
IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection


 , ,
, ,
Abstract
:1. Introduction
2. Case Presentation
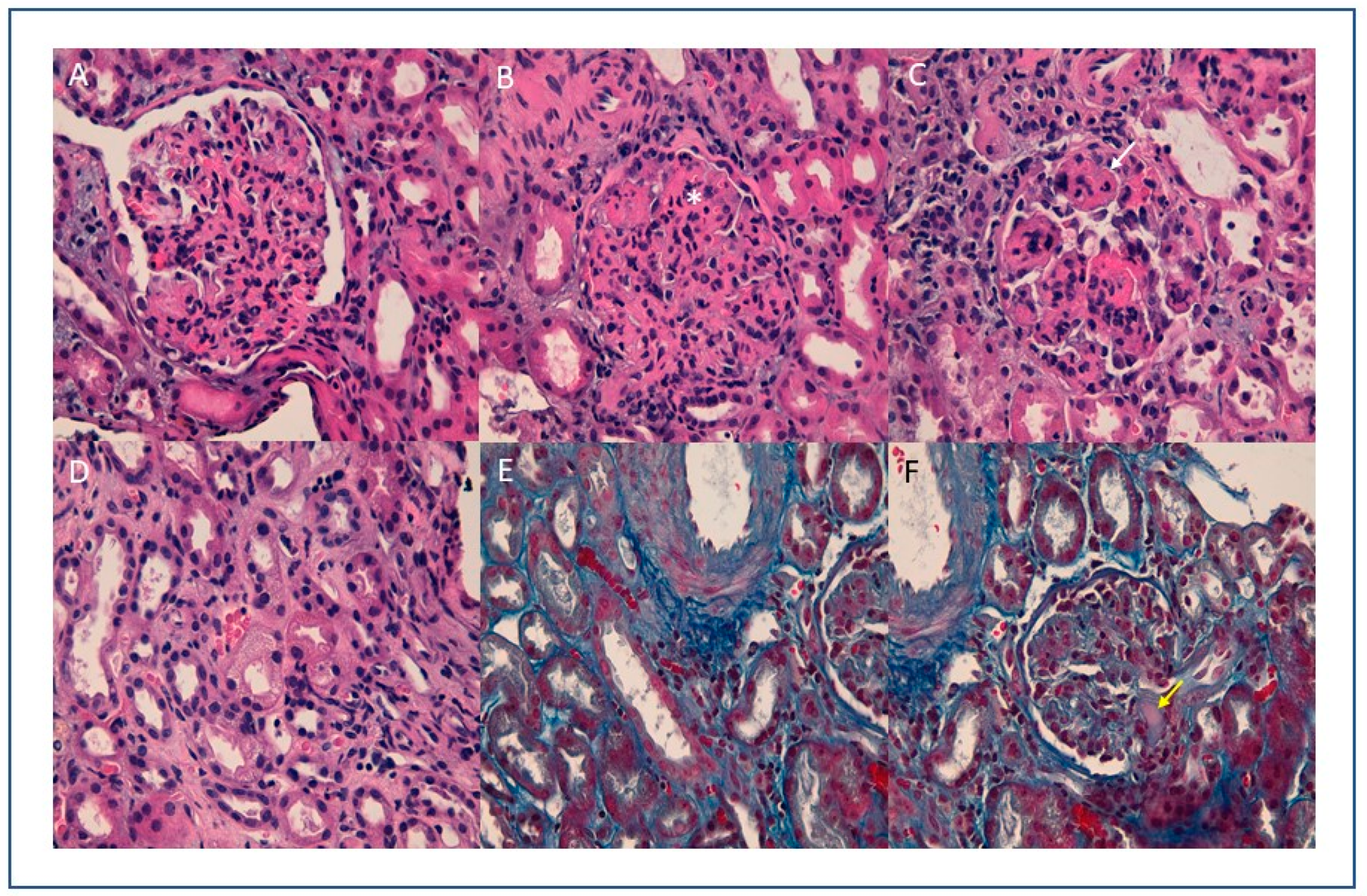
3. Kidney Biopsy Findings
4. Follow-Up
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; Abate, M.; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]
- Li, Y.; Zhou, W.; Yang, L.; You, R. Physiological and pathological regulation of ACE2, the SARS-CoV-2 receptor. Pharmacol. Res. 2020, 157, 104833. [Google Scholar] [CrossRef]
- Kissling, S.; Rotman, S.; Gerber, C.; Halfon, M.; Lamoth, F.; Comte, D.; Lhopitallier, L.; Sadallah, S.; Fakhouri, F. Collapsing glomerulopathy in a COVID-19 patient. Kidney Int. 2020, 98, 228–231. [Google Scholar] [CrossRef]
- Peleg, Y.; Kudose, S.; D’Agati, V.; Siddall, E.; Ahmad, S.; Nickolas, T.; Kisselev, S.; Gharavi, A.; Canetta, P. Acute Kidney Injury Due to Collapsing Glomerulopathy Following COVID-19 Infection. Kidney Int. Rep. 2020, 5, 940–945. [Google Scholar] [CrossRef]
- Larsen, C.P.; Bourne, T.D.; Wilson, J.D.; Saqqa, O.; Sharshir, M.A. Collapsing Glomerulopathy in a Patient With COVID-19. Kidney Int. Rep. 2020, 5, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef]
- Batlle, D.; Soler, M.J.; Sparks, M.A.; Hiremath, S.; South, A.M.; Welling, P.A.; Swaminathan, S. Acute Kidney Injury in COVID-19: Emerging Evidence of a Distinct Pathophysiology. J. Am. Soc. Nephrol. 2020, 31, 1380–1383. [Google Scholar] [CrossRef]
- D’Marco, L.; Puchades, M.J.; Romero-Parra, M.; Gimenez-Civera, E.; Soler, M.J.; Ortiz, A.; Gorriz, J.L. Coronavirus disease 2019 in chronic kidney disease. Clin. Kidney J. 2020, 13, 297–306. [Google Scholar] [CrossRef]
- Mohanty, S.K.; Satapathy, A.; Naidu, M.M.; Mukhopadhyay, S.; Sharma, S.; Barton, L.M.; Stroberg, E.; Duval, E.J.; Pradhan, D.; Tzankov, A.; et al. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19)–anatomic pathology perspective on current knowledge. Diagn. Pathol. 2020, 15, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Nasr, S.H.; Valeri, A.M.; Cornell, L.D.; Fidler, M.E.; Sethi, S.; D’Agati, V.D.; Leung, N. Renal Monoclonal Immunoglobulin Deposition Disease: A Report of 64 Patients from a Single Institution. Clin. J. Am. Soc. Nephrol. 2011, 7, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.-K.; Chen, M.-L. IgA-Dominant Postinfectious Glomerulonephritis: Not Peculiar to Staphylococcal Infection and Diabetic Patients. Ren. Fail. 2011, 33, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Bu, R.; Li, Q.; Duan, Z.-Y.; Wu, J.; Chen, P.; Chen, X.-M.; Cai, G.-Y. Clinicopathologic Features of IgA-Dominant Infection-Associated Glomerulonephritis: A Pooled Analysis of 78 Cases. Am. J. Nephrol. 2015, 41, 98–106. [Google Scholar] [CrossRef]
- Wallace, E.; Maillard, N.; Ueda, H.; Hall, S.; Fatima, H.; Novak, J.; Julian, B.A. Immune profile of IgA-dominant diffuse proliferative glomerulonephritis. Clin. Kidney J. 2014, 7, 479–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillén, A.O.O.; Silva, R.I.V.; González, B.M.; Guell, Y.A.; Fossas, P.G.; Gómez, I.G.C.; Araujo, O.M.; Abraham, V.S.; Piccoli, G.B.; Madero, M. Acute IgA-Dominant Glomerulonephritis Associated with Syphilis Infection in a Pregnant Teenager: A New Disease Association. J. Clin. Med. 2019, 8, 114. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.Y.; Kim, G.-H.; Park, H.; Park, M.H. Clinicopathologic Features of IgA-Dominant Postinfectious Glomerulonephritis. Korean J. Pathol. 2012, 46, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Rollino, C.; Vischini, G.; Coppo, R. IgA nephropathy and infections. J. Nephrol. 2016, 29, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Koyama, A.; Sharmin, S.; Sakurai, H.; Shimizu, Y.; Hirayama, K.; Usui, J.; Nagata, M.; Yoh, K.; Yamagata, K.; Muro, K.; et al. Staphylococcus aureus cell envelope antigen is a new candidate for the induction of IgA nephropathy. Kidney Int. 2004, 66, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Fraser, J.D. Clarifying the Mechanism of Superantigen Toxicity. PLoS Biol. 2011, 9, e1001145. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, G.S.; Nasr, S.H.; Stokes, M.B.; D’Agati, V.D. Treatment with IFN-α, -β, or -γ Is Associated with Collapsing Focal Segmental Glomerulosclerosis. Clin. J. Am. Soc. Nephrol. 2010, 5, 607–615. [Google Scholar] [CrossRef] [Green Version]
- Gianassi, I.; Allinovi, M.; Caroti, L.; Cirami, L.C.; Iacopo, G. Broad spectrum of interferon-related nephropathies-glomerulonephritis, systemic lupus erythematosus-like syndrome and thrombotic microangiopathy: A case report and review of literature. World J. Nephrol. 2019, 8, 109–117. [Google Scholar] [CrossRef]
- Li, Y.; Luo, C.; Li, W.; Xu, Z.; Zeng, C.; Bi, S.; Yu, J.; Wu, J.; Yang, H. Structure-Based Preliminary Analysis of Immunity and Virulence of SARS Coronavirus. Viral Immunol. 2004, 17, 528–534. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Ng, J.J.; Luo, Y.; Phua, K.; Choong, A.M. Acute kidney injury in hospitalized patients with coronavirus disease 2019 (COVID-19): A meta-analysis. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, P.; Uppal, N.N.; Wanchoo, R.; Shah, H.H.; Yang, Y.; Parikh, R.; Khanin, Y.; Madireddy, V.; Larsen, C.P.; Jhaveri, K.D.; et al. COVID-19–Associated Kidney Injury: A Case Series of Kidney Biopsy Findings. J. Am. Soc. Nephrol. 2020, 31, 1948–1958. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Diao, B.; Lv, X.; Liang, W.; Zhu, J.; Liu, L.; Zhang, S.; Shen, B.; Wang, H. 2019 novel coronavirus disease in hemodialysis (HD) patients: Report from one HD center in Wu-han China. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural Evidence for Direct Renal Infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020, 31, 1683–1687. [Google Scholar] [CrossRef] [PubMed]
- Nasr, S.H.; Kopp, J.B. COVID-19–Associated Collapsing Glomerulopathy: An Emerging Entity. Kidney Int. Rep. 2020, 5, 759–761. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Roufosse, C.; Curtis, E.; Moran, L.; Hollinshead, M.; Cook, T.; Hanley, B.; Horsfield, C.; Neil, D. Electron microscopic investigations in COVID-19: Not all crowns are coronas. Kidney Int. 2020, 98, 505–506. [Google Scholar] [CrossRef]
- Miller, S.E.; Goldsmith, C.S. Caution in Identifying Coronaviruses by Electron Microscopy. J. Am. Soc. Nephrol. 2020, 31, 2223–2224. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- D’Marco, L.; Puchades, M.J.; Romero-Parra, M.; Gorriz, J.L. Diabetic Kidney Disease and COVID-19: The Crash of Two Pandemics. Front. Med. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Murakami, M. COVID-19: A New Virus, but a Familiar Receptor and Cytokine Release Syndrome. Immunity 2020, 52, 731–733. [Google Scholar] [CrossRef]
- Cheng, M.H.; Zhang, S.; Porritt, R.A.; Arditi, M.; Bahar, I. An insertion unique to SARS-CoV-2 exhibits superantigenic character strengthened by recent mutations. BioRxiv 2020. [Google Scholar] [CrossRef]
- Rops, A.L.; Jansen, E.; Van Der Schaaf, A.; Pieterse, E.; Rother, N.; Hofstra, J.; Dijkman, H.B.; Van De Logt, A.-E.; Wetzels, J.; Van Der Vlag, J.; et al. Interleukin-6 is essential for glomerular immunoglobulin A deposition and the development of renal pathology in Cd37-deficient mice. Kidney Int. 2018, 93, 1356–1366. [Google Scholar] [CrossRef]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. J. Clin. Med. 2020, 9, 1417. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.-Q.; Sun, B.-Q.; Fang, Z.-F.; Zhao, J.-C.; Liu, X.-Y.; Li, Y.-M.; Sun, X.-Z.; Liang, H.-F.; Zhong, B.; Huang, Z.-F.; et al. Distinct features of SARS-CoV-2-specific IgA response in COVID-19 patients. Eur. Respir. J. 2020, 56, 2001526. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline (before Hospitalization) | Hospitalization COVID-19 | Discharge COVID-19 | Hospitalization IgA-CGMN | Hospitalization IgA-CGMN (+6 days) | Discharge IgA-CGMN (+11) | Range | |
|---|---|---|---|---|---|---|---|
| Creatinine (mg/dL) | 1.01 | 1.35 | 0.83 | 2.14 | 3.19 | 2.35 | 0.65–1.35 |
| eGFR (ml/min) | 66.2 | 46.6 | 26.6 | 23.8 | |||
| Urea (mg/dL) | 147 | 36 | 148 | 133 | 117 | 20–50 | |
| Na (mmol/L) | 143 | 136 | 141 | 145 | 139 | 136 | 135–145 |
| K+ (mmol/L) | 4.6 | 3.6 | 4.1 | 4.4 | 4.4 | 4.2 | 3.5–5.1 |
| Uric Acid (mg/dL) | 7.6 | 4.4 | 7.1 | 3.5–7.2 | |||
| Calcium (mg/dL) | 9.9 | 8.6 | 8.2 | 8.1–10.5 | |||
| Phosphate (mg/dL) | 5.3 | 3.5 | 2.5–5.0 | ||||
| Magnesium (mg/dL) | 2.6 | 2.4 | 1.9 | 1.7–2.6 | |||
| Ferritin (ng/mL) | 1681 | 664 | 316 | 20–300 | |||
| Albumin (g/dL) | 4.2 | 3 | 2.8 | 3.5–5.2 | |||
| AST (U/L) | 17 | 52 | 24 | 22 | 24 | 17 | 1.0–37 |
| ALT (U/L) | 20 | 25 | 24 | 11 | 25 | 22 | 1.0–41 |
| Bilirubin (mg/dL) | 1.04 | 0.93 | 0.77 | 0.47 | 0.1–1 | ||
| LDH (U/L) | 863 | 492 | 607 | 569 | 395 | 240–480 | |
| Procalcitonin (ng/mL) | 0.67 | 0.14 | 0.1 | 0.13 | 0.0–0.5 | ||
| CRP (mg/L) | 220.8 | 14.7 | 16.4 | 14 | 1.1 | 0–5 | |
| ASLO (UI/mL) | 34 | <200 | |||||
| WC (109/L) | 4.36 | 9.16 | 2.96 | 5.65 | 4.16 | 7.01 | 4.1–11 |
| Lymphocytes | 1.03 | 0.22 | 0.75 | 1.23 | 0.61 | 1.41 | 1.5–4.5 |
| Hemoglobin (g/dL) | 13.1 | 9.9 | 9.9 | 9.8 | 9.2 | 8.9 | 12.0–16.0 |
| Platelet (x 109) | 121 | 130 | 96 | 105 | 108 | 158 | 140–400 |
| IQ (%) | 91 | 97 | 97 | 100 | 92 | 75–110 | |
| D Dimer | 824 | 245 | 904 | 4485 | 458 | <250 | |
| Immunofixation | Oligoclonal band IgG kappa, IgM-kappa and lambda light chain | Oligoclonal bands IgG kappa, IgM-kappa and lambda light chain | |||||
| C3 (mg/dL) | 97 | 83 | 90–180 | ||||
| C4 (mg/dL) | 9 | 7 | 10–40 | ||||
| Rheumatoid Factor (UI/mL) | 179 | 170 | 0–14 | ||||
| URINE | |||||||
| Nitrites | Neg | Neg | Neg | Neg | Neg | ||
| Urobilinogen (mg/dL) | 2 | 0.2 | 0.2 | <2.0 mg/dL | |||
| Protein lab stick (mg/dL) | Neg | 70 | >600 | 300 | <20 mg/dL | ||
| RPC | 8.38 | 5.79 | 5.17 | <0.20 | |||
| pH | 5.5 | 5.5 | 6 | 7 | 5.0–8.0 | ||
| Density | 1.015 | 1.03 | 1.03 | 1.005 | 1.005 | ||
| Ketonic bodies | Neg | Neg | Neg | Neg | Neg | ||
| Biliary | Neg | Neg | Neg | Neg | Neg | ||
| Glucose (mg/dL) | Neg | Neg | Neg | 70 mg/dL | <30 mg/dL | ||
| RBC | Neg | 0–1 | >100 | >100 | Neg | ||
| Acanthocytes | 20–40% | Neg | |||||
| WC | Neg | 1–5 | 10–20 | 1–5 | Neg | ||
| Cast | Neg | Neg | Granular | Neg | Neg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez, A.; Torregrosa, I.; D’Marco, L.; Juan, I.; Terradez, L.; Solís, M.Á.; Moncho, F.; Carda-Batalla, C.; Forner, M.J.; Gorriz, J.L. IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection. Viruses 2021, 13, 587. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040587
Pérez A, Torregrosa I, D’Marco L, Juan I, Terradez L, Solís MÁ, Moncho F, Carda-Batalla C, Forner MJ, Gorriz JL. IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection. Viruses. 2021; 13(4):587. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040587
Chicago/Turabian StylePérez, Aurora, Isidro Torregrosa, Luis D’Marco, Isabel Juan, Liria Terradez, Miguel Ángel Solís, Francesc Moncho, Carmen Carda-Batalla, María J. Forner, and Jose Luis Gorriz. 2021. "IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection" Viruses 13, no. 4: 587. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040587