Systematic Review of PCR Proof of Parvovirus B19 Genomes in Endomyocardial Biopsies of Patients Presenting with Myocarditis or Dilated Cardiomyopathy



Abstract
:1. Introduction
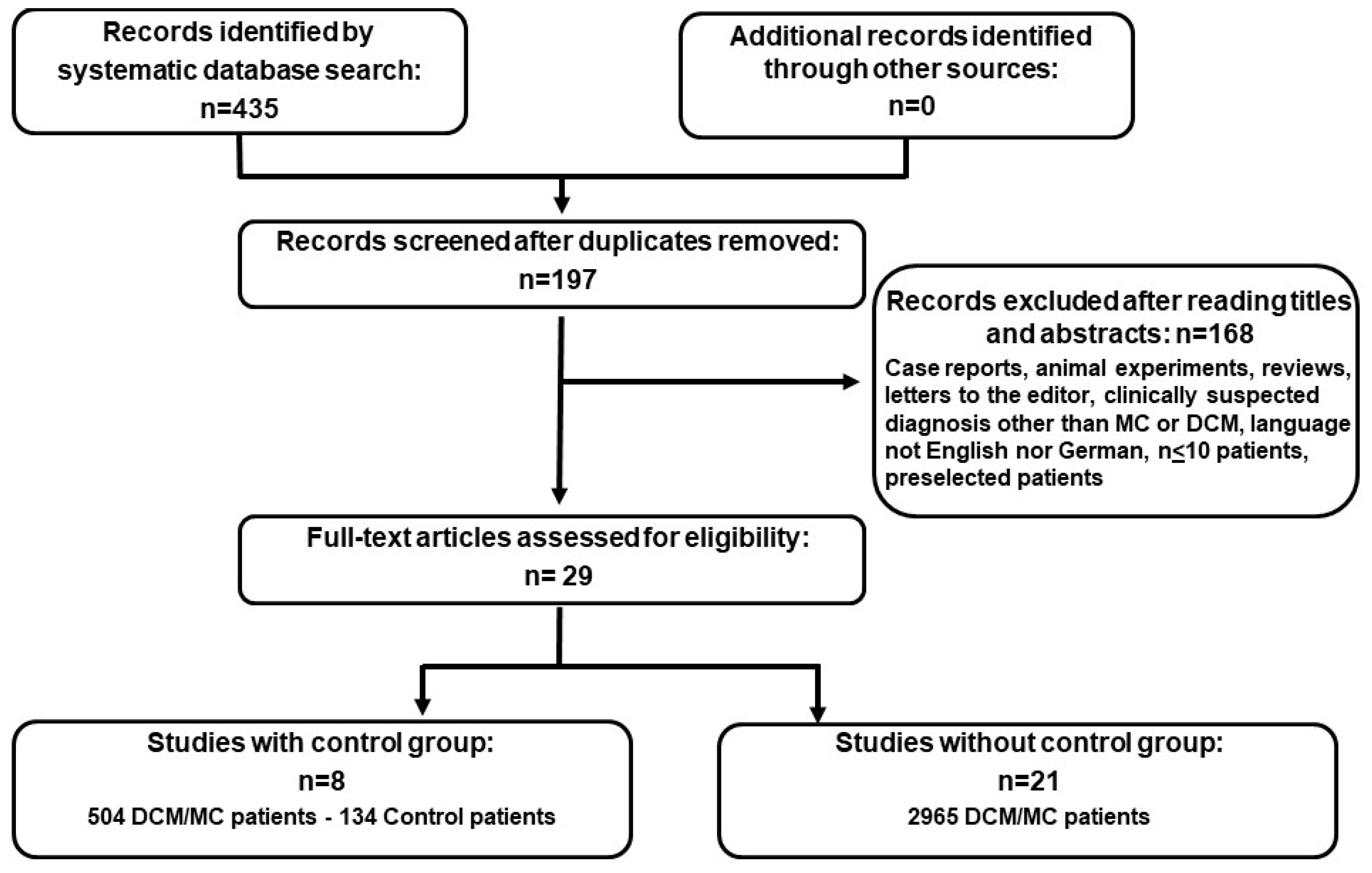
2. Materials and Methods
Statistical Analysis
3. Results
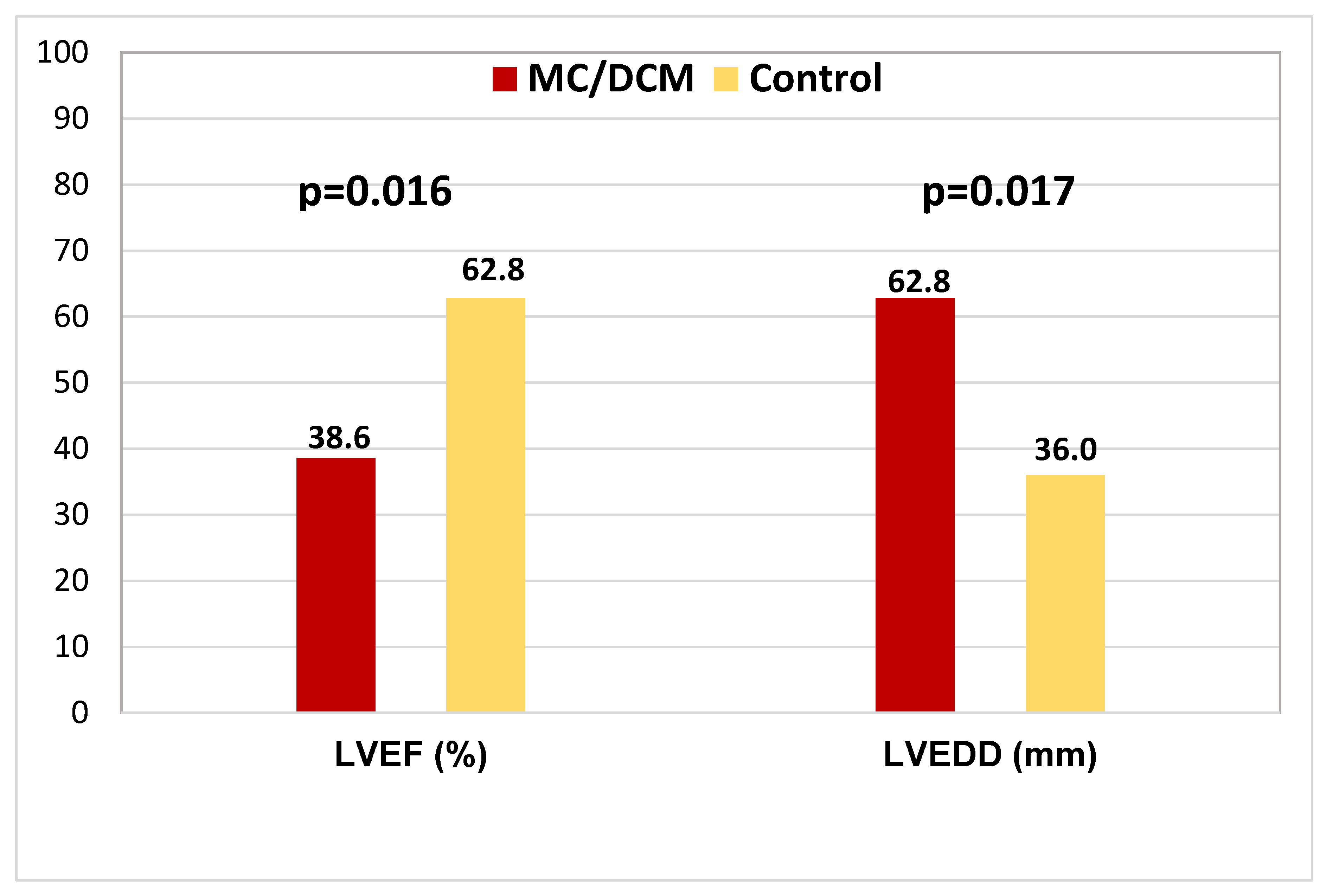
3.1. Comparison of the Cardiac Parameters between Study and Control Groups
3.2. Virus Detection Methods
3.3. Distribution of Viruses in Patients with DCM/MC and Control Patients
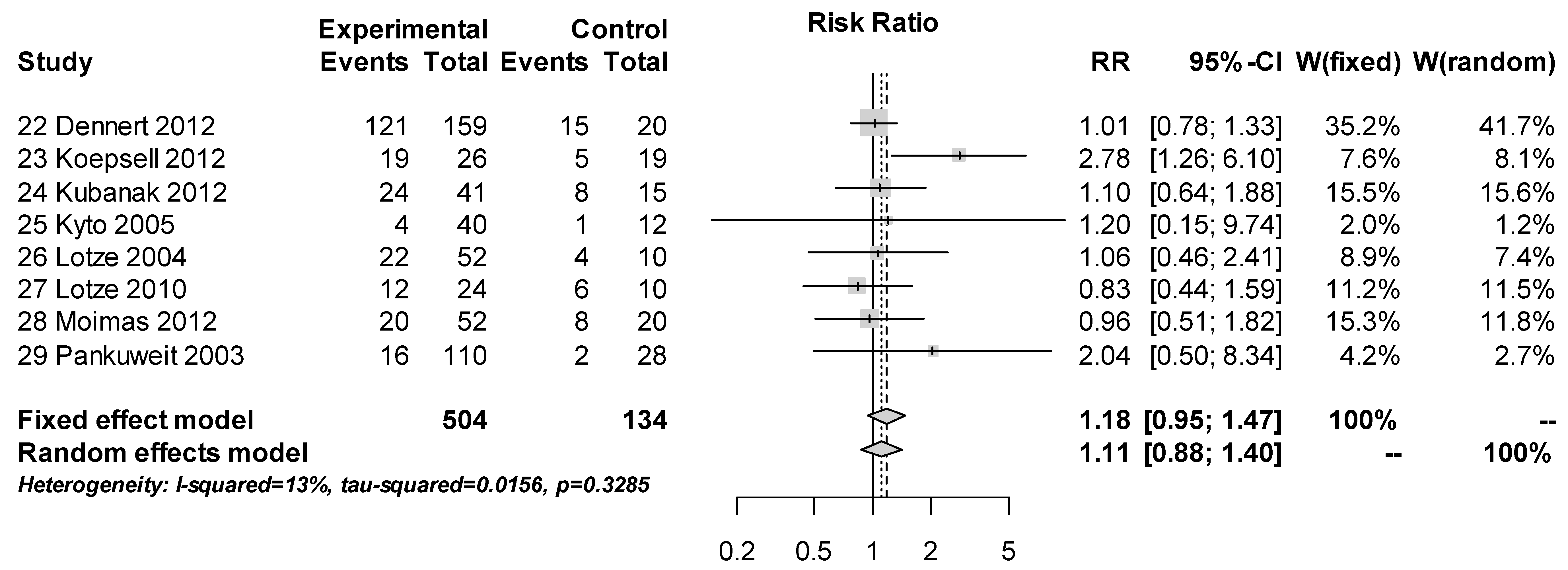
3.4. PCR Proof of B19V Genomes Comparing Patients with DCM/MC and Controls
4. Discussion
4.1. PCR Diagnosis of B19V
4.2. Factors Potentially Influencing EMB Diagnosis
4.3. Control Group
4.4. Prognostic Relevance of PCR Proven B19V Genomes in the Endomyocardium
4.5. Future Management Strategies
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| B19V | parvovirus B19 |
| CMR | cardiac magnetic resonance |
| DCM | dilated cardiomyopathy |
| DCMi | inflammatory cardiomyopathy |
| EMB | endomyocardial biopsy or biopsies |
| EV | enterovirus: enteroviral |
| IHC | immunohistochemical |
| LGE | late gadolinium enhancement |
| LVEF | left ventricular ejection fraction |
| LVEDD | left ventricular end-diastolic diameter |
| MC | myocarditis |
| PCR | polymerase chain reaction |
References
- Noutsias, M.; Maisch, B. Myocarditis and pericarditis. In The ESC Textbook of Acute and Intensive Cardiac Care, 2nd ed.; Tubaro, M., Vranckx, P., Price, S., Vrints, C., Eds.; Oxford University Press: Oxford, UK, 2014; Volume 2, pp. 547–560. [Google Scholar]
- D’Ambrosio, A.; Patti, G.; Manzoli, A.; Sinagra, G.; di Lenarda, A.; Silvestri, F.; di Sciascio, G. The fate of acute myocarditis between spontaneous improvement and evolution to dilated cardiomyopathy: A review. Heart 2001, 85, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Noutsias, M.; Seeberg, B.; Schultheiss, H.P.; Kühl, U. Expression of cell adhesion molecules in dilated cardiomyopathy: Evidence for endothelial activation in inflammatory cardiomyopathy. Circulation 1999, 99, 2124–2131. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Calzolari, V.; Calabrese, F.; Boffa, G.M.; Maddalena, F.; Chioin, R.; Thiene, G. Myocarditis mimicking acute myocardial infarction: Role of endomyocardial biopsy in the differential diagnosis. Heart 2000, 84, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Kühl, U.; Pauschinger, M.; Seeberg, B.; Lassner, D.; Noutsias, M.; Poller, W.; Schultheiss, H.P. Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation 2005, 112, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Kindermann, I.; Kindermann, M.; Kandolf, R.; Klingel, K.; Bultmann, B.; Muller, T.; Lindinger, A.; Bohm, M. Predictors of outcome in patients with suspected myocarditis. Circulation 2008, 118, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Mahrholdt, H.; Goedecke, C.; Wagner, A.; Meinhardt, G.; Athanasiadis, A.; Vogelsberg, H.; Fritz, P.; Klingel, K.; Kandolf, R.; Sechtem, U. Cardiovascular magnetic resonance assessment of human myocarditis: A comparison to histology and molecular pathology. Circulation 2004, 109, 1250–1258. [Google Scholar] [CrossRef]
- Mavrogeni, S.; Spargias, C.; Bratis, C.; Kolovou, G.; Markussis, V.; Papadopoulou, E.; Constadoulakis, P.; Papadimitropoulos, M.; Douskou, M.; Pavlides, G.; et al. Myocarditis as a precipitating factor for heart failure: Evaluation and 1-year follow-up using cardiovascular magnetic resonance and endomyocardial biopsy. Eur. J. Heart Fail. 2011, 13, 830–837. [Google Scholar] [CrossRef]
- Gutberlet, M.; Spors, B.; Thoma, T.; Bertram, H.; Denecke, T.; Felix, R.; Noutsias, M.; Schultheiss, H.P.; Kühl, U. Suspected chronic myocarditis at cardiac MR: Diagnostic accuracy and association with immunohistologically detected inflammation and viral persistence. Radiology 2008, 246, 401–409. [Google Scholar] [CrossRef]
- Mahfoud, F.; Gartner, B.; Kindermann, M.; Ukena, C.; Gadomski, K.; Klingel, K.; Kandolf, R.; Bohm, M.; Kindermann, I. Virus serology in patients with suspected myocarditis: Utility or futility? Eur. Heart J. 2011, 32, 897–903. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Helio, T.; Heymans, S.; Jahns, R.; et al. European Society of Cardiology Working Group on M.; Pericardial, D. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar]
- Pankuweit, S.; Moll, R.; Baandrup, U.; Portig, I.; Hufnagel, G.; Maisch, B. Prevalence of the parvovirus B19 genome in endomyocardial biopsy specimens. Hum. Pathol. 2003, 34, 497–503. [Google Scholar] [CrossRef]
- Kühl, U.; Pauschinger, M.; Noutsias, M.; Seeberg, B.; Bock, T.; Lassner, D.; Poller, W.; Kandolf, R.; Schultheiss, H.P. High prevalence of viral genomes and multiple viral infections in the myocardium of adults with “idiopathic” left ventricular dysfunction. Circulation 2005, 111, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Westphal, J.G.; Rigopoulos, A.G.; Bakogiannis, C.; Ludwig, S.E.; Mavrogeni, S.; Bigalke, B.; Doenst, T.; Pauschinger, M.; Tschope, C.; Schulze, P.C.; et al. The MOGE(S) classification for cardiomyopathies: Current status and future outlook. Heart Fail. Rev. 2017, 22, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Baboonian, C.; Treasure, T. Meta-analysis of the association of enteroviruses with human heart disease. Heart 1997, 78, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norja, P.; Hokynar, K.; Aaltonen, L.M.; Chen, R.; Ranki, A.; Partio, E.K.; Kiviluoto, O.; Davidkin, I.; Leivo, T.; Eis-Hubinger, A.M.; et al. Bioportfolio: Lifelong persistence of variant and prototypic erythrovirus DNA genomes in human tissue. Proc. Natl. Acad. Sci. USA 2006, 103, 7450–7453. [Google Scholar] [CrossRef] [Green Version]
- Kuhl, U.; Lassner, D.; von Schlippenbach, J.; Poller, W.; Schultheiss, H.P. Interferon-Beta improves survival in enterovirus-associated cardiomyopathy. J. Am. Coll Cardiol. 2012, 60, 1295–1296. [Google Scholar] [CrossRef]
- Zimmermann, O.; Rodewald, C.; Radermacher, M.; Vetter, M.; Wiehe, J.M.; Bienek-Ziolkowski, M.; Hombach, V.; Torzewski, J. Interferon beta-1b therapy in chronic viral dilated cardiomyopathy--is there a role for specific therapy? J. Card Fail. 2010, 16, 348–356. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Neupane, B.; Richer, D.; Bonner, A.J.; Kibret, T.; Beyene, J. Network meta-analysis using R: a review of currently available automated packages. PLoS ONE 2014, 9, e115065. [Google Scholar] [CrossRef]
- Kühl, U.; Pauschinger, M.; Bock, T.; Klingel, K.; Schwimmbeck, C.P.; Seeberg, B.; Krautwurm, L.; Noutsias, M.; Poller, W.; Schultheiss, H.P.; et al. Parvovirus B19 infection mimicking acute myocardial infarction. Circulation 2003, 108, 945–950. [Google Scholar] [CrossRef]
- Lotze, U.; Egerer, R.; Tresselt, C.; Gluck, B.; Dannberg, G.; Stelzner, A.; Figulla, H.R. Frequent detection of parvovirus B19 genome in the myocardium of adult patients with idiopathic dilated cardiomyopathy. Med. Microbiol. Immunol. (Berl.) 2004, 193, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Vallbracht, K.B.; Schwimmbeck, P.L.; Kuhl, U.; Seeberg, B.; Schultheiss, H.P. Endothelium-dependent flow-mediated vasodilation of systemic arteries is impaired in patients with myocardial virus persistence. Circulation 2004, 110, 2938–2945. [Google Scholar] [CrossRef] [PubMed]
- Kyto, V.; Vuorinen, T.; Saukko, P.; Lautenschlager, I.; Lignitz, E.; Saraste, A.; Voipio-Pulkki, L.M. Cytomegalovirus infection of the heart is common in patients with fatal myocarditis. Clin. Infect. Dis. 2005, 40, 683–688. [Google Scholar] [CrossRef]
- Tschöpe, C.; Bock, C.T.; Kasner, M.; Noutsias, M.; Westermann, D.; Schwimmbeck, P.L.; Pauschinger, M.; Poller, W.C.; Kühl, U.; Kandolf, R.; et al. High prevalence of cardiac parvovirus B19 infection in patients with isolated left ventricular diastolic dysfunction. Circulation 2005, 111, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Mahrholdt, H.; Wagner, A.; Deluigi, C.C.; Kispert, E.; Hager, S.; Meinhardt, G.; Vogelsberg, H.; Fritz, P.; Dippon, J.; Bock, C.T.; et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006, 114, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Kuethe, F.; Sigusch, H.H.; Hilbig, K.; Tresselt, C.; Gluck, B.; Egerer, R.; Figulla, H.R. Detection of viral genome in the myocardium: Lack of prognostic and functional relevance in patients with acute dilated cardiomyopathy. Am. Heart J. 2007, 153, 850–858. [Google Scholar] [CrossRef]
- Escher, F.; Kühl, U.; Sabi, T.; Suckau, L.; Lassner, D.; Poller, W.; Schultheiss, H.P.; Noutsias, M. Immunohistological detection of Parvovirus B19 capsid proteins in endomyocardial biopsies from dilated cardiomyopathy patients. Med. Sci. Monit. 2008, 14, CR333–CR338. [Google Scholar] [CrossRef]
- Escher, F.; Modrow, S.; Sabi, T.; Kuhl, U.; Lassner, D.; Schultheiss, H.P.; Noutsias, M. Parvovirus B19 profiles in patients presenting with acute myocarditis and chronic dilated cardiomyopathy. Med. Sci. Monit. 2008, 14, CR589–CR597. [Google Scholar]
- Kühl, U.; Lassner, D.; Pauschinger, M.; Gross, U.M.; Seeberg, B.; Noutsias, M.; Poller, W.; Schultheiss, H.P. Prevalence of erythrovirus genotypes in the myocardium of patients with dilated cardiomyopathy. J. Med. Virol. 2008, 80, 1243–1251. [Google Scholar] [CrossRef]
- Schenk, T.; Enders, M.; Pollak, S.; Hahn, R.; Huzly, D. High prevalence of human parvovirus B19 DNA in myocardial autopsy samples from subjects without myocarditis or dilative cardiomyopathy. J. Clin. Microbiol. 2009, 47, 106–110. [Google Scholar] [CrossRef]
- Yilmaz, A.; Mahrholdt, H.; Athanasiadis, A.; Vogelsberg, H.; Meinhardt, G.; Voehringer, M.; Kispert, E.M.; Deluigi, C.; Baccouche, H.; Spodarev, E.; et al. Coronary vasospasm as the underlying cause for chest pain in patients with PVB19 myocarditis. Heart 2008, 94, 1456–1463. [Google Scholar] [CrossRef]
- Zimmermann, O.; Bienek-Ziolkowski, M.; Wolf, B.; Vetter, M.; Baur, R.; Mailander, V.; Hombach, V.; Torzewski, J. Myocardial inflammation and non-ischaemic heart failure: Is there a role for C-reactive protein? Basic. Res. Cardiol. 2009, 104, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Moulik, M.; Breinholt, J.P.; Dreyer, W.J.; Kearney, D.L.; Price, J.F.; Clunie, S.K.; Moffett, B.S.; Kim, J.J.; Rossano, J.W.; Jefferies, J.L.; et al. Viral endomyocardial infection is an independent predictor and potentially treatable risk factor for graft loss and coronary vasculopathy in pediatric cardiac transplant recipients. J. Am. Coll Cardiol. 2010, 56, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Lotze, U.; Egerer, R.; Gluck, B.; Zell, R.; Sigusch, H.; Erhardt, C.; Heim, A.; Kandolf, R.; Bock, T.; Wutzler, P.; et al. Low level myocardial parvovirus B19 persistence is a frequent finding in patients with heart disease but unrelated to ongoing myocardial injury. J. Med. Virol. 2010, 82, 1449–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruppert, V.; Meyer, T.; Balbach, A.; Richter, A.; Muller, H.H.; Maisch, B.; Pankuweit, S. Genotype-specific effects on left ventricular function in parvovirus B19-positive patients with dilated cardiomyopathy. J. Med. Virol. 2011, 83, 1818–1825. [Google Scholar] [CrossRef] [PubMed]
- Stewart, G.C.; Lopez-Molina, J.; Gottumukkala, R.V.; Rosner, G.F.; Anello, M.S.; Hecht, J.L.; Winters, G.L.; Padera, R.F.; Baughman, K.L.; Lipes, M.A. Myocardial parvovirus B19 persistence: Lack of association with clinicopathologic phenotype in adults with heart failure. Circ. Heart Fail. 2011, 4, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Dennert, R.; van Paassen, P.; Wolffs, P.; Bruggeman, C.; Velthuis, S.; Felix, S.; van Suylen, R.J.; Crijns, H.J.; Cohen Tervaert, J.W.; Heymans, S. Differences in Virus Prevalence and Load in the Hearts of Patients with Idiopathic Dilated Cardiomyopathy with and without Immune-Mediated Inflammatory Diseases. Clin. Vaccine Immunol. 2012, 19, 1182–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koepsell, S.A.; Anderson, D.R.; Radio, S.J. Parvovirus B19 is a bystander in adult myocarditis. Cardiovasc. Pathol. 2012, 21, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Kubanek, M.; Sramko, M.; Berenova, D.; Hulinska, D.; Hrbackova, H.; Maluskova, J.; Lodererova, A.; Malek, I.; Kautzner, J. Detection of Borrelia burgdorferi sensu lato in endomyocardial biopsy specimens in individuals with recent-onset dilated cardiomyopathy. Eur. J. Heart Fail. 2012, 14, 588–596. [Google Scholar] [CrossRef]
- Moimas, S.; Zacchigna, S.; Merlo, M.; Buiatti, A.; Anzini, M.; Dreas, L.; Salvi, A.; Di Lenarda, A.; Giacca, M.; Sinagra, G. Idiopathic dilated cardiomyopathy and persistent viral infection: Lack of association in a controlled study using a quantitative assay. Heart Lung Circ. 2012, 21, 787–793. [Google Scholar] [CrossRef]
- Kuhl, U.; Lassner, D.; Dorner, A.; Rohde, M.; Escher, F.; Seeberg, B.; Hertel, E.; Tschope, C.; Skurk, C.; Gross, U.M.; et al. A distinct subgroup of cardiomyopathy patients characterized by transcriptionally active cardiotropic erythrovirus and altered cardiac gene expression. Basic. Res. Cardiol. 2013, 108, 372. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.O.; Costa, L.; Rodrigues, E.; Teles, E.L.; Baptista, M.J.; Areias, J.C. Paediatric dilated cardiomyopathy: Clinical profile and outcome. The experience of a tertiary centre for paediatric cardiology. Cardiol. Young 2015, 25, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kühl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: A scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007, 116, 2216–2233. [Google Scholar] [CrossRef] [PubMed]
- Bock, C.T.; Klingel, K.; Kandolf, R. Human parvovirus B19-associated myocarditis. N. Engl. J. Med. 2010, 362, 1248–1249. [Google Scholar] [CrossRef] [PubMed]
- Noutsias, M.; Liu, P. Coxsackievirus Induced Murine Myocarditis and Immunomodulatory Interventions. In Inflammatory Cardiomyopathy (DCMi)—Pathogenesis and Therapy; Schultheiss, H.P., Noutsias, M., Eds.; Birkhäuser Verlag: Basel, Switzerland, 2010; Volume 1, pp. 51–70. [Google Scholar]
- Young, N.S.; Brown, K.E. Parvovirus B19. N. Engl. J. Med. 2004, 350, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, C.; Gartner, B.; Sauerbrei, A.; Bohm, S.; Hottentrager, B.; Raab, U.; Thierfelder, W.; Wutzler, P.; Modrow, S. Seroprevalence of parvovirus B19 in the German population. Epidemiol. Infect. 2008, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.E. Detection and quantitation of parvovirus B19. J. Clin. Virol. 2004, 31, 1–4. [Google Scholar] [CrossRef]
- Pyoria, L.; Toppinen, M.; Mantyla, E.; Hedman, L.; Aaltonen, L.M.; Vihinen-Ranta, M.; Ilmarinen, T.; Soderlund-Venermo, M.; Hedman, K.; Perdomo, M.F. Extinct type of human parvovirus B19 persists in tonsillar B. cells. Nat. Commun. 2017, 8, 14930. [Google Scholar] [CrossRef]
- Modrow, S. Parvovirus B19: The causative agent of dilated cardiomyopathy or a harmless passenger of the human myocard? Ernst. Scher. Res. Found. Workshop 2006, 1, 63–82. [Google Scholar]
- Lindner, J.; Noutsias, M.; Lassner, D.; Wenzel, J.; Schultheiss, H.P.; Kuehl, U.; Modrow, S. Adaptive immune responses against parvovirus B19 in patients with myocardial disease. J. Clin. Virol. 2009, 44, 27–32. [Google Scholar] [CrossRef]
- Hauck, A.J.; Kearney, D.L.; Edwards, W.D. Evaluation of postmortem endomyocardial biopsy specimens from 38 patients with lymphocytic myocarditis: Implications for role of sampling error. Mayo. Clin. Proc. 1989, 64, 123545. [Google Scholar] [CrossRef]
- Noutsias, M. Myocarditis. In Algorithms in Heart Failure; Maisel, A.S., Filippatos, G., Eds.; Jaypee Brothers Medical Publishers (P.) Ltd.: New Delhi, India, 2016; Volume 1, pp. 323–345. [Google Scholar]
- Yilmaz, A.; Kindermann, I.; Kindermann, M.; Mahfoud, F.; Ukena, C.; Athanasiadis, A.; Hill, S.; Mahrholdt, H.; Voehringer, M.; Schieber, M.; et al. Comparative evaluation of left and right ventricular endomyocardial biopsy: Differences in complication rate and diagnostic performance. Circulation 2010, 122, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Streitz, M.; Noutsias, M.; Volkmer, R.; Rohde, M.; Brestrich, G.; Block, A.; Klippert, K.; Kotsch, K.; Ay, B.; Hummel, M.; et al. NS1 specific CD8+ T-cells with effector function and TRBV11 dominance in a patient with parvovirus B19 associated inflammatory cardiomyopathy. PLoS ONE 2008, 3, e2361. [Google Scholar] [CrossRef] [PubMed]
- Grun, S.; Schumm, J.; Greulich, S.; Wagner, A.; Schneider, S.; Bruder, O.; Kispert, E.M.; Hill, S.; Ong, P.; Klingel, K.; et al. Long-term follow-up of biopsy-proven viral myocarditis: Predictors of mortality and incomplete recovery. J. Am. Coll Cardiol. 2012, 59, 1604–1615. [Google Scholar] [CrossRef] [PubMed]
- Lehrke, S.; Lossnitzer, D.; Schob, M.; Steen, H.; Merten, C.; Kemmling, H.; Pribe, R.; Ehlermann, P.; Zugck, C.; Korosoglou, G.; et al. Use of cardiovascular magnetic resonance for risk stratification in chronic heart failure: Prognostic value of late gadolinium enhancement in patients with non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Nowalany-Kozielska, E.; Koziel, M.; Domal-Kwiatkowska, D.; Wojciechowska, C.; Jachec, W.; Kawecki, D.; Tomasik, A.; Przywara-Chowaniec, B.; Weglarz, L.; Reichman-Warmusz, E.; et al. Clinical Significance of Viral Genome Persistence in the Myocardium of Patients with Dilated Cardiomyopathy. Intervirology 2015, 58, 350–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. Authors/Task Force, M. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Schultheiss, H.P.; Piper, C.; Sowade, O.; Waagstein, F.; Kapp, J.F.; Wegscheider, K.; Groetzbach, G.; Pauschinger, M.; Escher, F.; Arbustini, E.; et al. Betaferon in chronic viral cardiomyopathy (BICC) trial: Effects of interferon-beta treatment in patients with chronic viral cardiomyopathy. Clin. Res. Cardiol. 2016, 105, 763–773. [Google Scholar] [CrossRef]
- Dennert, R.; Velthuis, S.; Schalla, S.; Eurlings, L.; van Suylen, R.J.; van Paassen, P.; Tervaert, J.W.; Wolffs, P.; Goossens, V.J.; Bruggeman, C.; et al. Intravenous immunoglobulin therapy for patients with idiopathic cardiomyopathy and endomyocardial biopsy-proven high PVB19 viral load. Antivir. Ther. 2010, 15, 193–201. [Google Scholar] [CrossRef]
- Ak, A.; Porokhovnikov, I.; Kuethe, F.; Schulze, P.C.; Noutsias, M.; Schlattmann, P. Transcatheter vs. surgical aortic valve replacement and medical treatment: Systematic review and meta-analysis of randomized and non-randomized trials. Herz 2018, 43, 325–337. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Code | First Author | Year | Journal; Citation | Total Number of Study Subjects (n) | Number of Patients in the MC-/DCM-Group (n) | Number of Patients in the Control Group (n) |
|---|---|---|---|---|---|---|
| 01 | Kuhl | 2003 | Circulation; [21] | 24 | 24 | |
| 02 | Pankuweit | 2003 | Hum Pathol; [12] | 138 | 110 | 28 |
| 03 | Lotze | 2004 | Med Microbiol Immunol; [22] | 62 | 52 | 10 |
| 04 | Mahrholdt | 2004 | Circulation; [7] | 32 | 32 | |
| 05 | Vallbracht | 2004 | Circulation; [23] | 124 | 124 | |
| 06 | Kuhl | 2005 | Circulation; [13] | 245 | 245 | |
| 07 | Kuhl | 2005 | Circulation; [5] | 172 | 172 | |
| 08 | Kyto | 2005 | Clin Infect Dis; [24] | 52 | 40 | 12 |
| 09 | Tschöpe | 2005 | Circulation; [25] | 70 | 70 | |
| 10 | Mahrholdt | 2006 | Circulation; [26] | 128 | 128 | |
| 11 | Kuethe | 2007 | Am Heart J; [27] | 197 | 197 | |
| 12 | Escher | 2008 | Med Sci Monit; [28] | 30 | 30 | |
| 13 | Escher | 2008 | Med Sci Monit; [29] | 62 | 62 | |
| 14 | Kuhl | 2008 | J Med Virol; [30] | 317 | 317 | |
| 15 | Schenk | 2008 | J Clin Microbiol; [31] | 69 | 69 | |
| 16 | Yilmaz | 2008 | Heart; [32] | 85 | 85 | |
| 17 | Zimmermann | 2009 | Basic Res Cardiol; [33] | 66 | 66 | |
| 18 | Moulik | 2010 | J Am Coll Cardiol; [34] | 94 | 94 | |
| 19 | Zimmermann | 2010 | J Card Fail; [18] | 110 | 110 | |
| 20 | Lotze | 2010 | J Med Virol; [35] | 34 | 24 | 10 |
| 21 | Mahfoud | 2011 | Eur Heart J; [10] | 124 | 124 | |
| 22 | Ruppert | 2011 | J Med Virol; [36] | 139 | 139 | |
| 23 | Stewart | 2011 | Circ Heart Fail; [37] | 100 | 100 | |
| 24 | Dennert | 2012 | Clin Vaccine Immunol; [38] | 179 | 159 | 20 |
| 25 | Koepsell | 2012 | Cardiovasc Pathol; [39] | 45 | 26 | 19 |
| 26 | Kubanek | 2012 | Eur J Heart Fail; [40] | 56 | 41 | 15 |
| 27 | Moimas | 2012 | Heart Lung Circ; [41] | 72 | 52 | 20 |
| 28 | Kuhl | 2013 | Basic Res Cardiol; [42] | 537 | 537 | |
| 29 | Miranda | 2014 | Cardiol Young; [43] | 61 | 61 |
| S1 | S2 | |
|---|---|---|
| Number of patients (DCM/MC) (n=) | 2786 | 504 |
| Male [%] | 63.92 | 63.76 |
| Age, mean ± SD [years] | 50.62 ± 14.65 | 46.37 ± 12.2 |
| LVEF, mean ± SD [%] | 45.17 ± 11.64 | 34.18 ± 8.96 |
| LVEDD, mean ± SD [mm] | 59.95 ± 8.98 | 63.83 ± 7.56 |
| PCR positive for B19V [%] | 49.6 | 47.2 |
| Virus | n (%) |
|---|---|
| Parvovirus B19 (B19V) | 1688 (46.85%) |
| Enterovirus (EV) | 203 (5.36%) |
| Human Herpes virus-6 (HHV-6) | 176 (4.88%) |
| Adenovirus (EDV) | 44 (1.22%) |
| Epstein-Barr virus (EBV) | 30 (0.83%) |
| Cytomegalovirus (CMV) | 28 (0.77%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigopoulos, A.G.; Klutt, B.; Matiakis, M.; Apostolou, A.; Mavrogeni, S.; Noutsias, M. Systematic Review of PCR Proof of Parvovirus B19 Genomes in Endomyocardial Biopsies of Patients Presenting with Myocarditis or Dilated Cardiomyopathy. Viruses 2019, 11, 566. https://0-doi-org.brum.beds.ac.uk/10.3390/v11060566
Rigopoulos AG, Klutt B, Matiakis M, Apostolou A, Mavrogeni S, Noutsias M. Systematic Review of PCR Proof of Parvovirus B19 Genomes in Endomyocardial Biopsies of Patients Presenting with Myocarditis or Dilated Cardiomyopathy. Viruses. 2019; 11(6):566. https://0-doi-org.brum.beds.ac.uk/10.3390/v11060566
Chicago/Turabian StyleRigopoulos, Angelos G., Bianca Klutt, Marios Matiakis, Athanasios Apostolou, Sophie Mavrogeni, and Michel Noutsias. 2019. "Systematic Review of PCR Proof of Parvovirus B19 Genomes in Endomyocardial Biopsies of Patients Presenting with Myocarditis or Dilated Cardiomyopathy" Viruses 11, no. 6: 566. https://0-doi-org.brum.beds.ac.uk/10.3390/v11060566