
Persistence of Anti-ZIKV-IgG over Time Is Not a Useful Congenital Infection Marker in Infants Born to ZIKV-Infected Mothers: The NATZIG Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Laboratory Testing
2.4. Data Analysis
3. Results
3.1. ZIKV-RNA and Anti-ZIKV-IgM Antibodies
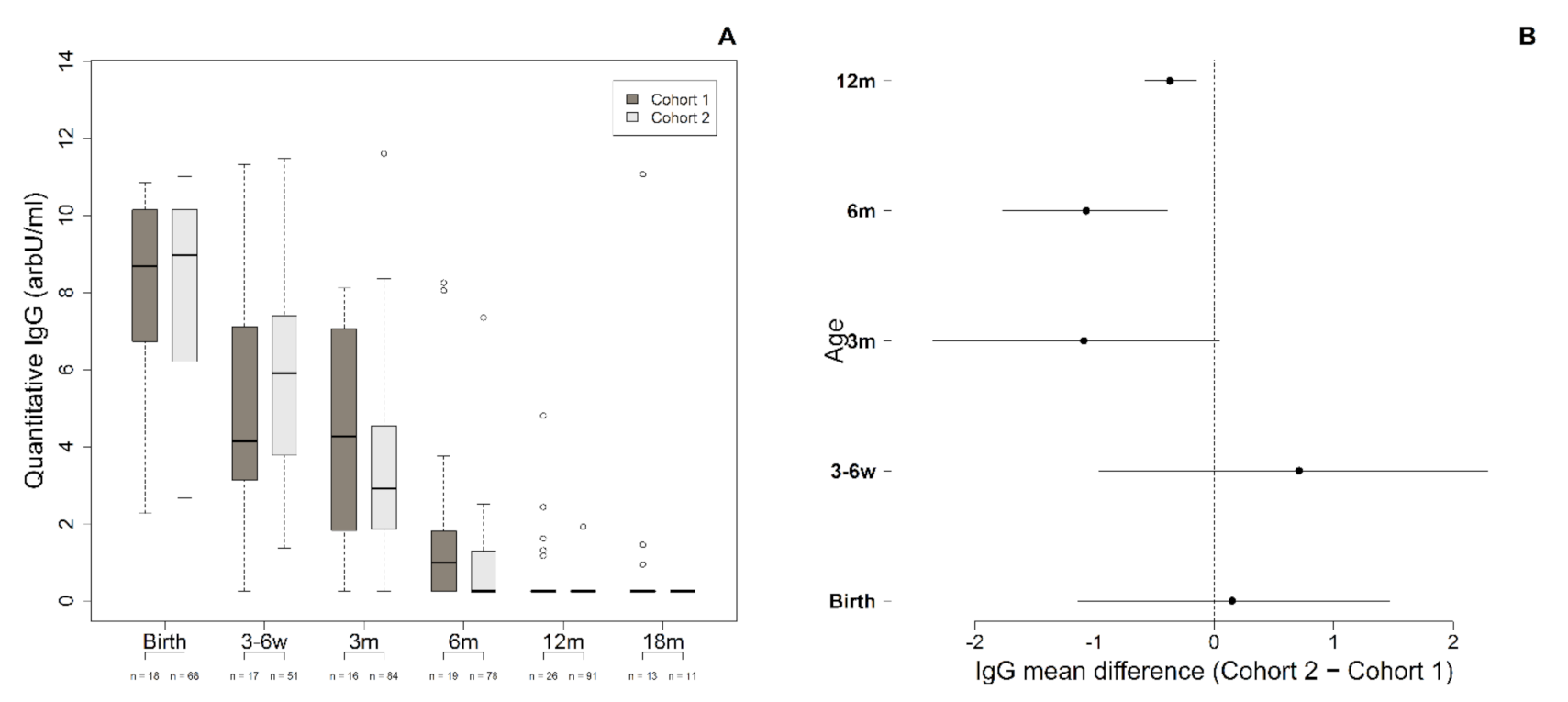
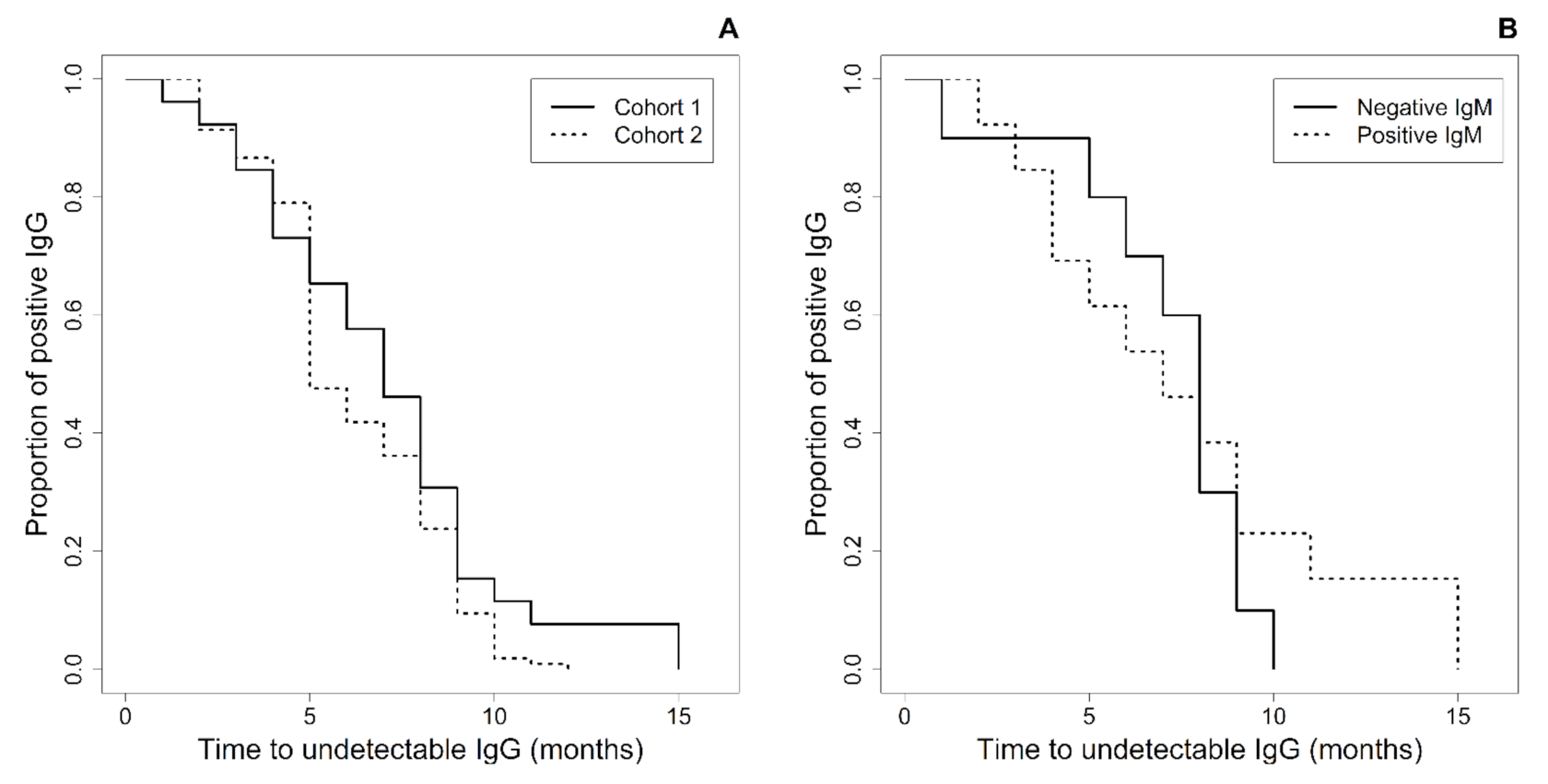
3.2. Anti-ZIKV-IgG Antibodies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; Da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the pattern of anomalies in congenital zika syndrome for pediatric clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, C.M.; de Negrini, S.F.B.M.; Araujo, D.C.A.; Teixeira, S.R.; Amaral, F.R.; Moro, M.C.R.; Fernandes, J.D.C.P.; da Motta, M.S.F.; de Negrini, B.V.M.; Caldas, C.A.C.T.; et al. Early maternal Zika infection predicts severe neonatal neurological damage: Results from the prospective Natural History of ZIKA Virus Infection in Gestation cohort study. BJOG Int. J. Obstet. Gynaecol. 2020, 128, 317–326. [Google Scholar] [CrossRef]
- de Oliveira Melo, A.S.; Aguiar, R.S.; Amorim, M.M.R.; Arruda, M.B.; De Oliveira Melo, F.; Ribeiro, S.T.C.; Batista, A.G.M.; Ferreira, T.; Dos Santos, M.P.; Sampaio, V.V.; et al. Congenital Zika virus infection: Beyond neonatal microcephaly. JAMA Neurol. 2016, 73, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Pomar, L.; Vouga, M.; Lambert, V.; Pomar, C.; Hcini, N.; Jolivet, A.; Benoist, G.; Rousset, D.; Matheus, S.; Malinger, G.; et al. Maternal-fetal transmission and adverse perinatal outcomes in pregnant women infected with Zika virus: Prospective cohort study in French Guiana. BMJ 2018, 363, k4431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musso, D.; Ko, A.I.; Baud, D. Zika virus infection—After the pandemic. N. Engl. J. Med. 2019, 381, 1444–1457. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.J.; Revell, P.A. Update in Pediatric Diagnostic Microbiology. Clin. Lab. Med. 2020, 40, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Honein, M.A.; Dawson, A.L.; Petersen, E.E.; Jones, A.M.; Lee, E.H.; Yazdy, M.M.; Ahmad, N.; Macdonald, J.; Evert, N.; Bingham, A.; et al. Birth defects among fetuses and infants of US women with evidence of possible zika virus infection during pregnancy. JAMA J. Am. Med. Assoc. 2017, 317, 59–68. [Google Scholar] [CrossRef]
- Carvalho, A.L.; Brandi, I.V.; Sarmento, M.; Brites, C.; Lucena, R. Difficulties with laboratory confirmation of congenital Zika virus infection in a tertiary hospital in Northeastern Brazil. Clin. Microbiol. Infect. 2019, 25, 524–525. [Google Scholar] [CrossRef] [Green Version]
- Schaub, B.; Vouga, M.; Najioullah, F.; Gueneret, M.; Monthieux, A.; Harte, C.; Muller, F.; Jolivet, E.; Adenet, C.; Dreux, S.; et al. Analysis of blood from Zika virus-infected fetuses: A prospective case series. Lancet Infect. Dis. 2017, 17, 520–527. [Google Scholar] [CrossRef] [Green Version]
- Maldonado, Y.A.; Read, J.S.; Byington, C.L.; Barnett, E.D.; Davies, H.D.; Edwards, K.M.; Lynfield, R.; Munoz, F.M.; Nolt, D.; Nyquist, A.C.; et al. Diagnosis, treatment, and prevention of congenital toxoplasmosis in the United States. Pediatrics 2017, 139, e20163860. [Google Scholar] [CrossRef] [Green Version]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- Soares de Oliveira-Szejnfeld, P.; Levine, D.; de Melo, A.S.O.; Amorim, M.M.R.; Batista, A.G.M.; Chimelli, L.; Tanuri, A.; Aguiar, R.S.; Malinger, G.; Ximenes, R.; et al. Congenital Brain Abnormalities and Zika Virus: What the Radiologist Can Expect to See Prenatally and Postnatally. Radiology 2016, 281, 203–218. [Google Scholar] [CrossRef] [PubMed]
- De Fatima Vasco Aragao, M.; van der Linden, V.; Brainer-Lima, A.M.; Coeli, R.R.; Rocha, M.A.; Sobral da Silva, P.; Durce Costa Gomes de Carvalho, M.; van der Linden, A.; Cesario de Holanda, A.; Valenca, M.M. Clinical features and neuroimaging (CT and MRI) findings in presumed Zika virus related congenital infection and microcephaly: Retrospective case series study. BMJ 2016, 353, i1901. [Google Scholar] [CrossRef] [Green Version]
- InBios International, Inc. ZIKV Detect 2.0 IgM Capture ELISA Instructions for Use; InBios International, Inc.: Seattle, WA, USA, 2018; pp. 1–18. [Google Scholar]
- Matheus, S.; Talla, C.; Labeau, B.; De Laval, F.; Briolant, S.; Berthelot, L.; Vray, M.; Rousset, D. Performance of 2 commercial serologic tests for diagnosing zika virus infection. Emerg. Infect. Dis. 2019, 25, 1153–1160. [Google Scholar] [CrossRef]
- Balmaseda, A.; Stettler, K.; Medialdea-Carrera, R.; Collado, D.; Jin, X.; Zambrana, J.V.; Jaconi, S.; Cameroni, E.; Saborio, S.; Rovida, F.; et al. Antibody-based assay discriminates Zika virus infection from other flaviviruses. Proc. Natl. Acad. Sci. USA 2017, 114, 8384–8389. [Google Scholar] [CrossRef] [Green Version]
- Conners, E.E.; Lee, E.H.; Thompson, C.N.; McGibbon, E.; Rakeman, J.L.; Iwamoto, M.; Cooper, H.; Vora, N.M.; Limberger, R.J.; Fine, A.D.; et al. Zika virus infection among pregnant women and their neonates in New York City, January 2016–June 2017. Obstet. Gynecol. 2018, 132, 487–495. [Google Scholar] [CrossRef]
- Cordeiro, M.T.; Brito, C.A.A.; Pena, L.J.; Castanha, P.M.S.; Gil, L.H.V.G.; Lopes, K.G.S.; Dhalia, R.; Meneses, J.A.; Ishigami, A.C.; Mello, L.M.; et al. Results of a Zika Virus (ZIKV) Immunoglobulin M-Specific Diagnostic Assay Are Highly Correlated with Detection of Neutralizing Anti-ZIKV Antibodies in Neonates with Congenital Disease. J. Infect. Dis. 2016, 214, 1897–1904. [Google Scholar] [CrossRef] [PubMed]
- Brasil, P.; Vasconcelos, Z.; Kerin, T.; Gabaglia, C.R.; Ribeiro, I.P.; Bonaldo, M.C.; Damasceno, L.; Pone, M.V.; Pone, S.; Zin, A.; et al. Zika virus vertical transmission in children with confirmed antenatal exposure. Nat. Commun. 2020, 11, 3510. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.O.; Gorchakov, R.; Carlson, A.R.; Berry, R.; Lai, L.; Natrajan, M.; Garcia, M.N.; Correa, A.; Patel, S.M.; Aagaard, K.; et al. Prolonged detection of zika virus in vaginal secretions and whole blood. Emerg. Infect. Dis. 2017, 23, 99–101. [Google Scholar] [CrossRef]
- Paz-Bailey, G.; Rosenberg, E.S.; Doyle, K.; Munoz-Jordan, J.; Santiago, G.A.; Klein, L.; Perez-Padilla, J.; Medina, F.A.; Waterman, S.H.; Adams, L.E.; et al. Persistence of Zika Virus in Body Fluids—Final Report. N. Engl. J. Med. 2017, 379, 1234–1243. [Google Scholar] [CrossRef]
- Adebanjo, T.; Godfred-Cato, S.; Viens, L.; Fischer, M.; Staples, J.E.; Kuhnert-Tallman, W.; Walke, H.; Oduyebo, T.; Polen, K.; Peacock, G.; et al. Update: Interim guidance for the diagnosis, evaluation, and management of infants with possible congenital zika virus infection—United States, October 2017. Morb. Mortal. Wkly. Rep. 2017, 66, 1089–1099. [Google Scholar] [CrossRef]
- Charrel, R.; Mögling, R.; Pas, S.; Papa, A.; Baronti, C.; Koopmans, M.; Zeller, H.; Leparc-Goffart, I.; Reusken, C.B. Variable sensitivity in molecular detection of zika virus in european expert laboratories: External quality assessment, November 2016. J. Clin. Microbiol. 2017, 55, 3219–3226. [Google Scholar] [CrossRef] [Green Version]
- Collins, M.H.; Waggoner, J.J. Detecting Vertical Zika Transmission: Emerging Diagnostic Approaches for an Emerged Flavivirus. ACS Infect. Dis. 2019, 5, 1055–1069. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, C.; Joguet, G.; Mengelle, C.; Chapuy-Regaud, S.; Pavili, L.; Prisant, N.; Izopet, J.; Bujan, L.; Mansuy, J.M. Kinetics of anti-ZIKV antibodies after Zika infection using two commercial enzyme-linked immunoassays. Diagn. Microbiol. Infect. Dis. 2018, 90, 26–30. [Google Scholar] [CrossRef]
- Singh, T.; Lopez, C.A.; Giuberti, C.; Dennis, M.L.; Itell, H.L.; Heimsath, H.J.; Webster, H.S.; Roark, H.K.; De Vargas, P.R.M.; Hall, A.; et al. Efficient transplacental IgG transfer in women infected with Zika virus during pregnancy. PLoS Negl. Trop. Dis. 2019, 13, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Castanha, P.M.S.; Souza, W.V.; Braga, C.; de Araújo, T.V.; Ximenes, R.A.; Maria de Fátima, M.; Albuquerque, P.M.; Montarroyos, U.R.; Miranda-Filho, D.B.; Cordeiro, M.T.; et al. Perinatal analyses of Zika- and dengue virus-specific neutralizing antibodies: A microcephaly case-control study in an area of high dengue endemicity in Brazil. PLoS Negl. Trop. Dis. 2019, 13, e0007246. [Google Scholar] [CrossRef] [Green Version]
- Rosenstierne, M.W.; Schaltz-Buchholzer, F.; Bruzadelli, F.; Có, A.; Cardoso, P.; Jørgensen, C.S.; Michiels, J.; Heyndrickx, L.; Ariën, K.K.; Fischer, T.K.; et al. Zika virus IgG in infants with microcephaly, Guinea-Bissau, 2016. Emerg. Infect. Dis. 2018, 24, 948–950. [Google Scholar] [CrossRef] [Green Version]
- Voordouw, B.; Rockx, B.; Jaenisch, T.; Fraaij, P.; Mayaud, P.; Vossen, A. Performance of Zika Assays in the Context of Toxoplasma gondii, Parvovirus B19, Rubella Virus, and Cytomegalovirus (TORCH) Diagnostic Assays. Clin. Microbiol. Rev. 2020, 33, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Watanaveeradej, V.; Endy, T.P.; Samakoses, R.; Kerdpanich, A.; Simasathien, S.; Polprasert, N.; Aree, C.; Vaughn, D.W.; Ho, C.; Nisalak, A. Transplacentally transferred maternal-infant antibodies to dengue virus. Am. J. Trop. Med. Hyg. 2003, 69, 123–128. [Google Scholar] [CrossRef]
- Chau, T.N.B.; Hieu, N.T.; Anders, K.L.; Wolbers, M.; Lien, L.B.; Hieu, L.T.M.; Hien, T.T.; Hung, N.T.; Farrar, J.; Whitehead, S.; et al. Dengue virus infections and maternal antibody decay in a prospective birth cohort study of vietnamese infants. J. Infect. Dis. 2009, 200, 1893–1900. [Google Scholar] [CrossRef] [Green Version]
- Heffron, A.S.; Mohr, E.L.; Baker, D.; Haj, A.K.; Buechler, C.R.; Bailey, A.; Dudley, D.M.; Newman, C.M.; Mohns, M.S.; Koenig, M.; et al. Antibody responses to Zika virus proteins in pregnant and non-pregnant macaques. PLoS Negl. Trop. Dis. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maness, N.J.; Schouest, B.; Singapuri, A.; Dennis, M.; Gilbert, M.H.; Bohm, R.P.; Schiro, F.; Aye, P.P.; Baker, K.; Van Rompay, K.K.A.; et al. Postnatal Zika virus infection of nonhuman primate infants born to mothers infected with homologous Brazilian Zika virus. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Moraes-Pinto, M.I.; Suano-Souza, F.; Aranda, C.S. Immune system: Development and acquisition of immunological competence. J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Zika Epidemiology Update—July 2019. Available online: https://www.who.int/docs/default-source/documents/emergencies/zika/zika-epidemiology-update-july-2019.pdf?sfvrsn=14a1b3a7_22019 (accessed on 15 January 2021).



{kind=link}
{kind=link}
| Characteristics | Cohort One (CZS) (n = 30) | Cohort Two (Asymptomatic) (n = 123) |
|---|---|---|
| Trimester of maternal ZIKV infection | ||
| 1st | 20 (66.7%) | 27 (21.9%) |
| 2nd | 1 (3.3%) | 72 (58.5%) |
| 3rd | 0 | 23 (18.7%) |
| No rash | 8 (26.7%) | 0 |
| Missing | 1 (3.3%) | 1 (0.9%) |
| Gestational age | ||
| Term | 24 (80.0%) | 110 (89.4%) |
| Preterm | 5 (16.7%) | 11 (8.7%) |
| Missing | 1 (3.3%) | 2 (0.8%) |
| Birth weight (g) | 2694 (623) | 3101 (661) |
| Head Circumference (cm) | 28.3 (5.6) | 33.4 (4.2) |
| Test | Cohort One (CZS) (n = 30) | Cohort Two (Asymptomatic) (n = 123) |
|---|---|---|
| ZIKV-RNA at birth (blood and/or urine) | ||
| Positive | 0 | 0 |
| Negative | 17 (56.7%) | 45 (36.6%) |
| Indeterminate | 0 | 1 (0.8%) |
| Missing | 13 (43.3%) | 77 (62.6%) |
| Anti-ZIKV-IgM within 6 months | ||
| Positive | 15 (50.0%) | 2 (1.6%) |
| Negative | 10 (33.3%) | 113 (91.9%) |
| Missing | 5 (16.7%) | 8 (6.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coutinho, C.M.; Fernandes, J.D.C.P.; Yamamoto, A.Y.; Negrini, S.F.B.d.M.; Negrini, B.V.d.M.; Teixeira, S.R.; Amaral, F.R.; Motta, M.S.F.d.; Bárbaro, A.A.T.; Aragon, D.C.; et al. Persistence of Anti-ZIKV-IgG over Time Is Not a Useful Congenital Infection Marker in Infants Born to ZIKV-Infected Mothers: The NATZIG Cohort. Viruses 2021, 13, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040711
Coutinho CM, Fernandes JDCP, Yamamoto AY, Negrini SFBdM, Negrini BVdM, Teixeira SR, Amaral FR, Motta MSFd, Bárbaro AAT, Aragon DC, et al. Persistence of Anti-ZIKV-IgG over Time Is Not a Useful Congenital Infection Marker in Infants Born to ZIKV-Infected Mothers: The NATZIG Cohort. Viruses. 2021; 13(4):711. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040711
Chicago/Turabian StyleCoutinho, Conrado Milani, Juliana Dias Crivelenti Pereira Fernandes, Aparecida Yulie Yamamoto, Silvia Fabiana Biason de Moura Negrini, Bento Vidal de Moura Negrini, Sara Reis Teixeira, Fabiana Rezende Amaral, Márcia Soares Freitas da Motta, Adriana Aparecida Tiraboschi Bárbaro, Davi Casale Aragon, and et al. 2021. "Persistence of Anti-ZIKV-IgG over Time Is Not a Useful Congenital Infection Marker in Infants Born to ZIKV-Infected Mothers: The NATZIG Cohort" Viruses 13, no. 4: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040711