Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
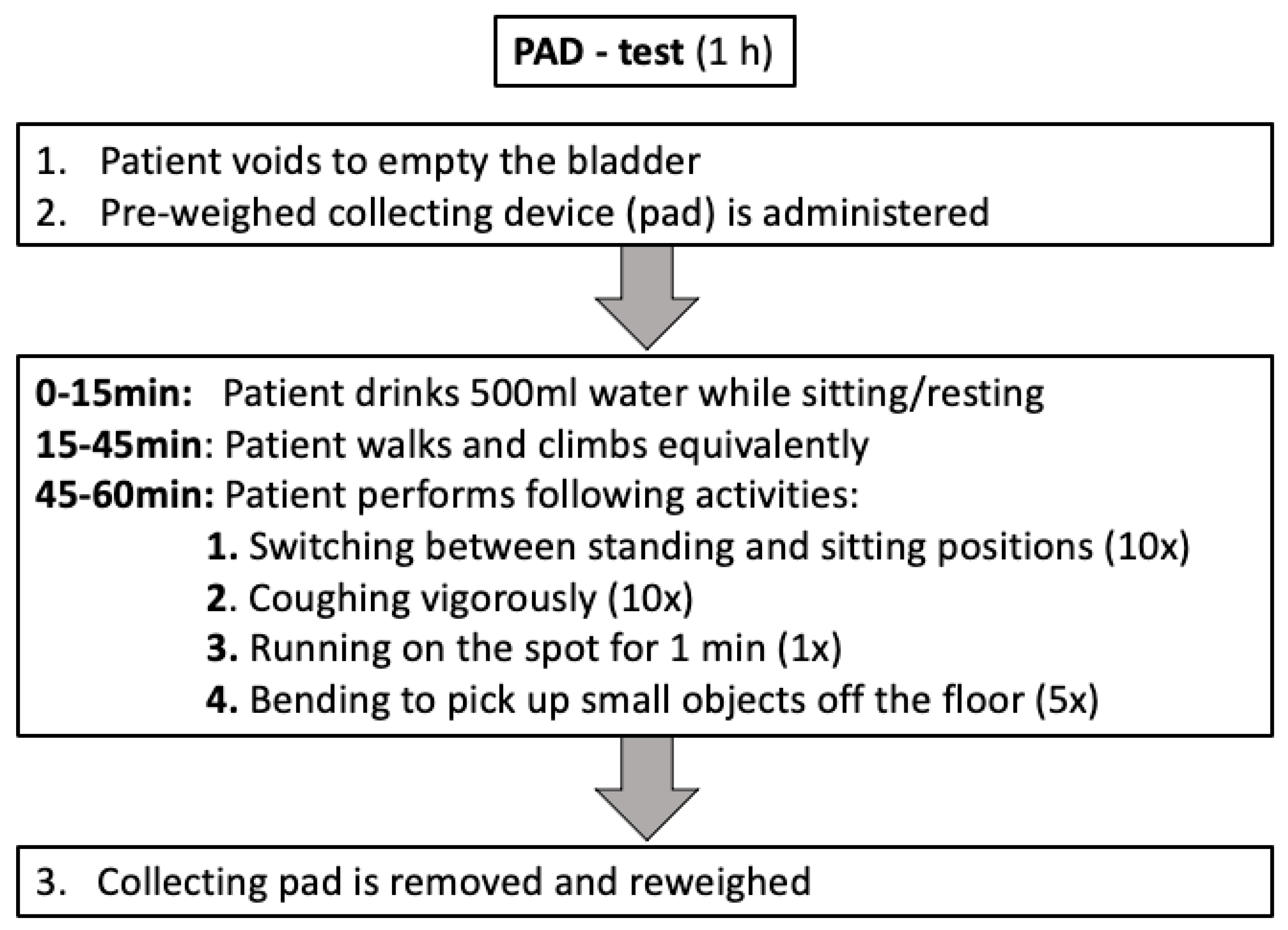
2.2. Outcome Measurements
2.3. Statistical Analyses
3. Results
3.1. Descriptive Characteristics of the Study Population
3.2. Perioperative and Early Continence Outcomes
3.3. Uni-and Multivariable Logistic Regression Models
3.4. Sample Selection Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Expert Patient Advocate (European Prostate Cancer Coalition/Europa UOMO); Santis, M.D.; Gillessen, S.; Grummet, J.; Henry, A.M.; van den Kwast, T.H.; et al. EAU Prostate Cancer Guidelines. Edn. Presented at the EAU Annual Congress Milan 2021; EAU Guidelines Office: Arnhem, The Netherlands, 2021; ISBN 978-94-92671-13-4. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Haese, A.; Knipper, S.; Isbarn, H.; Heinzer, H.; Tilki, D.; Salomon, G.; Michl, U.; Steuber, T.; Budäus, L.; Maurer, T.; et al. A comparative study of robot-assisted and open radical prostatectomy in 10 790 men treated by highly trained surgeons for both procedures. BJU Int. 2019, 123, 1031–1040. [Google Scholar] [CrossRef]
- Pompe, R.S.; Tian, Z.; Preisser, F.; Tennstedt, P.; Beyer, B.; Michl, U.; Graefen, M.; Huland, H.; Karakiewicz, P.I.; Tilki, D. Short- and Long-term Functional Outcomes and Quality of Life after Radical Prostatectomy: Patient-reported Outcomes from a Tertiary High-volume Center. Eur. Urol. Focus 2017, 3, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 13, 1415–1424. [Google Scholar] [CrossRef] [Green Version]
- Wilt, T.J.; Brawer, M.K.; Jones, K.M.; Barry, M.J.; Aronson, W.J.; Fox, S.; Gingrich, J.R.; Wei, J.T.; Gilhooly, P.; Grob, B.M.; et al. Radical Prostatectomy versus Observation for Localized Prostate Cancer. N. Engl. J. Med. 2012, 367, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Hoeh, B.; Preisser, F.; Wenzel, M.; Humke, C.; Wittler, C.; Köllermann, J.; Bodelle, B.; Bernatz, S.; Steuber, T.; Tilki, D.; et al. Feasibility and outcome of radical prostatectomy following inductive neoadjuvant therapy in patients with suspicion of rectal infiltration. Urol. Oncol. Semin. Orig. Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Moore, T.H.; Jameson, C.M.; Davies, P.; Rowlands, M.-A.; Burke, M.; Beynon, R.; Savovic, J.; Donovan, J.L. Symptomatic and quality-of-life outcomes after treatment for clinically localised prostate cancer: A systematic review. BJU Int. 2016, 118, 193–204. [Google Scholar] [CrossRef] [Green Version]
- Borges, R.C.; Tobias-Machado, M.; Gabriotti, E.N.; Dos Santos Figueiredo, F.W.; Bezerra, C.A.; Glina, S. Post-radical prostatectomy urinary incontinence: Is there any discrepancy between medical reports and patients’ perceptions? BMC Urol. 2019, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Ilie, G.; White, J.; Mason, R.; Rendon, R.; Bailly, G.; Lawen, J.; Bowes, D.; Patil, N.; Wilke, D.; Macdonald, C.; et al. Current Mental Distress Among Men with a History of Radical Prostatectomy and Related Adverse Correlates. Am. J. Men’s Health 2020, 14. [Google Scholar] [CrossRef] [PubMed]
- Mandel, P.; Graefen, M.; Michl, U.; Huland, H.; Tilki, D. The effect of age on functional outcomes after radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 203.e11–203.e18. [Google Scholar] [CrossRef]
- Mandel, P.; Kretschmer, A.; Chandrasekar, T.; Nguyen, H.; Buchner, A.; Stief, C.G.; Tilki, D. The effect of BMI on clinicopathologic and functional outcomes after open radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Holm, H.V.; Fosså, S.D.; Hedlund, H.; Schultz, A.; Dahl, A.A. How Should Continence and Incontinence after Radical Prostatectomy be Evaluated? A Prospective Study of Patient Ratings and Changes with Time. J. Urol. 2014, 192, 1155–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ficarra, V.; Novara, G.; Rosen, R.C.; Artibani, W.; Carroll, P.R.; Costello, A.; Menon, M.; Montorsi, F.; Patel, V.R.; Stolzenburg, J.-U.; et al. Systematic Review and Meta-analysis of Studies Reporting Urinary Continence Recovery After Robot-assisted Radical Prostatectomy. Eur. Urol. 2012, 62, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Moschovas, M.C.; Sighinolfi, M.C.; Rocco, B.; Bhat, S.; Onol, F.; Rogers, T.; Patel, V. Balancing the Effects of COVID-19 Against Potential Progression and Mortality in High-risk Prostate Cancer. Eur. Urol. 2020, 78, e14–e15. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Theissen, L.; Wild, P.; Bartelt, K.; Kluth, L.; Köllermann, J.; Graefen, M.; Steuber, T.; Huland, H.; Tilki, D.; et al. Implementation of Intraoperative Frozen Section During Radical Prostatectomy: Short-term Results from a German Tertiary-care Center. Eur. Urol. Focus 2021, 7, 95–101. [Google Scholar] [CrossRef]
- Theissen, L.; Preisser, F.; Wenzel, M.; Humke, C.; Roos, F.C.; Kluth, L.A.; Becker, A.; Banek, S.; Bodelle, B.; Köllermann, J.; et al. Very Early Continence After Radical Prostatectomy and Its Influencing Factors. Front. Surg. 2019, 6, 60. [Google Scholar] [CrossRef] [Green Version]
- Schlomm, T.; Heinzer, H.; Steuber, T.; Salomon, G.; Engel, O.; Michl, U.; Haese, A.; Graefen, M.; Huland, H. Full Functional-Length Urethral Sphincter Preservation During Radical Prostatectomy. Eur. Urol. 2011, 60, 320–329. [Google Scholar] [CrossRef]
- Beyer, B.; Schlomm, T.; Tennstedt, P.; Boehm, K.; Adam, M.; Schiffmann, J.; Sauter, G.; Wittmer, C.; Steuber, T.; Graefen, M.; et al. A Feasible and Time-efficient Adaptation of NeuroSAFE for da Vinci Robot-assisted Radical Prostatectomy. Eur. Urol. 2013, 66, 138–144. [Google Scholar] [CrossRef]
- Spinelli, M.G.; Cozzi, G.; Grasso, A.; Talso, M.; Varisco, D.; El Rahman, D.A.; Acquati, P.; Albo, G.; Rocco, B.; Maggioni, A.; et al. Ralp & Rocco Stitch: Original Technique. Urol. J. 2011, 78, 35–38. [Google Scholar] [CrossRef]
- Hahn, I.; Fall, M. Objective quantification of stress urinary incontinence: A short, reproducible, provocative pad-test. Neurourol. Urodyn. 1991, 10, 475–481. [Google Scholar] [CrossRef]
- RCT. R: A Language and Environment for Statistical Computing. 2017. Available online: https://wwwr-projectorg2017 (accessed on 10 October 2021).
- Harke, N.N.; Wagner, C.; Liakos, N.; Urbanova, K.; Addali, M.; Hadaschik, B.A.; Witt, J.H. Superior early and long-term continence following early micturition on day 2 after robot-assisted radical prostatectomy: A randomized prospective trial. World J. Urol. 2020, 39, 771–777. [Google Scholar] [CrossRef]
- Manfredi, M.; Checcucci, E.; Fiori, C.; Garrou, D.; Aimar, R.; Amparore, D.; De Luca, S.; Bombaci, S.; Stura, I.; Migliaretti, G.; et al. Total anatomical reconstruction during robot-assisted radical prostatectomy: Focus on urinary continence recovery and related complications after 1000 procedures. BJU Int. 2019, 124, 477–486. [Google Scholar] [CrossRef]
- Ates, M.; Teber, D.; Gozen, A.S.; Tefekli, A.; Hruza, M.; Sugiono, M.; Erdogan, S.; Rassweiler, J. A New Postoperative Predictor of Time to Urinary Continence after Laparoscopic Radical Prostatectomy: The Urine Loss Ratio. Eur. Urol. 2007, 52, 178–185. [Google Scholar] [CrossRef]
- Tienza, A.; Akin, Y.; Rassweiler, J.; Gözen, A.S. A match-pair analysis of continence in intermediate and high-risk prostate cancer patients after robot-assisted radical prostatectomy: The role of urine loss ratio and predictive analysis. Prostate Int. 2017, 6, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Park, M.; Pak, S.; Choi, S.-K.; Shim, M.; Song, C.; Ahn, H. Integrity of the Urethral Sphincter Complex, Nerve-sparing, and Long-term Continence Status after Robotic-assisted Radical Prostatectomy. Eur. Urol. Focus 2018, 5, 823–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenzel, M.; Preisser, F.; Mueller, M.; Theissen, L.H.; Welte, M.N.; Hoeh, B.; Humke, C.; Bernatz, S.; Bodelle, B.; Würnschimmel, C.; et al. Effect of prostatic apex shape (Lee types) and urethral sphincter length in preoperative MRI on very early continence rates after radical prostatectomy. Int. Urol. Nephrol. 2021, 53, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Mandel, P.; Preisser, F.; Graefen, M.; Steuber, T.; Salomon, G.; Haese, A.; Michl, U.; Huland, H.; Tilki, D. High Chance of Late Recovery of Urinary and Erectile Function Beyond 12 Months After Radical Prostatectomy. Eur. Urol. 2016, 71, 848–850. [Google Scholar] [CrossRef]
- Lee, J.K.; Assel, M.; Thong, A.E.; Sjoberg, D.D.; Mulhall, J.P.; Sandhu, J.; Vickers, A.J.; Ehdaie, B. Unexpected Long-term Improvements in Urinary and Erectile Function in a Large Cohort of Men with Self-reported Outcomes Following Radical Prostatectomy. Eur. Urol. 2015, 68, 899–905. [Google Scholar] [CrossRef] [Green Version]
- Heesakkers, J.; Farag, F.; Bauer, R.M.; Sandhu, J.; De Ridder, D.; Stenzl, A. Pathophysiology and Contributing Factors in Postprostatectomy Incontinence: A Review. Eur. Urol. 2016, 71, 936–944. [Google Scholar] [CrossRef]
- Massanova, M.; Bada, M.; Crocetto, F.; Barone, B.; Arcaniolo, D.; Silvestri, T.; De Concilio, B.; Zeccolini, G.; Mazzon, G.; Celia, A. Bowel suture technique for bladder neck reconstruction during RALP and its impact on early continence recovery. Minerva Urol. E Nefrol. 2020, 72, 640–641. [Google Scholar] [CrossRef]


{kind=link}
| Study Cohort, (n = 100) | |
|---|---|
| Age in years, Median (IQR) | 65 (58, 69) |
| PSA in mg/mL, Median (IQR) | 8 (6, 12) |
| Body Mass Index in kg/m2, Median (IQR) | 26.1 (24.3, 29.9) |
| International Prostate Symptom Score, Median (IQR) | 6.5 (3, 9) |
| Body Mass Index grouped in kg/m2, n (%) | |
| ≤25 | 33 (34%) |
| 25–30 | 40 (41%) |
| ≥30 | 25 (26%) |
| D’Amico risk classification, n (%) | |
| low | 13 (13%) |
| intermediate | 57 (57%) |
| high | 30 (30%) |
| Surgical approach, n (%) | |
| robotic-assisted RP | 74 (74%) |
| open RP | 26 (26%) |
| Operation time in min, Median (IQR) | 218 (189, 252) |
| Prostate volume in cm3, Median (IQR) | 40 (30, 50) |
| pT-stage, n (%) | |
| pT2a | 6 (6.0%) |
| pT2b | 1 (1.0%) |
| pT2c | 48 (48%) |
| pT3a | 33 (33%) |
| pT3b | 10 (10%) |
| pT4 | 2 (2.0%) |
| Extraprostatic extension of tumor, n (%) | |
| no | 55 (55%) |
| yes | 45 (45%) |
| pN-stage, n (%) | |
| pN0 | 85 (85%) |
| pN1 | 4 (4.0%) |
| pNx | 11 (11%) |
| cM-stage, n (%) | |
| M0 | 96 (96%) |
| M1 | 4 (4.0%) |
| Gleason Grade Group RP-specimen, n (%) | |
| I | 9 (9%) |
| II | 53 (54%) |
| III | 19 (19%) |
| IV | 4 (4%) |
| V | 13 (13%) |
| Nerve sparing, n (%) | |
| none | 7 (7%) |
| uni/bilateral | 93 (93%) |
| Positive surgical margin, n (%) | |
| R0 | 63 (63%) |
| R1 | 34 (34%) |
| Rx | 3 (3%) |
| 0–1(Safety) Pad/24 h | 1–2 Pads/24 h | 3–5 Pads/24 h | >5 Pads/24 h | ||
|---|---|---|---|---|---|
| Urine loss in g, n (%) | |||||
| <1 g | 24 (24.0%) | 21 (87.5%) | 2 (8.3%) | 1 (4.2%) | 0 (0%) |
| 1–10 g | 47 (47.0%) | 29 (61.7%) | 12 (25.6%) | 6 (12.7%) | 0 (0%) |
| 11–50 g | 15 (15.0%) | 6 (40.0%) | 6 (40.0%) | 2 (13.3%) | 1 (6.7%) |
| >50 g | 14 (14.0%) | 3 (21.4%) | 5 (35.7%) | 2 (14.3%) | 4 (28.6%) |
| Logistic Regression Models | ||||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | |||||||
| Odds Ratio | 95%-CI | p-Value | Odds Ratio | 95%-CI | p-Value | |||
| PAD-test urine loss in g | ||||||||
| <1 | Ref. | Ref. | ||||||
| 1–10 | 0.23 | 0.05 | 0.79 | 0.03 | 0.21 | 0.04 | 0.79 | 0.03 |
| 11–50 | 0.10 | 0.02 | 0.43 | 0.004 | 0.09 | 0.01 | 0.48 | 0.008 |
| >50 | 0.04 | 0.01 | 0.20 | <0.001 | 0.03 | 0.004 | 0.18 | <0.001 |
| Age in years | ||||||||
| ≤60 | Ref. | Ref. | ||||||
| 61–69 | 0.49 | 0.17 | 1.30 | 0.16 | 0.42 | 0.13 | 1.28 | 0.14 |
| ≥70 | 0.28 | 0.08 | 0.87 | 0.03 | 0.55 | 0.14 | 2.15 | 0.39 |
| Nerve-sparing approach | ||||||||
| No | Ref. | Ref. | ||||||
| Yes | 3.96 | 0.81 | 28.67 | 0.11 | 1.52 | 0.23 | 13.51 | 0.68 |
| Body Mass Index kg/m2 | ||||||||
| <25 | Ref. | Ref. | ||||||
| 25–30 | 1.55 | 0.60 | 4.02 | 0.36 | 2.04 | 0.66 | 6.56 | 0.22 |
| ≥30 | 1.06 | 0.37 | 3.05 | 0.91 | 1.06 | 0.29 | 3.86 | 0.93 |
| Extraprostatic Extension | ||||||||
| No | Ref. | Ref. | ||||||
| Yes | 0.77 | 0.34 | 1.72 | 0.53 | 1.29 | 0.46 | 3.71 | 0.63 |
| Prostate volume in mL | ||||||||
| ≤40 | Ref. | Ref. | ||||||
| >40 | 1.11 | 0.50 | 2.51 | 0.80 | 0.82 | 0.30 | 2.20 | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeh, B.; Preisser, F.; Wenzel, M.; Humke, C.; Wittler, C.; Hohenhorst, J.L.; Volckmann-Wilde, M.; Köllermann, J.; Steuber, T.; Graefen, M.; et al. Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy. Curr. Oncol. 2021, 28, 4738-4747. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28060399
Hoeh B, Preisser F, Wenzel M, Humke C, Wittler C, Hohenhorst JL, Volckmann-Wilde M, Köllermann J, Steuber T, Graefen M, et al. Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy. Current Oncology. 2021; 28(6):4738-4747. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28060399
Chicago/Turabian StyleHoeh, Benedikt, Felix Preisser, Mike Wenzel, Clara Humke, Clarissa Wittler, Jan L. Hohenhorst, Maja Volckmann-Wilde, Jens Köllermann, Thomas Steuber, Markus Graefen, and et al. 2021. "Correlation of Urine Loss after Catheter Removal and Early Continence in Men Undergoing Radical Prostatectomy" Current Oncology 28, no. 6: 4738-4747. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28060399