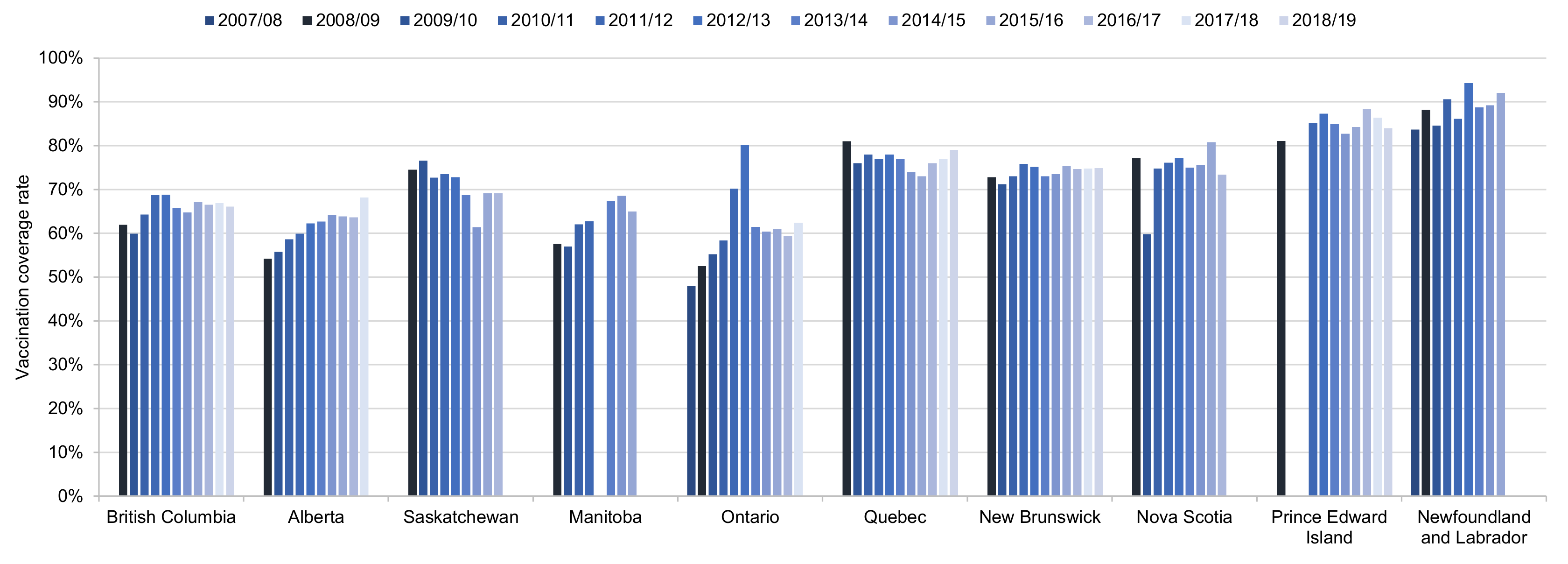
| British Columbia a | Grade 6 | Girls | 61.9% | 59.9% | 64.3% | 68.7% | 68.8% | 65.8% | 64.8% | 67.1% | 66.5% | 66.9% | 66.1% | |
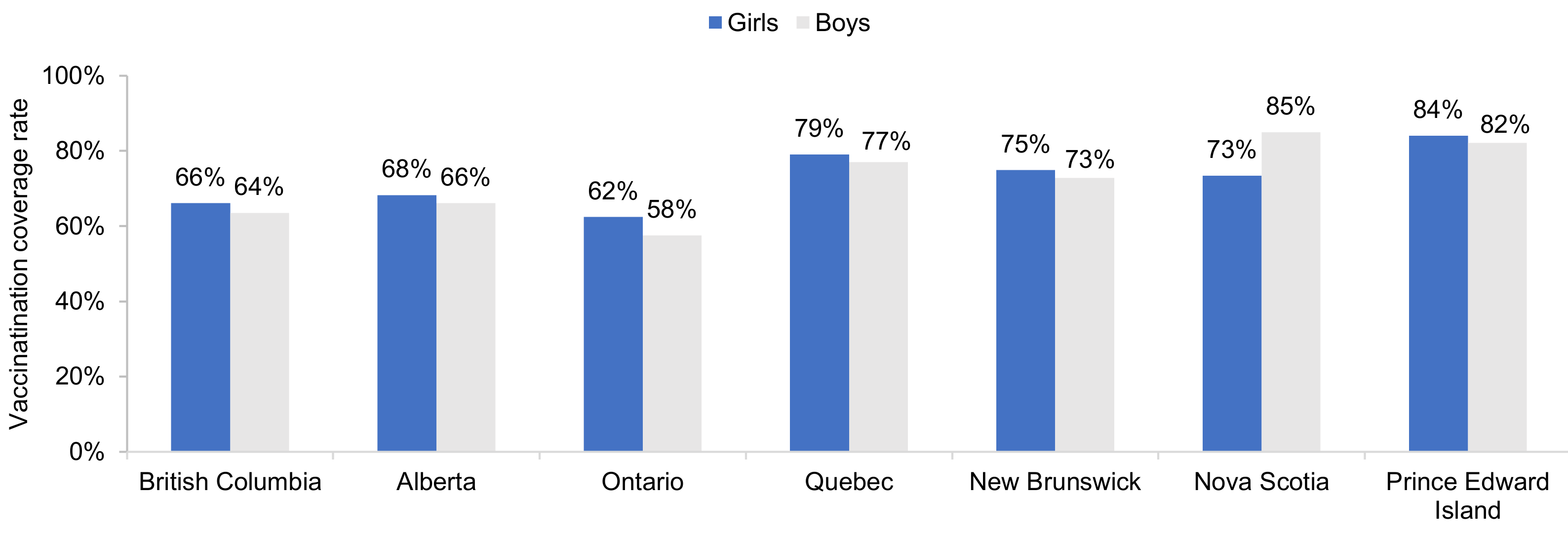
| Boys | 64.6% | 63.5% | ||||||||||||
| Alberta b | Grade 6 | Girls | 54.2% | 55.7% | 58.6% | 59.9% | 62.2% | 62.6% | 64.2% | 63.9% | 63.6% | 68.2% | N/A | |
| Boys | 60.3% | 62.9% | 63.6% | 66.1% | N/A | |||||||||
| Saskatchewan c | Grade 6 | Girls | 74.5% | 76.6% | 72.7% | 73.5% | 72.8% | 68.7% | 61.4% | 69.1% | 69.1% | N/A | N/A | |
| Boys | N/A | N/A | ||||||||||||
| Manitoba d | Grade 6 | Girls | 57.6% | 57.0% | 62.0% | 62.7% | N/A | 67.3% | 68.5% | 65.0% | N/A | N/A | N/A | |
| Boys | N/A | N/A | N/A | |||||||||||
| Ontario e | Grade 7 | Girls | 48.0% | 52.5% | 55.2% | 58.4% | 70.2% | 80.2% | 61.5% | 60.4% | 61.0% | 59.4% | 62.4% | N/A |
| Boys | 53.4% | 57.5% | N/A | |||||||||||
| Quebec f | Grade 4 | Girls | 81.0% | 76.0% | 78.0% | 77.0% | 78.0% | 77.0% | 74.0% | 73.0% | 76.0% | 77.0% | 79.0% | |
| Boys | 72.0% | 74.0% | 77.0% | |||||||||||
| New Brunswick | Grade 7 | Girls | 72.8% | 71.2% | 73.0% | 75.8% | 75.1% | 73.0% | 73.5% | 75.4% | 74.7% | 74.8% | 74.9% | |
| Boys | 70.2% | 72.8% | ||||||||||||
| Nova Scotia g | Grade 7 | Girls | N/A | 77.1% | 59.8% | 74.8% | 76.1% | 77.2% | 75.0% | 75.6% | 80.8% | 73.4% | N/A | N/A |
| Boys | 81.0% | 84.9% | N/A | N/A | ||||||||||
| Prince Edward Island | Grade 6 | Girls | N/A | 81.1% | N/A | N/A | 85.1% | 87.3% | 84.9% | 82.7% | 84.3% | 88.4% | 86.4% | 84.0% |
| Boys | 79.0% | 81.4% | 85.0% | 89.7% | 85.6% | 82.1% | ||||||||
| Newfoundland/Labrador | Grade 6 | Girls | 83.7% | 88.2% | 84.6% | 90.6% | 86.1% | 94.3% | 88.7% | 89.2% | 92.0% | N/A | N/A | N/A |
| Boys | N/A | N/A | ||||||||||||
| Yukon | Grade 6 | Girls | N/A | N/A | N/A | N/A | N/A | N/A | N/A | 66.5% | N/A | N/A | ||
| Boys | N/A | N/A | ||||||||||||
| Northwest Territories h | Grades 4–6 | Girls | N/A | N/A | N/A | N/A | 39.3% | N/A | 55.0% | N/A | N/A | N/A | ||
| Boys | N/A | N/A | ||||||||||||
| Nunavut i | Grade 6 | Girls | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |||
| Boys | N/A | N/A | ||||||||||||
 Three doses 4vHPV;
Three doses 4vHPV;  Two doses 4vHPV;
Two doses 4vHPV;  Three doses 9vHPV;
Three doses 9vHPV;  Two doses 9vHPV;
Two doses 9vHPV;  9vHPV + 2vHPV; N/A, not available. a In 2010, the British Columbia program schedule changed. Girls in Grade 6 in 2010/11 were vaccinated with two doses and received their 3rd and final dose in Grade 9. Girls in Grade 6 in 2011/12 to 2013/14 were scheduled to receive their 3rd dose in Grade 9, but the HPV program changed to two doses in 2014 and, therefore, these girls never received their 3rd dose. b In 2018, the Alberta program schedule changed from Grade 5 to Grade 6. Vaccination was in Grade 5 from 2008/09 to 2017/2018 and moved to Grade 6 in 2018/19. In 2018, the cohort in Grade 6 had already received the vaccine in Grade 5; therefore, no primary cohort was vaccinated for the school year 2018/19. Of note, Alberta reports coverage rates based on school year grade only since 2017/18 school year. Therefore, from 2008/09 to 2016/17, coverage rates were calculated based on 3 doses by age of 12; coverage rate might not be comparable year to year. c In Saskatchewan, vaccination coverage rates are calculated based on age cohorts and not on school grades. Therefore, the coverage rate of a given cohort is available only once they reach a certain age (i.e., 13, 15, or 17 years old). For example, for the cohort vaccinated in Grade 6 in 2016/17, the coverage rate is only available once they reach 13 years old, two years later, in 2018 (assuming they were aged of 11 years old at the time of the vaccine). For cohorts vaccinated in 2008/09 and 2009/10, calculations were based on 3 doses by the age of 15 as these were the only rates available for those cohorts. For cohorts vaccinated in 2010/11 to 2014/15, calculations were based on 3 doses by the age of 13, and for cohorts vaccinated in 2015/16 and 2016/17, calculations were based on 2 doses by the age of 13. d In Manitoba, vaccination coverage rates are calculated based on age cohorts (i.e., 13 and 17 years old). For cohorts vaccinated from 2008/09 to 2011/12, vaccination coverage rates were calculated at age 17, and for cohorts vaccinated from 2013/14 to 2015/16, vaccination coverage rates were calculated at age 13. e In 2016, the Ontario program schedule changed. Vaccination was in Grade 8 from 2007/08 to 2015/16 for females and moved to Grade 7 in 2016/17. As of 2018/19, the coverage rate reported by Ontario combined girls and boys and was 57.9%. f From 2008/09 to 2012/13, in Quebec, girls in Grade 4 received two doses of the 4vHPV and were scheduled to receive their 3rd dose in Grade 9. The program changed to two-dose in 2013 and, therefore, girls in Quebec never received the 3rd dose. In 2018, Quebec moved from 2 doses of the 9vHPV vaccine to a mixed vaccination schedule with one dose of the 9vHPV vaccine and one dose of the 2vHPV vaccine g In 2009/10, the Nova Scotia Public Health department was responding to the H1N1 flu pandemic and resources were only available to conduct immunization clinics for one grade level. Therefore, in the 2009/10 school year, Grade 10 students were immunized, and in 2010/11, Grades 7 and 8 were immunized. h Although Northwest Territories vaccinate girls in Grades 4–6, coverage estimates are conducted in Grade 7. Assume that vaccination was switched to two-dose vaccination schedule in 2016/17 based on Merck & Co., Inc., Kenilworth, NJ, USA, internal data. Some individuals may have received three doses. i Nunavut program was implemented in March 2010. Assume that vaccination was switched to two-dose vaccination schedule in 2016/17 based on Merck & Co., Inc., Kenilworth, NJ, USA, internal data. Some individuals may have received three doses. Sources: Provincial health authorities [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26].
9vHPV + 2vHPV; N/A, not available. a In 2010, the British Columbia program schedule changed. Girls in Grade 6 in 2010/11 were vaccinated with two doses and received their 3rd and final dose in Grade 9. Girls in Grade 6 in 2011/12 to 2013/14 were scheduled to receive their 3rd dose in Grade 9, but the HPV program changed to two doses in 2014 and, therefore, these girls never received their 3rd dose. b In 2018, the Alberta program schedule changed from Grade 5 to Grade 6. Vaccination was in Grade 5 from 2008/09 to 2017/2018 and moved to Grade 6 in 2018/19. In 2018, the cohort in Grade 6 had already received the vaccine in Grade 5; therefore, no primary cohort was vaccinated for the school year 2018/19. Of note, Alberta reports coverage rates based on school year grade only since 2017/18 school year. Therefore, from 2008/09 to 2016/17, coverage rates were calculated based on 3 doses by age of 12; coverage rate might not be comparable year to year. c In Saskatchewan, vaccination coverage rates are calculated based on age cohorts and not on school grades. Therefore, the coverage rate of a given cohort is available only once they reach a certain age (i.e., 13, 15, or 17 years old). For example, for the cohort vaccinated in Grade 6 in 2016/17, the coverage rate is only available once they reach 13 years old, two years later, in 2018 (assuming they were aged of 11 years old at the time of the vaccine). For cohorts vaccinated in 2008/09 and 2009/10, calculations were based on 3 doses by the age of 15 as these were the only rates available for those cohorts. For cohorts vaccinated in 2010/11 to 2014/15, calculations were based on 3 doses by the age of 13, and for cohorts vaccinated in 2015/16 and 2016/17, calculations were based on 2 doses by the age of 13. d In Manitoba, vaccination coverage rates are calculated based on age cohorts (i.e., 13 and 17 years old). For cohorts vaccinated from 2008/09 to 2011/12, vaccination coverage rates were calculated at age 17, and for cohorts vaccinated from 2013/14 to 2015/16, vaccination coverage rates were calculated at age 13. e In 2016, the Ontario program schedule changed. Vaccination was in Grade 8 from 2007/08 to 2015/16 for females and moved to Grade 7 in 2016/17. As of 2018/19, the coverage rate reported by Ontario combined girls and boys and was 57.9%. f From 2008/09 to 2012/13, in Quebec, girls in Grade 4 received two doses of the 4vHPV and were scheduled to receive their 3rd dose in Grade 9. The program changed to two-dose in 2013 and, therefore, girls in Quebec never received the 3rd dose. In 2018, Quebec moved from 2 doses of the 9vHPV vaccine to a mixed vaccination schedule with one dose of the 9vHPV vaccine and one dose of the 2vHPV vaccine g In 2009/10, the Nova Scotia Public Health department was responding to the H1N1 flu pandemic and resources were only available to conduct immunization clinics for one grade level. Therefore, in the 2009/10 school year, Grade 10 students were immunized, and in 2010/11, Grades 7 and 8 were immunized. h Although Northwest Territories vaccinate girls in Grades 4–6, coverage estimates are conducted in Grade 7. Assume that vaccination was switched to two-dose vaccination schedule in 2016/17 based on Merck & Co., Inc., Kenilworth, NJ, USA, internal data. Some individuals may have received three doses. i Nunavut program was implemented in March 2010. Assume that vaccination was switched to two-dose vaccination schedule in 2016/17 based on Merck & Co., Inc., Kenilworth, NJ, USA, internal data. Some individuals may have received three doses. Sources: Provincial health authorities [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26].| Province/Territory | Cohorts that Were Eligible for School-Based Catch-Up HPV Program | |
|---|---|---|
| Girls | Boys | |
| British Columbia | Catch-up in Grade 9 from 2008/09 to 2010/11 | No catch-up program |
| Alberta | Catch-up in Grade 9 from 2009/10 to 2011/12 | Catch-up in Grade 9 from 2014/15 to 2017/18 |
| Saskatchewan | Catch-up in Grade 7 in 2008/09 | No catch-up program |
| Manitoba | No catch-up program | Catch-up in Grades 8 or 9 from 2016/17 to 2018/19 |
| Ontario | Catch-up in Grade 8 in 2016/17 a | No catch-up program |
| Quebec | Catch-up in Grade 9 from 2008/09 to 2012/13 | Catch-up in Grade 9 from 2018/19 to 2020/21 |
| New Brunswick | Catch-up in Grade 8 in 2008/09 Catch-up in Grade 8 in 2010/11 b | No catch-up program |
| Nova Scotia c | Catch-up in Grade 10 in 2009/10 Catch-up Grade 8 in 2010/11 | No catch-up program |
| Prince Edward Island | No catch-up program | No catch-up program |
| Newfoundland/Labrador | Catch-up in Grade 9 from 2008/09 to 2009/10 | No catch-up program |
| Yukon | Catch-up in Grades 7 and 8 from 2009/10 | No catch-up program |
| Northwest Territories d | Catch-up in Grades 11 and 12 in 2009/10 Catch-up in Grades 10 and 11 in 2010/11 Catch-up in Grades 9 and 10 in 2011/12 Catch-up in Grade 9 from 2012/13 to 2014/15 | No catch-up program |
| Nunavut | No catch-up program | No catch-up program |
| Province/Territory | Birth Year | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1992 | 1993 | 1994 | 1995 | 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | |
| British Columbia | |||||||||||||||||||
| Alberta | |||||||||||||||||||
| Saskatchewan | |||||||||||||||||||
| Manitoba | |||||||||||||||||||
| Ontario | |||||||||||||||||||
| Quebec | |||||||||||||||||||
| New Brunswick | |||||||||||||||||||
| Nova Scotia | |||||||||||||||||||
| Prince Edward Island | |||||||||||||||||||
| Newfoundland/Labrador | |||||||||||||||||||
| Yukon | |||||||||||||||||||
| Northwest Territories | |||||||||||||||||||
| Nunavut | |||||||||||||||||||



{kind=link}
{kind=link}
{kind=link}
| Catch-Up Out of School | MSM | Transgender | HIV | Other High-Risk | |
| British Colombia | Females born ≥ 1994 and males born ≥ 2006 who did not get the vaccine in Grade 6 remain eligible if they start their vaccine series before their 19th birthday and complete it before their 26th birthday. | Males aged 9–26 years who: have sex with other men or are not yet sexually active but are questioning their sexual orientation. | Transgender individuals aged 9–26 years. | HIV positive individuals aged 9–26 years. | Males aged 9–26 years who are street involved. Males aged 9–18 in the care of the Ministry of Children and Family Development. Males of any age who are in youth custody services centres. |
| Alberta | Females and males who were eligible in Grade 6 are eligible up to the age of 26. | Males aged 17–26 years. | Hematopoietic Stem Cell Transplant recipients between the ages of 9 years up to the end of Grade 12. Solid Organ Transplant candidates and recipients between the ages of 9–26 years. | ||
| Saskatchewan | Females born ≥1994 and males born ≥2006 are eligible up to the age of 26. | Individuals aged 9–26 years. | Immunocompromised individuals aged 9–26 years. | ||
| Manitoba | Females born ≥1997 and males born ≥2002. | Males aged 9–26 years who identify as gay or bisexual. | Transgender individuals aged 9–26 years. | Immunocompetent HIV-infected females aged 9–45 years. Immunocompetent HIV-infected males aged 9–26 years. | Females aged 9–45 years and males aged 9–26 years who have congenital or acquired immune deficiencies. Males aged ≤ 18 years who are, or who have ever been, incarcerated.Individuals with recurrent respiratory papillomatosis. Females aged 9–45 years who have a newly diagnosed high-grade cervical histopathology result. Females aged 9–45 years and males aged 9–26 years who are victims of sexual assault. Patients currently under the care of a hematologist or oncologist who have malignant neoplasms or have completed immunosuppressive therapy or hypo- or asplenic. |
| Ontario | Females and males are eligible to initiate or complete the series until the end of their Grade 12 year, if previously eligible for the Grade 7 or 8 programs. | Males ≤ 26 years. | Individuals ≤ 26 years. | ||
| Quebec | Females < 18 years at their first dose. Males who have completed Grade 4 since 2016/17. | Males ≤ 26 years. | Individuals ≤ 26 years. | Males aged 9–17 years who attend rehabilitation centres for youth in difficulty, who are under the care of youth protection services, or who are homeless. Individuals ≤ 26 years who have weakened immune system. | |
| New Brunswick | Females born ≥ 1995 and males born ≥ 2005 are eligible up to the age of 26. | ||||
| Nova Scotia | Females and males who have missed or refused HPV vaccine as part of the school-based program (beginning September 2015 in male) up to and including 18 years of age. | Males ≤ 45 years. | Individuals ≤ 45 years. | ||
| Prince Edward Island | Females and males are eligible if missed HPV immunization in Grade 6 (since 2007 for females and 2012 for males). | All eligible individuals regardless of age. | All eligible individuals regardless of age. | Females aged 18–45 years and males aged 18–26 years who have unprotected sex with multiple partners, a history of genital warts, or an abnormal PAP test (female only). | |
| Newfoundland/ Labrador | Females and males who were eligible in Grade 6 are eligible until the person leave the school system (males in Grade 6 are eligible as of September 2017). | ||||
| Yukon | Females and male who were eligible in Grade 6 (starting in school year 2011/12 in female and in 2017/18 in male).Females up to 18 years of age at time of first dose. | Males ≤ 26 years. | Individuals ≤ 45 years. | Street involved males ≤ 26 years. | |
| Northwest Territories | Females and males are eligible up to the age of 26. | Females and males up to 26 years of age. | |||
| Nunavut | Females and males who would have been in Grade 6 in the 2017/18 school year or later are eligible until Grade 12. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goyette, A.; Yen, G.P.; Racovitan, V.; Bhangu, P.; Kothari, S.; Franco, E.L. Evolution of Public Health Human Papillomavirus Immunization Programs in Canada. Curr. Oncol. 2021, 28, 991-1007. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010097
Goyette A, Yen GP, Racovitan V, Bhangu P, Kothari S, Franco EL. Evolution of Public Health Human Papillomavirus Immunization Programs in Canada. Current Oncology. 2021; 28(1):991-1007. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010097
Chicago/Turabian StyleGoyette, Alexandra, Glorian P. Yen, Voica Racovitan, Parambir Bhangu, Smita Kothari, and Eduardo L. Franco. 2021. "Evolution of Public Health Human Papillomavirus Immunization Programs in Canada" Current Oncology 28, no. 1: 991-1007. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010097