
Characteristics and Factors Associated with SARS-CoV-2 Infections in Individuals That Attended Referral Hospitals from Southern Region of Bahia State, Brazil: A Surveillance Network Retrospective Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Curation
2.2. Laboratory Diagnosis
2.3. COVID-19 Symptoms Assessment
2.4. Assessment of the Period of Symptoms until Laboratory Testing
2.5. Assessment of Factors Associated with SARS-CoV-2 Infection
2.6. Ethical Considerations
3. Results
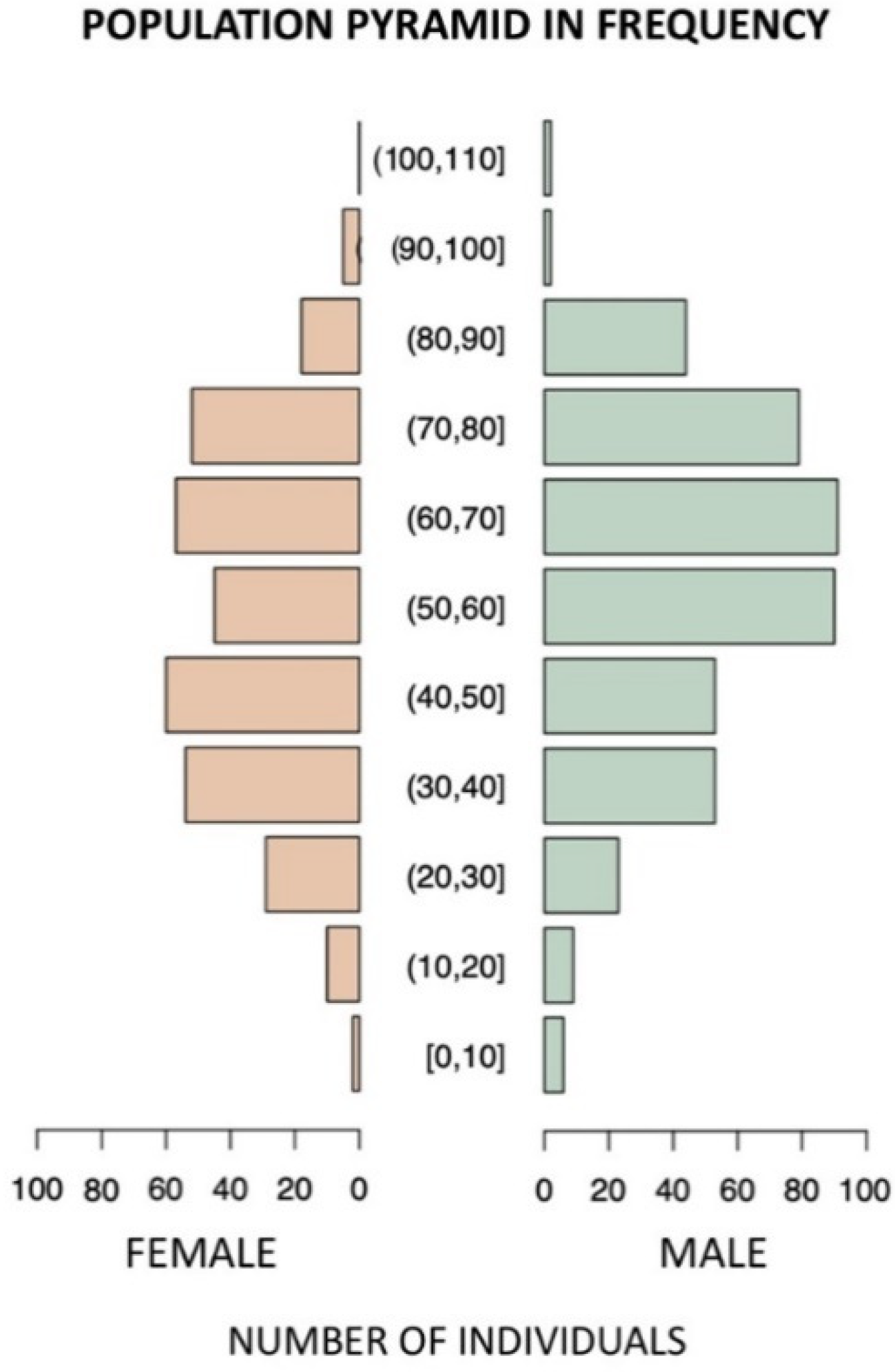
3.1. Demographic Characteristics of Study Population
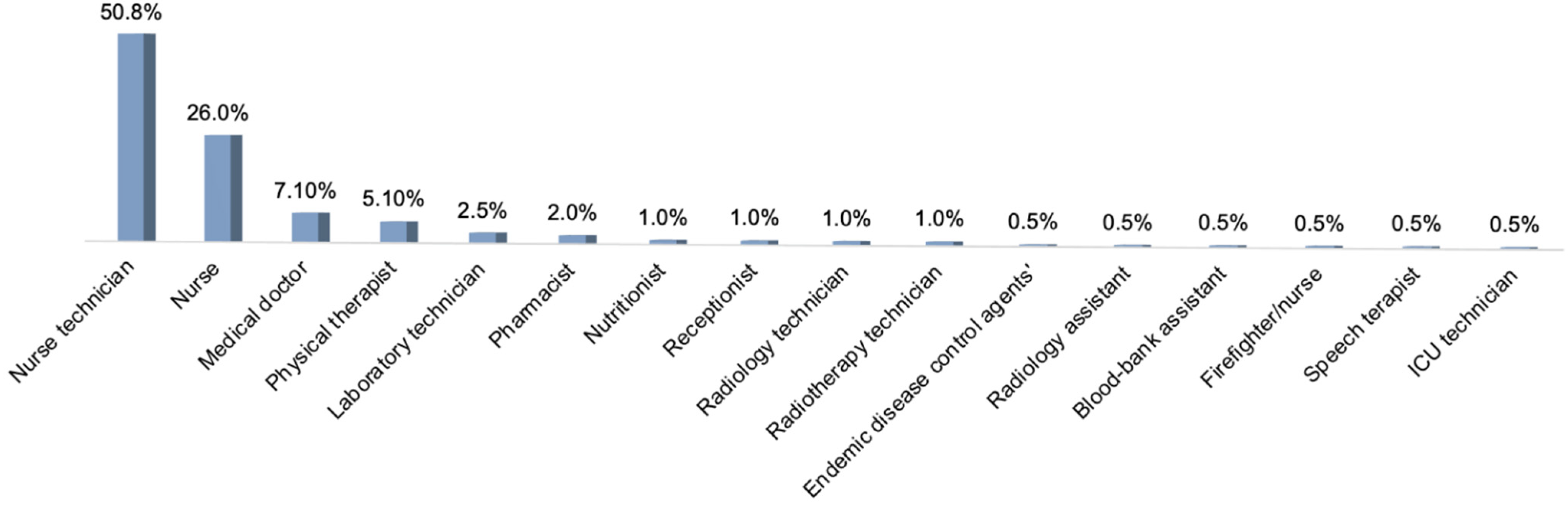
3.2. Occupational Status of Study Participants
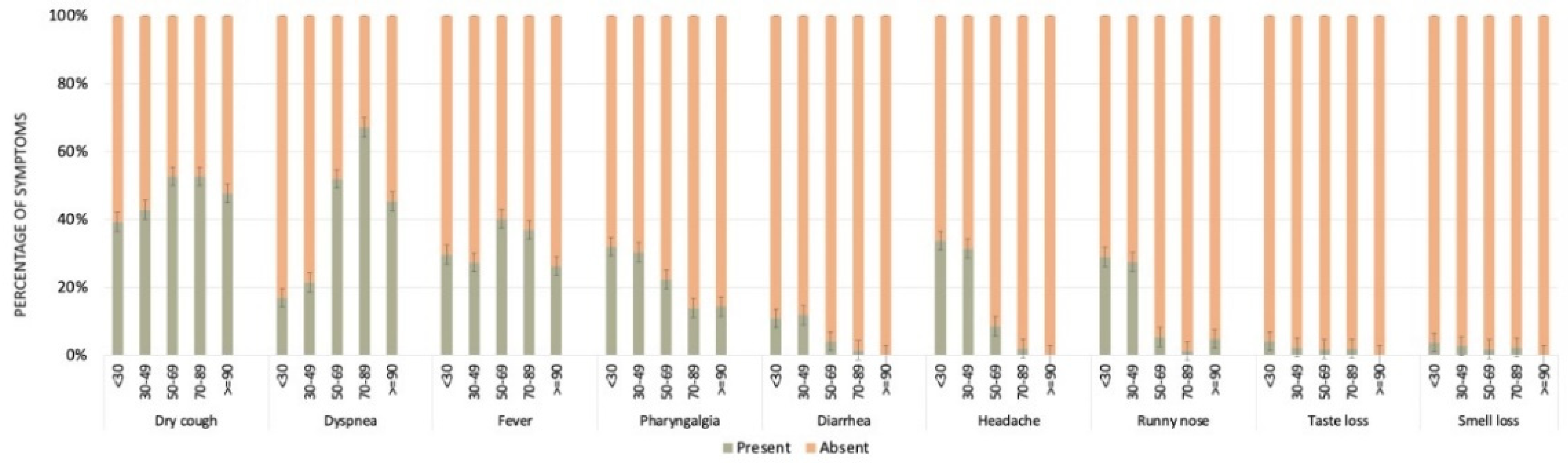
3.3. Characterization of Clinical Symptoms
3.4. Period of Onset of Clinical Symptoms until Laboratory Testing
3.5. Factors Significantly Associated with SARS-CoV-2 Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation report–51. Geneva, Switzerland: World Health Organization. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10pdficon (accessed on 11 June 2021).
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- de Jesus, J.G.; Sacchi, C.; Candido, D.D.S.; Claro, I.M.; Sales, F.C.S.; Manuli, E.R.; da Silva, D.B.B.; de Paiva, T.M.; Pinho, M.A.B.; Santos, K.C.D.O.; et al. Importation and early local transmission of COVID-19 in Brazil, 2020. Revista do Instituto de Medicina Tropical de São Paulo 2020, 62, e30. [Google Scholar] [CrossRef]
- Brasil Coronavírus Brasil. Available online: https://covid.saude.gov.br/ (accessed on 12 June 2020).
- Lai, C.C.; Liu, Y.H.; Wang, C.Y.; Wang, Y.H.; Hsueh, S.C.; Yen, M.Y.; Ko, W.C.; Hsueh, P.R. Asymptomatic Carrier State, Acute Respiratory Disease, and Pneumonia Due to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Facts and myths. J. Microbiol. Immunol. Infect. 2020, 53, 404–412. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- da Costa, K.V.; Carnaúba, A.T.L.; Rocha, K.W.; de Andrade, K.C.L.; Ferreira, S.M.; Menezes, P.D.L. Olfactory and taste disorders in COVID-19: A systematic review. Braz. J. Otorhinolaryngol. 2020, 86, 781–792. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html (accessed on 2 August 2021).
- Kariyawasam, J.C.; Jayarajah, U.; Riza, R.; Abeysuriya, V.; Seneviratne, S.L. Gastrointestinal manifestations in COVID-19. Trans. R. Soc. Trop. Med. Hyg. 2021. [Google Scholar] [CrossRef]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Rod, J.E.; Oviedo-Trespalacios, O.; Cortes-Ramirez, J. A brief-review of the risk factors for covid-19 severity. Revista de Saúde Pública 2020, 54, 60. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Felsenstein, S.; Hedrich, C.M. COVID-19 in children and young people. Lancet Rheumatol. 2020, 2, e514–e516. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Kissler, S.M.; Fauver, J.R.; Mack, C.; Olesen, S.W.; Tai, C.; Shiue, K.Y.; Kalinich, C.C.; Jednak, S.; Ott, I.M.; Vogels, C.B.F.; et al. Viral dynamics of acute SARS-CoV-2 infection and applications to diagnostic and public health strategies. PLoS Biol. 2021, 19, e3001333. [Google Scholar] [CrossRef]
- Jorge, D.C.; Rodrigues, M.S.; Silva, M.S.; Cardim, L.L.; da Silva, N.B.; Silveira, I.H.; Silva, V.A.; Pereira, F.A.; de Azevedo, A.R.; Amad, A.A.; et al. Assessing the nationwide impact of COVID-19 mitigation policies on the transmission rate of SARS-CoV-2 in Brazil. Epidemics 2021, 35, 100465. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Heal. 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Kameda, K.; Barbeitas, M.M.; Caetano, R.; Löwy, I.; de Oliveira, A.C.D.; Corrêa, M.C.D.V.; Cassier, M. Testing COVID-19 in Brazil: Fragmented efforts and challenges to expand diagnostic capacity at the Brazilian Unified National Health System. Cad. Saúde Pública 2021, 37, e00277420. [Google Scholar] [CrossRef]
- Sacchi, C.T.; Gonçalves, M.G.; Lemos, A.P.S.; Almeida, S.C.G.; Caterino-De-Araujo, A.; Fukasawa, L.O. Comparative performances of seven quantitative Reverse-Transcription Polymerase Chain Reaction assays (RT-qPCR) for detecting SARS-CoV-2 infection in samples from individuals suspected of COVID-19 in São Paulo, Brazil. J. Clin. Virol. Plus 2021, 1, 100012. [Google Scholar] [CrossRef]
- CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 1 July 2020).
- Cunningham, M. More than Just the Kappa Coefficient: A Program to Fully Characterize Inter-Rater Reliability between Two Raters. SAS Glob. Forum 2009, 242, 1–7. [Google Scholar]
- Team, R. R: A language and environment for statistical computing, Vienna, R Foundation for Statistical Computing. 2009. Available online: http://www.R-project.org (accessed on 1 September 2021).
- Brendish, N.J.; Poole, S.; Naidu, V.V.; Mansbridge, C.T.; Norton, N.; Borca, F.; Phan, H.T.; Wheeler, H.; Harvey, M.; Presland, L.; et al. Clinical characteristics, symptoms and outcomes of 1054 adults presenting to hospital with suspected COVID-19: A comparison of patients with and without SARS-CoV-2 infection. J. Infect. 2020, 81, 937–943. [Google Scholar] [CrossRef]
- Secretaria de Estado de Saúde. Centro de Operações de Emergências - COE/MS: Recomendações Técnicas COE sobre a Utilização dos Testes Diagnósticos para COVID-19 e para Retestagem Laboratorial diante de Resultados Divergentes de COVID-19. Available online: https://www.saude.ms.gov.br/coe/notas-tecnicas-e-orientacoes (accessed on 5 May 2020).
- Secretaria de Estado de Saúde. Diretoria de Vigilância Epidemiológica de Santa Catarina: MANUAL DE ORIENTAÇÕES DA COVID-19 (vírus SARS-CoV-2). Available online: https://www.saude.sc.gov.br/coronavirus/arquivos/Manual_08.09.pdf (accessed on 5 May 2020).
- Suleyman, G.; Fadel, R.A.; Malette, K.M.; Hammond, C.; Abdulla, H.; Entz, A.; Demertzis, Z.; Hanna, Z.; Failla, A.; Dagher, C.; et al. Clinical Characteristics and Morbidity Associated with Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit. JAMA Netw. Open 2020, 3, e2012270. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef]
- Khan, M.; Khan, H.; Khan, S.; Nawaz, M. Epidemiological and clinical characteristics of coronavirus disease (COVID-19) cases at a screening clinic during the early outbreak period: A single-centre study. J. Med. Microbiol. 2020, 69, 1114–1123. [Google Scholar] [CrossRef]
- Liu, Y.; Mao, B.; Liang, S.; Yang, J.-W.; Lu, H.-W.; Chai, Y.-H.; Wang, L.; Zhang, L.; Li, Q.-H.; Zhao, L.; et al. Association between age and clinical characteristics and outcomes of COVID-19. Eur. Respir. J. 2020, 55, 2001112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Porru, S.; Carta, A.; Monaco, M.G.L.; Verlato, G.; Battaggia, A.; Parpaiola, M.; Cascio, G.L.; Pegoraro, M.; Militello, V.; Moretti, F.; et al. Health Surveillance and Response to SARS-CoV-2 Mass Testing in Health Workers of a Large Italian Hospital in Verona, Veneto. Int. J. Environ. Res. Public Heal. 2020, 17, 5104. [Google Scholar] [CrossRef] [PubMed]
- Borraz, L.A.M.; López, M.G.; Lasfuentes, P.C.; Pérez, E.G.; Domingo, C.O.; Marteles, J.L.B.; Gaspar, C.V.; de la Nieta, F.A.; Heres, A.S.; Forcada, Á.L.G.; et al. Prevalencia de infección por coronavirus SARS-CoV-2 en pacientes y profesionales de un hospital de media y larga estancia en España. Rev. Española Geriatría Gerontol. 2021, 56, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Healthcare Workers: A Living Systematic Review and Meta-analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- De Carvalho, R.S.; Augusto, G.R.; Schoen, I.P.; De Oliveira, Y.S.; Zibordi, V.M.; Elias, Y.G.B.; Gobbi, D.R. Utilização de equipamentos de proteção individual em época de COVID-19. Glob. Acad. Nurs. J. 2020, 1, 6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Hospital | Satisfactory Results | Total | Inconclusive | |
|---|---|---|---|---|
| Positive (%) | Negative (%) | |||
| Hospital de Base Luis Eduardo Magalhães (HBLEM) | 296 (30.4) | 677 (69.6) | 973 | 14 |
| Hospital Calixto Midlej Filho (HCM) | 371 (43.6) | 479 (56.4) | 850 | 6 |
| Hospital de Ilhéus (HI) | 142 (41.2) | 203 (58.8) | 345 | 1 |
| Hospital Regional Costa do Cacau (HRCC) | 476 (50.9) | 458 (49.1) | 934 | 12 |
| Symptoms | RT-qPCR for SARS-CoV-2 | Qui-Squared Test | |||
|---|---|---|---|---|---|
| Positive (%) | Negative (%) | χ2 | df | p Value | |
| Fever Yes No | 580 (54.3) 787 (28.2) | 488 (45.7) 2007 (71.8) | 230.8 | 1 | <0.001 |
| Dyspnea Yes No | 524 (47.4) 848 (30.6) | 581 (52.6) 1924 (69.4) | 98.4 | 1 | <0.001 |
| Dry cough Yes No | 772 (50.7) 600 (25.5) | 752 (49.3) 1754 (74.5) | 256.9 | 1 | <0.001 |
| Pharyngalgia Yes No | 392 (45.5) 976 (32.4) | 469 (54.5) 2032 (67.6) | 49.9 | 1 | <0.001 |
| Diarrhea Yes No | 110 (44.9) 1254 (34.7) | 135 (55.1) 2355 (65.3) | 10.89 | 1 | <0.001 |
| Headache Yes No | 279 (40.6) 1083 (34.2) | 409 (59.4) 2083 (65.8) | 9.6 | 1 | <0.001 |
| Runny nose Yes No | 256 (43.5) 1109 (33.9) | 332 (56.5) 2158 (66.1) | 19.5 | 1 | <0.001 |
| Taste loss Yes No | 78 (64.5) 1286 (34.5) | 43 (35.5) 2446 (65.5) | 46.1 | 1 | <0.001 |
| Smell loss Yes No | 83 (65.4) 1280 (34.4) | 44 (34.6) 2445 (65.6) | 46.1 | 1 | <0.001 |
| Symptoms | Age Groups | Age Groups | |||
|---|---|---|---|---|---|
| <30 | 30–49 | 50–69 | 70–89 | ||
| Fever | 30–49 | 1.000 | |||
| 50–69 | 0.014 | 0.001 | |||
| 70–89 | 0.800 | 0.745 | 0.011 | ||
| ≥90 | 0.621 | 0.614 | 1.000 | 0.695 | |
| Dyspnea | 30–49 | 0.069 | |||
| 50–69 | 0.000 | 0.000 | |||
| 70–89 | 0.000 | 0.000 | 0.004 | ||
| ≥90 | 0.008 | 0.058 | 1.000 | 0.653 | |
| Dry cough | 30–49 | 0.910 | |||
| 50–69 | 0.003 | 0.000 | |||
| 70–89 | 0.036 | 0.012 | 0.452 | ||
| ≥90 | 0.392 | 0.408 | 1.000 | 0.868 | |
| Pharyngalgia | 30–49 | 0.509 | |||
| 50–69 | 0.128 | 0.269 | |||
| 70–89 | 0.001 | 0.001 | 0.033 | ||
| ≥90 | 0.701 | 0.856 | 1.000 | 1.000 | |
| Diarrhea | 30–49 | 0.065 | |||
| 50–69 | 0.192 | 0.000 | |||
| 70–89 | 0.008 | 0.000 | 0.123 | ||
| ≥90 | 0.632 | 0.327 | 0.904 | 1.000 | |
| Headache | 30–49 | 1.000 | |||
| 50–69 | 0.000 | 0.000 | |||
| 70–89 | 0.000 | 0.000 | 0.001 | ||
| ≥90 | 0.027 | 0.024 | 0.532 | 1.000 | |
| Runny nose | 30–49 | 0.932 | |||
| 50–69 | 0.000 | 0.000 | |||
| 70–89 | 0.000 | 0.000 | 0.000 | ||
| ≥90 | 0.044 | 0.037 | 0.559 | 1.000 | |
| Taste loss | 30–49 | 0.110 | |||
| 50–69 | 0.000 | 0.010 | |||
| 70–89 | 0.000 | 0.000 | 0.120 | ||
| ≥90 | 0.405 | 0.640 | 1.000 | 1.000 | |
| Smell loss | 30–49 | 0.582 | |||
| 50–69 | 0.000 | 0.000 | |||
| 70–89 | 0.000 | 0.000 | 0.549 | ||
| ≥90 | 0.459 | 0.545 | 1.000 | 1.000 | |
| Variables | RT-qPCR for SARS-CoV-2 | Multivariate Model | Univariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| Total Individuals | Positive (%) | Negative (%) | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Gender * Female Male | 1685 1417 | 668 (39.6) 617 (43.5) | 1017 (60.4) 800 (56.5) | Reference 1.17 (1.02–1.36) | 0.028 | ||
| Age group <30 30–49 50–69 70–89 ≥90 Not informed ** | 401 1223 824 604 48 2 | 128 (31.9) 443 (36.2) 404 (49.0) 294 (48.7) 14 (29.2) | 273 (68.1) 780 (63.8) 420 (51.0) 310 (51.3) 34 (70.8) | Reference 1.22 (0.94–1.57) 1.86 (1.42–2.44) 1.64 (1.23–2.19) 0.91 (0.46–1.78) | 0.124 <0.001 <0.001 0.783 | ||
| Self-reported skin color ‡ Mixed White/Yellow/Indigen Black Not informed ** | 849 337 127 1789 | 381 (44.9) 156 (42.0) 49 (38.6) | 468 (55.1) 181 (58.0) 78 (61.4) | Reference 1.05 (0.82–1.36) 0.77 (0.53–1.13) | 0.659 0.183 | ||
| Comorbidities * NoYes | 2282 820 | 899 (39.4) 386 (47.1) | 1383 (60.6) 434 (52.9) | Reference 1.37 (1.17–1.61) | <0.001 | ||
| Healthcare professionals No Yes Not informed ** | 1886 833 383 | 802 (42.5) 281 (33.7) | 1084 (57.5) 552 (66.3) | Reference 0.81 (0.67–0.99) | <0.001 | ||
| Variables | RT-qPCR for SARS-CoV-2 | Multivariate Model | Univariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| Total Individuals | Positive (%) | Negative (%) | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Gender * Female Male | 855 1031 | 355 (41.5) 447 (43.4) | 500 (58.5) 584 (56.6) | Reference 1.08 (0.9–1.29) | 0.436 | ||
| Age group <30 30–49 50–69 70–89 ≥90 Not informed ** | 221 512 599 510 43 1 | 73 (33.0) 192 (37.5) 293 (48.9) 229 (44.9) 14 (32.6) | 148 (67.0) 320 (62.5) 306 (51.1) 281 (55.1) 29 (67.4) | Reference 1.22 (0.87–1.69) 1.94 (1.4–2.68) 1.65 (1.19–2.29) 0.98 (0.48–1.96) | 0.248 <0.001 <0.001 0.095 | ||
| Self-reported skin color ‡ Mixed White/Yellow/Indigen Black Not informed ** | 706 274 93 813 | 326 (46.2) 131 (47.8) 43 (46.2) | 380 (53.8) 143 (52.2) 50 (53.8) | Reference 1.07 (0.81–1.41) 1.00 (0.65–1.55) | 0.645 0.991 | ||
| Comorbidities * No Yes | 1265 621 | 527 (41.7) 275 (44.3) | 738 (58.3) 346 (55.7) | Reference 1.11 (0.92–1.35) | 0.279 | ||
| Variables | RT-qPCR for SARS-CoV-2 | Multivariate Model | Univariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| Total Individuals | Positive (%) | Negative (%) | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Gender Female Male | 637 196 | 224 (35.2) 57 (29.1) | 413 (64.8) 139 (70.9) | Reference 0.76 (0.53–1.07) | 0.112 | ||
| Age group * <30 30–49 50–69 70–89 ≥90 Not informed ** | 142 593 92 4 2 0 | 42 (29.6) 200 (33.7) 36 (39.1) 3 (75.0) 0 | 100 (70.4) 393 (66.3) 56 (60.9) 1 (25.0) 2 (100.0) | Reference 1.22 (0.87–1.69) 1.94 (1.4–2.68) 1.65 (1.19–2.29) 0.98 (0.48–1.96) | 0.248 <0.001 <0.001 0.095 | Reference 1.21 (0.81–1.80) 1.53 (0.88–2.66) 0.14(0.72–70.65) 0 (0-Inf) | 0.345 0.131 0.093 0.97 |
| Self-reported skin color ‡ Mixed White/Yellow/Indigen Black Not informed ** | 83 39 31 680 | 23 (27.7) 14 (35.9) 3 (9.7) | 60 (72.3) 25 (64.1) 28 (90.3) | Reference 1.46 (0.65–3.29) 0.28 (0.08–1.01) | 0.36 0.052 | ||
| Comorbidities * No Yes | 774 59 | 257 (33.2) 24 (40.7) | 517 (66.8) 35 (59.3) | Reference 1.38 (0.8–2.37) | 0.248 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, F.B.; Barbosa Costa, G.; Sevá, A.d.P.; Albuquerque, G.R.; Mariano, A.P.M.; Sampaio Lopes, A.T.; Fehlberg, H.F.; Santos de Santana, Í.T.; dos Santos, P.R.; Santos, L.C.; et al. Characteristics and Factors Associated with SARS-CoV-2 Infections in Individuals That Attended Referral Hospitals from Southern Region of Bahia State, Brazil: A Surveillance Network Retrospective Study. Viruses 2021, 13, 2462. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122462
Ferreira FB, Barbosa Costa G, Sevá AdP, Albuquerque GR, Mariano APM, Sampaio Lopes AT, Fehlberg HF, Santos de Santana ÍT, dos Santos PR, Santos LC, et al. Characteristics and Factors Associated with SARS-CoV-2 Infections in Individuals That Attended Referral Hospitals from Southern Region of Bahia State, Brazil: A Surveillance Network Retrospective Study. Viruses. 2021; 13(12):2462. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122462
Chicago/Turabian StyleFerreira, Fabrício Barbosa, Galileu Barbosa Costa, Anaiá da Paixão Sevá, George Rego Albuquerque, Ana Paula Melo Mariano, Amanda Teixeira Sampaio Lopes, Hllytchaikra Ferraz Fehlberg, Íris Terezinha Santos de Santana, Pérola Rodrigues dos Santos, Luciano Cardoso Santos, and et al. 2021. "Characteristics and Factors Associated with SARS-CoV-2 Infections in Individuals That Attended Referral Hospitals from Southern Region of Bahia State, Brazil: A Surveillance Network Retrospective Study" Viruses 13, no. 12: 2462. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122462