
Biomaterials and Adipose-Derived Mesenchymal Stem Cells for Regenerative Medicine: A Systematic Review

 ,
,  ,
, 

Abstract
:1. Introduction
1.1. Biomaterial: The Biological Generation Template
1.2. Stem Cells: Origin, Design and Differentiation
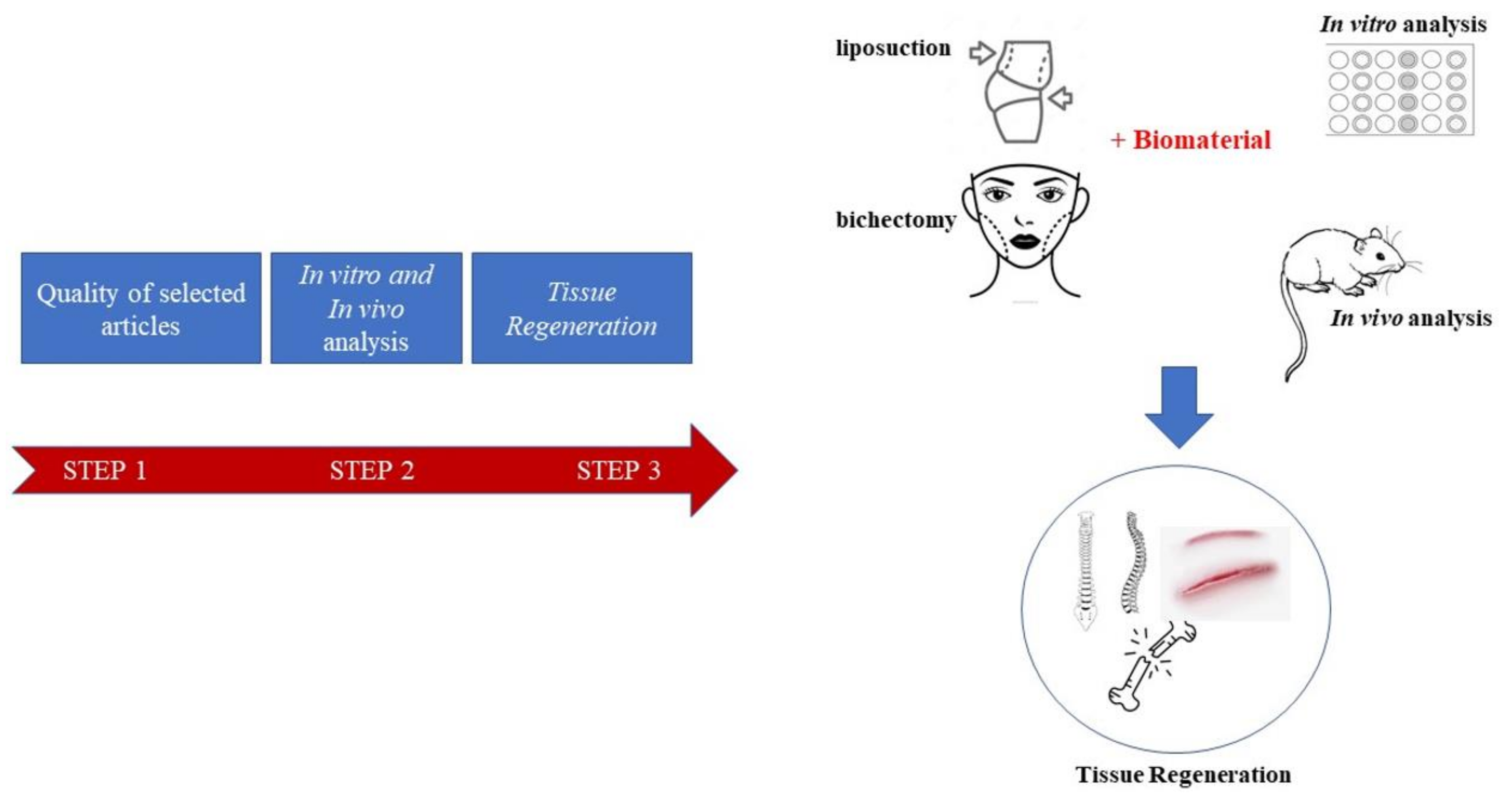
1.3. Our Efforts
2. Materials and Methods
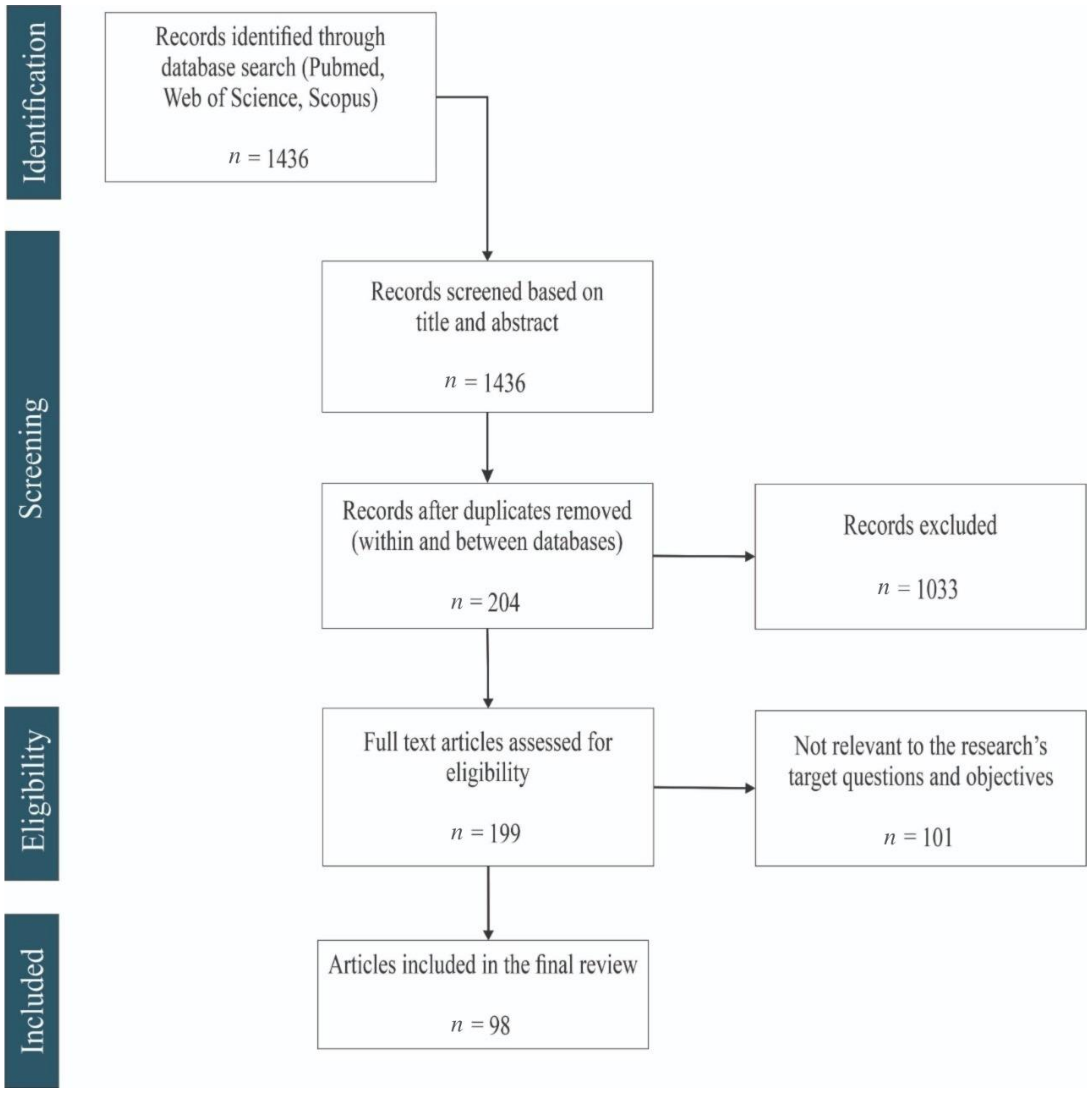
2.1. Literature Search in PubMed, Scopus and Web of Science (Flow Diagram)
2.2. Questions for the Quality Assessment of Retrieved Articles
3. Results
3.1. General Findings (Flow Diagram Results)
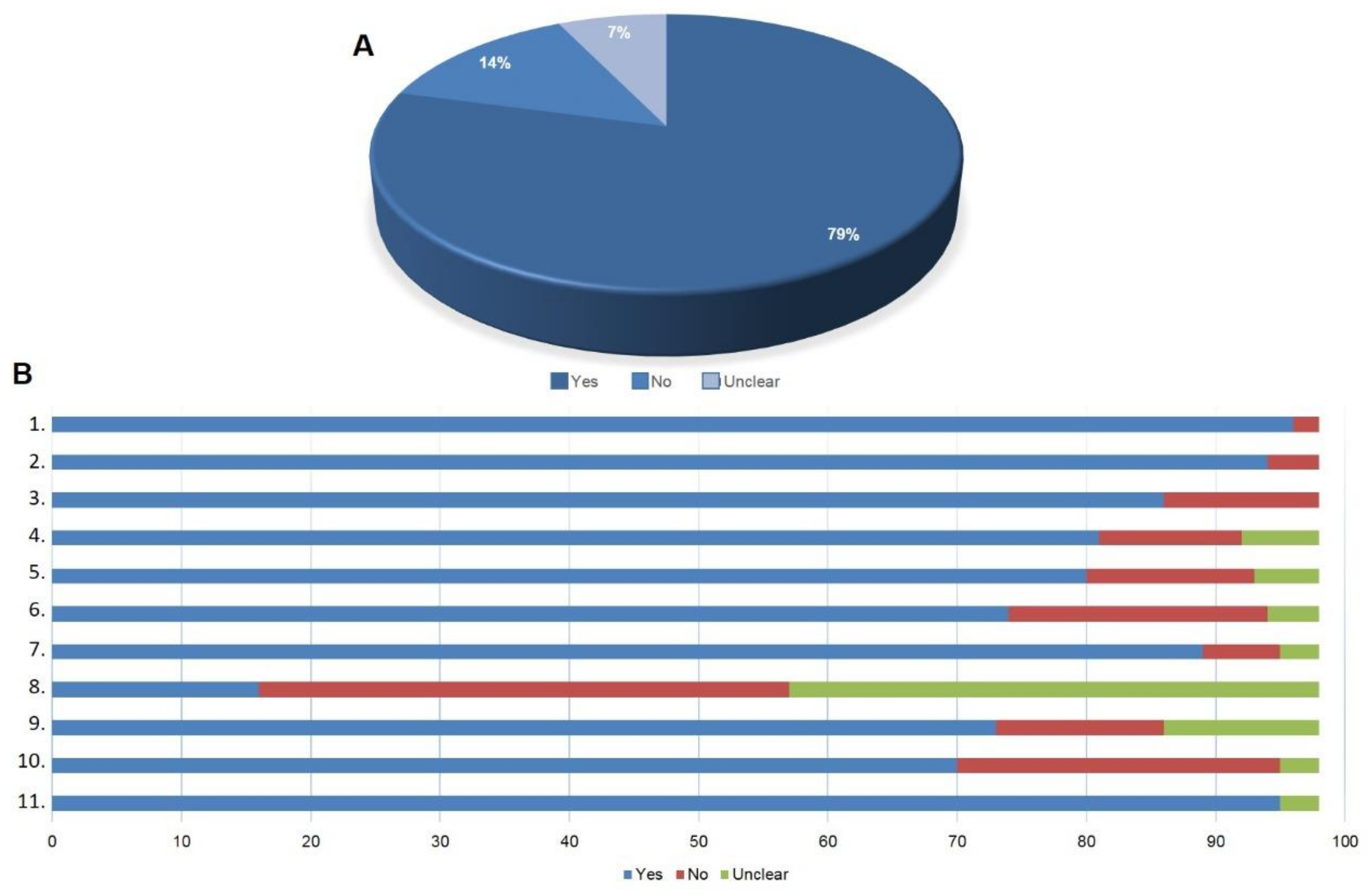
3.2. Quality of the Selected Articles
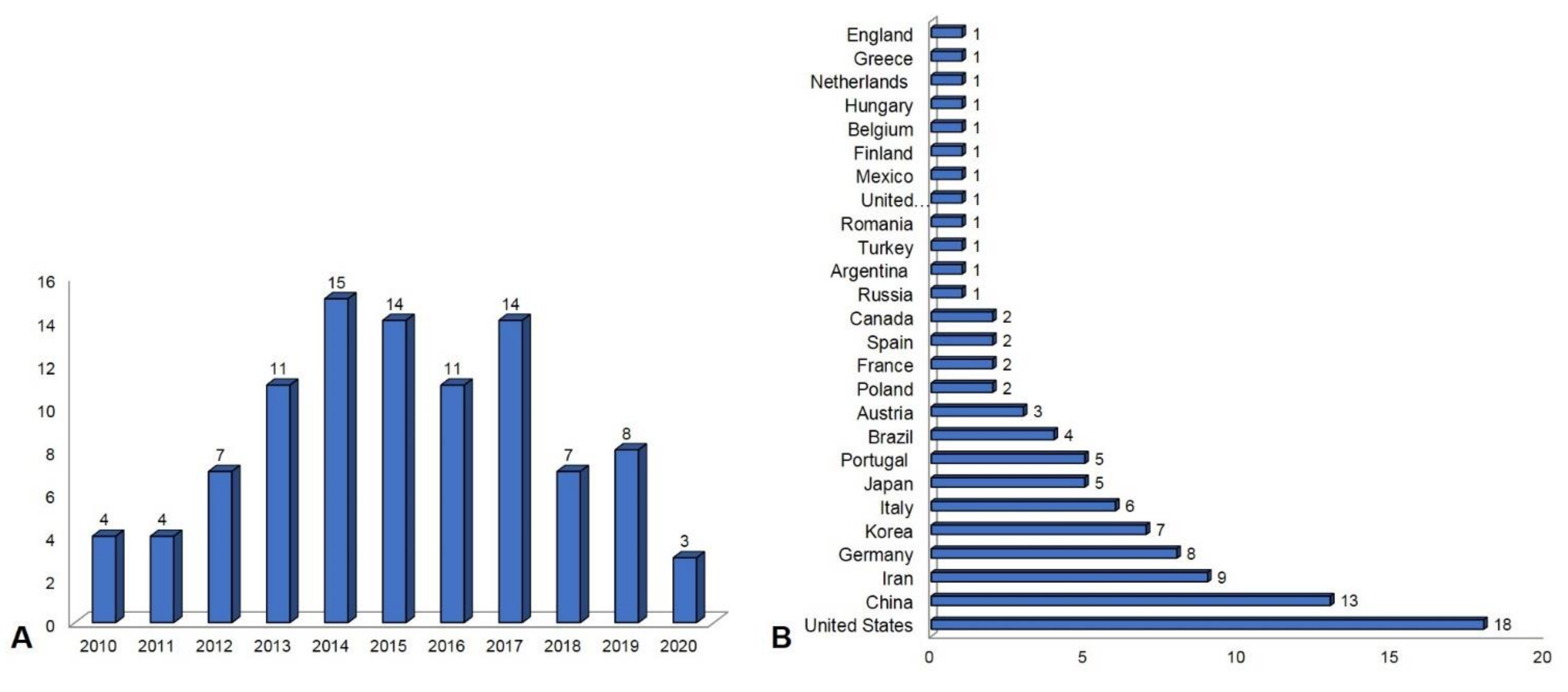
3.3. Publication Overview between 2010 and 2020
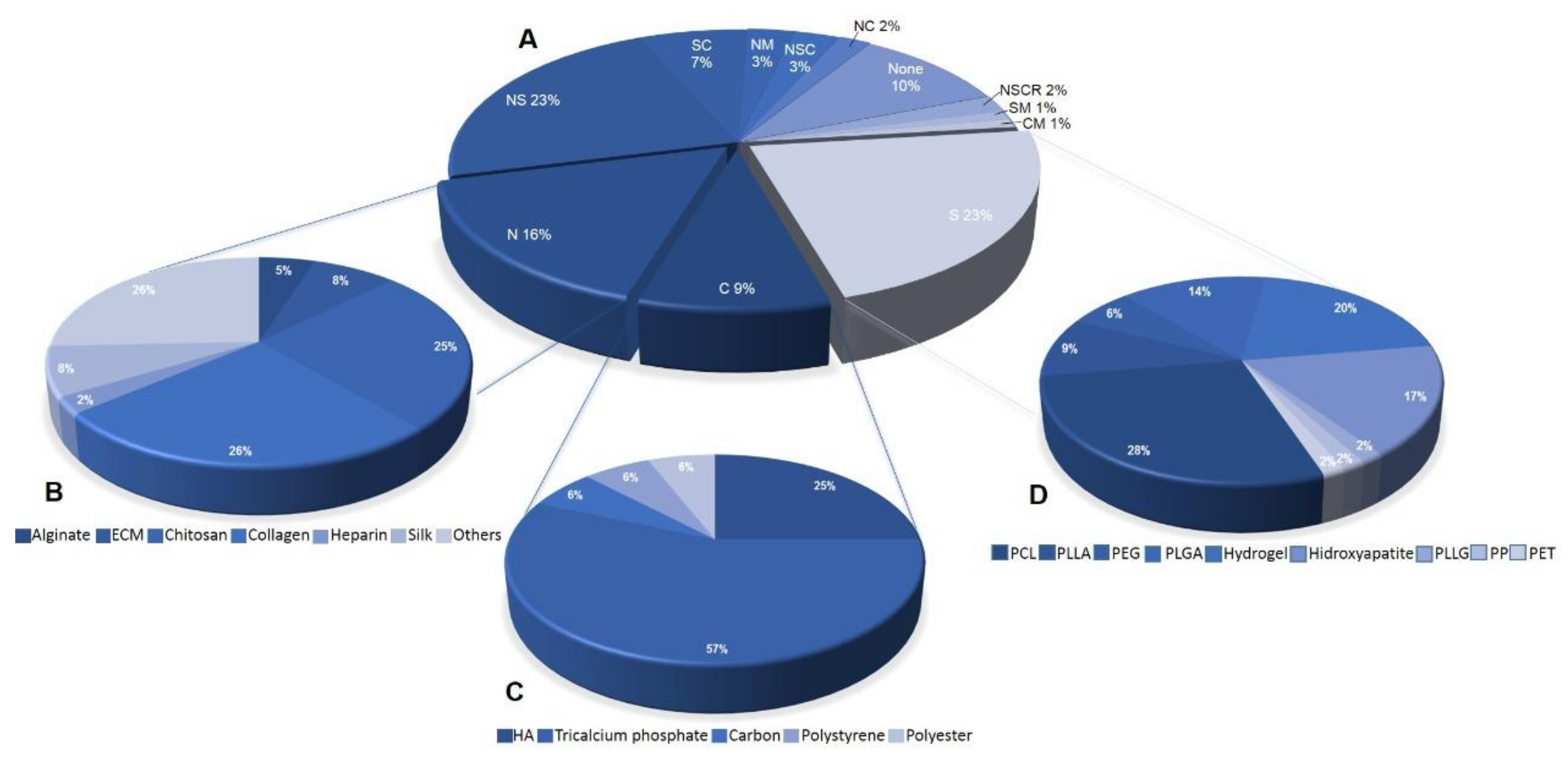
3.4. Biomaterial Used with AD-MSCs for Regenerative Medicine
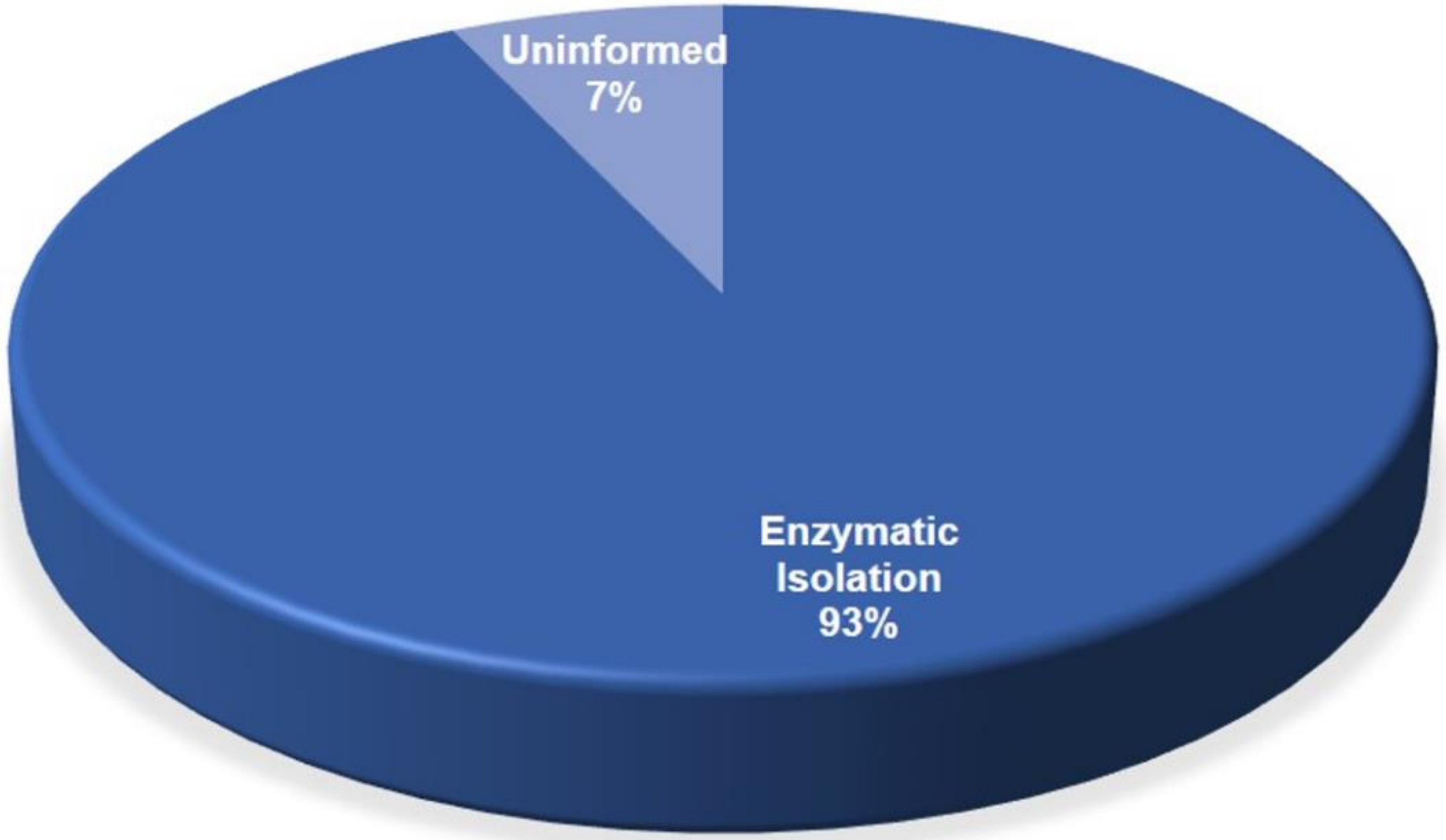
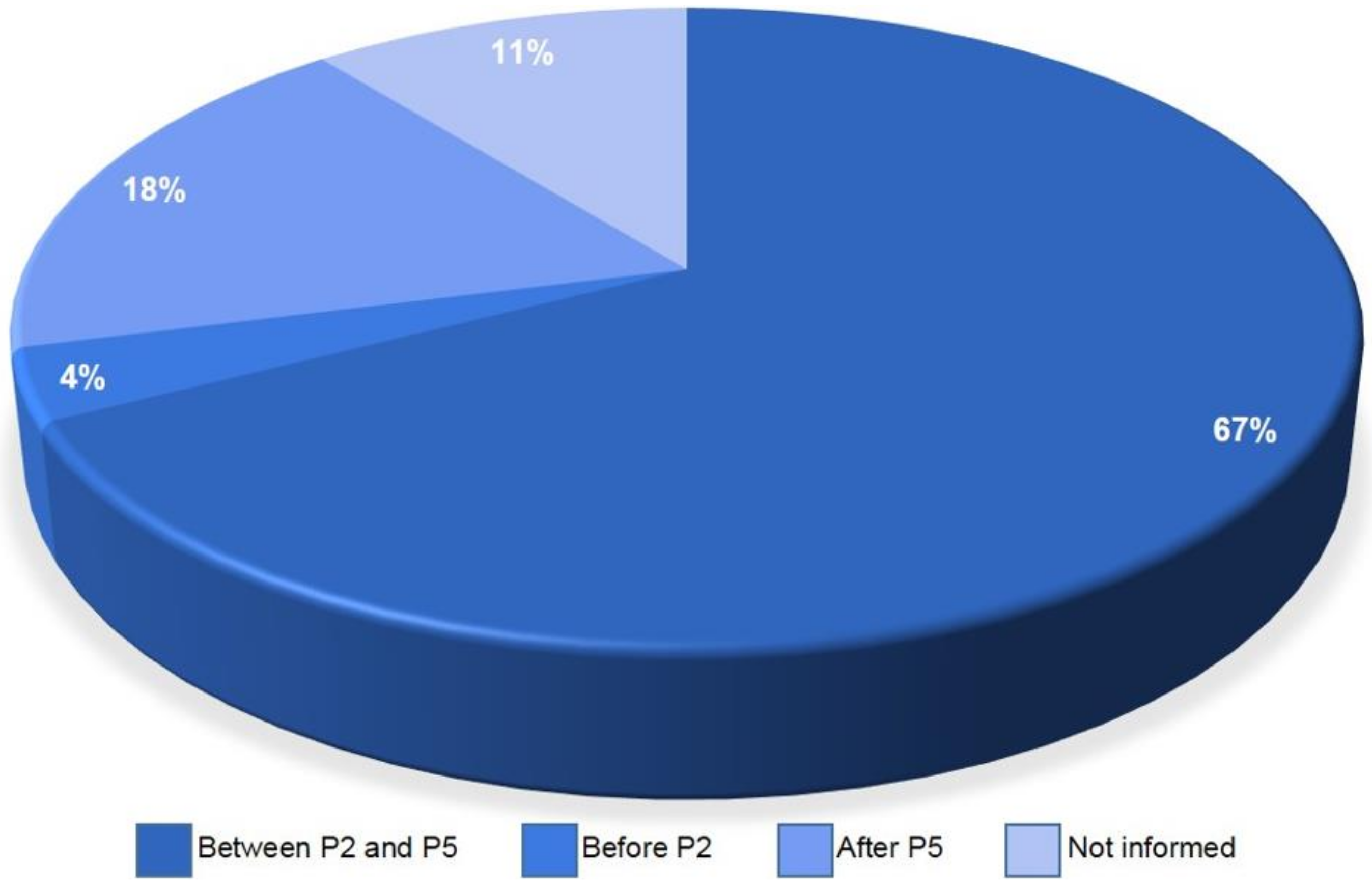
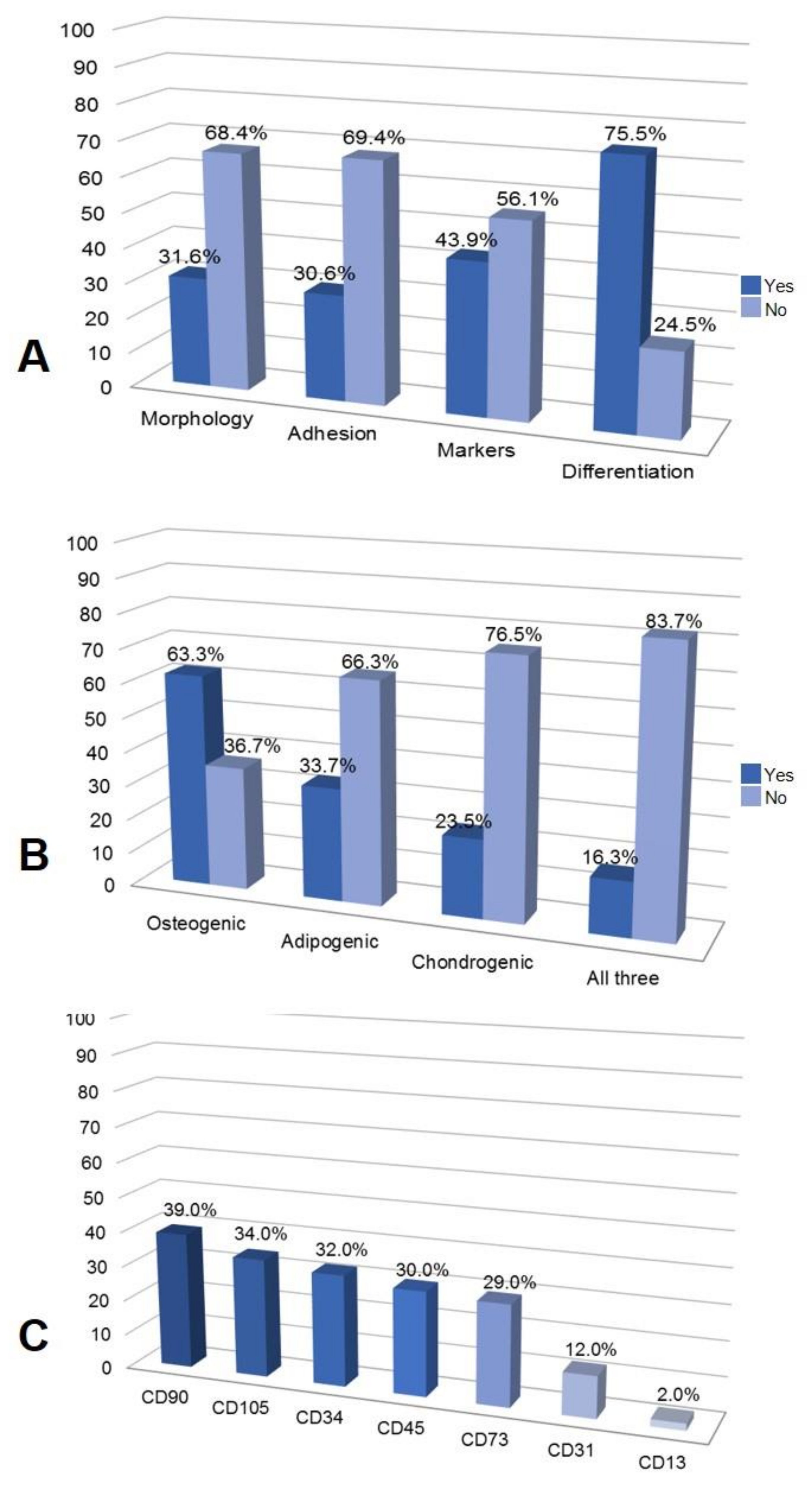
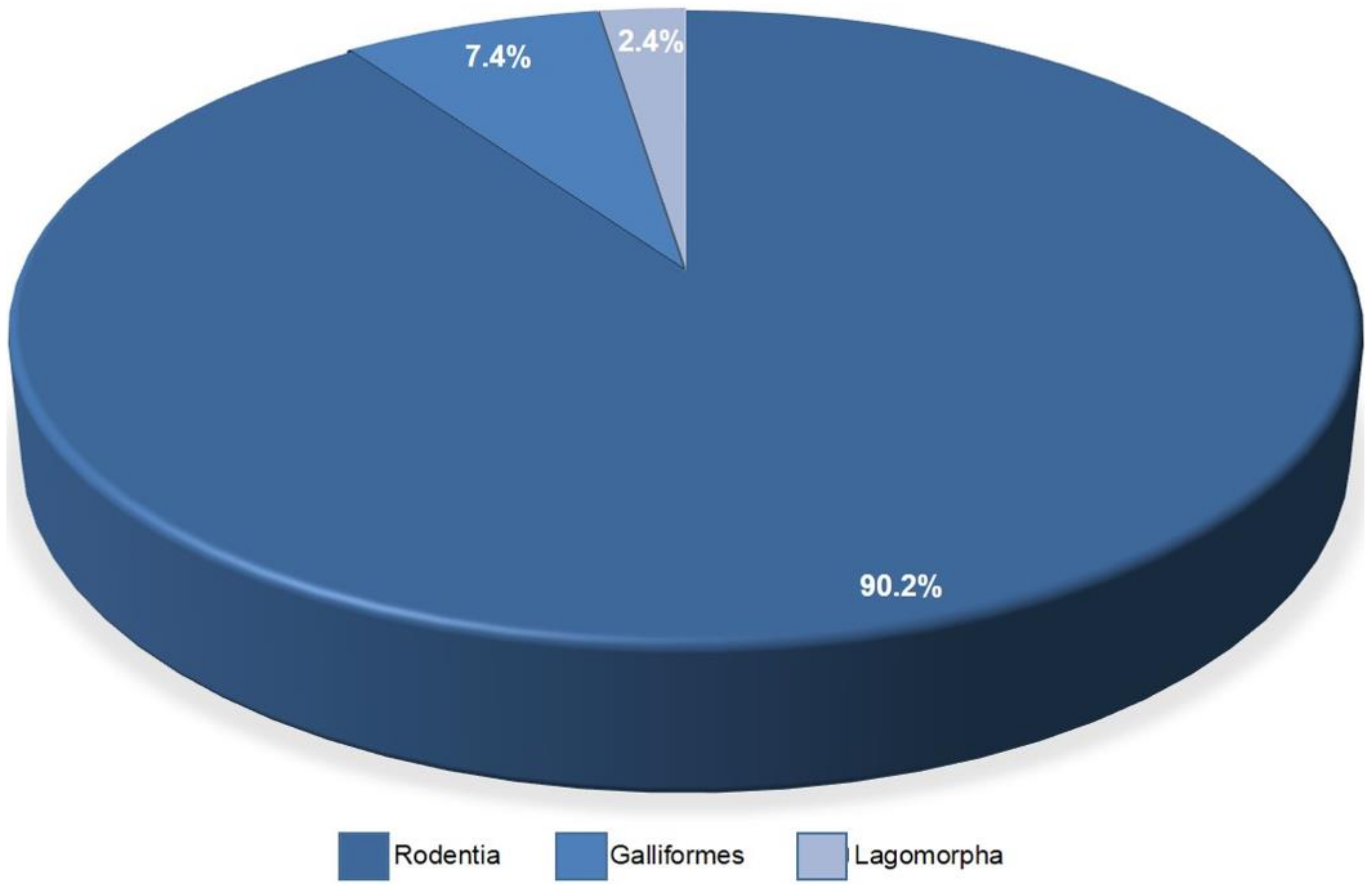
3.5. Adipose Tissue Resources for AD-MSCs Isolation, Culture and Characterization
3.6. In Vitro and In Vivo Assays
3.7. Regenerative Medicine Applications
4. Discussion
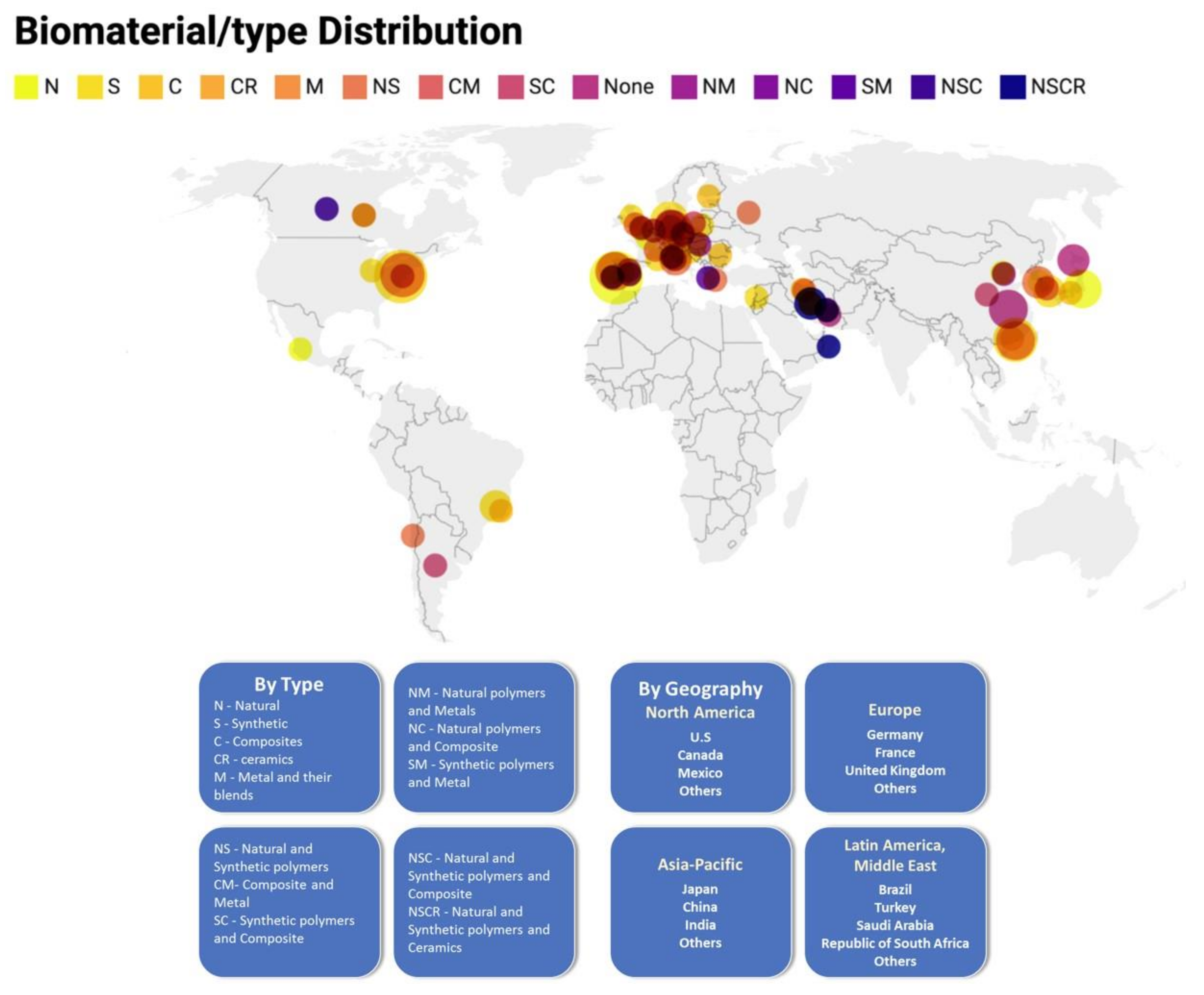
4.1. The United States and China Published More Papers on AD-MSC and Nanomaterials Than Other Research Centers
4.2. Biomaterials Used for Applications in Regenerative Medicine
4.3. AD-MSCs Resources, Isolation, Culture and Characterization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matichescu, A.; Ardelean, L.C.; Rusu, L.-C.; Craciun, D.; Bratu, E.A.; Babucea, M.; Leretter, M. Advanced Biomaterials and Techniques for Oral Tissue Engineering and Regeneration—A Review. Materials 2020, 13, 5303. [Google Scholar] [CrossRef]
- Raghavendra, G.M.; Varaprasad, K.; Jayaramudu, T. Biomaterials. In Nanotechnology Applications for Tissue Engineering; Elsevier: Amsterdam, The Neterlands, 2015; pp. 21–44. [Google Scholar] [CrossRef]
- Solanki, A.; Kim, J.D.; Lee, K.-B. Nanotechnology for regenerative medicine: Nanomaterials for stem cell imaging. Nanomedicine 2008, 3, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Pryjmaková, J.; Kaimlová, M.; Hubáček, T.; Švorčík, V.; Siegel, J. Nanostructured Materials for Artificial Tissue Replacements. Int. J. Mol. Sci. 2020, 21, 2521. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Webster, T.J. Nanotechnology and nanomaterials: Promises for improved tissue regeneration. Nano Today 2009, 4, 66–80. [Google Scholar] [CrossRef]
- Verma, S.; Domb, A.J.; Kumar, N. Nanomaterials for regenerative medicine. Nanomedicine 2011, 6, 157–181. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, S.; Shi, Y.; Galipeau, J.; Krampera, M.; Leblanc, K.; Martin, I.; Nolta, J.; Phinney, D.G.; Sensebe, L. Mesenchymal stem versus stromal cells: International Society for Cell & Gene Therapy (ISCT(R)) Mesenchymal Stromal Cell committee position statement on nomenclature. Cytotherapy 2019, 21, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Harasymiak-Krzyżanowska, I.; Niedojadło, A.; Karwat, J.; Kotuła, L.; Gil-Kulik, P.; Sawiuk, M.; Kocki, J. Adipose tissue-derived stem cells show considerable promise for regenerative medicine applications. Cell. Mol. Biol. Lett. 2013, 18, 479–493. [Google Scholar] [CrossRef]
- Afra, S.; Matin, M.M. Potential of mesenchymal stem cells for bioengineered blood vessels in comparison with other eligible cell sources. Cell Tissue Res. 2020, 380, 1–13. [Google Scholar] [CrossRef]
- Hentze, H.; Soong, P.L.; Wang, S.T.; Phillips, B.W.; Putti, T.C.; Dunn, N.R. Teratoma formation by human embryonic stem cells: Evaluation of essential parameters for future safety studies. Stem Cell Res. 2009, 2, 198–210. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.; McKee, C.; Bakshi, S.; Walker, K.; Hakman, E.; Halassy, S.; Svinarich, D.; Dodds, R.; Govind, C.K.; Chaudhry, G.R. Mesenchymal stem cells: Cell therapy and regeneration potential. J. Tissue Eng. Regen. Med. 2019, 13, 1738–1755. [Google Scholar] [CrossRef]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human mesenchymal stem cells—Current trends and future prospective. Biosci. Rep. 2015, 35. [Google Scholar] [CrossRef]
- Wright, A.; Arthaud-Day, M.L.; Weiss, M.L. Therapeutic Use of Mesenchymal Stromal Cells: The Need for Inclusive Characterization Guidelines to Accommodate All Tissue Sources and Species. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef]
- Salehi-Nik, N.; Rad, M.R.; Kheiri, L.; Nazeman, P.; Nadjmi, N.; Khojasteh, A. Buccal Fat Pad as a Potential Source of Stem Cells for Bone Regeneration: A Literature Review. Stem Cells Int. 2017, 2017, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Cherian, D.S.; Bhuvan, T.; Meagher, L.; Heng, T.S.P. Biological Considerations in Scaling Up Therapeutic Cell Manufacturing. Front. Pharmacol. 2020, 11, 654. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Chen, Y.; Yuan, L.; Liu, H.; Wang, J.; Liu, Q.; Zhang, Y. Adipose-Derived Stem Cells: Current Applications and Future Directions in the Regeneration of Multiple Tissues. Stem Cells Int. 2020, 2020, 1–26. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, version 6.1; John Wiley & Sons: New York, NY, USA, 2019. [Google Scholar]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.L.R.; Bierhalz, A.C.K.; Moraes, A.M. Biomateriais: Tipos, Aplicações e Mercado. Quim. Nova 2015, 38, 957–971. [Google Scholar] [CrossRef]
- Buddy, D.; Ratner, A.; Hoffman, S.; Frederick, J.; Schoen, J.; Lemons, E. Biomaterials Science, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Kwist, K.; Bridges, W.C.; Burg, K.J.L. The effect of cell passage number on osteogenic and adipogenic characteristics of D1 cells. Cytotechnology 2015, 68, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Tang, X.; Gohil, S.V.; Laurencin, C.T. Biomaterials for Bone Regenerative Engineering. Adv. Health Mater. 2015, 4, 1268–1285. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Yan, X.; Huang, C.; Melerzanov, A.; Du, Y. Biomaterials as carrier, barrier and reactor for cell-based regenerative medicine. Protein Cell 2015, 6, 638–653. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.; Kundu, S.; Motiani, R.; Sreekanth, V.; Motiani, R.K.; Sengupta, S.; Srivastava, A.; Bajaj, A. Injectable small molecule hydrogel as a potential nanocarrier for localized and sustained in vivo delivery of doxorubicin. Nanoscale 2014, 6, 12849–12855. [Google Scholar] [CrossRef]
- Perez-Estenaga, I.; Prosper, F.; Pelacho, B. Allogeneic Mesenchymal Stem Cells and Biomaterials: The Perfect Match for Cardiac Repair? Int. J. Mol. Sci. 2018, 19, 3236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, B.P.; Naved, B.A.; Nyberg, E.L.; Dias, M.; Holmes, C.; Elisseeff, J.H.; Dorafshar, A.; Grayson, W.L. Three-Dimensional Printing of Bone Extracellular Matrix for Craniofacial Regeneration. ACS Biomater. Sci. Eng. 2016, 2, 1806–1816. [Google Scholar] [CrossRef]
- Jeong, S.I.; Kim, S.H.; Kim, Y.H.; Jung, Y.; Kwon, J.H.; Kim, B.-S.; Lee, Y.M. Manufacture of elastic biodegradable PLCL scaffolds for mechano-active vascular tissue engineering. J. Biomater. Sci. Polym. Ed. 2004, 15, 645–660. [Google Scholar] [CrossRef]
- Huri, P.Y.; Ozilgen, B.A.; Hutton, D.L.; Grayson, W.L. Scaffold pore size modulates in vitro osteogenesis of human adipose-derived stem/stromal cells. Biomed. Mater. 2014, 9, 045003. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, G.B.; Chacon, E.; Chacon, P.G.; Bordeaux-Rego, P.; Duarte, A.S.; Saad, S.T.O.; Zavaglia, C.A.; Cunha, M.R. Fatty acid is a potential agent for bone tissue induction: In vitro and in vivo approach. Exp. Biol. Med. 2017, 242, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Song, L.; Wang, J.; Yan, S.; Li, G.; Cui, L.; Yin, J. Strategy for constructing vascularized adipose units in poly(l-glutamic acid) hydrogel porous scaffold through inducing in-situ formation of ASCs spheroids. Acta Biomater. 2017, 51, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Denost, Q.; Adam, J.-P.; Pontallier, A.; Montembault, A.; Bareille, R.; Siadous, R.; Delmond, S.; Rullier, E.; David, L.; Bordenave, L. Colorectal tissue engineering: A comparative study between porcine small intestinal submucosa (SIS) and chitosan hydrogel patches. Surgery 2015, 158, 1714–1723. [Google Scholar] [CrossRef]
- Ribeiro, V.; Correia, J.S.; Nascimento, A.I.; Morais, A.D.S.; Marques, A.; Ribeiro, A.S.; Silva, C.; Bonifácio, G.; Sousa, R.; Oliveira, J.M.; et al. Silk-based anisotropical 3D biotextiles for bone regeneration. Biomaterials 2017, 123, 92–106. [Google Scholar] [CrossRef]
- Bellas, E.; Panilaitis, B.J.; Glettig, D.L.; Kirker-Head, C.A.; Yoo, J.J.; Marra, K.; Rubin, J.P.; Kaplan, D.L. Sustained volume retention in vivo with adipocyte and lipoaspirate seeded silk scaffolds. Biomaterials 2013, 34, 2960–2968. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-B.; Kim, Y.S.; Lee, G.; Yun, B.G.; Kim, C.-H. The effect of surface treatment of titanium with sand-blasting/acid-etching or hydroxyapatite-coating and application of bone morphogenetic protein-2 on attachment, proliferation, and differentiation of stem cells derived from buccal fat pad. Tissue Eng. Regen. Med. 2013, 10, 115–121. [Google Scholar] [CrossRef]
- Bastami, F.; Paknejad, Z.; Jafari, M.; Salehi, M.; Rad, M.R.; Khojasteh, A. Fabrication of a three-dimensional β-tricalcium-phosphate/gelatin containing chitosan-based nanoparticles for sustained release of bone morphogenetic protein-2: Implication for bone tissue engineering. Mater. Sci. Eng. C 2017, 72, 481–491. [Google Scholar] [CrossRef]
- Choi, J.S.; Yang, H.-J.; Kim, B.S.; Kim, J.D.; Lee, S.H.; Lee, E.K.; Park, K.; Cho, Y.W.; Lee, H.Y. Fabrication of Porous Extracellular Matrix Scaffolds from Human Adipose Tissue. Tissue Eng. Part C: Methods 2010, 16, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Chattopadhyay, A.; Galvez, M.G.; Bachmann, M.; Legrand, A.; McGoldrick, R.; Lovell, A.; Jacobs, M.; Crowe, C.; Umansky, E.; Chang, J. Tendon Regeneration with Tendon Hydrogel–Based Cell Delivery: A Comparison of Fibroblasts and Adipose-Derived Stem Cells. Plast. Reconstr. Surg. 2016, 138, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Eke, G.; Mangir, N.; Hasirci, N.; MacNeil, S.; Hasirci, V. Development of a UV crosslinked biodegradable hydrogel containing adipose derived stem cells to promote vascularization for skin wounds and tissue engineering. Biomaterials 2017, 129, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Tatrai, P.; Sági, B.; Szigeti, A.; Szepesi, Á.; Szabó, I.; Bosze, S.; Kristóf, Z.; Markó, K.; Szakacs, G.; Urbán, I.; et al. A novel cyclic RGD-containing peptide polymer improves serum-free adhesion of adipose tissue-derived mesenchymal stem cells to bone implant surfaces. J. Mater. Sci. Mater. Med. 2012, 24, 479–488. [Google Scholar] [CrossRef]
- Razavi, S.; SeyedEbrahimi, R.; Jahromi, M. Biodelivery of nerve growth factor and gold nanoparticles encapsulated in chitosan nanoparticles for schwann-like cells differentiation of human adipose-derived stem cells. Biochem. Biophys. Res. Commun. 2019, 513, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Doglioli, P.; Scortecci, G.; Falatouni, M. A novel spectrofluorometric technique for specific biocompatibility testing of implantable materials by cell culture. Report on use for multiparameter analysis of human osteoblasts cultured on commercially pure titanium and hydroxyapatite. Cytotechnology 2001, 35, 93–100. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Ashjian, P.; De Ugarte, D.A.; Huang, J.I.; Mizuno, H.; Alfonso, Z.C.; Fraser, J.K.; Benhaim, P.; Hedrick, M.H. Human Adipose Tissue Is a Source of Multipotent Stem Cells. Mol. Biol. Cell 2002, 13, 4279–4295. [Google Scholar] [CrossRef]
- Sarugaser, R.; Lickorish, D.; Baksh, D.; Hosseini, M.M.; Davies, J.E. Human Umbilical Cord Perivascular (HUCPV) Cells: A Source of Mesenchymal Progenitors. Stem Cells 2005, 23, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farré-Guasch, E.; Martí-Pagès, C.; Hernández-Alfaro, F.; Klein-Nulend, J.; Casals, N. Buccal Fat Pad, an Oral Access Source of Human Adipose Stem Cells with Potential for Osteochondral Tissue Engineering: An In Vitro Study. Tissue Eng. Part C Methods 2010, 16, 1083–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrin, I.; Beloqui, I.; Zabaleta, L.; Salcedo, J.M.; Trigueros, C.; Martin, A.G. Isolation, Culture, and Expansion of Mesenchymal Stem Cells. In Stem Cell Banking. Methods in Molecular Biology; Crook, J., Ludwig, T., Eds.; Humana Press: New York, NY, USA, 2017; Volume 1590, pp. 177–190. [Google Scholar] [CrossRef]
- Jiang, T.; Xu, G.; Wang, Q.; Yang, L.; Zheng, L.; Zhao, J.; Zhang, X. In vitro expansion impaired the stemness of early passage mesenchymal stem cells for treatment of cartilage defects. Cell Death Dis. 2017, 8, e2851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pamies, D.; Bal-Price, A.; Simeonov, A.; Tagle, D.; Allen, D.; Gerhold, D.; Yin, D.; Pistollato, F.; Inutsuka, T.; Sullivan, K.; et al. Good Cell Culture Practice for Stem Cells and Stem-Cell-Derived Models. Altex 2017, 34, 95–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellotti, C.; Stanco, D.; Ragazzini, S.; Romagnoli, L.; Martella, E.; Lazzati, S.; Marchetti, C.; Donati, D.M.; Lucarelli, E. Analysis of the Karyotype of Expanded Human Adipose-Derived Stem Cells for Bone Reconstruction of the Maxillo-Facial Region. Int. J. Immunopathol. Pharmacol. 2013, 26, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Mushahary, D.; Spittler, A.; Kasper, C.; Weber, V.; Charwat, V. Isolation, cultivation, and characterization of human mesenchymal stem cells. Cytom. Part A 2018, 93, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Bourin, P.; Bunnell, B.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal cells from the adipose tissue-derived stromal vascular fraction and culture expanded adipose tissue-derived stromal/stem cells: A joint statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Müller, D.J.; Dufrêne, Y. Atomic force microscopy: A nanoscopic window on the cell surface. Trends Cell Biol. 2011, 21, 461–469. [Google Scholar] [CrossRef]
- Heo, S.C.; Shin, W.C.; Lee, M.J.; Kim, B.R.; Jang, I.H.; Choi, E.-J.; Lee, J.S.; Kim, J.H. Periostin Accelerates Bone Healing Mediated by Human Mesenchymal Stem Cell-Embedded Hydroxyapatite/Tricalcium Phosphate Scaffold. PLoS ONE 2015, 10, e0116698. [Google Scholar] [CrossRef]
- Grotenhuis, N.; De Witte, S.F.; Van Osch, G.J.; Bayon, Y.; Lange, J.F.; Bastiaansen-Jenniskens, Y.M. Biomaterials Influence Macrophage–Mesenchymal Stem Cell Interaction In Vitro. Tissue Eng. Part A 2016, 22, 1098–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, T.; Vandrovcová, M.; Kročilová, N.; Keppler, J.K.; Zárubová, J.; Skirtach, A.G.; Bacakova, L. Application of whey protein isolate in bone regeneration: Effects on growth and osteogenic differentiation of bone-forming cells. J. Dairy Sci. 2018, 101, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Yang, F.; Both, S.K.; Prins, H.-J.; Helder, M.N.; Pan, J.; Cui, F.-Z.; Jansen, J.A.; Beucken, J.J.V.D. Bone forming capacity of cell- and growth factor-based constructs at different ectopic implantation sites. J. Biomed. Mater. Res. Part A 2014, 103, 439–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samsonraj, R.M.; Raghunath, M.; Nurcombe, V.; Hui, J.H.; Van Wijnen, A.J.; Cool, S.M. Concise Review: Multifaceted Characterization of Human Mesenchymal Stem Cells for Use in Regenerative Medicine. Stem Cells Transl. Med. 2017, 6, 2173–2185. [Google Scholar] [CrossRef] [Green Version]
- Loring, J.F.; Rao, M.S. Establishing Standards for the Characterization of Human Embryonic Stem Cell Lines. Stem Cells 2006, 24, 145–150. [Google Scholar] [CrossRef]
- Henkel, J.; Woodruff, M.; Epari, D.; Steck, R.; Glatt, V.; Dickinson, I.C.; Choong, P.; Schuetz, M.A.; Hutmacher, D.W. Bone Regeneration Based on Tissue Engineering Conceptions—A 21st Century Perspective. Bone Res. 2013, 1, 216–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical Trials. Clinical Trials.Gov. Available online: https://clinicaltrials.gov/ct2/results/map?term=adipose+stem+cells&cond=bone&map (accessed on 28 June 2021).
- Bryda, E.C. The Mighty Mouse: The Impact of Rodents on Advances in Biomedical Research. Mo. Med. 2013, 110, 207–211. [Google Scholar] [PubMed]
- Zolocinska, A.; Siennicka, K.; Debski, T.; Gut, G.; Mazur, S.; Gajewska, M.; Kaminski, A.; Pojda, Z. Comparison of mouse, rat and rabbit models for adipose—Derived stem cells (ASC) research. Curr. Res. Transl. Med. 2020, 68, 205–210. [Google Scholar] [CrossRef]
- Ribatti, D. The chick embryo chorioallantoic membrane (CAM). A multifaceted experimental model. Mech. Dev. 2016, 141, 70–77. [Google Scholar] [CrossRef]
- Moticka, E.J. The Thymus in Lymphocyte Maturation. In A Historical Perspective on Evidence-Based Immunology; Elsevier: Amsterdam, The Netherlands, 2016; pp. 69–74. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selected Articles | Number of Articles | % |
|---|---|---|
| Electronic Microscopy | 51 | 52.04 |
| Microscopy | 92 | 93.88 |
| ELISA | 19 | 19.39 |
| Immunohistochemistry | 24 | 24.49 |
| Immunocytochemistry | 17 | 17.35 |
| Spectrometry | 45 | 45.92 |
| Genetic testing | 61 | 62.24 |
| Metabolic assays | 49 | 50.00 |
| Viability and cytotoxicity | 32 | 32.66 |
| Flow cytometry | 32 | 32.66 |
| Others | 44 | 44.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Goulart, V.; Carvalho, L.N.; Marinho, A.L.G.; de Oliveira Souza, B.L.; de Aquino Pinto Palis, G.; Lage, H.G.D.; de Lima, I.L.; Guimarães, L.D.; Peres, L.C.; Silveira, M.M.; et al. Biomaterials and Adipose-Derived Mesenchymal Stem Cells for Regenerative Medicine: A Systematic Review. Materials 2021, 14, 4641. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14164641
Alonso-Goulart V, Carvalho LN, Marinho ALG, de Oliveira Souza BL, de Aquino Pinto Palis G, Lage HGD, de Lima IL, Guimarães LD, Peres LC, Silveira MM, et al. Biomaterials and Adipose-Derived Mesenchymal Stem Cells for Regenerative Medicine: A Systematic Review. Materials. 2021; 14(16):4641. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14164641
Chicago/Turabian StyleAlonso-Goulart, Vivian, Loyna Nobile Carvalho, Ana Leticia Galante Marinho, Bianca Lourenço de Oliveira Souza, Gabriela de Aquino Pinto Palis, Henrique Guerra Drumond Lage, Isabela Lemos de Lima, Laura Duarte Guimarães, Lucas Correia Peres, Márcia Marques Silveira, and et al. 2021. "Biomaterials and Adipose-Derived Mesenchymal Stem Cells for Regenerative Medicine: A Systematic Review" Materials 14, no. 16: 4641. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14164641