Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Dromedary Camels in Africa and Middle East

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Locations
2.2. Serological Testing
2.3. Molecular Testing
2.4. Statistical Analysis
2.5. Ethics Approval
3. Results
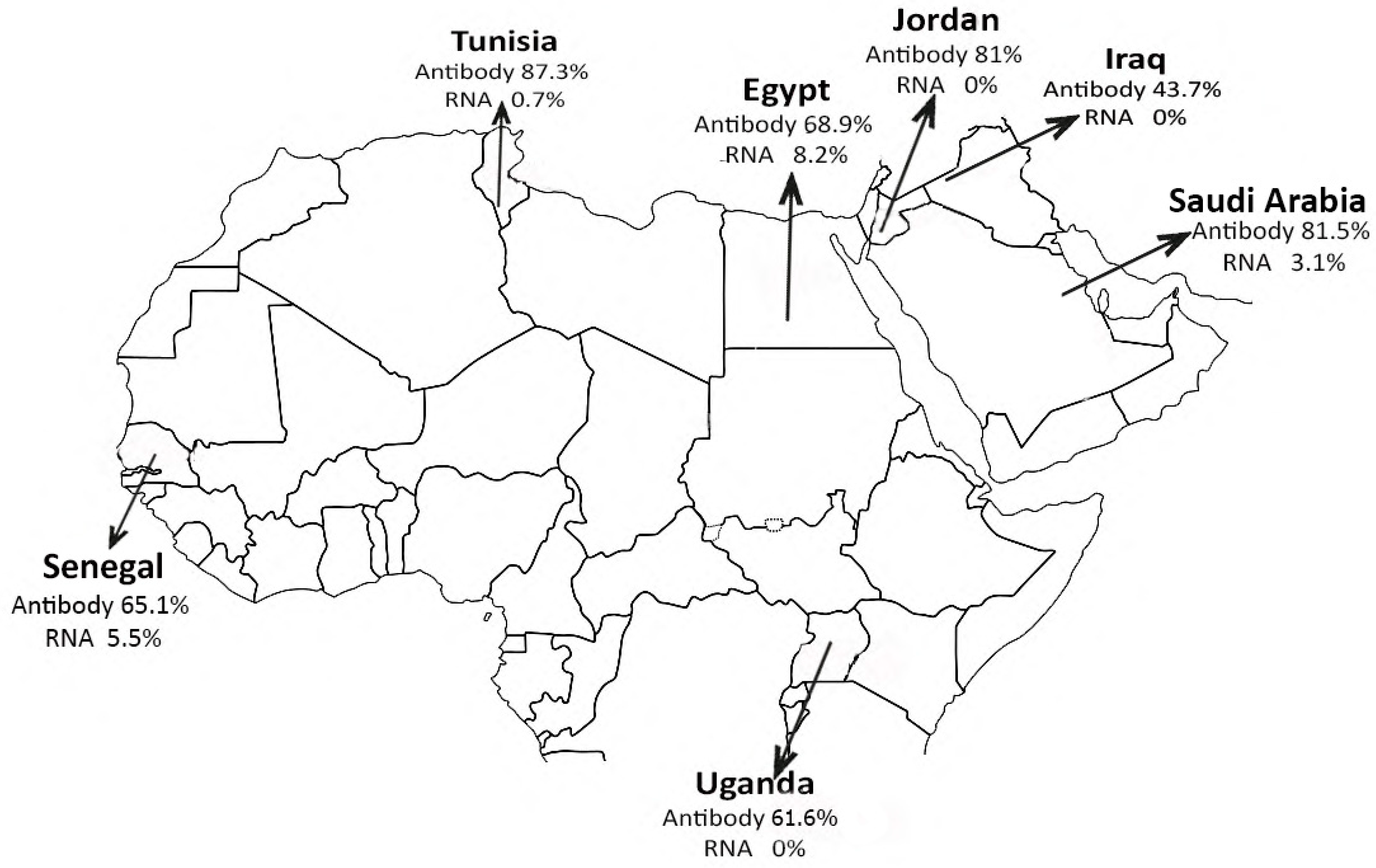
3.1. Egypt
3.2. Senegal
3.3. Uganda
3.4. Tunisia
3.5. KSA
3.6. Jordan
3.7. Iraq
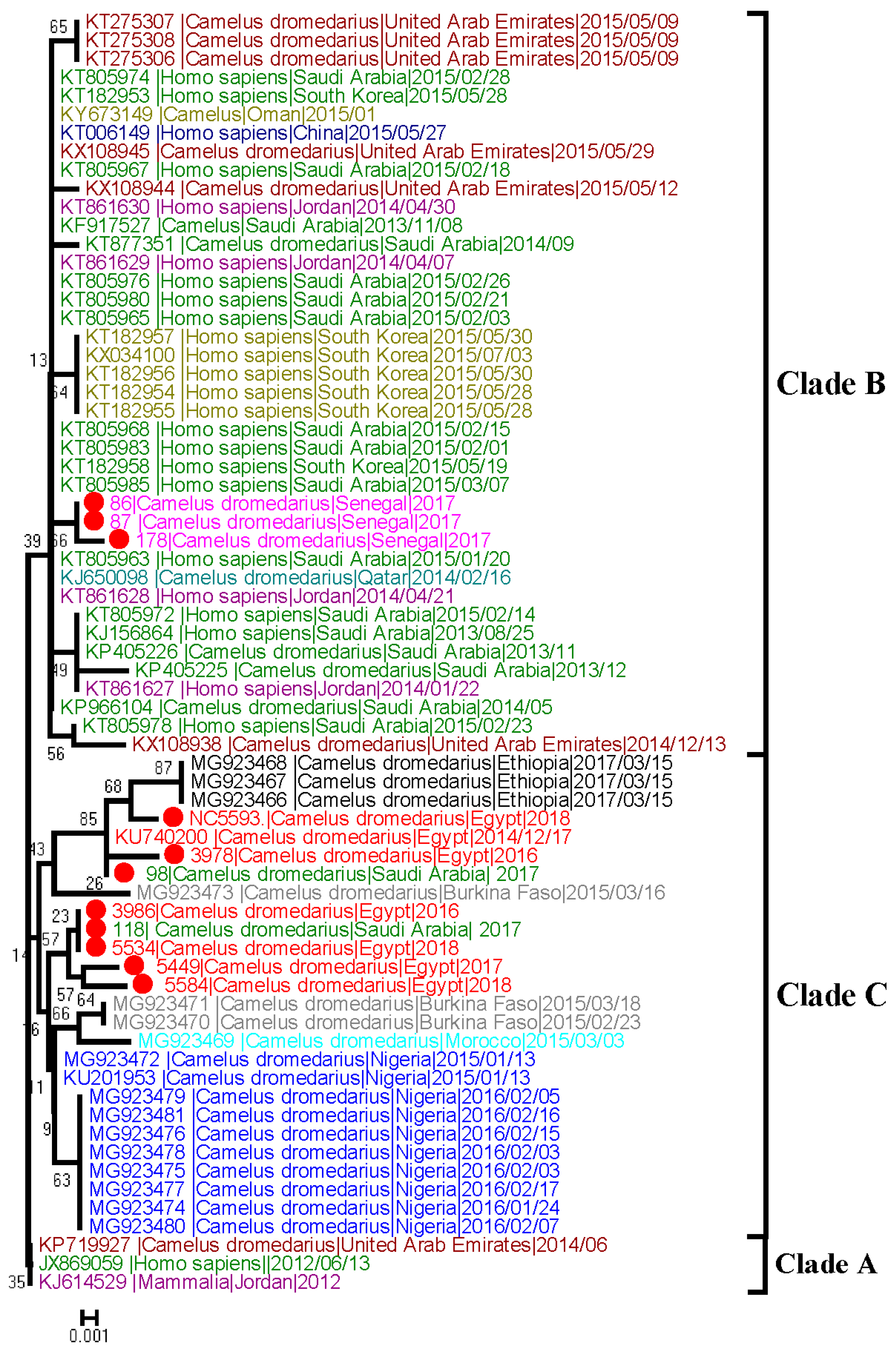
3.8. Sequence Analysis
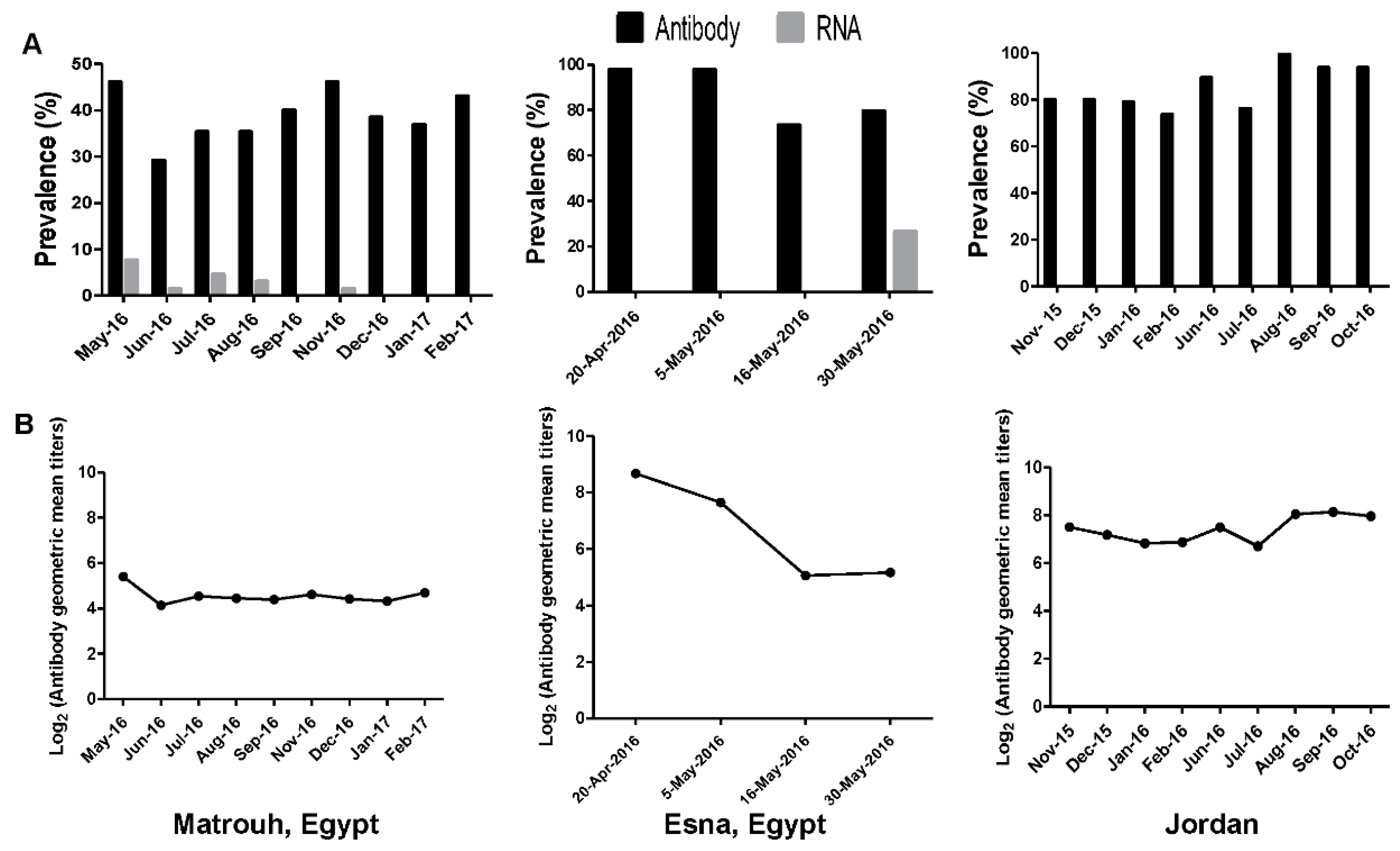
3.9. Longitudinal Studies
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Data Availability Statements
References
- Zaki, A.M.; van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a novel coronavirus from a man with pneumonia in saudi arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- WHO. Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: http://www.who.int/emergencies/mers-cov/en/ (accessed on 19 June 2019).
- Alagaili, A.N.; Briese, T.; Mishra, N.; Kapoor, V.; Sameroff, S.C.; Burbelo, P.D.; de Wit, E.; Munster, V.J.; Hensley, L.E.; Zalmout, I.S.; et al. Middle east respiratory syndrome coronavirus infection in dromedary camels in saudi arabia. mBio 2014, 5, e00884-14. [Google Scholar] [CrossRef] [PubMed]
- Meyer, B.; Muller, M.A.; Corman, V.M.; Reusken, C.B.; Ritz, D.; Godeke, G.J.; Lattwein, E.; Kallies, S.; Siemens, A.; van Beek, J.; et al. Antibodies against mers coronavirus in dromedary camels, united arab emirates, 2003 and 2013. Emerg. Infect. Dis. 2014, 20, 552–559. [Google Scholar] [CrossRef]
- Memish, Z.A.; Cotten, M.; Meyer, B.; Watson, S.J.; Alsahafi, A.J.; Al Rabeeah, A.A.; Corman, V.M.; Sieberg, A.; Makhdoom, H.Q.; Assiri, A.; et al. Human infection with mers coronavirus after exposure to infected camels, saudi arabia, 2013. Emerg. Infect. Dis. 2014, 20, 1012–1015. [Google Scholar] [CrossRef] [PubMed]
- Azhar, E.I.; El-Kafrawy, S.A.; Farraj, S.A.; Hassan, A.M.; Al-Saeed, M.S.; Hashem, A.M.; Madani, T.A. Evidence for camel-to-human transmission of mers coronavirus. N. Engl. J. Med. 2014, 370, 2499–2505. [Google Scholar] [CrossRef] [PubMed]
- Azhar, E.I.; Hashem, A.M.; El-Kafrawy, S.A.; Sohrab, S.S.; Aburizaiza, A.S.; Farraj, S.A.; Hassan, A.M.; Al-Saeed, M.S.; Jamjoom, G.A.; Madani, T.A. Detection of the middle east respiratory syndrome coronavirus genome in an air sample originating from a camel barn owned by an infected patient. mBio 2014, 5, e01450. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Cheon, S.; Min, C.K.; Sohn, K.M.; Kang, Y.J.; Cha, Y.J.; Kang, J.I.; Han, S.K.; Ha, N.Y.; Kim, G.; et al. Spread of mutant middle east respiratory syndrome coronavirus with reduced affinity to human cd26 during the south korean outbreak. mBio 2016, 7, e00019. [Google Scholar] [CrossRef]
- Memish, Z.A.; Zumla, A.I.; Al-Hakeem, R.F.; Al-Rabeeah, A.A.; Stephens, G.M. Family cluster of middle east respiratory syndrome coronavirus infections. N. Engl. J. Med. 2013, 368, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Drosten, C.; Muth, D.; Corman, V.M.; Hussain, R.; Al Masri, M.; HajOmar, W.; Landt, O.; Assiri, A.; Eckerle, I.; Al Shangiti, A.; et al. An observational, laboratory-based study of outbreaks of middle east respiratory syndrome coronavirus in jeddah and riyadh, kingdom of saudi arabia, 2014. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 60, 369–377. [Google Scholar] [CrossRef]
- FAO. Available online: http://faostat3.fao.org/browse/Q/QA/E (accessed on 20 May 2019).
- Corman, V.M.; Jores, J.; Meyer, B.; Younan, M.; Liljander, A.; Said, M.Y.; Gluecks, I.; Lattwein, E.; Bosch, B.J.; Drexler, J.F.; et al. Antibodies against mers coronavirus in dromedary camels, kenya, 1992–2013. Emerg. Infect. Dis. 2014, 20, 1319. [Google Scholar] [CrossRef]
- Perera, R.A.; Wang, P.; Gomaa, M.R.; El-Shesheny, R.; Kandeil, A.; Bagato, O.; Siu, L.Y.; Shehata, M.M.; Kayed, A.S.; Moatasim, Y.; et al. Seroepidemiology for mers coronavirus using microneutralisation and pseudoparticle virus neutralisation assays reveal a high prevalence of antibody in dromedary camels in egypt, june 2013. Euro Surveill. 2013, 18, 20574. [Google Scholar] [CrossRef] [PubMed]
- Hemida, M.G.; Chu, D.K.; Poon, L.L.; Perera, R.A.; Alhammadi, M.A.; Ng, H.Y.; Siu, L.Y.; Guan, Y.; Alnaeem, A.; Peiris, M. Mers coronavirus in dromedary camel herd, saudi arabia. Emerg. Infect. Dis. 2014, 20, 1231. [Google Scholar] [CrossRef] [PubMed]
- Reusken, C.B.; Messadi, L.; Feyisa, A.; Ularamu, H.; Godeke, G.J.; Danmarwa, A.; Dawo, F.; Jemli, M.; Melaku, S.; Shamaki, D.; et al. Geographic distribution of mers coronavirus among dromedary camels, africa. Emerg. Infect. Dis. 2014, 20, 1370–1374. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.A.; Shehata, M.M.; Gomaa, M.R.; Kandeil, A.; El-Shesheny, R.; Kayed, A.S.; El-Taweel, A.N.; Atea, M.; Hassan, N.; Bagato, O.; et al. Systematic, active surveillance for middle east respiratory syndrome coronavirus in camels in egypt. Emerg. Microbes Infect. 2017, 6, e1. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.A.; Corman, V.M.; Jores, J.; Meyer, B.; Younan, M.; Liljander, A.; Bosch, B.J.; Lattwein, E.; Hilali, M.; Musa, B.E.; et al. Mers coronavirus neutralizing antibodies in camels, eastern africa, 1983–1997. Emerg. Infect. Dis. 2014, 20, 2093–2095. [Google Scholar] [CrossRef] [PubMed]
- Omrani, A.S.; Al-Tawfiq, J.A.; Memish, Z.A. Middle east respiratory syndrome coronavirus (mers-cov): Animal to human interaction. Pathog. Glob. Health 2015, 109, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Muller, M.A.; Costabel, U.; Timm, J.; Binger, T.; Meyer, B.; Kreher, P.; Lattwein, E.; Eschbach-Bludau, M.; Nitsche, A.; et al. Assays for laboratory confirmation of novel human coronavirus (hcov-emc) infections. Euro Surveill. 2012, 17, 20334. [Google Scholar] [CrossRef] [PubMed]
- WHO. Laboratory Testing for Middle East Respiratory Syndrome Coronavirus. Available online: www.who.int/csr/disease/coronavirus_infections/MERS_Lab_recos_16_Sept_2013.pdf?ua=1 (accessed on 15 August 2018).
- Farag, E.A.; Reusken, C.B.; Haagmans, B.L.; Mohran, K.A.; Stalin Raj, V.; Pas, S.D.; Voermans, J.; Smits, S.L.; Godeke, G.J.; Al-Hajri, M.M.; et al. High proportion of mers-cov shedding dromedaries at slaughterhouse with a potential epidemiological link to human cases, qatar 2014. Infect. Ecol. Epidemiol. 2015, 5, 28305. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.; Poon, L.L.; Gomaa, M.M.; Shehata, M.M.; Perera, R.A.; Abu Zeid, D.; El Rifay, A.S.; Siu, L.Y.; Guan, Y.; Webby, R.J.; et al. Mers coronaviruses in dromedary camels, Egypt. Emerg. Infect. Dis. 2014, 20, 1049–1053. [Google Scholar] [CrossRef] [PubMed]
- Faye, B. Camel Meat in the World; CAB International: Oxfordshire, UK, 2013. [Google Scholar]
- Hemida, M.G.; Alnaeem, A.; Chu, D.K.; Perera, R.A.; Chan, S.M.; Almathen, F.; Yau, E.; Ng, B.C.; Webby, R.J.; Poon, L.L.; et al. Longitudinal study of middle east respiratory syndrome coronavirus infection in dromedary camel herds in saudi arabia, 2014–2015. Emerg. Microbes Infect. 2017, 6, e56. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.T. The one-humped camel in uganda. J. Camel Pract. Res. 2017, 24, 1–7. [Google Scholar] [CrossRef]
- Ommeh, S.; Zhang, W.; Zohaib, A.; Chen, J.; Zhang, H.; Hu, B.; Ge, X.Y.; Yang, X.L.; Masika, M.; Obanda, V.; et al. Genetic evidence of middle east respiratory syndrome coronavirus (mers-cov) and widespread seroprevalence among camels in kenya. Virol. Sin. 2018, 33, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Kasem, S.; Qasim, I.; Al-Hufofi, A.; Hashim, O.; Alkarar, A.; Abu-Obeida, A.; Gaafer, A.; Elfadil, A.; Zaki, A.; Al-Romaihi, A.; et al. Cross-sectional study of mers-cov-specific rna and antibodies in animals that have had contact with mers patients in saudi arabia. J. Infect. Public Health 2018, 11, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.W.; Hui, K.P.Y.; Perera, R.; Miguel, E.; Niemeyer, D.; Zhao, J.; Channappanavar, R.; Dudas, G.; Oladipo, J.O.; Traore, A.; et al. Mers coronaviruses from camels in africa exhibit region-dependent genetic diversity. Proc. Natl. Acad. Sci. USA 2018, 115, 3144–3149. [Google Scholar] [CrossRef] [PubMed]
- Kandeil, A.; Shehata, M.M.; El Shesheny, R.; Gomaa, M.R.; Ali, M.A.; Kayali, G. Complete genome sequence of middle east respiratory syndrome coronavirus isolated from a dromedary camel in egypt. Genome Announc. 2016, 4, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Wernery, U.; Corman, V.M.; Wong, E.Y.; Tsang, A.K.; Muth, D.; Lau, S.K.; Khazanehdari, K.; Zirkel, F.; Ali, M.; Nagy, P.; et al. Acute middle east respiratory syndrome coronavirus infection in livestock dromedaries, dubai, 2014. Emerg. Infect. Dis. 2015, 21, 1019–1022. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Sampling Variable | Microneutralization Assay | Nasal Swabs RT-PCR | ||
|---|---|---|---|---|---|
| No. Tested | No. (Positive) | No. Tested | No. (Positive) | ||
| Egypt | Sampling Site | ||||
| Live Animal Market | 309 | 254 (82.2) | 286 | 12 (4.1) | |
| Free Herd | 187 | 129 (68.9) | 187 | 3 (1.6) | |
| Farm | 924 | 474 (51.2) | 944 | 33 (3.4) | |
| Quarantine | 164 | 143 (87.1) | 164 | 2 (1.2) | |
| Slaughterhouse | 449 | 401 (89.3) | 649 | 133 (20.4) | |
| p-value | <0.0001 | <0.0001 | |||
| Governorate | |||||
| Aswan | 340 | 300 (88.2) | 317 | 4 (1.2) | |
| Beheira | 68 | 39 (57.3) | 68 | 3 (4.4) | |
| Cairo | 202 | 178 (88.1) | 265 | 57 (21.5) | |
| Giza | 287 | 236 (82.2) | 430 | 74 (17.2) | |
| Qaliobia | 93 | 87 (93.5) | 96 | 13 (13.5) | |
| Luxor | 238 | 197 (82.7) | 236 | 16 (6.7) | |
| Matrouh | 715 | 297 (41.5) | 728 | 16 (2.1) | |
| Sharkia | 90 | 67 (74.4) | 90 | 0 (0) | |
| p-value | <0.0001 | <0.0001 | |||
| Age | |||||
| Juvenile | 447 | 72 (16.1) | 462 | 8 (1.7) | |
| Adult | 1586 | 1329 (84) | 1768 | 175 (9.8) | |
| p-value | <0.0001 | <0.0001 | |||
| Sex | |||||
| Male | 1400 | 1053 (75.4) | 1592 | 169 (10.6) | |
| Female | 633 | 348 (55) | 638 | 14 (2.05) | |
| p-value | <0.0001 | <0.0001 | |||
| Animal Origin | |||||
| Imported | 922 | 798 (86.5) | 1099 | 147 (13.3) | |
| Local | 1111 | 603 (54.2) | 1131 | 36 (3.1) | |
| p-value | <0.0001 | <0.0001 | |||
| Total | 2033 | 1401 (68.9) | 2230 | 183 (8.2) | |
| Senegal | Sampling Site | ||||
| Gandon | 28 | 18 (64.2) | 0 | 0 | |
| Ndaye | 23 | 23 (100) | 23 | 1 (4.3) | |
| Gantour | 20 | 19 (95) | 20 | 1 (5) | |
| Ndoye | 43 | 30 (69.7) | 16 | 3 (18.7) | |
| Tongon | 13 | 3 (23.07) | 13 | 0 (0) | |
| Toug | 37 | 36 (97.2) | 21 | 0 (0) | |
| Rao | 34 | 0 | 34 | 2 (5.8) | |
| p-value | <0.0001 | ns | |||
| Age | |||||
| Juvenile | 17 | 5 (29.4) | 15 | 2 (13.3) | |
| Adult | 181 | 124 (68.5) | 112 | 5 (4.4) | |
| p-value | <0.01 | ns | |||
| Sex | |||||
| Male | 16 | 7 (43.7) | 15 | 2 (13.3) | |
| Female | 182 | 122 (67) | 112 | 5 (4.4) | |
| p-value | ns | ns | |||
| Total | 198 | 129 (65.1) | 127 | 7 (5.5) | |
| Uganda | Sampling Site | ||||
| Moroto | 443 | 271 (61.1) | 443 | 0 | |
| Amudat | 57 | 37 (64.9) | 57 | 0 | |
| p-value | ns | ns | |||
| Age | |||||
| Juvenile | 150 | 78 (52) | 150 | 0 | |
| Adult | 350 | 230 (65.7) | 350 | 0 | |
| p-value | <0.003 | ns | |||
| Sex | |||||
| Male | 145 | 89(61.3) | 145 | 0 | |
| Female | 355 | 219 (61.6) | 355 | 0 | |
| p-value | ns | ns | |||
| Total | 500 | 308 (61.6) | 500 | 0 (0) | |
| Tunisia | Sampling Site | ||||
| Douz | 293 | 228 (77.8) | 341 | 0 | |
| Ghlissia | 34 | 31 (91.1) | 34 | 1 (2.9) | |
| Gollaa | 24 | 13(54.1) | 24 | 0 | |
| Ksar Ghilane | 58 | 38 (65.5) | 59 | 8 (13.5) | |
| Ghidma | 208 | 208 (100) | 338 | 0 (0) | |
| Jamnah | 41 | 41 (100) | 45 | 0 (0) | |
| Zaafrana | 124 | 124 (100) | 229 | 0 (0) | |
| p-value | <0.0001 | <0.0001 | |||
| Age | |||||
| Juvenile | 28 | 28 (100) | 82 | 0 (0) | |
| Adult | 754 | 655 (86.8) | 988 | 9 (0.9) | |
| p-value | 0.02 | ns | |||
| Sex | |||||
| Male | 281 | 243 (86.4) | 550 | 9 (1.6) | |
| Female | ‘ | 440 | 620 | 0 | |
| p-value | ns | 0.001 | |||
| Total | 782 | 683 (87.3) | 1170 | 9 (0.7) | |
| KSA | Sampling Site | ||||
| Alkhomra | 36 | 29 (80.5) | 36 | 1 (2.7) | |
| alsheaeba | 17 | 10 (58.8) | 17 | 0 (0) | |
| Asfan | 62 | 56 (90.3) | 62 | 0 (0) | |
| Dahban | 26 | 19 (73.07) | 26 | 3 (11.5) | |
| Khlees | 10 | 8 (80) | 11 | 0 (0) | |
| Mecca | 19 | 17 (89.4) | 19 | 0 (0) | |
| Umm al Jurm | 12 | 10 (83.3) | 13 | 0 (0) | |
| Alad | 24 | 22 (91.6) | 24 | 3 (12.5) | |
| Um Marekh | 16 | 15 (93.7) | 16 | 0 (0) | |
| p-value | ns | 0.03 | |||
| Age | |||||
| Juvenile | 11 | 9 (81.8) | 11 | 0 (0) | |
| Adult | 211 | 172 (81.5) | 213 | 7 (3.2) | |
| p-value | ns | ns | |||
| Sex | |||||
| Male | 2 | 1 (50) | 2 | 0 (0) | |
| Female | 220 | 180 (81.8) | 222 | 7 (3.1) | |
| p-value | ns | ns | |||
| Total | 222 | 181 (81.5) | 224 | 7 (3.1) | |
| Jordan | Sampling Site | ||||
| Aqaba | 304 | 246 (80.9) | 304 | 0 (0) | |
| Age | |||||
| Juvenile | 82 | 41 (50) | 82 | 0 (0) | |
| Adult | 222 | 205 (92) | 222 | 0 (0) | |
| p-value | <0.0001 | ||||
| Sex | |||||
| Male | 7 | 2 (28.5) | 7 | 0 (0) | |
| Female | 297 | 244 (82.1) | 297 | 0 (0) | |
| p-value | <0.003 | ||||
| Total | 304 | 246 (81) | 304 | 0 0 (0) | |
| Iraq | Sampling Site | ||||
| Wasit | 14 | 13 (92.8) | 13 | 0 (0) | |
| Muthana | 13 | 1 (7.6) | 13 | 0 (0) | |
| p-value | |||||
| Age | |||||
| Juvenile | 6 | 2 (33.3) | 6 | 0 (0) | |
| Adult | 21 | 12 (57.1) | 20 | 0 (0) | |
| p-value | ns | ||||
| Sex | |||||
| Male | 9 | 5 (55.5) | 8 | 0 (0) | |
| Female | 18 | 8 (44.4) | 18 | 0 (0) | |
| p-value | ns | ||||
| Total | 32 | 14 (43.7) | 26 | 0 (0) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kandeil, A.; Gomaa, M.; Nageh, A.; Shehata, M.M.; Kayed, A.E.; Sabir, J.S.M.; Abiadh, A.; Jrijer, J.; Amr, Z.; Abi Said, M.; et al. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Dromedary Camels in Africa and Middle East. Viruses 2019, 11, 717. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080717
Kandeil A, Gomaa M, Nageh A, Shehata MM, Kayed AE, Sabir JSM, Abiadh A, Jrijer J, Amr Z, Abi Said M, et al. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Dromedary Camels in Africa and Middle East. Viruses. 2019; 11(8):717. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080717
Chicago/Turabian StyleKandeil, Ahmed, Mokhtar Gomaa, Ahmed Nageh, Mahmoud M. Shehata, Ahmed E. Kayed, Jamal S. M. Sabir, Awatef Abiadh, Jamel Jrijer, Zuhair Amr, Mounir Abi Said, and et al. 2019. "Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Dromedary Camels in Africa and Middle East" Viruses 11, no. 8: 717. https://0-doi-org.brum.beds.ac.uk/10.3390/v11080717