Increasing Prevalence of HIV-1 Transmitted Drug Resistance in Portugal: Implications for First Line Treatment Recommendations

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Drug Resistance Analyses and Subtyping
2.3. Statistical Analysis
3. Results
3.1. Population
3.2. Characteristics of Portuguese Population
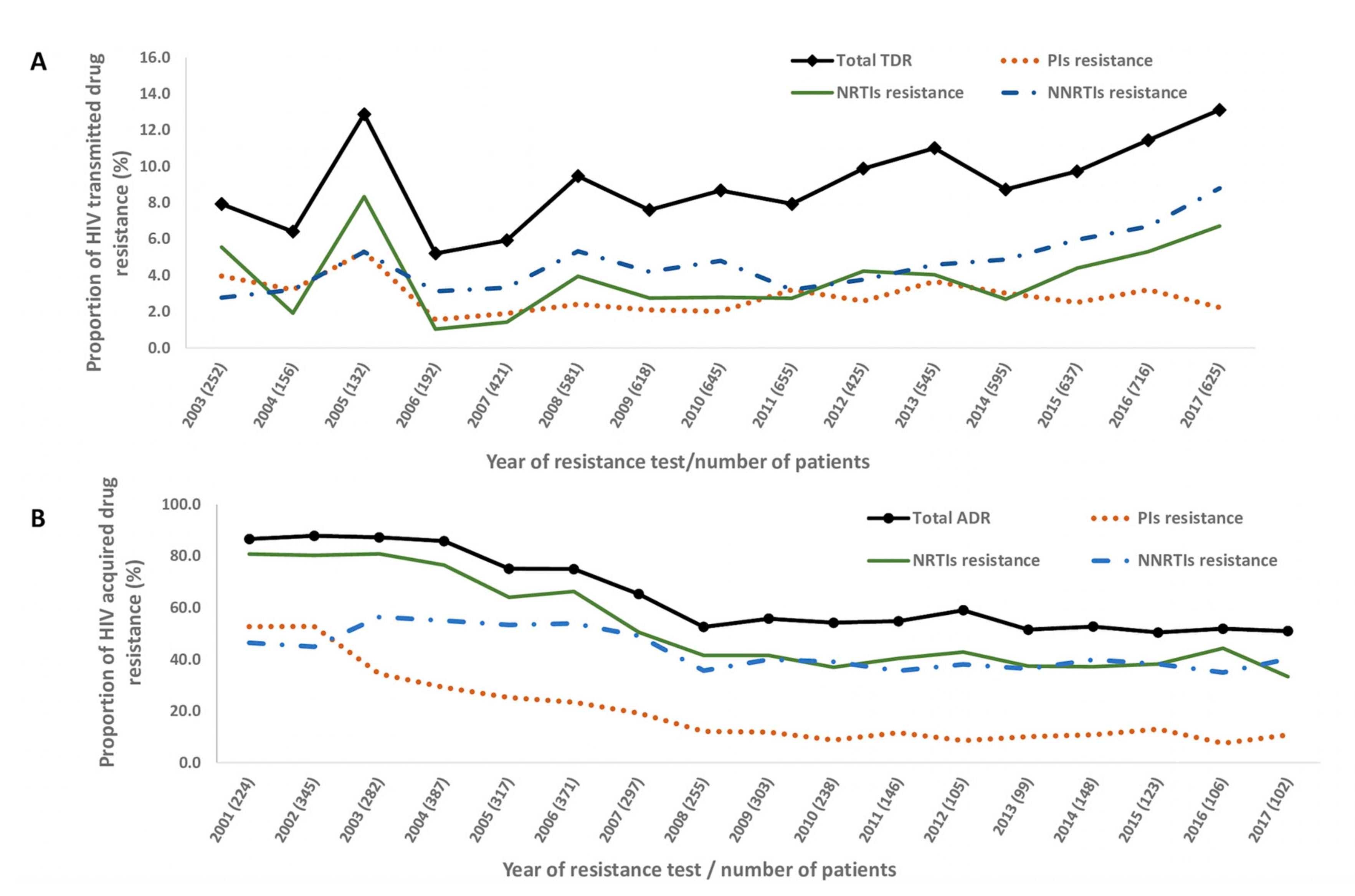
3.3. Transmitted HIV Drug Resistance (TDR)
3.4. Acquired HIV Drug Resistance (ADR)
3.5. Drug Susceptibility
3.6. Predictors of TDR
3.7. Predictors of ADR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- 90-90-90: Treatment for All. Available online: https://www.unaids.org/en/resources/909090 (accessed on 23 September 2020).
- Direção Geral da Saúde, Instituto Nacional de Saúde Doutor Ricardo Jorge. Infeção VIH e SIDA Em Portugal-2019; Direção Geral de Saúde (DGS): Lisbon, Portugal, 2019. [Google Scholar]
- Palella, F.J.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef]
- Clavel, F.; Hance, A.J. HIV drug resistance. N. Engl. J. Med. 2004, 350, 1023–1035. [Google Scholar] [CrossRef]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Prevention of HIV-1 infection with early antiretroviral therapy. N. Engl. J. Med. 2011, 365, 493–505. [Google Scholar] [CrossRef] [Green Version]
- Gazzard, B.G.; Anderson, J.; Babiker, A.; Boffito, M.; Brook, G.; Brough, G.; Churchill, D.; Cromarty, B.; Das, S.; Fisher, M.; et al. British HIV Association Guidelines for the treatment of HIV-1-infected adults with antiretroviral therapy 2008. HIV Med. 2008, 9, 563–608. [Google Scholar] [CrossRef]
- Hicks, C.B. Guideline watch. Antiretroviral drug resistance testing—Updated guidelines from the IAS-USA. AIDS Clin. Care 2008, 20, 64. [Google Scholar]
- Libin, P.; Beheydt, G.; Deforche, K.; Imbrechts, S.; Ferreira, F.; Van Laethem, K.; Theys, K.; Carvalho, A.P.; Cavaco-Silva, J.; Lapadula, G.; et al. RegaDB: Community-driven data management and analysis for infectious diseases. Bioinforma 2013, 29, 1477–1480. [Google Scholar] [CrossRef]
- Bennett, D.E.; Camacho, R.J.; Otelea, D.; Kuritzkes, D.R.; Fleury, H.; Kiuchi, M.; Heneine, W.; Kantor, R.; Jordan, M.R.; Schapiro, J.M.; et al. Drug resistance mutations for surveillance of transmitted HIV-1 drug-resistance: 2009 update. PLoS ONE 2009, 4, e4724. [Google Scholar] [CrossRef] [Green Version]
- Pineda-Peña, A.C.; Faria, N.R.; Imbrechts, S.; Libin, P.; Abecasis, A.B.; Deforche, K.; Gómez-López, A.; Camacho, R.J.; De Oliveira, T.; Vandamme, A.-M. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: Performance evaluation of the new REGA version 3 and seven other tools. Infect. Genet. Evol. 2013, 19, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Struck, D.; Lawyer, G.; Ternes, A.M.; Schmit, J.C.; Bercoff, D.P. COMET: Adaptive context-based modeling for ultrafast HIV-1 subtype identification. Nucleic Acids Res. 2014, 42, e144. [Google Scholar] [CrossRef]
- Antiretroviral Treatment of Adult HIV Infection: 2014 Recommendations of the International Antiviral Society–USA Panel Clinical Pharmacy and Pharmacology. JAMA Network. Available online: https://jamanetwork.com/journals/jama/fullarticle/1889146 (accessed on 1 October 2020).
- Pingarilho, M.; Pineda-Peña, A.; Gomes, P.; Libin, P.; Theys, K.; Abecasis, A. Molecular Epidemiology Of HIV Infection in Portuguese Migrant Population. Presented at the 15th European Meeting on HIV & Hepatitis, Rome, Italy, 30 May–1 June 2018. [Google Scholar]
- Pimentel, V.F.; Pingarilho, M.; Alves, D.A.; Diogo, I.; Fernandes, S.; Miranda, M.; Pineda-Peña, A.C.; Libin, P.; Martins, M.D.R.O.; Vandamme, A.-M.; et al. Molecular epidemiology of HIV-1 infected migrants followed up in Portugal: Trends between 2001–2017. Viruses 2020, 12, 268. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.-Y.; Blanco, J.L.; Jordan, M.R.; Taylor, J.; Lemey, P.; Varghese, V.; Hamers, R.L.; Bertagnolio, S.; De Wit, T.F.R.; Aghokeng, A.F.; et al. Geographic and temporal trends in the molecular epidemiology and genetic mechanisms of transmitted HIV-1 drug resistance: An individual-patient- and sequence-level meta-analysis. PLoS Med. 2015, 12, e1001810. [Google Scholar] [CrossRef] [Green Version]
- Rocheleau, G.; Brumme, C.; Shoveller, J.; Lima, V.; Harrigan, P. Longitudinal trends of HIV drug resistance in a large Canadian cohort, 1996–2016. Clin. Microbiol. Infect. 2018, 24, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, D.; Kollan, C.; Fätkenheuer, G.; Schülter, E.; Stellbrink, H.J.; Noah, C.; Jensen, B.-E.O.; Stoll, M.; Bogner, J.R.; Eberle, J.; et al. Estimating trends in the proportion of transmitted and acquired HIV drug resistance in a long term observational cohort in germany. PLoS ONE 2014, 9, e104474. [Google Scholar] [CrossRef] [Green Version]
- Tostevin, A.; White, E.; Dunn, D.; Croxford, S.; Delpech, V.; Williams, I.; Asboe, D.; Pozniak, A.; Churchill, D.; Geretti, A.M.; et al. Recent trends and patterns in HIV-1 transmitted drug resistance in the United Kingdom. HIV Med. 2016, 18, 204–213. [Google Scholar] [CrossRef]
- Olson, A.; Bannert, N.; Sönnerborg, A.; De Mendoza, C.; Price, M.; Zangerle, R.; Chaix, M.L.; Prins, M.; Kran, A.M.B.; Gill, J.; et al. Temporal trends of transmitted HIV drug resistance in a multinational seroconversion cohort. AIDS 2017, 32, 161–169. [Google Scholar] [CrossRef] [Green Version]
- UK Collaborative Group on HIV Drug Resistance; Dolling, D.; Sabin, C. Time trends in drug resistant HIV-1 infections in the United Kingdom up to 2009: Multicentre observational study. BMJ 2012, 345, e5253. [Google Scholar] [CrossRef] [Green Version]
- Colafigli, M.; Torti, C.; Trecarichi, E.; Albini, L.; Rosi, A.; Micheli, V.; Manca, N.; Penco, G.; Bruzzone, B.; Punzi, G.; et al. Evolution of transmitted HIV-1 drug resistance in HIV-1-infected patients in Italy from 2000 to 2010. Clin. Microbiol. Infect. 2012, 18, E299–E304. [Google Scholar] [CrossRef] [Green Version]
- Kerr, C.; Allen, N.; Moynan, D. 06/Screening for Sexual Health Infections Including Chlamydia, Gonorrhea and Syphilis in Accordance with European Aids Clinical Society (EACS) Guidelines. EACS Guidelines 2018; Morressier: Berlin, Germany, 2018. [Google Scholar]
- Lambert-Niclot, S.; Charpentier, C.; Storto, A.; Fofana, D.B.; Soulié, C.; Fourati, S.; Visseaux, B.; Wirden, M.; Morand-Joubert, L.; Masquelier, B.; et al. Prevalence of pre-existing resistance-associated mutations to rilpivirine, emtricitabine and tenofovir in antiretroviral-naive patients infected with B and non-B subtype HIV-1 viruses. J. Antimicrob. Chemother. 2013, 68, 1237–1242. [Google Scholar] [CrossRef] [Green Version]
- Ross, L.L.; Shortino, D.; Shaefer, M.S. Changes from 2000 to 2009 in the prevalence of HIV-1 containing drug resistance-associated mutations from antiretroviral therapy-naive, HIV-1-infected patients in the United States. AIDS Res. Hum. Retroviruses 2018, 34, 672–679. [Google Scholar] [CrossRef]
- Descamps, D.; Chaix, M.-L.; Montes, B.; Pakianather, S.; Charpentier, C.; Storto, A.; Barin, F.; Dos Santos, G.; Krivine, A.; Delaugerre, C.; et al. Increasing prevalence of transmitted drug resistance mutations and non-B subtype circulation in antiretroviral-naive chronically HIV-infected patients from 2001 to 2006/2007 in France. J. Antimicrob. Chemother. 2010, 65, 2620–2627. [Google Scholar] [CrossRef] [Green Version]
- Riva, C.; Lai, A.; Caramma, I.; Corvasce, S.; Violin, M.; Dehò, L.; Prati, F.; Rossi, C.; Colombo, M.C.; Capetti, A.; et al. Transmitted HIV Type 1 drug resistance and Non-B subtypes prevalence among seroconverters and newly diagnosed patients from 1992 to 2005 in Italy. AIDS Res. Hum. Retroviruses 2010, 26, 41–49. [Google Scholar] [CrossRef]
- Bracciale, L.; Colafigli, M.; Zazzi, M.; Corsi, P.; Meraviglia, P.; Micheli, V.; Maserati, R.; Gianotti, N.; Penco, G.; Setti, M.; et al. Prevalence of transmitted HIV-1 drug resistance in HIV-1-infected patients in Italy: Evolution over 12 years and predictors. J. Antimicrob. Chemother. 2009, 64, 607–615. [Google Scholar] [CrossRef]
- Pineda-Peña, A.-C.; Schrooten, Y.; Vinken, L.; Ferreira, F.; Li, G.; Trovão, N.S.; Khouri, R.; Derdelinckx, I.; De Munter, P.; Kücherer, C.; et al. Trends and predictors of transmitted drug resistance (TDR) and clusters with TDR in a local belgian HIV-1 epidemic. PLoS ONE 2014, 9, e101738. [Google Scholar] [CrossRef]
- Pimentel, V.; Serova, E.; Pingarilho, M.; Miranda, A.C.; Miranda, M.; Baptista, T.; Peres, S.; Antunes, I.; Borges, F.; Diogo, I.; et al. O Papel do Diagnóstico Tardio na Transmissão da Infeção de VIH-1 em Portugal. Presented at the 12th Joanadas de actualização em doenças infeciosas do Hospital Curry Cabral (CHULC), Lisbon, Portugal, 23–24 January 2020. [Google Scholar]
- Mourad, R.; Chevennet, F.; Dunn, D.T.; Fearnhill, E.; Delpech, V.; Asboe, D.; Gascuel, O.; Hue, S. A phylotype-based analysis highlights the role of drug-naive HIV-positive individuals in the transmission of antiretroviral resistance in the UK. AIDS 2015, 29, 1917–1925. [Google Scholar] [CrossRef]
- Drescher, S.M.; Von Wyl, V.; Yang, W.L.; Böni, J.; Yerly, S.; Shah, C.; Aubert, V.; Klimkait, T.; Taffé, P.; Furrer, H.; et al. Treatment-naive individuals are the major source of transmitted HIV-1 drug resistance in men who have sex with men in the swiss HIV cohort study. Clin. Infect. Dis. 2013, 58, 285–294. [Google Scholar] [CrossRef] [Green Version]
- Paraskevis, D.; Kostaki, E.; Magiorkinis, G.; Gargalianos, P.; Xylomenos, G.; Lazanas, M.; Chini, M.; Nikolopoulos, G.; Skoutelis, A.; Papastamopoulos, V.; et al. Prevalence of drug resistance among HIV-1 treatment-naive patients in Greece during 2003–2015: Transmitted drug resistance is due to onward transmissions. Infect. Genet. Evol. 2017, 54, 183–191. [Google Scholar] [CrossRef]
- Paraskevis, D.; Kostaki, E.; Gargalianos, P.; Xylomenos, G.; Lazanas, M.; Chini, M.; Skoutelis, A.T.; Papastamopoulos, V.; Paraskeva, D.; Antoniadou, A.; et al. Transmission dynamics of HIV-1 drug resistance among treatment-naïve individuals in Greece: The added value of molecular epidemiology to public health. Genes 2017, 8, 322. [Google Scholar] [CrossRef] [Green Version]
- Kühnert, D.; Kouyos, R.; Shirreff, G.; Pečerska, J.; Scherrer, A.U.; Böni, J.; Yerly, S.; Klimkait, T.; Aubert, V.; Günthard, H.F.; et al. Quantifying the fitness cost of HIV-1 drug resistance mutations through phylodynamics. PLOS Pathog. 2018, 14, e1006895. [Google Scholar] [CrossRef]
- Franzetti, M.; De Luca, A.; Ceccherini-Silberstein, F.; Spagnuolo, V.; Nicastri, E.; Mussini, C.; Antinori, A.; Monno, L.; Vecchiet, J.; Fanti, I.; et al. Evolution of HIV-1 transmitted drug resistance in Italy in the 2007–2014 period: A weighted analysis. J. Clin. Virol. 2018, 106, 49–52. [Google Scholar] [CrossRef]
- Scherrer, A.U.; Von Wyl, V.; Yang, W.L.; Kouyos, R.D.; Böni, J.; Yerly, S.; Klimkait, T.; Aubert, V.; Cavassini, M.; Battegay, M.; et al. Emergence of acquired HIV-1 drug resistance almost stopped in Switzerland: A 15-year prospective cohort analysis. Clin. Infect. Dis. 2016, 62, 1310–1317. [Google Scholar] [CrossRef] [Green Version]
- Cong, M.-E.; Heneine, W.; García-Lerma, J.G. The fitness cost of mutations associated with human immunodeficiency virus type 1 drug resistance is modulated by mutational interactions. J. Virol. 2006, 81, 3037–3041. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, K.L.; Lee, T.-H.; Essex, M. Replicative fitness costs of nonnucleoside reverse transcriptase inhibitor drug resistance mutations on HIV subtype C. Antimicrob. Agents Chemother. 2011, 55, 2146–2153. [Google Scholar] [CrossRef] [Green Version]
- Winand, R.; Theys, K.; Eusébio, M.; Aerts, J.; Camacho, R.J.; Gomes, P.; Suchard, M.A.; Vandamme, A.-M.; Abecasis, A.B. Assessing transmissibility of HIV-1 drug resistance mutations from treated and from drug-naive individuals. AIDS 2015, 29, 2045–2052. [Google Scholar] [CrossRef] [Green Version]
- Wertheim, J.O.; Pond, S.L.K.; Forgione, L.A.; Mehta, S.R.; Murrell, B.; Shah, S.; Smith, D.M.; Scheffler, K.; Torian, L.V. Social and genetic networks of HIV-1 transmission in New York City. PLOS Pathog. 2017, 13, e1006000. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.-L.; Kouyos, R.D.; Böni, J.; Yerly, S.; Klimkait, T.; Aubert, V.; Scherrer, A.U.; Shilaih, M.; Hinkley, T.; Petropoulos, C.; et al. Persistence of transmitted HIV-1 drug resistance mutations associated with fitness costs and viral genetic backgrounds. PLOS Pathog. 2015, 11, e1004722. [Google Scholar] [CrossRef] [Green Version]
- De Luca, A.; Dunn, D.; Zazzi, M.; Camacho, R.; Torti, C.; Fanti, I.; Kaiser, R.; Sönnerborg, A.; Codoñer, F.M.; Van Laethem, K.; et al. Declining prevalence of HIV-1 drug resistance in antiretroviral treatment-exposed individuals in Western Europe. J. Infect. Dis. 2013, 207, 1216–1220. [Google Scholar] [CrossRef] [Green Version]
- De Mendoza, C.; Garrido, C.; Corral, A.; Ramírez-Olivencia, G.; Jiménez-Nacher, I.; Zahonero, N.; González-Lahoz, J.; Soriano, V. Changing rates and patterns of drug resistance mutations in antiretroviral-experienced HIV-infected patients. AIDS Res. Hum. Retroviruses 2007, 23, 879–885. [Google Scholar] [CrossRef]
- Franzetti, M.; Violin, M.; Antinori, A.; De Luca, A.; Ceccherini-Silberstein, F.; Gianotti, N.; Torti, C.; Bonora, S.; Zazzi, M.; Balotta, C. Trends and correlates of HIV-1 resistance among subjects failing an antiretroviral treatment over the 2003–2012 decade in Italy. BMC Infect. Dis. 2014, 14, 398. [Google Scholar] [CrossRef]
- Yang, W.L.; Scherrer, A.U.; Shah, C.; Held, L.; Günthard, H.F.; Aubert, V.; Battegay, M.; Bernasconi, E.; Böni, J.; Bucher, H.C.; et al. Assessing the paradox between transmitted and acquired HIV Type 1 drug resistance mutations in the Swiss HIV cohort study from 1998 to 2012. J. Infect. Dis. 2015, 212, 28–38. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | ART-NP | ART-EP |
|---|---|---|
| Total, n (%) | 7310 (100%) | 3848 (100%) |
| Sex, n (%) | ||
| Female | 2521 (34.5%) | 1239 (32.2%) |
| Male | 4719 (64.6%) | 2588 (67.3%) |
| Median age at genotyping in years (IQR) | 38.0 (31.0–48.0) | 39.0 (33.0–46.0) |
| 18–25 | 766 (10.5%) | 153 (4.0%) |
| 26–40 | 3287 (45.0%) | 1930 (50.2%) |
| 41–55 | 2263 (31.0%) | 1366 (35.5%) |
| >56 | 843 (11.5%) | 340 (8.8%) |
| Mode of transmission, n (%) | ||
| Heterosexuals | 358 (4.9%) | 181 (4.7%) |
| Men who have sex with men | 193 (2.6%) | 69 (1.8%) |
| Intravenous drug use | 189 (2.6%) | 173 (4.5%) |
| Others | 78 (1.1%) | 106 (2.8%) |
| Unknown | 6492 (88.8%) | 3319 (86.3%) |
| Region of origin, n (%) | ||
| Portugal | 2535 (34.7%) | 1152 (29.9%) |
| Sub-Saharan Africa | 972 (13.3%) | 427 (11.1%) |
| South America | 201 (2.8%) | 46 (1.2%) |
| Europe | 81 (1.1%) | 20 (0.5%) |
| Others | 10 (0.1%) | 4 (0.1%) |
| Unknown | 3511 (48.0%) | 2199 (57.2%) |
| Year of genotyping, n (%) | ||
| 2001–2005 | 655 (9.0%) | 1555 (40.4%) |
| 2006–2009 | 1812 (24.8%) | 1226 (31.9%) |
| 2010–2013 | 2270 (31.1%) | 588 (15.3%) |
| 2014–2017 | 2573 (35.2%) | 479 (12.4%) |
| HIV-1 subtype, n (%) | ||
| Subtype B | 2686 (36.7%) | 1639 (42.6%) |
| Subtype G | 1845 (25.2%) | 1262 (32.8%) |
| Subtype C | 499 (6.8%) | 149 (3.9%) |
| Subtype A | 312 (4.3%) | 55 (1.4%) |
| Subtype F1 | 265 (3.6%) | 72 (1.9%) |
| Circulating Recombinants Forms (CRFs) | 1621 (22.2%) | 635 (16.5%) |
| Other HIV-1 subtypes | 67 (0.92%) | 28 (0.7%) |
| CD4 count at time of resistance test (cells/mL) | ||
| Median CD4 count (IQR; range) | 321.5 (145.0–505.0) (0.0–1905.0) | 262.0 (136.0–440.0) (0.0–1844.0) |
| <50 | 415 (5.7%) | 308 (8.0%) |
| 51–200 | 762 (10.4%) | 868 (22.6%) |
| 201–350 | 807 (11.0%) | 817 (21.2%) |
| 351–500 | 735 (10.1%) | 533 (13.9%) |
| 501 | 929 (12.7%) | 565 (14.7%) |
| Unknown | 3662 (50.1%) | 757 (19.7%) |
| Viral Load at time of resistance test (log10 copies/mL) | ||
| Median Log Viral Load (IQR) | 4.8 (4.2–5.4) | 4.2 (3.5–4.8) |
| <4.0 | 1111 (15.2%) | 1526 (39.7%) |
| 4.1 to 5.0 | 2354 (32.2%) | 1227 (31.9%) |
| >5.1 | 2187 (29.9%) | 620 (16.1%) |
| Unknown | 1658 (22.7%) | 475 (12.3%) |
| Transmitted Drug Resistance (TDR) | n (%) | 95% CI | OR (95% CI) | p for Trend (2003–2017) |
|---|---|---|---|---|
| Prot/RT Sequence from ART-NP | ||||
| Total | 7310 (100.0%) | |||
| Any DRMs | 690 (9.4%) | 1.046 (1.024–1.068) | <0.001 | |
| NRTI resistance | 289 (4.0%) | 3.5–4.4 | 1.053 (1.019–1.088) | 0.002 |
| NNRTI resistance | 367 (5.0%) | 4.5–5.5 | 1.053 (1.028–1.078) | <0.001 |
| PI resistance | 206 (2.8%) | 2.5–3.2 | 1.000 (0.964–1.038) | 0.985 |
| Single class resistance | 535 (7.3%) | 6.7–7.9 | 1.038 (1.014–1.063) | 0.002 |
| Dual class resistance | 138 (1.9%) | 1.6–2.2 | 1.071 (1.021–1.123) | 0.005 |
| PI + NRTI resistance | 30 (0.4%) | 0.3–0.6 | 0.891 (0.808–0.982) | 0.021 |
| PI + NNRTI resistance | 18 (0.2%) | 0.2–0.4 | 0.999 (0.883–1.132) | 0.994 |
| NRTI+NNRTI resistance | 90 (1.2%) | 0.9-1.5 | 1.163 (1.091–1.240) | <0.001 |
| Triple class resistance | 17 (0.2%) | 0.1–0.4 | 1.019 (0.895–1.160) | 0.779 |
| Acquired drug resistance (ADR) | n (%) | 95% CI | OR (95% CI) | p for trend (2001–2017) |
| Prot/RT sequence from ART-EP | ||||
| Total | 3848 (100.0%) | |||
| Any DRMs | 2657 (69.0%) | 67.6–70.5 | 0.867 (0.852–0.881) | <0.001 |
| NRTI resistance | 2225 (57.8%) | 56.2–59.4 | 0.854 (0.840–0.868) | <0.001 |
| NNRTI resistance | 1763 (45.8%) | 44.2–47.4 | 0.952 (0.938–0.967) | <0.001 |
| PI resistance | 909 (23.6%) | 22.3–25.0 | 0.822 (0.804–0.841) | <0.001 |
| Single class resistance | 798 (20.7%) | 19.0–22.0 | 1.022 (1.004–1.040) | 0.019 |
| Dual class resistance | 1478 (38.0%) | 37.0–40.0 | 0.908 (0.893–0.923) | <0.001 |
| PI + NRTI resistance | 449 (11.6%) | 10.6-12.7 | 0.813 (0.788–0.839) | <0.001 |
| PI + NNRTI resistance | 24 (0.6%) | 0.4–0.9 | 0.959 (0.870–1.058) | 0.405 |
| NRTI+NNRTI resistance | 1005 (26.0%) | 24.7–27.5 | 0.974 (0.957–0.990) | 0.002 |
| Triple class resistance | 381 (9.9%) | 9.0–10.9 | 0.840 (0.814–0.867) | <0.001 |
| Any TDR | NRTI TDR | NNRTI TDR | PI TDR | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p |
| Sex | ||||||||
| Female * | ||||||||
| Male | 1.21(0.95–1.55) | 0.124 | 1.07(0.73–1.59) | 0.708 | 1.03(0.75–1.40) | 0.852 | 1.67(1.07–2.94) | 0.024 |
| Age at diagnosis | ||||||||
| 18–25 * | ||||||||
| 26–40 | 0.97(0.69–1.36) | 0.860 | 1.33(0.72–2.44) | 0.361 | 0.75(0.49–1.15) | 0.186 | 1.78(0.91–3.50) | 0.093 |
| 41–55 | 0.98(0.68–1.40) | 0.896 | 1.74(0.63–3.07) | 0.082 | 0.76(0.48–1.21) | 0.248 | 1.44(0.70–2.94) | 0.319 |
| >56 | 1.15(0.74–1.79) | 0.520 | 1.40(0.63–3.07) | 0.405 | 1.20(0.71–2.03) | 0.498 | 2.02(0.89–4.59) | 0.091 |
| Subtypes | ||||||||
| B * | ||||||||
| Non-B | 0.74(0.60–0.92) | 0.006 | 0.45(0.31–0.65) | <0.001 | 1.19(0.89–1.59) | 0.240 | 0.65(0.45–0.94) | 0.021 |
| Viral Load (log10 copies/mL) | ||||||||
| < 4.0 * | ||||||||
| 4.1 to 5.0 | 0.73(0.56–0.96) | 0.024 | 0.42(0.28–0.63) | <0.001 | 0.70(0.49–1.00) | 0.054 | 0.76(0.49–1.19) | 0.234 |
| >5.1 | 0.66(0.49–0.87) | 0.004 | 0.38(0.25–0.59) | <0.001 | 0.65(0.44–0.94) | 0.023 | 0.50(0.31–0.83) | 0.007 |
| Any ADR | NRTI ADR | NNRTI ADR | PI ADR | |||||
| Variable | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p |
| Sex | ||||||||
| Female * | ||||||||
| Male | 1.44(1.20–1.73) | <0.001 | 1.40(1.18–1.67) | <0.001 | 1.15(0.97–1.35) | 0.112 | 1.66(1.35–2.05) | <0.001 |
| Age at diagnosis | ||||||||
| 18–25 * | ||||||||
| 26–40 | 1.12(0.73–1.73) | 0.602 | 1.13(0.74–1.72) | 0.565 | 0.85(0.57–1.27) | 0.420 | 1.71(0.95–3.07) | 0.072 |
| 41–55 | 1.07(0.69–1.67) | 0.764 | 1.11(0.72–1.70) | 0.626 | 0.83(0.55–1.25) | 0.375 | 1.76(0.97–3.18) | 0.062 |
| >56 | 1.27(0.76–2.12) | 0.367 | 1.37(0.84–2.24) | 0.207 | 0.84(0.53–1.35) | 0.481 | 2.65(1.40–5.02) | 0.003 |
| Subtypes | ||||||||
| B * | ||||||||
| Non-B | 0.68(0.57–0.80) | <0.001 | 0.61(0.52–0.72) | <0.001 | 0.98(0.84–1.14) | 0.789 | 0.64(0.54–0.77) | <0.001 |
| Viral Load (log10 copies/mL) | ||||||||
| <4.0 * | ||||||||
| 4.1 to 5.0 | 0.63(0.52–0.76) | <0.001 | 0.60(0.50–0.71) | <0.001 | 0.89(0.75–1.05) | 0.165 | 0.85(0.70–1.03) | 0.090 |
| >5.1 | 0.34(0.27–0.42) | <0.001 | 0.29(0.23–0.36) | <0.001 | 0.69(0.56–0.85) | 0.001 | 0.50(0.38–0.65) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pingarilho, M.; Pimentel, V.; Diogo, I.; Fernandes, S.; Miranda, M.; Pineda-Pena, A.; Libin, P.; Theys, K.; O. Martins, M.R.; Vandamme, A.-M.; et al. Increasing Prevalence of HIV-1 Transmitted Drug Resistance in Portugal: Implications for First Line Treatment Recommendations. Viruses 2020, 12, 1238. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111238
Pingarilho M, Pimentel V, Diogo I, Fernandes S, Miranda M, Pineda-Pena A, Libin P, Theys K, O. Martins MR, Vandamme A-M, et al. Increasing Prevalence of HIV-1 Transmitted Drug Resistance in Portugal: Implications for First Line Treatment Recommendations. Viruses. 2020; 12(11):1238. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111238
Chicago/Turabian StylePingarilho, Marta, Victor Pimentel, Isabel Diogo, Sandra Fernandes, Mafalda Miranda, Andrea Pineda-Pena, Pieter Libin, Kristof Theys, M. Rosário O. Martins, Anne-Mieke Vandamme, and et al. 2020. "Increasing Prevalence of HIV-1 Transmitted Drug Resistance in Portugal: Implications for First Line Treatment Recommendations" Viruses 12, no. 11: 1238. https://0-doi-org.brum.beds.ac.uk/10.3390/v12111238