
Prognostic Role of the Expression of Latent-Membrane Protein 1 of Epstein–Barr Virus in Classical Hodgkin Lymphoma

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
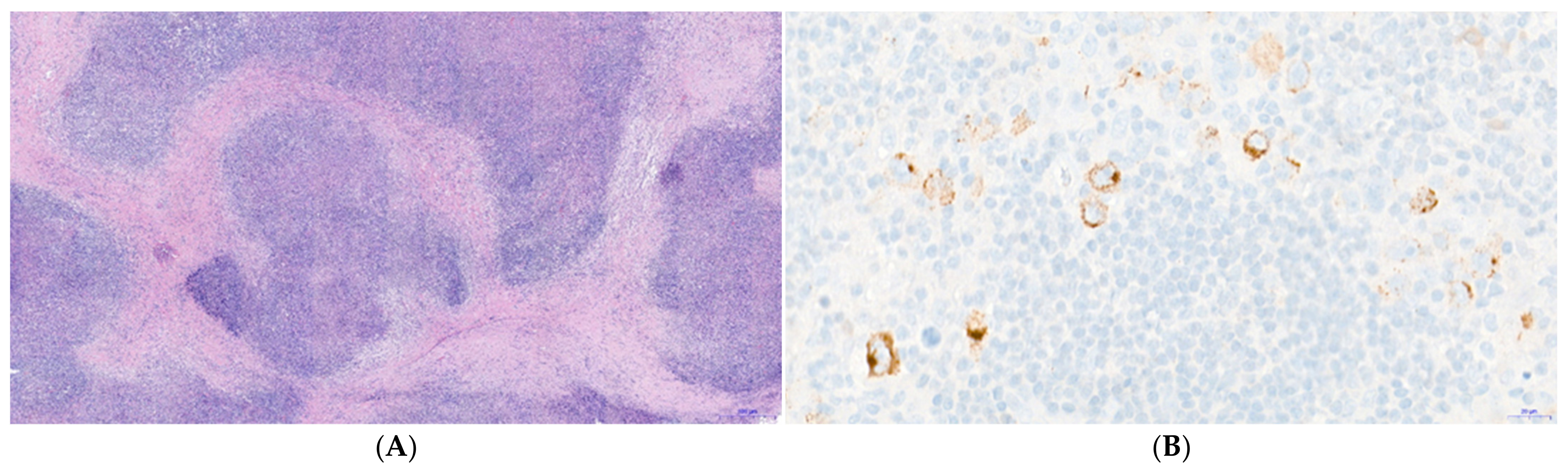
2.2. Epstein–Barr Virus Detection
2.3. Statistical Analysis
2.4. Outcome
3. Results
3.1. Patient Demographics
3.2. Survival Analysis
3.2.1. Univariate Analysis
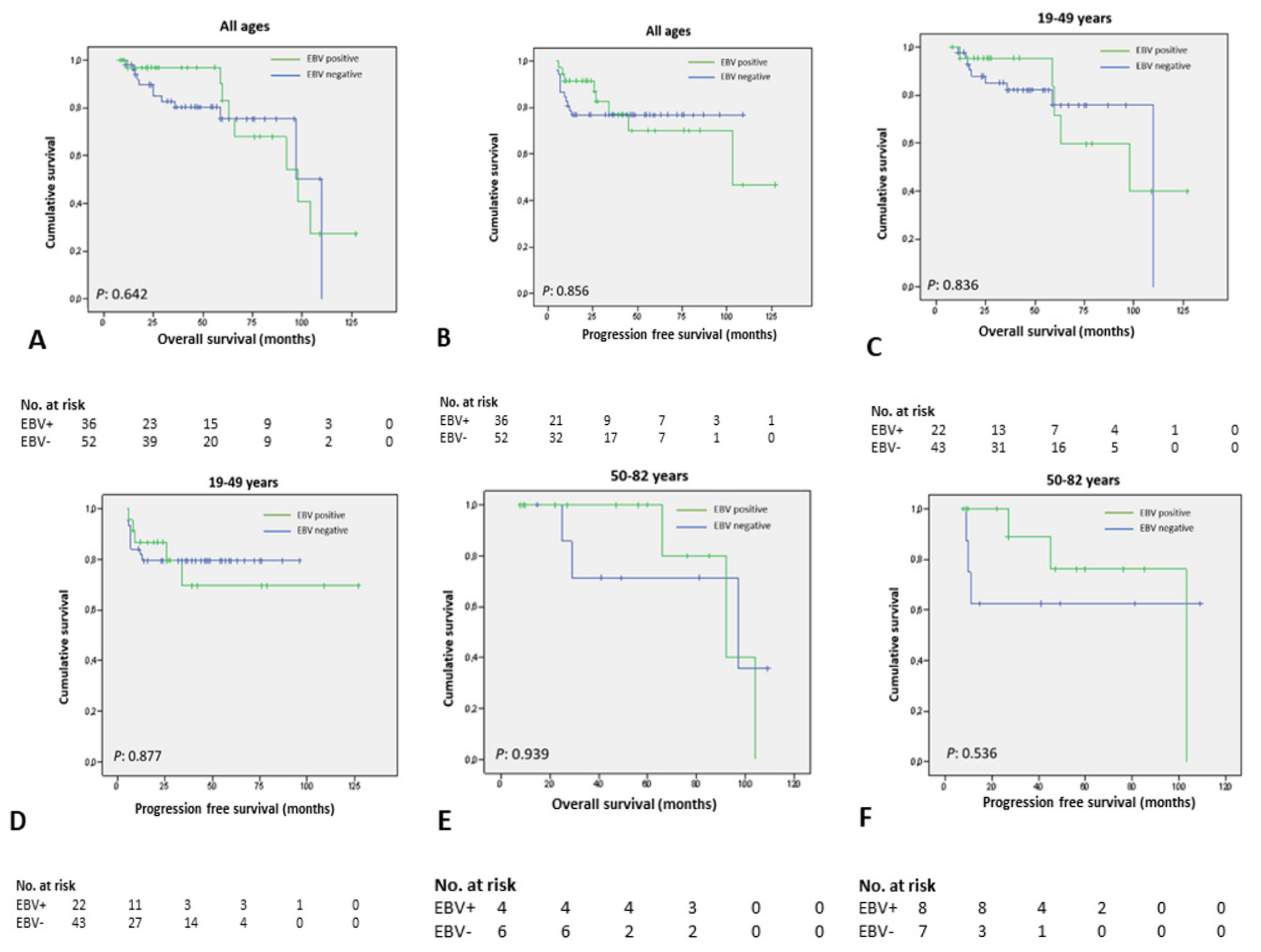
3.2.2. Analysis by Age Subgroups
3.3. Multivariate Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weniger, M.A.; Küppers, R. Molecular biology of Hodgkin lymphoma. Leukemia 2021, 35, 968–981. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, R.A.; Watkins, G. Epidemiology of Hodgkin’s disease: A review. Hematol. Oncol. 2004, 22, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Hjalgrim, H.; Smedby, K.E.; Rostgaard, K.; Molin, D.; Hamilton-Dutoit, S.; Chang, E.T.; Ralfkiaer, E.; Sundström, C.; Adami, H.O.; Glimelius, B.; et al. Infectious mononucleosis, childhood social environment, and risk of Hodgkin lymphoma. Cancer Res. 2007, 67, 2382–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poppema, S.; van Imhoff, G.; Torensma, R.; Smit, J. Lymphadenopathy morphologically consistent with Hodgkin’s disease associated with Epstein-Barr virus infection. Am. J. Clin. Pathol. 1985, 84, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Jarrett, R.F. Viruses and Hodgkin’s lymphoma. Ann. Oncol. 2002, 13 (Suppl. S1), 23–29. [Google Scholar] [CrossRef]
- Diepstra, A.; van Imhoff, G.W.; Schaapveld, M.; Karim-Kos, H.; van den Berg, A.; Vellenga, E.; Poppema, S. Latent Epstein-Barr virus infection of tumor cells in classical Hodgkin’s lymphoma predicts adverse outcome in older adult patients. J. Clin. Oncol. 2009, 27, 3815–3821. [Google Scholar] [CrossRef]
- Morente, M.M.; Piris, M.A.; Abraira, V.; Acevedo, A.; Aguilera, B.; Bellas, C.; Fraga, M.; Garcia-Del-Moral, R.; Gomez-Marcos, F.; Menarguez, J.; et al. Adverse clinical outcome in Hodgkin’s disease is associated with loss of retinoblastoma protein expression, high Ki67 proliferation index, and absence of Epstein-Barr virus-latent membrane protein 1 expression. Blood J. Am. Soc. Hematol. 1997, 90, 2429–2436. [Google Scholar]
- Montalban, C.; Abraira, V.; Morente, M.; Acevedo, A.; Aguilera, B.; Bellas, C.; Fraga, M.; Del Moral, R.G.; Menarguez, J.; Oliva, H.; et al. Epstein-Barr virus-latent membrane protein 1 expression has a favorable influence in the outcome of patients with Hodgkin’s Disease treated with chemotherapy. Leuk. Lymphoma 2000, 39, 563–572. [Google Scholar] [CrossRef]
- Krugmann, J.; Tzankov, A.; Gschwendtner, A.; Fischhofer, M.; Greil, R.; Fend, F.; Dirnhofer, S. Longer failure-free survival interval of Epstein-Barr virus-associated classical Hodgkin’s lymphoma: A single-institution study. Mod. Pathol. 2003, 16, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Herling, M.; Rassidakis, G.Z.; Medeiros, L.J.; Vassilakopoulos, T.P.; Kliche, K.O.; Nadali, G.; Viviani, S.; Bonfante, V.; Giardini, R.; Chilosi, M.; et al. Expression of Epstein-Barr virus latent membrane protein-1 in Hodgkin and Reed-Sternberg cells of classical Hodgkin’s lymphoma: Associations with presenting features, serum interleukin 10 levels, and clinical outcome. Clin. Cancer Res. 2003, 9, 2114–2120. [Google Scholar]
- Glavina-Durdov, M.; Jakic-Razumovic, J.; Capkun, V.; Murray, P. Assessment of the prognostic impact of the Epstein-Barr virus-encoded latent membrane protein-1 expression in Hodgkin’s disease. Br. J. Cancer 2001, 84, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Jarrett, R.F.; Stark, G.L.; White, J.; Angus, B.; Alexander, F.E.; Krajewski, A.S.; Freeland, J.; Taylor, G.M.; Taylor, P.R.A. Impact of tumor Epstein-Barr virus status on presenting features and outcome in age-defined subgroups of patients with classic Hodgkin lymphoma: A population-based study. Blood 2005, 106, 2444–2451. [Google Scholar] [CrossRef]
- Huppmann, A.R.; Nicolae, A.; Slack, G.W.; Pittaluga, S.; Davies-Hill, T.; Ferry, J.A.; Harris, N.L.; Jaffe, E.S.; Hasserjian, R.P. EBV may be expressed in the LP cells of nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) in both children and adults. Am. J. Surg. Pathol. 2014, 38, 316–324. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Medeiros, L.J.; Xu-Monette, Z.Y.; Zhang, S.; O’Malley, D.P.; Orazi, A.; Zuo, Z.; Bueso-Ramos, C.E.; Yin, C.C.; Liu, Z.; et al. Epstein-Barr virus-positive nodular lymphocyte predominant Hodgkin lymphoma. Ann. Diagn. Pathol. 2014, 18, 203–209. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood J. Am. Soc. Hematol. 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Hasenclever, D.; Diehl, V. A prognostic score for advanced Hodgkin’s disease. International Prognostic Factors Project on Advanced Hodgkin’s Disease. N. Engl. J. Med. 1998, 339, 1506–1514. [Google Scholar] [CrossRef]
- Engert, A.; Plütschow, A.; Eich, H.T.; Lohri, A.; Dörken, B.; Borchmann, P.; Berger, B.; Greil, R.; Willborn, K.C.; Wilhelm, M.; et al. Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma. N. Engl. J. Med. 2010, 363, 640–652. [Google Scholar] [CrossRef] [Green Version]
- Claviez, A.; Tiemann, M.; Peters, J.; Kreipe, H.; Schneppenheim, R.; Parwaresch, R. The impact of EBV, proliferation rate, and Bcl-2 expression in Hodgkin’s disease in childhood. Ann. Hematol. 1994, 68, 61–66. [Google Scholar] [CrossRef]
- Gulley, M.L.; Glaser, S.L.; Craig, F.E.; Borowitz, M.; Mann, R.B.; Shema, S.J.; Ambinder, R.F. Guidelines for interpreting EBER in situ hybridization and LMP1 immunohistochemical tests for detecting Epstein-Barr virus in Hodgkin lymphoma. Am. J. Clin. Pathol. 2002, 117, 259–267. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life tables. J. R. Stat. Soc. Ser. B 1982, 34, 187–220. [Google Scholar]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised Response Criteria for Malignant Lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Young, L.S.; Dawson, C.W. Epstein-Barr virus and nasopharyngeal carcinoma. Chin. J. Cancer 2014, 33, 581–590. [Google Scholar] [CrossRef]
- Brady, G.; MacArthur, G.J.; Farrell, P.J. Epstein-Barr virus and Burkitt lymphoma. J. Clin. Pathol. 2007, 60, 1397–1402. [Google Scholar] [CrossRef]
- Mancao, C.; Altmann, M.; Jungnickel, B.; Hammerschmidt, W. Rescue of “crippled” germinal center B cells from apoptosis by Epstein-Barr virus. Blood 2005, 106, 4339–4344. [Google Scholar] [CrossRef]
- Dirmeier, U.; Neuhierl, B.; Kilger, E.; Reisbach, G.; Sandberg, M.L.; Hammerschmidt, W. Latent membrane protein 1 is critical for efficient growth transformation of human B cells by epstein-barr virus. Cancer Res. 2003, 63, 2982–2989. [Google Scholar]
- Küppers, R. B cells under influence: Transformation of B cells by Epstein-Barr virus. Nature reviews. Immunology 2003, 3, 801–812. [Google Scholar] [CrossRef]
- Germini, D.; Sall, F.B.; Shmakova, A.; Wiels, J.; Dokudovskaya, S.; Drouet, E.; Vassetzky, Y. Oncogenic Properties of the EBV ZEBRA Protein. Cancers 2020, 12, 1479. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.; Buisson, M.; Lupo, J.; Agbalika, F.; Socié, G.; Germi, R.; Baccard, M.; Imbert-Marcille, B.-M.; Dantal, J.; Morand, P.; et al. Lytic EBV infection investigated by detection of Soluble Epstein-Barr virus ZEBRA in the serum of patients with PTLD. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hong, G.K.; Gulley, M.L.; Feng, W.-H.; Delecluse, H.-J.; Holley-Guthrie, E.; Kenney, S.C. Epstein-Barr Virus Lytic Infection Contributes to Lymphoproliferative Disease in a SCID Mouse Model. J. Virol. 2005, 79, 13993–14003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothe, R.; Liguori, L.; Villegas-Mendez, A.; Marques, B.; Grunwald, D.; Drouet, E.; Lenormand, J.-L. Characterization of the Cell-penetrating Properties of the Epstein-Barr Virus ZEBRA trans-Activator. J. Biol. Chem. 2010, 285, 20224–20233. [Google Scholar] [CrossRef] [Green Version]
- Connors, J.M.; Cozen, W.; Steidl, C.; Carbone, A.; Hoppe, R.T.; Flechtner, H.-H.; Bartlett, N.L. Hodgkin lymphoma. Nat. Rev. Dis. Prim. 2020, 6, 61. [Google Scholar] [CrossRef]
- Siegler, G.; Kremmer, E.; Gonnella, R.; Niedobitek, G. Epstein-Barr virus encoded latent membrane protein 1 (LMP1) and TNF receptor associated factors (TRAF): Colocalisation of LMP1 and TRAF1 in primary EBV infection and in EBV associated Hodgkin lymphoma. Mol. Pathol. 2003, 56, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Weniger, M.A.; Küppers, R. NF-κB deregulation in Hodgkin lymphoma. Semin. Cancer Biol. 2016, 39, 32–39. [Google Scholar] [CrossRef]
- Piris, M.A.; Medeiros, L.J.; Chang, K.-C. Hodgkin lymphoma: A review of pathological features and recent advances in pathogenesis. Pathology 2020, 52, 154–165. [Google Scholar] [CrossRef] [Green Version]
- Qi, Z.-L.; Han, X.-Q.; Hu, J.; Wang, G.-H.; Gao, J.-W.; Wang, X.; Liang, D.-Y. Comparison of three methods for the detection of Epstein-Barr virus in Hodgkin’s lymphoma in paraffin-embedded tissues. Mol. Med. Rep. 2012, 7, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, E.; Arber, D.; Harris, N.L.; Campo, E.; Quintanilla-Martinez, L.; Orazi, A. Hematopathology, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2016; ISBN 9780323296137. [Google Scholar]
- Trivedi, P.; Hu, L.F.; Chen, F.; Christensson, B.; Masucci, M.G.; Klein, G.; Winberg, G. Epstein-Barr virus (EBV)-encoded membrane protein LMP1 from a nasopharyngeal carcinoma is non-immunogenic in a murine model system, in contrast to a B cell-derived homologue. Eur. J. Cancer 1994, 30, 84–88. [Google Scholar] [CrossRef]
- Landais, E.; Saulquin, X.; Houssaint, E. The human T cell immune response to Epstein-Barr virus. Int. J. Dev. Biol. 2005, 49, 285–292. [Google Scholar] [CrossRef]
- Eichenauer, D.A.; Aleman, B.M.P.; André, M.; Federico, M.; Hutchings, M.; Illidge, T.; Engert, A.; Ladetto, M.; ESMO Guidelines Committee. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv19–iv29. [Google Scholar] [CrossRef]
- Hoppe, R.T.; Advani, R.H.; Ai, W.Z.; Ambinder, R.F.; Armand, P.; Bello, C.M.; Benitez, C.M.; Bierman, P.J.; Boughan, K.M.; Dabaja, B.; et al. Hodgkin Lymphoma, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 755–781. [Google Scholar] [CrossRef]
- Armstrong, A.A.; Lennard, A.; Alexander, F.E.; Angus, B.; Proctor, S.J.; Onions, D.E.; Jarrett, R.F. Prognostic significance of Epstein-Barr virus association in Hodgkin’s disease. Eur. J Cancer 1994, 30A, 1045–1046. [Google Scholar] [CrossRef]
- Enblad, G.; Sandvej, K.; Lennette, E.; Sundström, C.; Klein, G.; Glimelius, B.; Pallesen, G. Lack of correlation between EBV serology and presence of EBV in the Hodgkin and Reed-Sternberg cells of patients with Hodgkin’s disease. Int. J. Cancer 1997, 72, 394–397. [Google Scholar] [CrossRef]
- Amini, R.-M.; Glimelius, B.; Gustavsson, A.; Ekman, T.; Erlanson, M.; Haapaniemi, E.; Enblad, G. A population-based study of the outcome for patients with first relapse of Hodgkin’s lymphoma. Eur. J. Haematol. 2002, 68, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Herling, M.; Rassidakis, G.Z.; Vassilakopoulos, T.P.; Medeiros, L.J.; Sarris, A.H.; on behalf of the International Hodgkin Lymphoma Study Group. Impact of LMP-1 expression on clinical outcome in age-defined subgroups of patients with classical Hodgkin lymphoma. Blood 2006, 107, 1240–1241. [Google Scholar] [CrossRef]
- Middeldorp, J.M. Epstein-Barr Virus-Specific Humoral Immune Responses in Health and Disease. Curr. Top. Microbiol. Immunol. 2015, 391, 289–323. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | n = 88 (%) |
|---|---|
| Sex | |
| Male | 49 (56) |
| Female | 39 (44) |
| Age (years) | |
| Mean (range) | 39 (19–82) |
| <30 | 28 (32) |
| ≥30 | 60 (68) |
| Histological subtype | |
| NS | 55 (63) |
| MC | 16 (18) |
| LR | 8 (9) |
| NOS | 9 (10) |
| Ann Arbor stage | |
| I | 2 (2) |
| II | 36 (41) |
| III | 10 (11) |
| IV | 40 (46) |
| B symptoms at diagnosis | |
| Present | 53 (60) |
| Absent | 35 (40) |
| Bulky disease | |
| Present | 12 (14) |
| Absent | 76 (86) |
| EBV-LMP1 | |
| Positive | 36 (41) |
| Negative | 52 (59) |
| IPS | |
| 0–2 | 47 (53) |
| 3–7 | 41 (47) |
| GHSG | |
| Limited stages | 7 (8) |
| Intermediate stages | 16 (18) |
| Advanced stages | 65 (74) |
| Response to first-line therapy | |
| Complete remission | 68 (77) |
| Refractory/relapsed | 20 (23) |
| Characteristic | EBV Positive n = 36 (%) | EBV Negative n = 52 (%) | p |
|---|---|---|---|
| Sex | 0.084 | ||
| Male | 24 (67) | 25 (48) | |
| Female | 12 (23) | 27 (52) | |
| Age (years) | 0.011 | ||
| <30 | 6 (17) | 22 (42) | |
| ≥30 | 30 (83) | 30 (58) | |
| Histological subtype | <0.001 | ||
| NS | 13 (36) | 42 (81) | |
| MC | 15 (42) | 1 (2) | |
| LR | 5 (14) | 3 (5) | |
| NOS | 3 (8) | 6 (12) | |
| Ann Arbor stage | 0.089 | ||
| I | 2 (6) | 0 (0) | |
| II | 10 (28) | 26 (50) | |
| III | 5 (14) | 5 (10) | |
| IV | 19 (52) | 21 (40) | |
| B symptoms at diagnosis | 0.056 | ||
| Absent | 10 (28) | 25 (48) | |
| Present | 26 (72) | 27 (52) | |
| Bulky disease | 0.066 | ||
| Absent | 34 (95) | 42 (81) | |
| Present | 2 (5) | 10 (19) | |
| IPS | 0.023 | ||
| 0–2 | 14 (39) | 33 (63) | |
| 3–7 | 22 (61) | 19 (37) | |
| GHSG | 0.112 | ||
| Limited stages | 4 (11) | 3 (6) | |
| Intermediate stages | 3 (8) | 13 (25) | |
| Advanced stages | 29 (81) | 36 (69) | |
| Response to therapy | 0.925 | ||
| Complete remission | 28 (78) | 40 (77) | |
| Refractory/relapsed | 8 (22) | 12 (23) |
| Characteristic | N (Mean OS *) | 95% CI | p |
|---|---|---|---|
| Sex | 0.400 | ||
| Male | 49 (92) | 79–105 | |
| Female | 39 (82) | 67–97 | |
| Age (years) | 0.103 | ||
| <30 | 28 (80) | 62–98 | |
| ≥30 | 60 (96) | 83–109 | |
| Histological subtype | 0.137 | ||
| NS | 55 (80) | 67–93 | |
| MC | 16 (117) | 102–133 | |
| LR | 8 (86) | 60–111 | |
| NOS | 9 (93) | 66–121 | |
| Ann Arbor stage | 0.132 | ||
| I/II | 38 (87) | 78–96 | |
| III | 10 (86) | 60–112 | |
| IV | 40 (79) | 64–94 | |
| B symptoms at diagnosis | 0.998 | ||
| Present | 53 (89) | 77–101 | |
| Absent | 35 (87) | 72–102 | |
| Bulky disease at diagnosis | 0.009 | ||
| Present | 12 (52) | 37–67 | |
| Absent | 76 (93) | 82–104 | |
| EBV-LMP1 | 0.642 | ||
| Positive | 36 (93) | 78–108 | |
| Negative | 52 (87) | 75–99 | |
| IPS | 0.774 | ||
| 0–2 | 47 (87) | 75–99 | |
| 3–7 | 41 (88) | 73–102 | |
| GHSG | 0.282 | ||
| Limited/Intermediate stages | 23 (74) | 66–83 | |
| Advanced stages | 65 (87) | 75–99 |
| Characteristic | N (Mean PFS *) | 95% CI | p |
|---|---|---|---|
| Sex | 0.794 | ||
| Male | 49 (96) | 81–111 | |
| Female | 39 (85) | 73–98 | |
| Age (years) | 0.102 | ||
| <30 | 28 (68) | 52–83 | |
| ≥30 | 60 (99) | 85–114 | |
| Histological subtype | 0.286 | ||
| NS | 55 (80) | 68–93 | |
| MC | 16 (119) | 105–134 | |
| LR | 8 (49) | 28–70 | |
| NOS | 9 (93) | 66–120 | |
| Ann Arbor stage | 0.016 | ||
| I/II | 38 (89) | 82–97 | |
| III | 10 (73) | 35–111 | |
| IV | 40 (76) | 61–91 | |
| B symptoms at diagnosis | 0.394 | ||
| Present | 53 (91) | 75–107 | |
| Absent | 35 (91) | 72–104 | |
| Bulky disease at diagnosis | 0.055 | ||
| Present | 12 (47) | 27–66 | |
| Absent | 76 (99) | 85–112 | |
| EBV-LMP1 | 0.856 | ||
| Positive | 36 (91) | 71–111 | |
| Negative | 52 (86) | 74–97 | |
| IPS | 0.214 | ||
| 0–2 | 47 (88) | 77–99 | |
| 3–7 | 41 (89) | 72–107 | |
| GHSG | 0.086 | ||
| Limited/Intermediate stages | 23 (75) | 66–83 | |
| Advanced stages | 65 (90) | 75–104 |
| Characteristic (Reference) | OS * | PFS ** | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Sex (male) | 4.121 | 1.11–15.27 | 0.034 | 1.379 | 0.45–4.20 | 0.571 |
| Age (≥30 years) | 2.023 | 0.64–6.44 | 0.233 | 1.817 | 0.67–4.96 | 0.244 |
| Histological subtype (NS) | ||||||
| MC | 0.112 | 0.01–1.07 | 0.057 | 0.147 | 0.02–1.39 | 0.093 |
| LR | 0.866 | 0.14–5.46 | 0.878 | 1.427 | 0.27–7.64 | 0.678 |
| NOS | 0.189 | 0.03–1.22 | 0.080 | 0.292 | 0.06–1.47 | 0.134 |
| Ann Arbor stage (IV) | ||||||
| I/II | 0.074 | 0.01–0.47 | 0.006 | 0.145 | 0.04–0.57 | 0.006 |
| III | 2.077 | 0.49–8.75 | 0.319 | 1.815 | 0.49–6.71 | 0.371 |
| B symptoms (absence) | 0.695 | 0.23–2.07 | 0.514 | 0.482 | 0.16–1.42 | 0.185 |
| Bulky disease (presence) | 0.102 | 0.02–0.48 | 0.004 | 0.289 | 0.08–1.06 | 0.062 |
| EBV-LMP1 (positive) | 0.605 | 0.20–1.82 | 0.370 | 0.754 | 0.27–2.09 | 0.588 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santisteban-Espejo, A.; Perez-Requena, J.; Atienza-Cuevas, L.; Moran-Sanchez, J.; Fernandez-Valle, M.d.C.; Bernal-Florindo, I.; Romero-Garcia, R.; Garcia-Rojo, M. Prognostic Role of the Expression of Latent-Membrane Protein 1 of Epstein–Barr Virus in Classical Hodgkin Lymphoma. Viruses 2021, 13, 2523. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122523
Santisteban-Espejo A, Perez-Requena J, Atienza-Cuevas L, Moran-Sanchez J, Fernandez-Valle MdC, Bernal-Florindo I, Romero-Garcia R, Garcia-Rojo M. Prognostic Role of the Expression of Latent-Membrane Protein 1 of Epstein–Barr Virus in Classical Hodgkin Lymphoma. Viruses. 2021; 13(12):2523. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122523
Chicago/Turabian StyleSantisteban-Espejo, Antonio, Jose Perez-Requena, Lidia Atienza-Cuevas, Julia Moran-Sanchez, Maria del Carmen Fernandez-Valle, Irene Bernal-Florindo, Raquel Romero-Garcia, and Marcial Garcia-Rojo. 2021. "Prognostic Role of the Expression of Latent-Membrane Protein 1 of Epstein–Barr Virus in Classical Hodgkin Lymphoma" Viruses 13, no. 12: 2523. https://0-doi-org.brum.beds.ac.uk/10.3390/v13122523