
Bioabsorbable Polymeric Stent for the Treatment of Coarctation of the Aorta (CoA) in Children: A Methodology to Evaluate the Design and Mechanical Properties of PLA Polymer

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stent Geometry
2.2. Determination of the Mechanical Properties of PLA
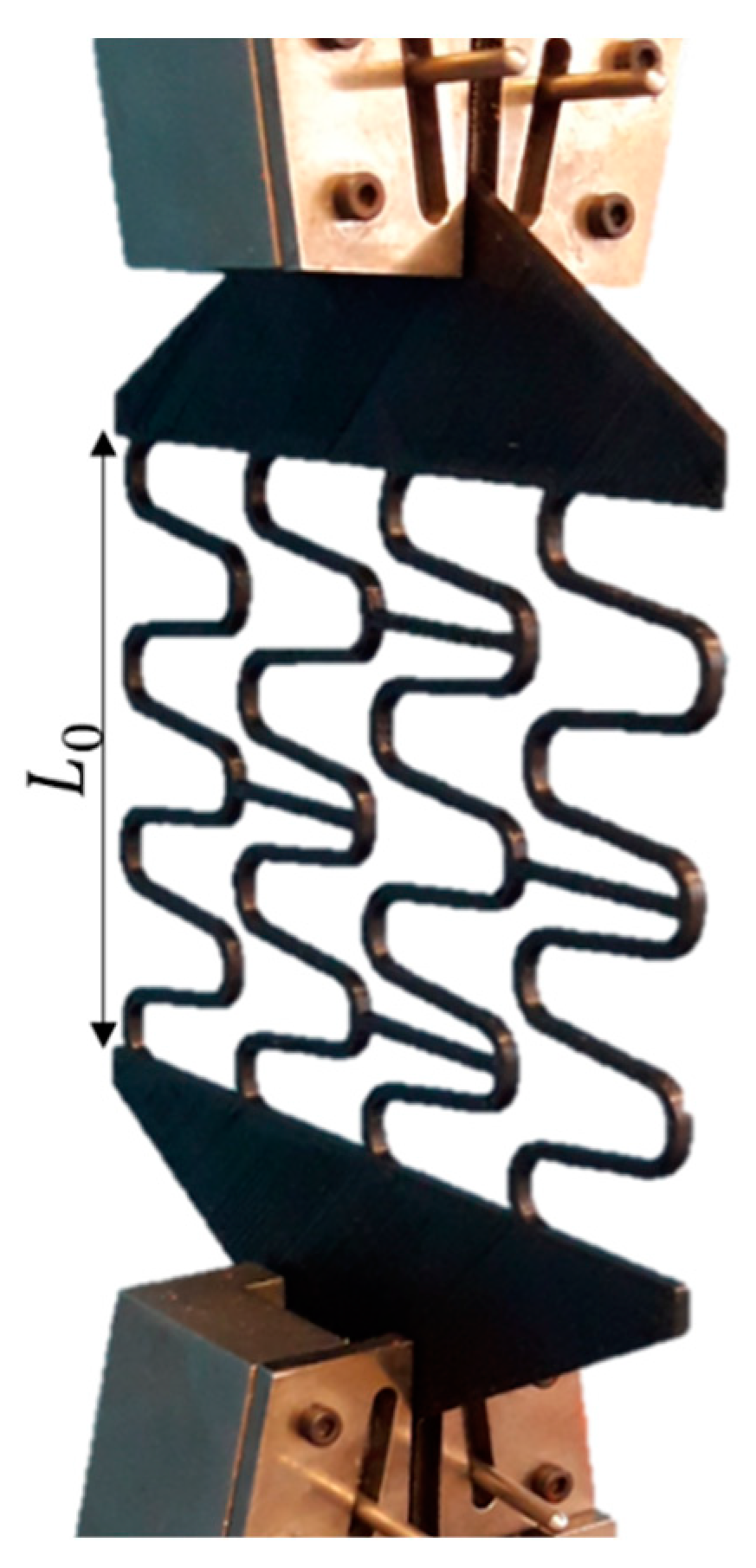
2.3. Model’s Validation Experiment
2.4. Finite Element Modelling
2.4.1. Finite Element Modelling of Experimental Tests
2.4.2. Finite Element Modelling of Crimping
- (1)
- A radial displacement by the rigid crimper was applied to reduce the stent’s initial diameter from 6.75 mm to 5 mm.
- (2)
- The crimper was removed so that the stent could go through the linear-recoil effect.
- (3)
- The stent was expanded from 5 mm to a maximum value that ranged from 12 to 15 mm by applying a radial displacement by the balloon.
- (4)
- The balloon was removed to measure the elastic recoil.
3. Results
3.1. Mechanical Properties of PLA
3.2. Finite Element Model Validation
3.3. Assessment of Crimping Effect on Stent’s Mechanical Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doshi, A.R.; Chikkabyrappa, S. Coarctation of Aorta in Children. Cureus 2018, 10, e3690. [Google Scholar] [CrossRef] [Green Version]
- Castaldi, B.; Ciarmoli, E.; Di Candia, A.; Sirico, D.; Tarantini, G.; Scattolin, F.; Padalino, M.; Vida, V.; Di Salvo, G. Safety and efficacy of aortic coarctation stenting in children and adolescents. Int. J. Cardiol. Congenit. Heart Dis. 2022, 8, 100389. [Google Scholar] [CrossRef]
- Nguyen, L.; Cook, S.C. Coarctation of the Aorta Strategies for Improving Outcomes. Cardiol. Clin. 2015, 33, 521–530. [Google Scholar] [CrossRef]
- Brown, M.L.; Burkhart, H.M.; Connolly, H.M.; Dearani, J.A.; Cetta, F.; Li, Z.; Oliver, W.C.; Warnes, C.A.; Schaff, H.V. Coarctation of the Aorta Lifelong Surveillance Is Mandatory Following Surgical Repair. J. Am. Coll. Cardiol. 2013, 62, 1020–1025. [Google Scholar] [CrossRef] [Green Version]
- Nance, J.W.; Ringel, R.E.; Fishman, E.K. Coarctation of the aorta in adolescents and adults: A review of clinical features and CT imaging. J. Cardiovasc. Comput. Tomogr. 2016, 10, 1–12. [Google Scholar] [CrossRef]
- Torok, R.D.; Campbell, M.J.; Fleming, G.A.; Hill, K.D. Coarctation of the aorta: Management from infancy to adulthood. World J. Cardiol. 2015, 7, 765–775. [Google Scholar] [CrossRef]
- Van Der Linde, D.; Konings, E.E.M.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.M.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [Green Version]
- Pathirana, D.; Johnston, B.; Johnston, P. The effects of tapering and artery wall stiffness on treatments for Coarctation of the Aorta. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 1512–1524. [Google Scholar] [CrossRef]
- Alexy, R.D.; Levi, D.S. Materials and Manufacturing Technologies Available for Production of a Pediatric Bioabsorbable Stent. BioMed Res. Int. 2013, 2013, 137985. [Google Scholar] [CrossRef] [Green Version]
- Homsi, M.; El Khoury, M.; Hmedeh, C.; Arabi, M.; El Rassi, I.; Bulbul, Z.; Sawaya, F.; Bitar, F.; Haddad, F. Endovascular Stent Repair of Aortic Coarctation in a Developing Country: A Single-Center Experience. Cardiovasc. Revasc. Med. 2022, 39, 66–72. [Google Scholar] [CrossRef]
- Kasar, T.; Erkut, O.; Tanidir, I.C.; Şahin, M.; Topkarci, M.A.; Guzeltas, A. Balloon-expandable stents for native coarctation of the aorta in children and adolescents. Medicine 2022, 101, e32332. [Google Scholar] [CrossRef] [PubMed]
- Van Kalsbeek, R.J.; Krings, G.J.; Molenschot, M.M.C.; Breur, J.M.P.J. Early and midterm outcomes of bare metal stenting in small children with recurrent aortic coarctation. EuroIntervention 2021, 16, e1281–e1287. [Google Scholar] [CrossRef] [PubMed]
- Qiu, T.Y.; Song, M.; Zhao, L.G. A computational study of crimping and expansion of bioresorbable polymeric stents. Mech. Time-Depend. Mater. 2018, 22, 273–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghi, T.C., Jr.; Costa, J.R., Jr.; Abizaid, A.; Chamié, D.; Silva, M.V.; Taiguara, D.; Costa, R.; Staico, R.; Feres, F.; Chaves, Á.J.; et al. Comparação da retração aguda do stent entre o suporte vascular bioabsorvível eluidor de everolimus e dois diferentes stents metálicos farmacológicos. Rev. Bras. Cardiol. Invasiva 2013, 21, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Veeram Reddy, S.R.; Welch, T.R.; Wang, J.; Richardson, J.A.; Forbess, J.M.; Riegel, M.; Nugent, A.W. A novel design biodegradable stent for use in congenital heart disease: Mid-term results in rabbit descending aorta. Catheter. Cardiovasc. Interv. 2015, 85, 629–639. [Google Scholar] [CrossRef]
- Veeram, S.R.; Welch, T.R.; Nugent, A.W. Biodegradable stent use for congenital heart disease. Prog. Pediatr. Cardiol. 2021, 61, 101349. [Google Scholar] [CrossRef]
- Wright, J.; Nguyen, A.; D’Souza, N.; Forbess, J.M.; Nugent, A.; Reddy, S.R.V.; Jaquiss, R.; Welch, T.R. Bioresorbable stent to manage congenital heart defects in children. Materialia 2021, 16, 101078. [Google Scholar] [CrossRef]
- Torki, M.M.; Hassanajili, S.; Jalisi, M.M. Design optimizations of PLA stent structure by FEM and investigating its function in a simulated plaque artery. Math. Comput. Simul. 2020, 169, 103–116. [Google Scholar] [CrossRef]
- Ammarullah, M.I.; Hartono, R.; Supriyono, T.; Santoso, G.; Sugiharto, S.; Permana, M.S. Polycrystalline Diamond as a Potential Material for the Hard-on-Hard Bearing of Total Hip Prosthesis: Von Mises Stress Analysis. Biomedicines 2023, 11, 951. [Google Scholar] [CrossRef]
- Schiavone, A.; Qiu, T.Y.; Zhao, L.G. Crimping and deployment of metallic and polymeric stents—Finite element modelling. Vessel Plus 2017, 1, 12–21. [Google Scholar] [CrossRef] [Green Version]
- ASTM D638-14; Standard Test Method for Tensile Properties of Plastics. ASTM International: New York, NY, USA, 2014.
- Donik, Ž.; Nečemer, B.; Vesenjak, M.; Glodež, S.; Kramberger, J. Computational Analysis of Mechanical Performance for Composite Polymer Biodegradable Stents. Materials 2021, 14, 6016. [Google Scholar] [CrossRef] [PubMed]
- Schiavone, A.; Zhao, L.G. A study of balloon type, system constraint and artery constitutive model used in finite element simulation of stent deployment. Mech. Adv. Mater. Mod. Process. 2015, 1, 1. [Google Scholar] [CrossRef]
- Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Wibowo, D.B.; Kurdi, O.; Tauviqirrahman, M.; Jamari, J. Minimizing Risk of Failure from Ceramic-on-Ceramic Total Hip Prosthesis by Selecting Ceramic Materials Based on Tresca Stress. Sustainability 2022, 14, 13413. [Google Scholar] [CrossRef]
- Borghi, A.; Murphy, O.; Bahmanyar, R.; Mcleod, C. Effect of Stent Radial Force on Stress Pattern after Deployment: A Finite Element Study. J. Mater. Eng. Perform. 2014, 23, 2599–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caimi, A.; Pasquali, M.; Sturla, F.; Pluchinotta, F.R.; Giugno, L.; Carminati, M.; Redaelli, A.; Votta, E. Prediction of post-stenting biomechanics in coarcted aortas: A pilot finite element study. J. Biomech. 2020, 105, 109796. [Google Scholar] [CrossRef] [PubMed]
- Forbes, T.J.; Gowda, S.T. Intravascular Stent Therapy for Coarctation of the Aorta. Methodist DeBakey Cardiovasc. J. 2014, 10, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Akturk, Y.; Ozbal Gunes, S. Normal abdominal aorta diameter in infants, children and adolescents. Pediatr. Int. 2018, 60, 455–460. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Simulation | Element Size (mm) | Von Mises (MPa) | Error (%) |
|---|---|---|---|
| S1 | 0.16 | 40.34 | - |
| S2 | 0.14 | 38.53 | 4.48 |
| S3 | 0.12 | 37.88 | 1.70 |
| S4 | 0.10 | 37.43 | 1.19 |
| Part | Element Hype | Element Order | Number of Elements |
|---|---|---|---|
| Planned Stent | SOLID187 | Quadratic | 36,428 |
| Stent | SOLID187 | Quadratic | 153,430 |
| Crimper | SHELL181 | Linear | 1540 |
| Balloon | SHELL181 | Linear | 672 |
| Sample | L0 (mm) | Lmax (mm) | Lf (mm) | Lf − L0 | Linear Recoil (%) | Load (N) |
|---|---|---|---|---|---|---|
| 1 | 73.21 | 130.00 | 81.54 | 8.33 | 37.28 | 44.13 |
| 2 | 73.23 | 129.92 | 81.73 | 8.50 | 37.09 | 38.00 |
| 3 | 73.18 | 130.07 | 80.66 | 7.48 | 37.99 | 45.36 |
| 4 | 73.21 | 130.00 | 84.75 | 11.54 | 34.81 | 30.65 |
| 5 | 73.29 | 130.10 | 85.03 | 11.74 | 34.64 | 31.87 |
| Average | 73.22 | 130.02 | 82.74 | 9.52 | 36.36 | 38.00 |
| Standard deviation | 0.04 | 0.07 | 2.00 | 1.97 | 1.53 | 6.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
dos Santos, F.J.; Hernandez, B.A.; Santos, R.; Machado, M.; Souza, M.; Capello Sousa, E.A.; Andrade, A. Bioabsorbable Polymeric Stent for the Treatment of Coarctation of the Aorta (CoA) in Children: A Methodology to Evaluate the Design and Mechanical Properties of PLA Polymer. Materials 2023, 16, 4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ma16124403
dos Santos FJ, Hernandez BA, Santos R, Machado M, Souza M, Capello Sousa EA, Andrade A. Bioabsorbable Polymeric Stent for the Treatment of Coarctation of the Aorta (CoA) in Children: A Methodology to Evaluate the Design and Mechanical Properties of PLA Polymer. Materials. 2023; 16(12):4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ma16124403
Chicago/Turabian Styledos Santos, Flávio José, Bruno Agostinho Hernandez, Rosana Santos, Marcel Machado, Mateus Souza, Edson A. Capello Sousa, and Aron Andrade. 2023. "Bioabsorbable Polymeric Stent for the Treatment of Coarctation of the Aorta (CoA) in Children: A Methodology to Evaluate the Design and Mechanical Properties of PLA Polymer" Materials 16, no. 12: 4403. https://0-doi-org.brum.beds.ac.uk/10.3390/ma16124403