Caucasian Ethnicity, but Not Treatment Cessation Is Associated with HBsAg Loss Following Nucleos(t)ide Analogue-Induced HBeAg Seroconversion

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Cohort Characteristics
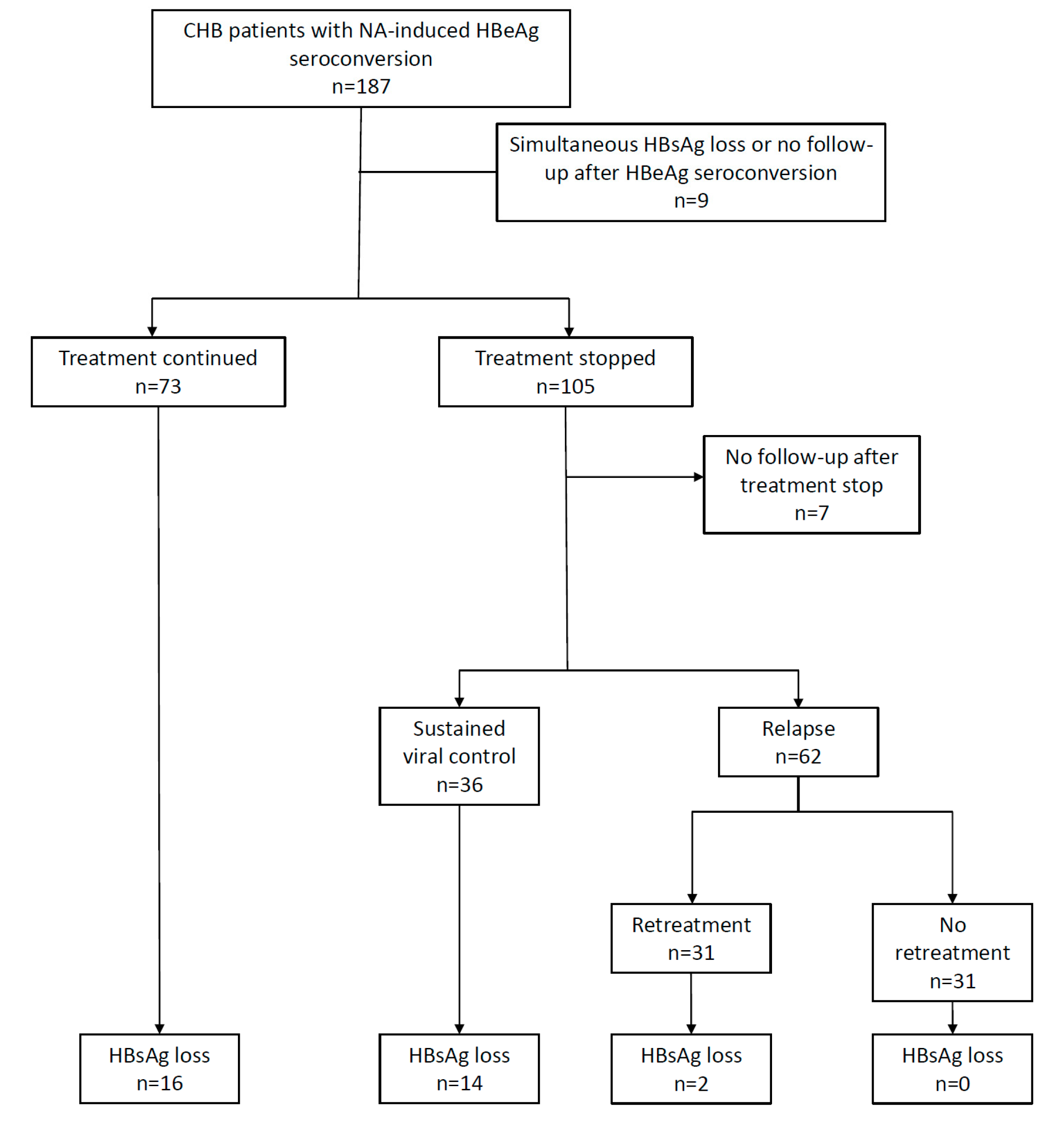
3.2. HBsAg Loss Following HBeAg Seroconversion
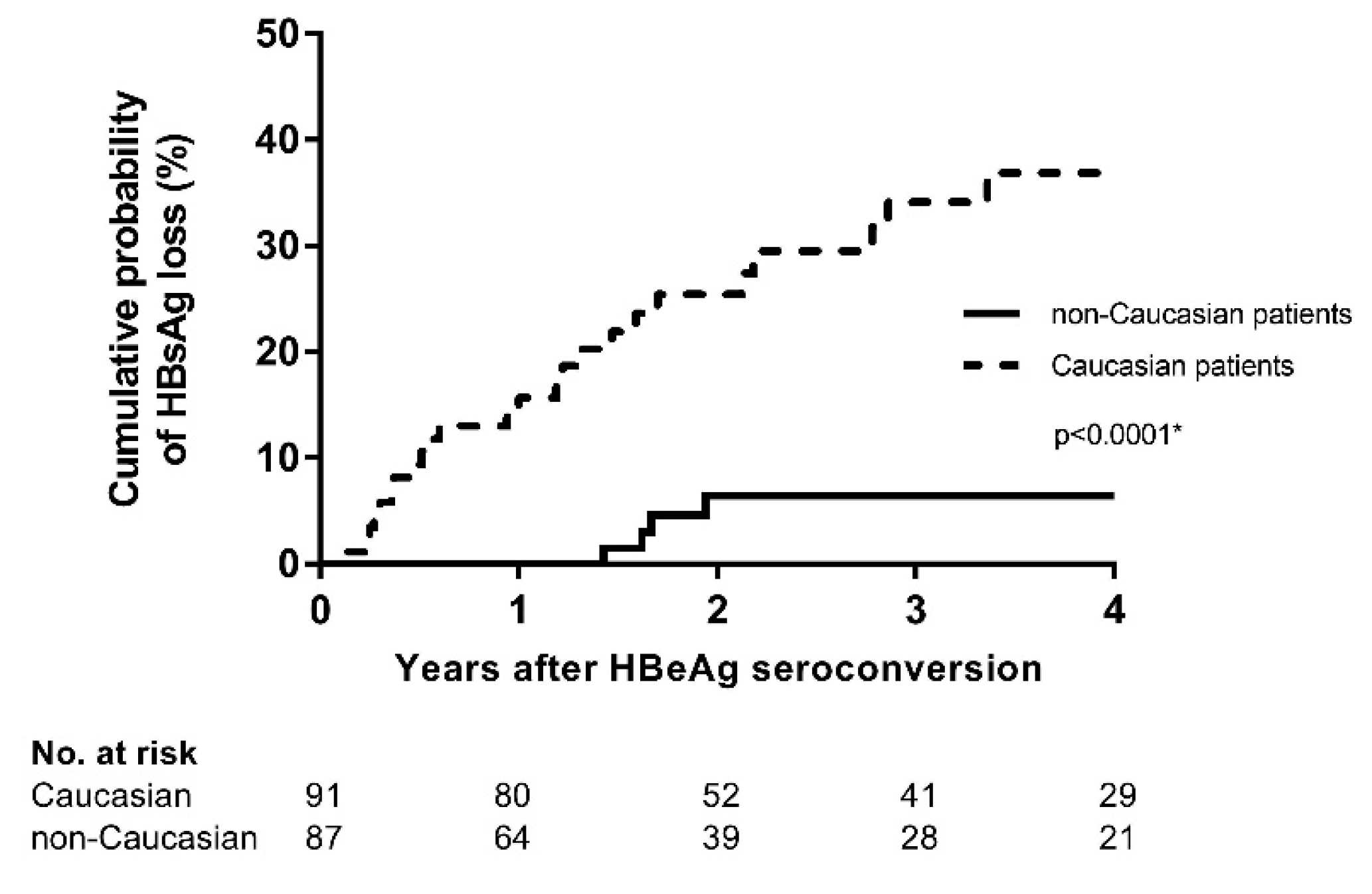
3.3. Caucasian Ethnicity, but not Treatment Cessation Is Associated with HBsAg Loss
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Seto, W.K.; Lo, Y.R.; Pawlotsky, J.M.; Yuen, M.F. Chronic hepatitis B virus infection. Lancet (Lond. Engl.) 2018, 392, 2313–2324. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Flaxman, A.D.; Naghavi, M.; Fitzmaurice, C.; Vos, T.; Abubakar, I.; Abu-Raddad, L.J.; Assadi, R.; Bhala, N.; Cowie, B.; et al. The global burden of viral hepatitis from 1990 to 2013: Findings from the Global Burden of Disease Study 2013. Lancet (Lond. Engl.) 2016, 388, 1081–1088. [Google Scholar] [CrossRef]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.C.; Sheen, I.S.; Chu, C.M.; Liaw, Y.F. Prognosis following spontaneous HBsAg seroclearance in chronic hepatitis B patients with or without concurrent infection. Gastroenterology 2002, 123, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.A.; Lim, Y.S.; An, J.; Lee, D.; Shim, J.H.; Kim, K.M.; Lee, H.C.; Chung, Y.H.; Lee, Y.S.; Suh, D.J. HBsAg seroclearance after nucleoside analogue therapy in patients with chronic hepatitis B: Clinical outcomes and durability. Gut 2014, 63, 1325–1332. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.I.; Lu, S.N.; Liaw, Y.F.; You, S.L.; Sun, C.A.; Wang, L.Y.; Hsiao, C.K.; Chen, P.J.; Chen, D.S.; Chen, C.J. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N. Engl. J. Med. 2002, 347, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Wong, D.; Peng, J.; Cao, J.; Van Hees, S.; Vanwolleghem, T.; Qi, X.; Chen, L.; Feld, J.J.; de Knegt, R.J.; et al. Durability of Response After Hepatitis B Surface Antigen Seroclearance During Nucleos(t)ide Analogue Treatment in a Multiethnic Cohort of Chronic Hepatitis B Patients: Results After Treatment Cessation. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 65, 680–683. [Google Scholar] [CrossRef]
- Zoutendijk, R.; Hansen, B.E.; van Vuuren, A.J.; Boucher, C.A.; Janssen, H.L. Serum HBsAg decline during long-term potent nucleos(t)ide analogue therapy for chronic hepatitis B and prediction of HBsAg loss. J. Infect. Dis. 2011, 204, 415–418. [Google Scholar] [CrossRef]
- Chevaliez, S.; Hezode, C.; Bahrami, S.; Grare, M.; Pawlotsky, J.M. Long-term hepatitis B surface antigen (HBsAg) kinetics during nucleoside/nucleotide analogue therapy: Finite treatment duration unlikely. J. Hepatol. 2013, 58, 676–683. [Google Scholar] [CrossRef]
- Jeng, W.J.; Chen, Y.C.; Chien, R.N.; Sheen, I.S.; Liaw, Y.F. Incidence and predictors of hepatitis B surface antigen seroclearance after cessation of nucleos(t)ide analogue therapy in hepatitis B e antigen-negative chronic hepatitis B. Hepatol. (Baltim. Md.) 2018, 68, 425–434. [Google Scholar] [CrossRef]
- Hadziyannis, S.J.; Sevastianos, V.; Rapti, I.; Vassilopoulos, D.; Hadziyannis, E. Sustained responses and loss of HBsAg in HBeAg-negative patients with chronic hepatitis B who stop long-term treatment with adefovir. Gastroenterology 2012, 143, 629–636.e1. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.H.; Wang, J.H.; Lu, S.N.; Hu, T.H.; Lee, C.M.; Chen, C.H. Hepatitis B surface antigen loss and clinical outcomes between HBeAg-negative cirrhosis patients who discontinued or continued nucleoside analogue therapy. J. Viral Hepat. 2017, 24, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Van Bommel, F.; Berg, T. Stopping long-term treatment with nucleos(t)ide analogues is a favourable option for selected patients with HBeAg-negative chronic hepatitis B. Liver Int. Off. J. Int. Assoc. Study Liver 2018, 38, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinker, F.; Zimmer, C.L.; Honer Zu Siederdissen, C.; Manns, M.P.; Kraft, A.R.M.; Wedemeyer, H.; Bjorkstrom, N.K.; Cornberg, M. Hepatitis B virus-specific T cell responses after stopping nucleos(t)ide analogue therapy in HBeAg-negative chronic hepatitis B. J. Hepatol. 2018, 69, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zou, Z.Q.; Wang, K. Clinical Relevance of HLA Gene Variants in HBV Infection. J. Immunol. Res. 2016, 2016, 9069375. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Thio, C.L.; Apps, R.; Qi, Y.; Gao, X.; Marti, D.; Stein, J.L.; Soderberg, K.A.; Moody, M.A.; Goedert, J.J.; et al. A novel variant marking HLA-DP expression levels predicts recovery from hepatitis B virus infection. J. Virol. 2012, 86, 6979–6985. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, S.; Chi, H.; Hansen, B.; Bourgeois, S.; van Vlierberghe, H.; Serste, T.; Francque, S.; Wong, D.; Sprengers, D.; Moreno, C.; et al. Sustained off-treatment viral control is associated with high hepatitis B surface antigen seroclearance rates in Caucasian patients with nucleos(t)ide analogue-induced HBeAg seroconversion. J. Viral Hepat. 2019, 26, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.S.; Fung, S.K.; Alvarez, F.; Cooper, C.L.; Doucette, K.E.; Fournier, C.; Kelly, E.; Ko, H.H.; Ma, M.M.; Martin, S.R.; et al. Management of Hepatitis B Virus Infection: 2018 Guidelines from the Canadian Association for the Study of Liver Disease and Association of Medical Microbiology and Infectious Disease Canada. Can. Liver J. 2018, 1, 156–217. [Google Scholar] [CrossRef]
- Buster, E.H.; Baak, B.C.; Bakker, C.M.; Beuers, U.H.; Brouwer, J.T.; Drenth, J.P.; van Erpecum, K.J.; van Hoek, B.; Honkoop, P.; Kerbert-Dreteler, M.J.; et al. The 2012 revised Dutch national guidelines for the treatment of chronic hepatitis B virus infection. Neth. J. Med. 2012, 70, 381–385. [Google Scholar]
- Van Hees, S.; Bourgeois, S.; van Vlierberghe, H.; Serste, T.; Francque, S.; Michielsen, P.; Sprengers, D.; Reynaert, H.; Henrion, J.; Negrin Dastis, S.; et al. Stopping nucleos(t)ide analogue treatment in Caucasian hepatitis B patients after HBeAg seroconversion is associated with high relapse rates and fatal outcomes. Aliment. Pharmacol. Ther. 2018, 47, 1170–1180. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.D.; Lin, D.Y. Time-dependent covariates in the Cox proportional-hazards regression model. Annu. Rev. Public Health 1999, 20, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, A.J.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.F.; Lammert, F.; Duarte-Rojo, A.; Heathcote, E.J.; Manns, M.P.; Kuske, L.; et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA 2012, 308, 2584–2593. [Google Scholar] [CrossRef] [PubMed]
- Westreich, D.; Cole, S.R.; Tien, P.C.; Chmiel, J.S.; Kingsley, L.; Funk, M.J.; Anastos, K.; Jacobson, L.P. Time scale and adjusted survival curves for marginal structural cox models. Am. J. Epidemiol. 2010, 171, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Eulenburg, C.; Mahner, S.; Woelber, L.; Wegscheider, K. A systematic model specification procedure for an illness-death model without recovery. PLoS ONE 2015, 10, e0123489. [Google Scholar] [CrossRef] [PubMed]
- Lim, T.H.; Gane, E.; Moyes, C.; Borman, B.; Cunningham, C. HBsAg loss in a New Zealand community study with 28-year follow-up: Rates, predictors and long-term outcomes. Hepatol. Int. 2016, 10, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Hoang, J.; Nguyen, N.H.; Vu, V.D.; Wang, C.; Trinh, H.N.; Li, J.; Zhang, J.Q.; Nguyen, M.H. Ethnic differences in incidence of hepatitis B surface antigen seroclearance in a real-life multicenter clinical cohort of 4737 patients with chronic hepatitis B infection. Aliment. Pharmacol. Ther. 2016, 44, 390–399. [Google Scholar] [CrossRef]
- Tan, A.T.; Loggi, E.; Boni, C.; Chia, A.; Gehring, A.J.; Sastry, K.S.; Goh, V.; Fisicaro, P.; Andreone, P.; Brander, C.; et al. Host ethnicity and virus genotype shape the hepatitis B virus-specific T-cell repertoire. J. Virol. 2008, 82, 10986–10997. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| NA Stop | Continuing NA | p-Value | ||
|---|---|---|---|---|
| n = 105 | n = 73 | |||
| Baseline characteristics | Male gender | 78 (74%) | 56 (77%) | 0.713 |
| Age at treatment start ° | 40.2 ± 15.2 | 41.4 ± 15.0 | 0.484 | |
| Ethnicity | 0.874 | |||
| Asian (n) | 46 | 33 | ||
| Black (n) | 7 | 5 | ||
| Caucasian (n) | 52 | 34 | ||
| Other (n) | 1 | |||
| Cirrhosis (n) | 24 (22.8%) | 30 (41.1%) | 0.012 | |
| Previous interferon treatment (n) | 24 (22.6%) | 19 (26.4%) | 0.722 | |
| HBV genotype * | 7A, 1B, 7C, 3D | 10A, 4B, 10C, 5D, 1G | 0.836 | |
| Treatment start | HBV DNA (10log) ° | 6.86 ± 1.62 | 7.13 ± 1.85 | 0.296 |
| ALT (ULN) °° | 2.9 (2.0–5.4) | 3.7 (1.7–7.0) | 0.728 | |
| Year of treatment start °° | 2006 (2003–2010) | 2010 (2007–2012) | <0.001 | |
| HBeAg seroconversion | HBV DNA (10log) ° | 1.75 ± 0.73 | 1.85 ± 1.08 | 0.588 |
| ALT (ULN) °° | 0.8 (0.5–1.0) | 0.8 (0.6-1.2) | 0.230 | |
| Type NA | <0.001 | |||
| First generation (Lamivudine-Adefovir-Telbivudine) | 62 | 12 | ||
| Second generation (Entecavir-Tenofovir) | 43 | 61 | ||
| Time to HBeAg seroconversion (months) °° | 17.8 (8.4–31.9) | 14.2 (6.0–26.4) | 0.611 | |
| FU-time after HBeAg seroconversion (months) °° | 64.9 (34.0–97.2) | 22.2 (12.0–42.1) | <0.001 | |
| Consolidation treatment (months) °° | 11.4 (6.1–18.0) | NA | NA | |
| FU-time after treatment stop (months) °° | 39.8 (13.7–81.4) | NA | NA |
| Univariate | Multivariate Model 1 | Multivariate Model 2 | Multivariate Model 3 | Multivariate Model 4 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| p | HR (95% C.I.) | p | HR (95% C.I.) | p | HR (95% C.I.) | p | HR (95% C.I.) | p | HR (95% C.I.) | ||
| Baseline characteristics | Caucasian ethnicity | 0.001 | 6.70 (2.26–21.40) | 0.032 | 3.79 (1.12–12.77) | 0.047 | 8.09 (1.03–63.81) | 0.008 | 6.03 (1.59–22.84) | 0.006 | 5.25 (1.62–17.03) |
| Male gender | 0.198 | 2.01 (0.70–5.87) | |||||||||
| Prior interferon treatment | 0.724 | 1.16 (0.51–2.62) | |||||||||
| Cirrhosis | 0.192 | 0.61 (0.28–1.29) | |||||||||
| Treatment start | Age at start of treatment (years) | 0.006 | 1.03 (1.01–1.05) | 0.095 | 1.02 (1.00–1.05) | 0.169 | 1.02 (0.99–1.05) | 0.129 | 1.02 (1.00–1.04) | ||
| ALT (per 10 units increment) | 0.724 | 1.00 (0.99–1.01) | |||||||||
| AST (per 10 units increment) | 0.475 | 1.00 (0.99–1.02) | |||||||||
| Gamma-GT (per 10 units increment) | 0.006 | 1.02 (1.01–1.04) | 0.091 | 1.02 (1.00–1.03) | |||||||
| HBV DNA (10log) | <0.001 | 2.29 (1.60–3.27) | <0.001 | 1.90 (1.36–2.66) | |||||||
| Platelets (per 104 units increment) | 0.989 | 1.00 (0.94–1.06) | |||||||||
| HBeAg seroconversion | ALT (per 10 units increment) | 0.005 | 1.07 (1.02–1.13) | 0.141 | 1.06 (0.98–1.13) | 0.028 | 1.06 (1.01–1.11) | ||||
| AST (per 10 units increment) | 0.432 | 1.07 (0.91–1.26) | |||||||||
| Gamma-GT (per 10 units increment) | 0.106 | 1.04 (0.99–1.09) | |||||||||
| HBV DNA (10log) | 0.059 | 1.63 (0.98–2.70) | 0.751 | 1.11 (0.59–2.07) | |||||||
| Platelets (per 104 units increment) | 0.273 | 1.03 (0.98–1.09) | |||||||||
| Time to HBV DNA <2000 IU/mL (years) | 0.998 | 1.00 (0.74–1.35) | |||||||||
| Time to HBeAg seroconversion (years) | 0.381 | 0.91 (0.73–1.13) | |||||||||
| First/second generation NA | 0.823 | 1.09 (0.51–2.33) | |||||||||
| Treatment cessation | Overall (Yes/No) | 0.372 | 1.45 (0.64–3.29) | ||||||||
| At least 6 months consolidation | 0.289 | 1.73 (0.63–4.79) | |||||||||
| At least 12 months consolidation | 0.525 | 1.52 (0.42–5.47) | |||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Hees, S.; Chi, H.; Hansen, B.; Bourgeois, S.; Van Vlierberghe, H.; Sersté, T.; Francque, S.; Wong, D.; Sprengers, D.; Moreno, C.; et al. Caucasian Ethnicity, but Not Treatment Cessation Is Associated with HBsAg Loss Following Nucleos(t)ide Analogue-Induced HBeAg Seroconversion. Viruses 2019, 11, 687. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080687
Van Hees S, Chi H, Hansen B, Bourgeois S, Van Vlierberghe H, Sersté T, Francque S, Wong D, Sprengers D, Moreno C, et al. Caucasian Ethnicity, but Not Treatment Cessation Is Associated with HBsAg Loss Following Nucleos(t)ide Analogue-Induced HBeAg Seroconversion. Viruses. 2019; 11(8):687. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080687
Chicago/Turabian StyleVan Hees, Stijn, Heng Chi, Bettina Hansen, Stefan Bourgeois, Hans Van Vlierberghe, Thomas Sersté, Sven Francque, David Wong, Dirk Sprengers, Christophe Moreno, and et al. 2019. "Caucasian Ethnicity, but Not Treatment Cessation Is Associated with HBsAg Loss Following Nucleos(t)ide Analogue-Induced HBeAg Seroconversion" Viruses 11, no. 8: 687. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080687