
Hypovitaminosis D Is Associated with Higher Levels of Inflammatory Cytokines and with HAM/TSP in HTLV-Infected Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Laboratory Assays
2.3. Statistics Analyses
2.4. Ethical Considerations
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Holick, M.F. The Vitamin D Solution: A 3-Step Strategy to Cure Our Most Common; Penguin/Hudson Street Press: Youngstown, OH, USA, April 2010. [Google Scholar]
- Rosen, C.J. Clinical practice, Vitam. D Insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef]
- Thacher, T.D.; Clarke, B.L. Vitamin D insufficiency. Mayo Clin. Proc. 2011, 86, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Skrobot, A.; Demkow, U.; Wachowska, M. Immunomodulatory Role of Vitamin D: A Review. Curr. Trends Immun. Respir. Infect. 2018, 1108, 13–23. [Google Scholar] [CrossRef]
- Aranow, C. Vitamin D and the Immune System. J. Investig. Med. 2011, 59, 881–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [Green Version]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and Immune Function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and immune function: An overview. Proc. Nutr. Soc. 2011, 71, 50–61. [Google Scholar] [CrossRef] [Green Version]
- Bearden, A.; Abad, C.; Gangnon, R.; Sosman, J.M.; Binkley, N.; Safdar, N. Cross-Sectional Study of Vitamin D Levels, Immunologic and Virologic Outcomes in HIV-Infected Adults. J. Clin. Endocrinol. Metab. 2013, 98, 1726–1733. [Google Scholar] [CrossRef] [Green Version]
- Lake, J.E.; Adams, J.S. Vitamin D in HIV-Infected Patients. Curr. HIV/AIDS Rep. 2011, 8, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinzone, M.R.; Di Rosa, M.; Malaguarnera, M.; Madeddu, G.; Foca, E.; Ceccarelli, G.; d’Ettorre, G.; Vullo, V.; Fisichella, R.; Cacopardo, B.; et al. Vitamin D deficiency in HIV infection: An underestimated and undertreated epidemic. Eur Rev. Med. Pharm. Sci. 2013, 17, 1218–1232. [Google Scholar]
- Mansueto, P.; Seidita, A.; Vitale, G.; Gangemi, S.; Iaria, C.; Cascio, A. Vitamin D Deficiency in HIV Infection: Not Only a Bone Disorder. BioMed Res. Int. 2015, 2015, 1–18. [Google Scholar] [CrossRef]
- Egessain, A.; Ecassar, O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front. Microbiol. 2012, 3, 388. [Google Scholar] [CrossRef] [Green Version]
- Castro-Costa, C.M.; Araújo, A.Q.; Barreto, M.M.; Takayanagui, O.M.; Sohler, M.P.; Silva, E.L.; Paula, S.M.; Ishak, R.; Ribas, J.G.; Rovirosa, L.C.; et al. Proposal for Diagnostic Criteria of Tropical Spastic Paraparesis/HTLV-I-Associated Myelopathy (TSP/HAM). AIDS Res. Hum. Retroviruses. 2006, 22, 931–935. [Google Scholar] [CrossRef]
- Castro-Costa, C.M.; de Araújo, A.Q.-C.; Menna-Barreto, M.; Penalva-de-Oliveira, A.C. Guide of clinical management of HTLV patient: Neurological aspects. Arq. Neuropsiquiatr. 2005, 63, 548–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, M.; Eiraku, N.; Usuku, K.; Nobuhara, Y.; Matsumoto, W.; Kodama, D.; Sabouri, A.H.; Izumo, S.; Arimura, K.; Osame, M. ApaI polymorphism of vitamin D receptor gene is associated with susceptibility to HTLV-1-associated myelopathy/tropical spastic paraparesis in HTLV-1 infected individuals. J. Neurol. Sci. 2005, 232, 29–35. [Google Scholar] [CrossRef]
- Yamano, Y.; Sato, T. Clinical Pathophysiology of Human T-Lymphotropic Virus-Type 1-Associated Myelopathy/Tropical Spastic Paraparesis. Front. Microbiol. 2012, 3, 389. [Google Scholar] [CrossRef] [Green Version]
- Souza, A.; Tanajura, D.; Toledo-Cornell, C.; Santos, S.; De Carvalho, E.M. Immunopathogenesis and neurological manifestations associated to HTLV-1 infection. Rev. Da Soc. Bras. De Med. Trop. 2012, 45, 545–552. [Google Scholar] [CrossRef]
- Quaresma, J.A.S.; Yoshikawa, G.T.; Koyama, R.V.L.; Dias, G.A.S.; Fujihara, S.; Fuzii, H.T. HTLV-1, Immune Response and Autoimmunity. Viruses 2015, 8, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derakhshan, R.; Mirhoseini, A.; Ghezeldasht, S.A.; Jahantigh, H.R.; Mohareri, M.; Boostani, R.; Derakhshan, M.; Rezaee, S.A. Abnormal vitamin D and lipid profile in HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP) patients. Mol. Biol. Rep. 2019, 47, 631–637. [Google Scholar] [CrossRef]
- Osame, M. Review of WHO Kagoshima meeting and diagnostic guidelines for HAM/TSP. In Human Retrovirology: HTLV; Raven Press: New York, NY, USA, 1990; pp. 191–197. [Google Scholar]
- Hoffer, M.M.; Feiwell, E.; Perry, R.; Perry, J.; Bonnett, C. Functional Ambulation in Patients with Myelomeningocele. J. Bone Jt. Surg.-Am. Vol. 1973, 55, 137–148. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Holick, M.; Binkley, N.C.; Bischoff-Ferrari, H.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Dehée, A.; Césaire, R.; Désiré, N.; Lézin, A.; Bourdonné, O.; Béra, O.; Plumelle, Y.; Smadja, D.; Nicolas, J.-C. Quantitation of HTLV-I proviral load by a TaqMan real-time PCR assay. J. Virol. Methods 2001, 102, 37–51. [Google Scholar] [CrossRef]
- National Institute of Health (NIH). 2018. Available online: https://ods.od.nih.gov/factsheets/VitaminDHealthProfessional/ (accessed on 25 September 2021).
- Ferreira, C.E.S.; Maeda, S.S.; Batista, M.C.; Lazaretti-Castro, M.; Vasconcelos, L.S.; Madeira, M.; Soares, L.M.; Borba, V.Z.C.; Moreira, C.A. Consensus-reference ranges of vitamin D [25(OH)D] from Brazilian medical societies. Braz. Soc. Endocrinol. Metab. (SBEM). J. Bras. Patol. Med. Lab. 2017, 53, 377–381. [Google Scholar]
- Zhang, L.; Tin, A.; Brown, T.T.; Margolick, J.B.; Witt, M.D.; Palella, F.J.; Kingsley, L.A.; Hoofnagle, A.N.; Jacobson, L.P.; Abraham, A.G. Vitamin D Deficiency and Metabolism in HIV-Infected and HIV-Uninfected Men in the Multicenter AIDS Cohort Study. AIDS Res. Hum. Retrovir. 2017, 33, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Hidron, A.I.; Hill, B.; Guest, J.L.; Rimland, D. Risk Factors for Vitamin D Deficiency among Veterans with and without HIV Infection. PLoS ONE 2015, 10, e0124168. [Google Scholar] [CrossRef]
- Dao, C.N.; Patel, P.; Overton, E.T.; Rhame, F.; Pals, S.L.; Johnson, C.; Bush, T.; Brooks, J.T. the Study to Understand the Natural History of HIV and AIDS in the Era of Effective Therapy (SUN) Investigators Low Vitamin D among HIV-Infected Adults: Prevalence of and Risk Factors for Low Vitamin D Levels in a Cohort of HIV-Infected Adults and Comparison to Prevalence among Adults in the US General Population. Clin. Infect. Dis. 2011, 52, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, N.; Costa, L.; Pinto, M.; Rosinha, P.; Rosinha, I.; Couto, M. Vitamin D and HIV Infection: A Systematic Review. J. Immunodefic. Disord. 2014, 3, 1. [Google Scholar]
- Rejnmark, L.; Bislev, L.S.; Cashman, K.D.; Eiríksdottir, G.; Gaksch, M.; Gruebler, M.; Grimnes, G.; Gudnason, V.; Lips, P.; Pilz, S.; et al. Non-skeletal health effects of vitamin D supplementation: A systematic review on findings from meta-analyses summarizing trial data. PLoS ONE 2017, 12, e0180512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepherd, L.; Souberbielle, J.-C.; Bastard, J.-P.; Fellahi, S.; Capeau, J.; Reekie, J.; Reiss, P.; Blaxhult, A.; Bickel, M.; Leen, C.; et al. Prognostic Value of Vitamin D Level for All-cause Mortality, and Association With Inflammatory Markers, in HIV-infected Persons. J. Infect. Dis. 2014, 210, 234–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckard, A.R.; Judd, S.E.; Ziegler, T.R.; Camacho-Gonzalez, A.F.; Fitzpatrick, A.M.; Hadley, G.R.; Grossmann, R.E.; Seaton, L.; Seydafkan, S.; Mulligan, M.J.; et al. Risk factors for vitamin D deficiency and relationship with cardiac biomarkers, inflammation and immune restoration in HIV-infected youth. Antivir. Ther. 2012, 17, 1069–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansemant, T.; Mahy, S.; Piroth, C.; Ornetti, P.; Ewing, S.; Guilland, J.-C.; Croisier, D.; Duvillard, L.; Chavanet, P.; Maillefert, J.-F.; et al. Severe hypovitaminosis D correlates with increased inflammatory markers in HIV infected patients. BMC Infect. Dis. 2013, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Rafatpanah, H.; Hosseini, R.F.; Pourseyed, S.H. The Impact of Immune Response on HTLV-I in HTLV-I-Associated Myelopathy/Tropical Spastic Paraparesis (HAM/TSP). Iran. J. Basic Med. Sci. 2013, 16, 235–241. [Google Scholar] [PubMed]
- Aguilar-Jiménez, W.; Zapata, W.; Rugeles, L.M.T. Participación de la vitamina D en la patogénesis de la infección por el virus de la inmunodeficiencia humana tipo Infectio. Rev. Asoc. Colomb. Infectología. 2013, 17, 146–152. [Google Scholar]
- Haug, C.J.; Aukrust, P.; Haug, E.; Mørkrid, L.; Müller, F.; Frøland, S.S. Severe Deficiency of 1,25-Dihydroxyvitamin D3 in Human Immunodeficiency Virus Infection: Association with Immunological Hyperactivity and Only Minor Changes in Calcium Homeostasis. J. Clin. Endocrinol. Metab. 1998, 83, 3832–3838. [Google Scholar] [CrossRef]
- Hanevold, C.; Yamaguchi, D.; Jordan, S. Tumor necrosis factor α modulates parathyroid hormone action in UMR-106-01 osteoblastic cells. J. Bone Miner. Res. 2009, 8, 1191–1200. [Google Scholar] [CrossRef]
- Neco, H.V.P.D.C.; Teixeira, V.G.D.S.; da Trindade, A.C.L.; Magalhães, P.M.R.; de Lorena, V.M.B.; Castellano, L.R.C.; de Souza, J.R.; Vasconcelos, L.R.; de Moura, P.M.M.F.; de Morais, C.N.L. Mediators Go Together: High Production of CXCL9, CXCL10, IFN-γ, and TNF-α in HTLV-1-Associated Myelopathy/Tropical Spastic Paraparesis. AIDS Res. Hum. Retrovir. 2017, 33, 1134–1139. [Google Scholar] [CrossRef]
- Luna, T.; Santos, S.; Nascimento, M.; Porto, M.; Muniz, A.; Carvalho, E.; Jesus, A. Effect of TNF-α production inhibitors on the production of pro-inflammatory cytokines by peripheral blood mononuclear cells from HTLV-1-infected individuals. Braz. J. Med Biol. Res. 2011, 44, 1134–1140. [Google Scholar] [CrossRef] [Green Version]
- Ijichi, S.; Izumo, S.; Eiraku, N.; Machigashira, K.; Kubota, R.; Nagai, M.; Ikegami, N.; Kashio, N.; Umehara, F.; Maruyama, I.; et al. An autoaggressive process against bystander tissues in HTLV-I-infected individuals: A possible pathomechanism of HAMTSP. Med. Hypotheses 1993, 41, 542–547. [Google Scholar] [CrossRef]
- Hoe, E.; Nathanielsz, J.; Toh, Z.Q.; Spry, L.; Marimla, R.; Balloch, A.; Mulholland, K.; Licciardi, P.V. Anti-Inflammatory Effects of Vitamin D on Human Immune Cells in the Context of Bacterial Infection. Nutrients 2016, 8, 806. [Google Scholar] [CrossRef] [Green Version]
- Cantorna, M.T.; Snyder, L.; Lin, Y.-D.; Yanng, L. Vitamin D and 1, 25(OH)2D regulation of T cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netto, E.; Gomes-Neto, M.; Brites, C. Vitamin D and HTLV Infection: A Systematic Review. Open Infect. Dis. J. 2019, 11, 35–42. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | HAM/TSP N = 129 (%) | HTLV-Asymptomatic Carriers N = 32 (%) | HTLV-Negative Controls N = 161 (%) | p-Value |
|---|---|---|---|---|
| Gender Male Female | 38 (29.5) 91 (70.5) | 8 (25) 24 (75) | 46 (28.6) 115 (71.4) | 0.88 |
| Age in Years (Mean ± SD) | 51.6 ± 13.6 | 48.5 ± 13.4 | 51.6 ± 13.5 | 0.58 |
| Variables | HTLV+ (N = 161) 1 | HAM/TSP (N = 129) 2 | Asymptomatic Carriers HTLV 3 (N = 32) | Controls (N = 161) |
|---|---|---|---|---|
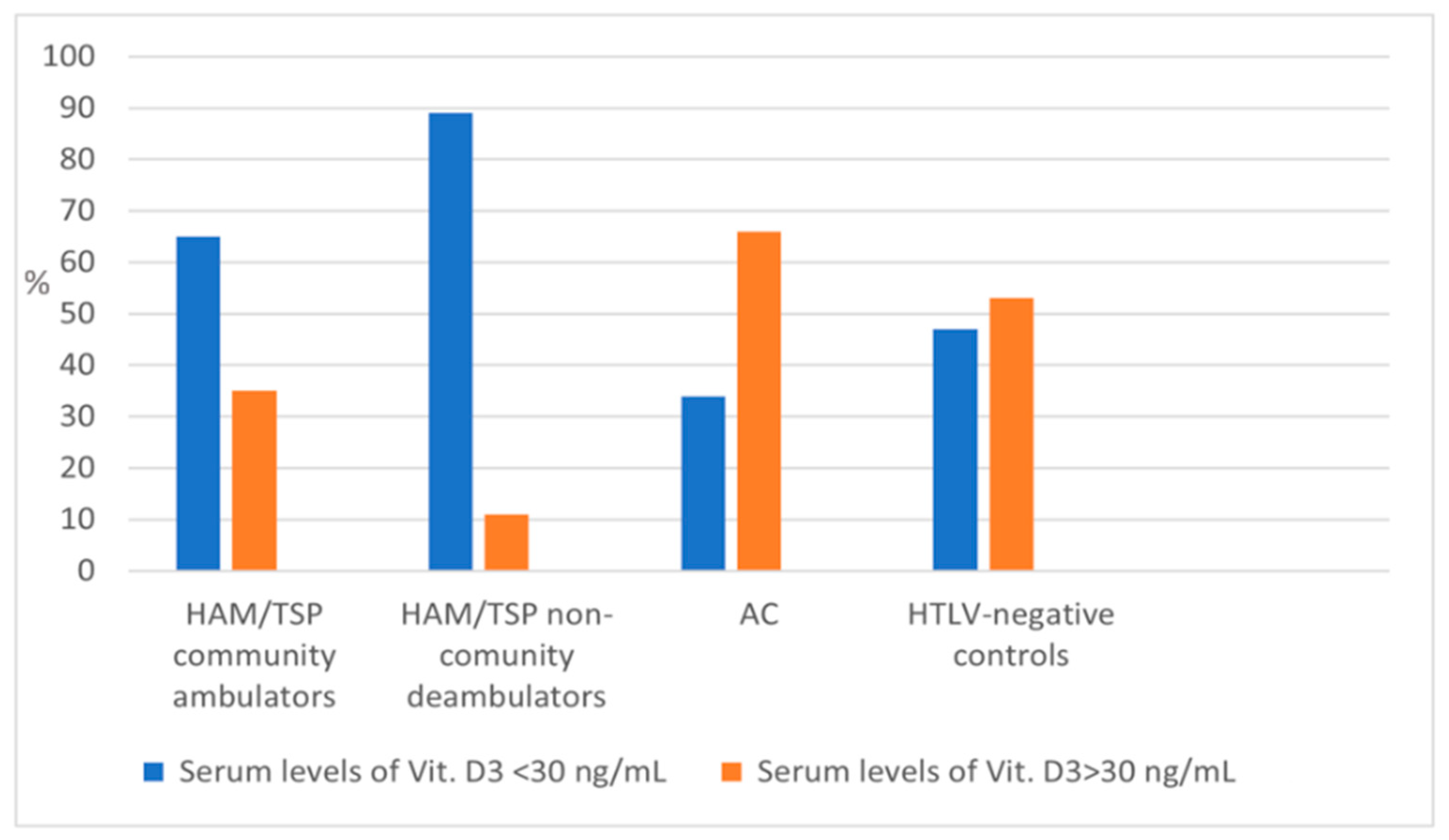
| Mean 25(OH)D3 * ng/mL (SD) 25(OH)D <20 (%) ** 25(OH)D ≥ 20 (%) ** 25(OH)D < 30 (%) *** 25(OH)D ≥ 30 (%) *** | 26.3 (10.5) 47 (29.2%) 114 (70.8%) 105 (65.3%) 56 (34.7%) | 24.5 (10.3) 46 (35.7%) 83 (64.3%) 94 (72.9%) 35 (27.1%) | 33.5 (8.3) 1 (3.1%) 31 (96.8%) 11 (34.4%) 21 (65.6%) | 29.5 (10.3) 30 (18.6%) 131 (81.4%) 82 (51%) 79 (49%) |
| Mean proviral HTLV load (copies of HTLV-1/105 cells/mLSD ) | - | 5.94 ± 14.04 | 508 ± 1.04 | - |
| Serum Levels of Pro-Inflammatory Cytokines (pg/mL) | HAM/TSP | HTLV-Asymptomatic Carriers | p-Value |
|---|---|---|---|
| IL-2 | 74.1 (39.9–92.1) | 50.2 (31–85.8) | 0.121 1 |
| IL-6 | 87.8 (52.7–117.3) | 34.8 (26.2–91) | <0.001 2 |
| TNF-α | 41.2 (8.1–81.5) | 58.1 (31.4–64.4) | 0.341 3 |
| IFN-γ | 98.2 (58.6–171) | 66.2 (32.2–108.6) | 0.001 4 |
| Serum Levels of Pro-Inflammatory Cytokines (pg/mL) | HAM/TSP | HTLV-Asymptomatic Carriers | p-Value |
|---|---|---|---|
| IL-2 | 74.1 (39.9–92.1) | 50.2 (31–85.8) | 0.121 1 |
| IL-6 | 87.8 (52.7–117.3) | 34.8 (26.2–91) | <0.001 2 |
| TNF-α | 41.2 (8.1–81.5) | 58.1 (31.4–64.4) | 0.341 3 |
| IFN-γ | 98.2 (58.6–171) | 66.2 (32.2–108.6) | 0.001 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Netto, E.C.; Silva, A.C.; Pedroso, C.; Brites, C. Hypovitaminosis D Is Associated with Higher Levels of Inflammatory Cytokines and with HAM/TSP in HTLV-Infected Patients. Viruses 2021, 13, 2223. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112223
Netto EC, Silva AC, Pedroso C, Brites C. Hypovitaminosis D Is Associated with Higher Levels of Inflammatory Cytokines and with HAM/TSP in HTLV-Infected Patients. Viruses. 2021; 13(11):2223. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112223
Chicago/Turabian StyleNetto, Elaine Coutinho, Alfredo Carlos Silva, Célia Pedroso, and Carlos Brites. 2021. "Hypovitaminosis D Is Associated with Higher Levels of Inflammatory Cytokines and with HAM/TSP in HTLV-Infected Patients" Viruses 13, no. 11: 2223. https://0-doi-org.brum.beds.ac.uk/10.3390/v13112223