Case Fatality Rate Related to Microcephaly Congenital Zika Syndrome and Associated Factors: A Nationwide Retrospective Study in Brazil † †

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
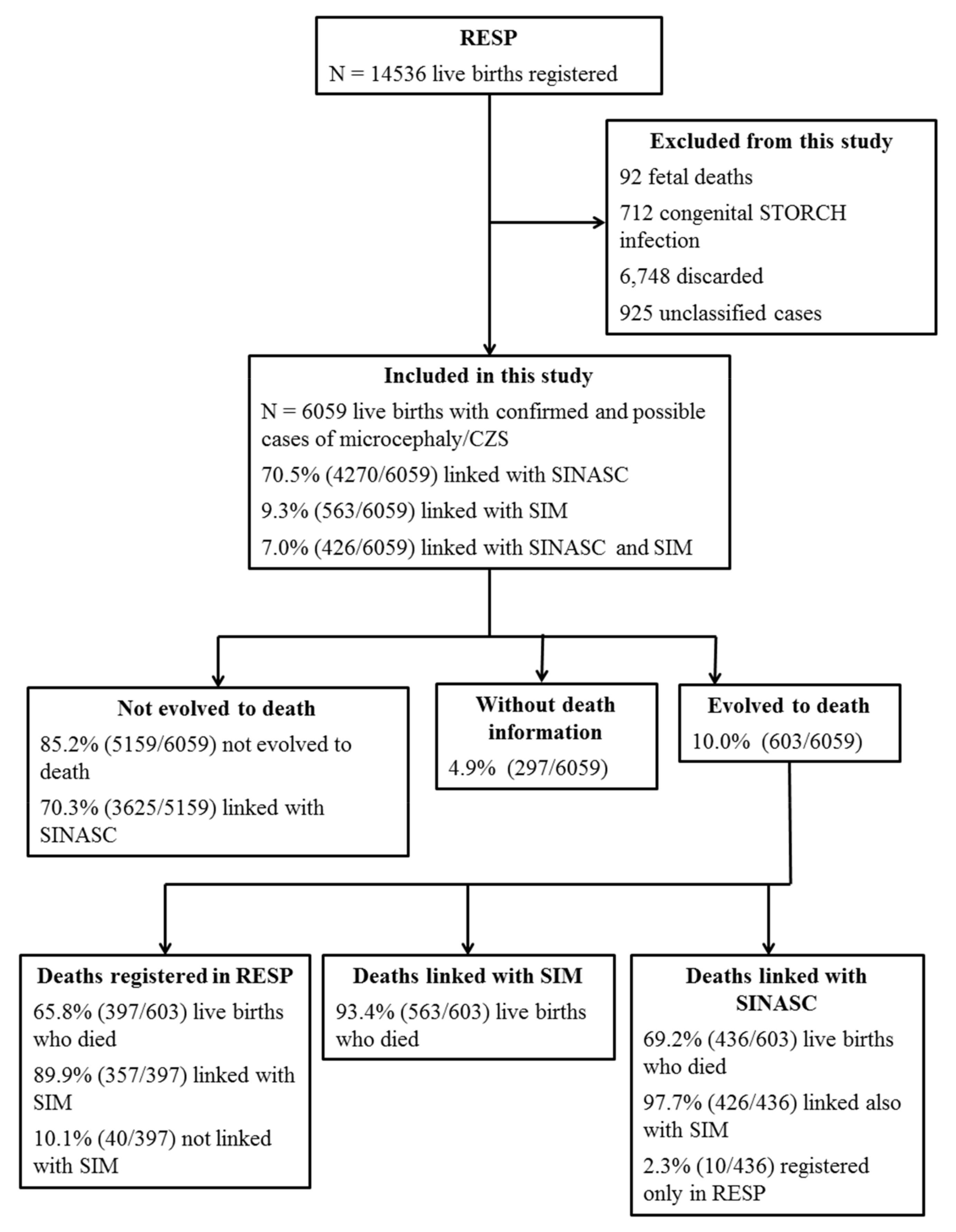
2.2. Linkage Process
2.3. Procedures
2.4. Data Analysis
2.5. Ethics Statement
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Ethics Approval
References
- Teixeira, M.G.; da Conceição NCosta, M.; de Oliveira, W.K.; Nunes, M.L.; Rodrigues, L.C. The Epidemic of Zika Virus–Related Microcephaly in Brazil: Detection, Control, Etiology, and Future Scenarios. Am. J. Public Health 2016, 106, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.A.; Jamieson, D.J.; Honein, M.A.; Petersen, L.R. Zika Virus and Birth Defects—Reviewing the Evidence for Causality. N. Engl. J. Med. 2016, 374, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Dick, G.W.A.; Kitchen, S.F.; Haddow, A.J. Zika Virus (I). Isolations and serological specificity. Trans. R. Soc. Trop. Med. Hyg. 1952, 46, 509–520. [Google Scholar] [CrossRef]
- Krauer, F.; Riesen, M.; Reveiz, L.; Oladapo, O.T.; Martínez-Vega, R.; Porgo, T.V.; Haefliger, A.; Broutet, N.J.; Low, N.; WHO Zika Causality Working Group. Zika Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain–Barré Syndrome: Systematic Review. PLoS Med. 2017, 14, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan American Health Organization. Timeline of Emergence of Zika Virus in the Americas; Pan American Health Organization: Washington, WA, USA, 2016. Available online: www.paho.org (accessed on 30 September 2020).
- World Health Organization WHO. WHO Statement on the First Meeting of the International Health Regulations. Emergency Committee on Zika Virus and Observed Increase in Neurological Disorders and Neonatal Malformations. Available online: www.who.int/mediacentre/news/statements/2016/1st-emergency-committee-zika/en/ (accessed on 28 February 2018).
- Alvarado-Socarras, J.L.; Idrovo, Á.J.; Contreras-García, G.A.; Rodriguez-Morales, A.J.; Audcent, T.A.; Mogollon-Mendoza, A.C.; Paniz-Mondolfi, A. Congenital microcephaly: A diagnostic challenge during Zika epidemics. Travel Med. Infect. Dis. 2018, 23, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde do Brasil; Secretaria de Vigilância em Saúde; Secretaria de Atenção à Saúde. Orientações Integradas de Vigilância e Atenção à Saúde no Âmbito da Emergência de Saúde Pública de Importância Nacional: Procedimentos Para o Monitoramento das Alterações no Crescimento e Desenvolvimento a Partir da Gestação Até a Primeira Infância, Relac, 1a ed.; Ministério da Saúde do Brasil: Brasília, Brazil, 2017; ISBN 9788533424890.
- Ximenes, A.S.F.C.; Pires, P.; Werner, H.; Jungmann, P.M.; Rolim Filho, E.L.; Andrade, E.P.; Lemos, R.S.; Peixoto, A.B.; Zare Mehrjardi, M.; Tonni, G.; et al. Neuroimaging findings using transfontanellar ultrasound in newborns with microcephaly: A possible association with congenital Zika virus infection. J. Matern. Neonatal Med. 2019, 32, 493–501. [Google Scholar] [CrossRef]
- Araujo, E.; Carvalho, F.H.C.; Tonni, G.; Werner, H. Prenatal imaging findings in fetal Zika virus infection. Curr. Opin. Obstet. Gynecol. 2017, 29, 95–105. [Google Scholar] [CrossRef]
- Carvalho, F.H.C.; Cordeiro, K.M.; Peixoto, A.B.; Tonni, G.; Moron, A.F.; Feitosa, F.E.L.; Feitosa, H.N.; Araujo Júnior, E. Associated ultrasonographic findings in fetuses with microcephaly because of suspected Zika virus (ZIKV) infection during pregnancy. Prenat. Diagn. 2016, 36, 882–887. [Google Scholar] [CrossRef]
- Bertolli, J.; Attell, J.E.; Rose, C.; Moore, C.A.; Melo, F.; Staples, J.E.; Kotzky, K.; Krishna, N.; Satterfield-Nash, A.; Pereira, I.O.; et al. Functional outcomes among a cohort of children in northeastern Brazil meeting criteria for follow-up of congenital Zika virus infection. Am. J. Trop. Med. Hyg. 2020, 102, 955–963. [Google Scholar] [CrossRef]
- Oliveira-Filho, J.; Felzemburgh, R.; Costa, F.; Nery, N.; Mattos, A.; Henriques, D.F.; Ko, A.I.; Fukuda, J.S.; Khouri, R.; Pereira, L.P.; et al. Seizures as a complication of congenital Zika syndrome in early infancy. Am. J. Trop. Med. Hyg. 2018, 98, 1860–1862. [Google Scholar] [CrossRef] [Green Version]
- Leal, M.C.; van der Linden, V.; Bezerra, T.P.; de Valois, L.; Borges, A.C.G.; Antunes, M.M.C.; Brandt, K.G.; Moura, C.X.; Rodrigues, L.C.; Ximenes, C.R. Characteristics of dysphagia in infants with microcephaly caused by congenital zika virus infection, Brazil, 2015. Emerg. Infect. Dis. 2017, 23, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Sauer, R.; Costa, M.D.C.N.; Barreto, F.R.; Teixeira, M.G. Congenital Zika Syndrome: Prevalence of low birth weight and associated factors. Bahia, 2015–2017. Int. J. Infect. Dis. 2019, 82, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Campo, M.; Feitosa, I.M.L.L.; Ribeiro, E.M.; Horovitz, D.D.G.G.; Pessoa, A.L.S.S.; França, G.V.A.A.; García-Alix, A.; Doriqui, M.J.R.R.; Wanderley, H.Y.C.C.; Sanseverino, M.V.T.T.; et al. The phenotypic spectrum of congenital Zika syndrome. Am. J. Med. Genet. 2017, 173, 841–857. [Google Scholar] [CrossRef] [Green Version]
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterising the pattern of anomalies in congenital zika syndrome for pediatric clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.W.W.; Choi, G.K.Y.Y.; Yip, C.C.Y.Y.; Cheng, V.C.C.C.; Yuen, K.Y. Zika fever and congenital Zika syndrome: An unexpected emerging arboviral disease. J. Infect. 2016, 72, 507–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, A.; Dua, T.; Duran, P.; Gülmezoglu, M.; Oladapo, O.T.; Perea, W.; Pires, J.; Ramon-Pardo, P.; Rollins, N.; Saxena, S. Defining the syndrome associated with congenital Zika virus infection. Bull. World Health Organ. 2016, 94, 406. [Google Scholar] [CrossRef]
- Adachi, K.; Romero, T.; Nielsen-Saines, K.; Pone, S.; Aibe, M.; Barroso De Aguiar, E.; Sim, M.; Brasil, P.; Zin, A.; Tsui, I.; et al. Clinical Infectious Diseases Early Clinical Infancy Outcomes for Microcephaly and/or Small for Gestational Age Zika-Exposed Infants. Clin. Infect. Dis. 2020, 70, 2663–2672. [Google Scholar] [CrossRef]
- Barbeito-Andrés, J.; Schuler-Faccini, L.; Garcez, P.P. Why is congenital Zika syndrome asymmetrically distributed among human populations? PLoS Biol. 2018, 16, e2006592. [Google Scholar] [CrossRef]
- Ministério da Saúde do Brasil. RESP-Registro de Eventos Em Saúde Pública. Available online: http://www.resp.saude.gov.br/microcefalia#/painel (accessed on 3 September 2020).
- De Bonilha, E.A.; Vico, E.S.R.; de Freitas, M.; Barbuscia, D.M.; Galleguillos, T.G.B.; Okamura, M.N.; Dos Santos, P.C.; de Lira, M.M.T.A.; Torloni, M.R. Cobertura, completude e confiabilidade das informações do Sistema de Informações sobre Nascidos Vivos de maternidades da rede pública no município de São Paulo, 2011. Epidemiol. E Serv. Saude Rev. Do Sist. Unico Saude Do Bras. 2018, 27, e201712811. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde do Brasil; Secretaria de Vigilância em Saúde. Coordenação Geral de Informações e Análise Epidemiológica. In Sistema de Informações Sobre Mortalidade-SIM Consolidação da Base de Dados de 2011; Ministério da Saúde do Brasil: Brasília, Brazil, 2013. [Google Scholar]
- Almeida, D.; Gorender, D.; Ichihara, M.Y.; Sena, S.; Menezes, L.; Barbosa, G.C.G.; Fiaccone, R.L.; Paixão, E.S.; Pita, R.; Barreto, M.L. Examining the quality of record linkage process using nationwide Brazilian administrative databases to build a large birth cohort. BMC Med. Inform. Decis. Mak. 2020, 20, 173. [Google Scholar] [CrossRef]
- Mendes Neto, N.N.; da Silva Maia, J.T.; Zacarkim, M.R.; Queiroz, I.; Labeaud, A.D.; Aronoff, D.M. Perinatal Case Fatality Rate Related to Congenital Zika Syndrome in Brazil: A Cross-Sectional Study. Pediatr. Neurol. 2018, 81, 47–48. [Google Scholar] [CrossRef] [Green Version]
- Da Cunha, A.J.L.A.; de Magalhães-Barbosa, M.C.; Lima-Setta, F.; Medronho, R.d.A.; Prata-Barbosa, A. Microcephaly Case Fatality Rate Associated with Zika Virus Infection in Brazil: Current Estimates. Pediatr. Infect. Dis. J. 2017, 36, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, H.; Yamada, T.; Takahashi, Y.; Nakayama, T.; Wada, T.; Kosugi, S. Epidemiology of Birth Defects in Very Low Birth Weight Infants in Japan. J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.; Lee, A.C.C.; Kozuki, N.; Lawn, J.E.; Cousens, S.; Blencowe, H.; Ezzati, M.; Bhutta, Z.A.; Marchant, T.; Willey, B.A.; et al. Mortality risk in preterm and small-for-gestational-age infants in low-income and middle-income countries: A pooled country analysis. Lancet 2013, 382, 417–425. [Google Scholar] [CrossRef] [Green Version]
- Pessoa, A.; Linden, V.V.D.; Yeargin-allsopp, M.; Costa, D.; Van Der Linden, V.; Yeargin-allsopp, M.; Carvalho, M.D.C.G.; Ribeiro, E.M.; Van Naarden Braun, K.; Durkin, M.S.; et al. Motor Abnormalities and Epilepsy in Infants and Children With Evidence of Congenital Zika Virus Infection. Pediatrics 2018, 141, S167–S179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Saúde do Brasil. Gabinete do Ministro. Portaria N° 930, de 10 de Maio de 2012. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt0930_10_05_2012.html (accessed on 22 October 2020).
- Ministério da Saúde do Brasil. DATASUS-Informações de Saúde (TABNET) Sobre Rede Assistencial. Available online: http://www2.datasus.gov.br/DATASUS/index.php?area=0204&id=1479586&VObj=http://tabnet.datasus.gov.br/cgi/deftohtm.exe?cnes/cnv/leiuti (accessed on 22 October 2020).
- Ministério da Saúde do Brasil. DATASUS TabNet Win32 3.0: Nascidos Vivos. Available online: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sinasc/cnv/nvuf.def (accessed on 22 October 2020).


{kind=link}
| Immediate (or Terminal) Cause of Death (ICD 10) | N | % |
|---|---|---|
| Respiratory insufficiency of the newborn (P28) | 71 | 12.6 |
| Unspecified septicemia (A41) | 67 | 11.9 |
| Acute Resp. insufficiency; Unspecified Resp. insuffic. (J96) | 39 | 6.9 |
| Bacterial septicemia, unspecified newborn (P36) | 41 | 7.3 |
| Unspecified Cong malformations (Q89) | 40 | 7.1 |
| Conditions originating in the specific period (P96) | 26 | 4.6 |
| Microcephaly (Q02) | 19 | 3.4 |
| Cardiog. shock; Shock Hipov; Shock not specified (R57) | 21 | 3.7 |
| Other specific symptoms and general signs (R68) | 17 | 3.0 |
| Asphyxia at birth, unspecified (P21) | 18 | 3.2 |
| Insufficiency Neonatal heart (P29) | 12 | 2.1 |
| Dextrocardia; Malform. does not specify heart (Q24) | 10 | 1.8 |
| Bronchopneumonia. (not specified (J18)) | 10 | 1.8 |
| Pulmonary hemorrhages originating in the perinatal period (P26) | 10 | 1.8 |
| Malform Cong non-brain (Q04) | 8 | 1.4 |
| Respiratory Arrest (R09) | 8 | 1.4 |
| Other causes poorly defined and unspecified (R99) | 8 | 1.4 |
| Unspecified cardiac arrest (I46) | 6 | 1.1 |
| Very low birth weight; preterm newborn (P07) | 7 | 1.2 |
| Other Causes | 125 | 22.2 |
| TOTAL | 563 | 100.0 |
| Live Birth with Microcephaly/CZS | Nonsurvivors | Survivors | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Male | Female | Total b | Male | Female | Total b | ||||||
| Characteristics | N | % | N | % | N | % | N | % | N | % | N | % |
| Birth weight (grams) | ||||||||||||
| 500–1499 | 35 | 18.4 | 38 | 16.4 | 73 | 16.9 | 44 | 2.8 | 63 | 3.1 | 107 | 3.0 |
| 1.500–2499 | 86 | 45.3 | 115 | 49.6 | 209 | 48.5 | 429 | 26.9 | 705 | 34.8 | 1134 | 31.3 |
| ≥2500 | 69 | 36.3 | 79 | 34.0 | 149 | 34.6 | 1123 | 70.4 | 1257 | 62.1 | 2381 | 65.7 |
| Prematurity | ||||||||||||
| <32 | 19 | 10.4 | 22 | 10.2 | 41 | 10.0 | 39 | 2.5 | 46 | 2.3 | 85 | 2.4 |
| 32–36 | 62 | 33.9 | 59 | 27.3 | 122 | 29.9 | 245 | 15.8 | 277 | 14.1 | 522 | 14.8 |
| ≥37 | 102 | 55.7 | 135 | 62.5 | 245 | 60.1 | 1264 | 81.7 | 1647 | 83.6 | 2912 | 82.8 |
| Apgar at 1 min | ||||||||||||
| <7 | 111 | 60.0 | 125 | 55.6 | 244 | 58.4 | 152 | 9.9 | 199 | 10.2 | 351 | 10.0 |
| 7–10 | 74 | 40.0 | 100 | 44.4 | 174 | 41.6 | 1388 | 90.1 | 1760 | 89.8 | 3149 | 90.0 |
| Apgar at 5 min | ||||||||||||
| <7 | 64 | 34.8 | 59 | 26.1 | 128 | 30.6 | 35 | 2.3 | 41 | 2.1 | 76 | 2.2 |
| 7–10 | 120 | 65.2 | 167 | 73.9 | 290 | 69.4 | 1507 | 97.7 | 1918 | 97.9 | 3426 | 97.8 |
| Congenital Anomalies | ||||||||||||
| Yes | 130 | 68.8 | 151 | 65.4 | 290 | 67.6 | 680 | 43.4 | 840 | 42.2 | 1521 | 42.7 |
| No | 59 | 31.2 | 80 | 34.6 | 139 | 32.4 | 888 | 56.6 | 1151 | 57.8 | 2039 | 57.3 |
| Small for gestational age | ||||||||||||
| No | 47 | 40.9 | 79 | 55.6 | 133 | 50.2 | 278 | 59.7 | 511 | 68.5 | 789 | 65.1 |
| Yes | 68 | 59.1 | 63 | 44.4 | 132 | 49.8 | 188 | 40.3 | 235 | 31.5 | 423 | 34.9 |
| Live Birth with Microcephaly/CZS | Nonsurvivors | Survivors | p | ||
|---|---|---|---|---|---|
| Maternal Characteristics | N | % | N | % | |
| Age group (years) | |||||
| 15–19 | 101 | 23.5 | 786 | 22.0 | |
| 20–29 | 206 | 48.0 | 1783 | 49.8 | NS b |
| 30–50 | 122 | 28.5 | 1009 | 28.2 | |
| Marital status | |||||
| Single/widow/divorced | 245 | 57.0 | 1891 | 52.8 | |
| Married/union | 185 | 43.0 | 1690 | 47.2 | NS b |
| Race/color | |||||
| White | 68 | 17.1 | 589 | 17.1 | NS b |
| Black/Mixed | 318 | 80.1 | 2824 | 82.2 | |
| Yellow/indigenous c | 11 | 2.8 | 25 | 0.7 | |
| Educational Level | |||||
| Illiterate | 3 | 0.7 | 22 | 0.6 | |
| Elementary I | 30 | 7.1 | 240 | 6.7 | |
| Elementary II | 352 | 83.2 | 2928 | 82.1 | |
| Incomplete High school | 16 | 3.8 | 139 | 3.9 | |
| Complete High School | 22 | 5.2 | 239 | 6.7 | NS b |
| Type of delivery | |||||
| Vaginal | 177 | 40.8 | 1977 | 54.6 | <0.001 |
| Caesarean section | 257 | 59.2 | 1644 | 45.4 | |
| Pregnancy type | |||||
| Only | 420 | 96.8 | 3575 | 98.7 | 0.005 * |
| Twins or more | 14 | 3.2 | 46 | 1.3 | |
| Pregnancy duration (weeks) | |||||
| <34 | 74 | 18.1 | 180 | 5.1 | |
| 34–36 | 89 | 21.8 | 427 | 12.1 | |
| ≥37 | 245 | 60.1 | 2912 | 82.8 | <0.001 |
| Numbers of prenatal visits | |||||
| <7 | 227 | 53.0 | 1508 | 42.0 | |
| ≥7 | 201 | 47.0 | 2085 | 58.0 | <0.001 |
| Newborn presentation | |||||
| Cephalic | 350 | 82.9 | 3350 | 94.4 | <0.001 * |
| Pelvic | 70 | 16.6 | 191 | 5.4 | |
| Transversal | 2 | 0.5 | 6 | 0.2 | |
| Model Variables | Crude | Adjusted | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Birth weight (g) | ||||
| 2500–7000 | 1.00 | ... | 1.00 | ... |
| 1500–2499 | 2.06 | 1.56–2.71 | 2.15 | 1.63–2.83 |
| 500–1499 | 3.56 | 2.07–6.11 | 3.77 | 2.20–6.46 |
| Number of week of gestation | ||||
| ≥37 | 1.00 | ... | 1.00 | ... |
| 32–36 | 1.65 | 1.21–2.25 | 1.65 | 1.21–2.23 |
| <32 | 1.15 | 0.59–2.23 | 1.27 | 0.66–2.42 |
| Apgar at 5 min | ||||
| 7–10 | 1.00 | ... | 1.00 | ... |
| <7 | 4.24 | 2.84–6.32 | 4.13 | 2.78–6.13 |
| Apgar at 1 min | ||||
| 7–10 | 1.00 | ... | 1.00 | ... |
| <7 | 5.91 | 4.40–7.95 | 5.98 | 4.46–8.02 |
| Congenital anomaly | ||||
| No | 1.00 | ... | 1.00 | ... |
| Yes | 2.69 | 2.06–3.50 | 2.64 | 2.03–3.43 |
| Delivery type | ||||
| Vaginal | 1.00 | ... | 1.00 | ... |
| Caesarean | 1.59 | 1.23–2.06 | 1.54 | 1.19–1.98 |
| Number of babies | ||||
| Singleton | 1.00 | ... | ... | ... |
| Twins or more | 2.75 | 1.34–5.64 | 2.63 | 1.29–5.39 |
| Numbers of prenatal visits | ||||
| ≥7 | 1.00 | ... | ... | ... |
| <7 | 1.26 | 0.97–1.63 | ... | ... |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
N. Costa, M.C.; Cardim, L.L.; Teixeira, M.G.; Barreto, M.L.; Carvalho-Sauer, R.d.C.O.d.; Barreto, F.R.; Carvalho, M.S.I.; Oliveira, W.K.; França, G.V.A.; Carmo, E.H.; et al. Case Fatality Rate Related to Microcephaly Congenital Zika Syndrome and Associated Factors: A Nationwide Retrospective Study in Brazil †. Viruses 2020, 12, 1228. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111228
N. Costa MC, Cardim LL, Teixeira MG, Barreto ML, Carvalho-Sauer RdCOd, Barreto FR, Carvalho MSI, Oliveira WK, França GVA, Carmo EH, et al. Case Fatality Rate Related to Microcephaly Congenital Zika Syndrome and Associated Factors: A Nationwide Retrospective Study in Brazil †. Viruses. 2020; 12(11):1228. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111228
Chicago/Turabian StyleN. Costa, Maria Conceição, Luciana Lobato Cardim, Maria Gloria Teixeira, Mauricio L. Barreto, Rita de Cassia Oliveira de Carvalho-Sauer, Florisneide R. Barreto, Martha Suely Itaparica Carvalho, Wanderson K. Oliveira, Giovanny V. A. França, Eduardo Hage Carmo, and et al. 2020. "Case Fatality Rate Related to Microcephaly Congenital Zika Syndrome and Associated Factors: A Nationwide Retrospective Study in Brazil †" Viruses 12, no. 11: 1228. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111228