
Uptake of Human Papillomavirus Vaccine and Intention to Vaccinate among Healthy Pregnant Women in Serbia: A Cross-Sectional Study on Awareness, Knowledge, and Attitudes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Instrument
2.2. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Gynecological Data
3.2. HPV and HPV Vaccine Awareness
3.3. HPV and HPV Vaccine Knowledge
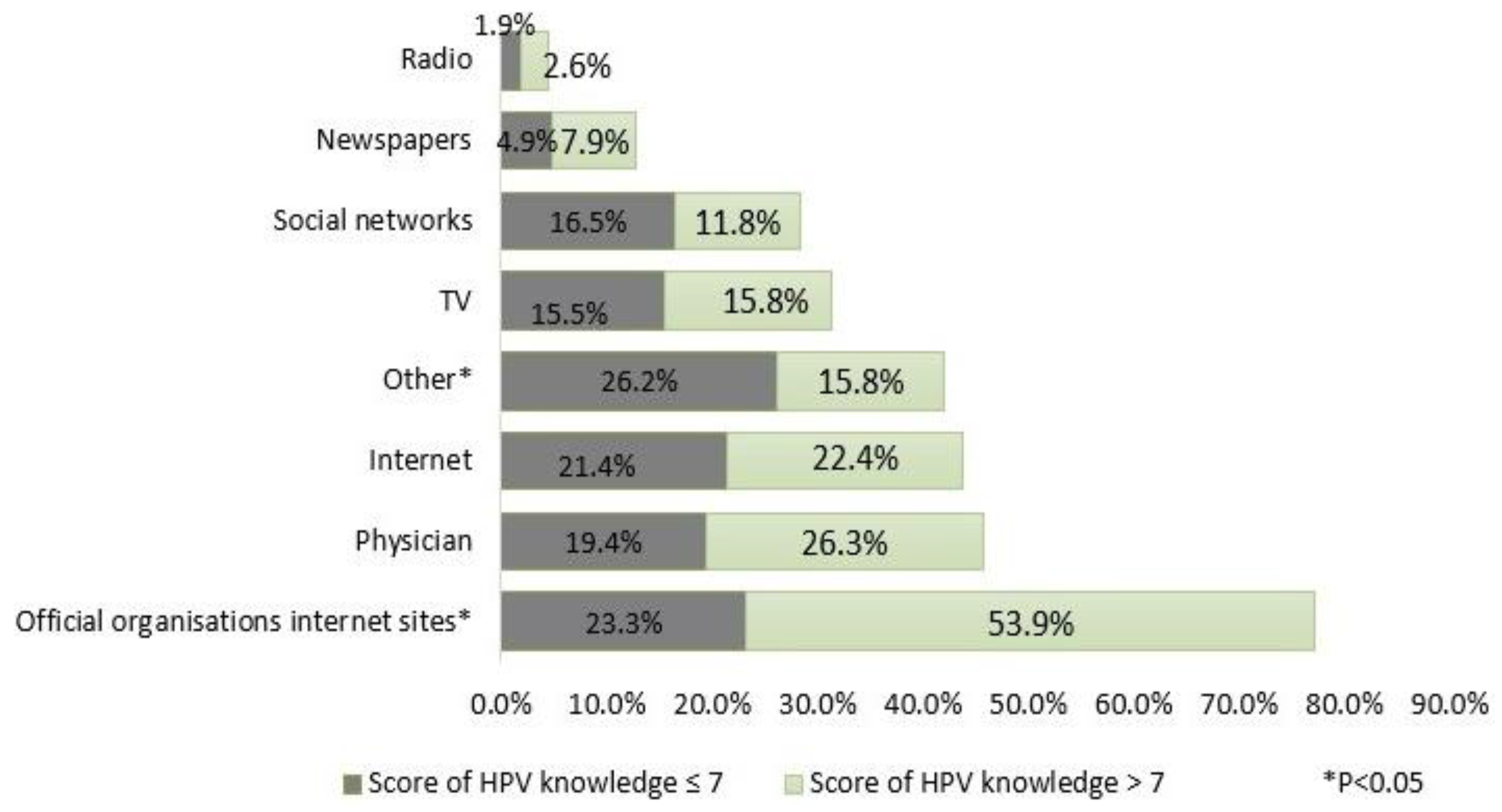
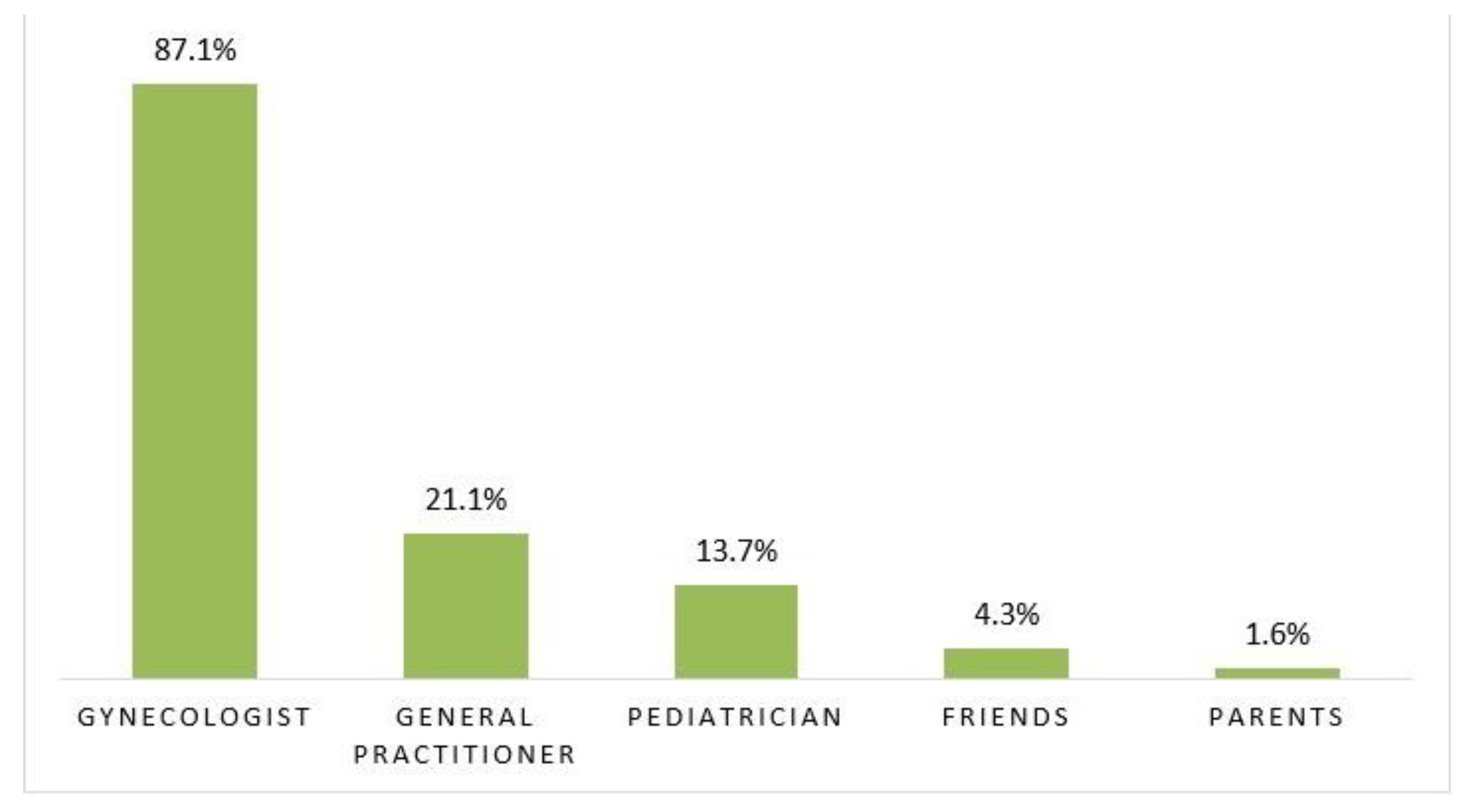
3.4. Sources of Information
3.5. HPV Vaccine Coverage
3.6. Attitudes towards Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Genital HPV Infection—CDC Fact Sheet. Available online: https://www.cdc.gov/std/hpv/hpv-Fs-July-2017.pdf (accessed on 28 November 2020).
- Serrano, B.; Brotons, M. Best Practice & Research Clinical Obstetrics and Gynaecology Epidemiology and burden of HPV-related disease. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 14–26. [Google Scholar] [CrossRef]
- ICO/IARC HPV Information Centre. Human Papillomavirus and Related Cancers, Fact Sheet 2018 (2019-06-17) I. Key Data on HPV and HPV-Related Cancers; ICO/IARC HPV Information Centre: Barcelona, Spain, 2019. [Google Scholar]
- Perišic, Ž.; Plešinac-Karapandžic, V.; Džinic, M. Cervical cancer screening in Serbia [Skrining karcinoma grlica materice u Srbiji]. Vojn Pregl. 2013, 70, 86–89. [Google Scholar] [CrossRef]
- Canfell, K. Towards the global elimination of cervical cancer. Papillomavirus Res. 2019, 8, 100170. [Google Scholar] [CrossRef]
- Grigore, M.; Teleman, S.I.; Pristavu, A.; Matei, M. Awareness and Knowledge about HPV and HPV Vaccine among Romanian Women. J. Cancer Educ. 2016, 33, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Flood, T.; Wilson, I.M.; Prue, G.; Mclaughlin, M.; Hughes, C.M. Impact of school-based educational interventions in middle adolescent populations (15–17 yrs) on human papillomavirus (HPV) vaccination uptake and perceptions / knowledge of HPV and its associated cancers: A systematic review. Prev. Med. 2020, 139, 106168. [Google Scholar] [CrossRef] [PubMed]
- Mediately. Medication Database. 2020. Available online: https://mediately.co/rs/atcs/J07B (accessed on 29 November 2020).
- Government of Republic of Serbia. Rule Bookon Immunization and the Way of Protection with Medicines. Official Gazette of RS, 88/2017. Available online: http://demo.paragraf.rs/WebParagrafDemo/?did=423949 (accessed on 29 November 2020).
- Institute of Public Health of Serbia “Dr Milan Jovanovic Batut”. Guidelines for Conduction of Obligatory and Recommended Active Immunization of the Population; Institute of Public Health of Serbia “Dr Milan Jovanovic Batut”: Belgrade, Serbia, 2018. [Google Scholar]
- Maric, G.; Bircanin, D.; Kisic, V.; Dotlic, J.; Zaric, M.; Kisic-Tepavcevic, D.; Gazibara, T. Parental perspective on human papillomavirus (HPV) vaccination in Serbia: Knowledge, attitudes and practice. Sex. Reprod. Healthc. 2018, 16, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.Z.; Kamizaki, S.S.; Quintana, S.M.; Pacagnella, R.D.C.; Surita, F.G. Knowledge of Pregnant Adolescents about Human Papillomavirus. Rev. Bras. Ginecol. Obstet. 2019, 41, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Loke, A.Y.; Kwan, M.L.; Wong, Y.T.; Wong, A.K.Y. The uptake of human papillomavirus vaccination and its associated factors among adolescents: A systematic review. J. Prim. Care Community Health 2017, 8, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.C.W.; Leung, G.M.; Woo, P.P.S.; Jit, M.; Wu, J.T. Acceptability and uptake of female adolescent HPV vaccination in Hong Kong: A survey of mothers and adolescents. Vaccine 2013, 32, 78–84. [Google Scholar] [CrossRef]
- Lee, A.; Ho, M.; Cheung, C.K.M.; Keung, V.M.W. Factors influencing adolescent girls’ decision in initiation for human papillomavirus vaccination: A cross-sectional study in Hong Kong. BMC Public Health 2014, 8, 925. [Google Scholar] [CrossRef] [Green Version]
- Djuric, O.; Markovic-Denic, L.; Popovac, S.; Todorovic, J.; Marusic, V.; Maksimovic, N. Awarennes and knowledge about HPV infection and HPV vaccination among women undergoing cytology and colposcopy in Serbian cervical cancer counseling center. JBUON 2020, 25, 116–124. [Google Scholar] [PubMed]
- Kesic, V.; Markovic, M.; Matejic, B.; Topic, L. Awareness of cervical cancer screening among women in Serbia. Gynecol. Oncol. 2005, 99 (Suppl. 1), S222–S225. [Google Scholar] [CrossRef] [PubMed]
- Musa, J.; Achenbach, C.J.; O’Dwyer, L.C.; Evans, C.T.; McHugh, M.; Hou, L.; Simon, M.A.; Murphy, R.L.; Jordan, N. Effect of cervical cancer education and provider recommendation for screening on screening rates: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0183924. [Google Scholar] [CrossRef] [PubMed]
- Heyman, K.P.; Worley, M.J.; Frey, M.K.; Kessler, R.T.; Bodurka, D.C.; Slomovitz, B.M. Willingness of pregnant women to vaccinate themselves and their newborns with the HPV vaccine. Vaccine 2011, 29, 4618–4622. [Google Scholar] [CrossRef]
- Riaz, L.; Manazir, S.; Jawed, F.; Arshad, A.S.; Ramsha Riaz, R. Knowledge, Perception, and Prevention Practices Related to Human Papillomavirus-based Cervical Cancer and Its Socioeconomic Correlates among Women in Karachi, Pakistan. Cureus 2020, 12, e7183. [Google Scholar] [CrossRef] [Green Version]
- ECDC. Guidance for the Introduction of HPV Vaccines in EU Countries. 2018. Available online: https://www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/0801_GUI_Introduction_of_HPV_Vaccines_in_EU.pdf (accessed on 29 November 2020).
- Niyibizi, J.; Zanré, N.; Mayrand, M.H.; Trottier, H. Association Between Maternal Human Papillomavirus Infection and Adverse Pregnancy Outcomes: Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 221, 1925–1937. [Google Scholar] [CrossRef]
- Vitek, W.S.; Akers, A.; Meyn, L.A.; Switzer, G.E.; Lee, B.Y.; Beigi, R.H. Vaccine eligibility and acceptance among ambulatory obstetric and gynecologic patients. Vaccine 2011, 29, 2024–2028. [Google Scholar] [CrossRef]
- Rosso, A.; Massimi, A.; De Vito, C.; Adamo, G.; Baccolini, V.; Marzuillo, C.; Vacchio, M.R.; Villari, P. Knowledge and attitudes on pediatric vaccinations and intention to vaccinate in a sample of pregnant women from the City of Rome. Vaccine 2019, 37, 1954–1963. [Google Scholar] [CrossRef]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Newman, P.A.; Logie, C.H.; Lacombe-duncan, A.; Baiden, P.; Tepjan, S.; Rubincam, C.; Doukas, N.; Asey, F. Parents’ uptake of human papillomavirus vaccines for their children: A systematic review and meta- analysis of observational studies. BMJ Open 2018, 8, e019206. [Google Scholar] [CrossRef]
- Chen, J.; Gopala, K.; Akarsh, P.K.; Struyf, F.; Rosillon, D. Prevalence and Incidence of Human Papillomavirus (HPV) Infection Before and After Pregnancy: Pooled Analysis of the Control Arms of Efficacy Trials of HPV-16/18 AS04-Adjuvanted Vaccine. Open Forum Infect. Dis. 2019, 6, ofz486. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total (n = 256) | |
|---|---|
| Demographic characteristics | n (%) |
| Age ** | 33.0 ± 7.1 |
| Level of education—school | |
| Elementary | 16 (6.3) |
| Secondary | 97 (38.2) |
| Faculty | 141 (55.5) |
| Marital status | |
| Married/Cohabiting | 245 (96.9) |
| Single | 8 (3.2) |
| Residence | |
| Rural | 31 (12.2) |
| Urban | 223 (87.8) |
| Employment | |
| Non-employed | 65 (25.8) |
| Employed | 187 (74.2) |
| Gynecological data | |
| Age at menarche (years) ** | 12.9 ± 1.5 |
| Age at first sexual intercourse (years) ** | 19.1 ± 3.1 |
| Treated for infertility | 27 (10.5) |
| Number of abortions | |
| 0 | 179 (69.9) |
| ≥1 | 68 (26.6) |
| Missing | 9 (3.5) |
| Number of children | |
| 0 | 114 (44.5) |
| ≥1 | 119 (46.5) |
| Missing | 23 (9.0) |
| Number of sexual partners (total) | |
| 1 | 65 (25.4) |
| 2–5 | 120 (46.9) |
| ≥6 | 31 (12.1) |
| Missing | 40 (15.6) |
| Number of sexual partners (in last 3 months) | |
| 0 | 15 (5.9) |
| 1 | 206 (80.5) |
| 2–5 | 0 (0.0) |
| ≥6 | 0 (0.0) |
| Missing | 35 (13.7) |
| Ever Heard of HPV (n = 203) | Ever Heard of HPV Vaccine (n = 96) | |||||
|---|---|---|---|---|---|---|
| n (%) | OR (95% CI) | Knowledge score * | n (%) | OR (95% CI) | Knowledge score * | |
| Demographic characteristics | ||||||
| Age ** | 33.4 ± 7.2 | 1.05 (1.00–1.10) | / | 35.1 ± 7.3 | 1.07 (1.03–1.12) | / |
| Level of ducation | ||||||
| Elementary | 5 (2.5) | ref. | 2 (4) | / | / | / |
| Secondary | 72 (35.6) | 6.34 (2.00–20.03) | 5 (5) | 20 (20.8) | ref. | 3 (1) |
| Faculty | 125 (61.9) | 17.19 (5.29–55.84) | 7 (4) | 76 (79.2) | 4.55 (2.50–8.27) | 3 (2) |
| Marital status | ||||||
| Married/Cohabiting | 197 (97.5) | ref. | 7 (4) | 93 (97.9) | ref. | 3 (2) |
| Single | 5 (2.5) | 0.41 (0.09–1.76) | 8 (9) | 2 (2.1) | 0.62 (0.12–3.28) | 2 (0) |
| Residence | ||||||
| Rural | 20 (9.9) | ref. | 4 (6) | 5 (5.2) | ref. | 3 (2) |
| Urban | 183 (90.1) | 2.52 (1.12–5.66) | 7 (4) | 91 (94.8) | 3.85 (1.42–10.40) | 3 (2) |
| Employment | ||||||
| Non-employed | 44 (22.0) | ref. | 6 (5) | 18 (18.8) | ref. | 3.5 (2) |
| Employed | 156 (78.0) | 2.40 (1.26–4.59) | 7 (4) | 78 (81.3) | 1.85 (0.99–3.45) | 3 (2) |
| Gynecological data | ||||||
| Age at menarche (years) ** | 12.8 ± 1.5 | 0.79 (0.65–0.97) | / | 12.8 ± 1.4 | 0.88 (0.73–1.05) | / |
| Age at first sexual intercourse (years) ** | 19.1 ± 3.1 | 1.01 (0.91–1.12) | / | 19.7 ± 3.5 | 1.10 (1.01–1.20) | / |
| Treated for infertility | 21 (10.3) | 0.91 (0.35–2.39) | 7 (5) | 11 (11.5) | 1.17 (0.51–2.67) | 3 (2) |
| Number of abortions | ||||||
| 0 | 142 (70.0) | ref. | 7 (5) | 64 (66.7) | ref. | 3 (2) |
| ≥1 | 54 (26.6) | 1.10 (0.22–5.50) | 7 (5) | 25 (26.0) | 0.08 (0.01–0.70) | 3 (2) |
| Missing | 7 (3.4) | 1.10 (0.21–5.90) | 6 (4) | 7 (7.3) | 0.08 (0.01–0.73) | 2 (1) |
| Number of children | ||||||
| 0 | 88 (43.3) | ref. | 7 (5) | 40 (41.7) | ref. | 3 (2) |
| ≥1 | 96 (47.3) | 0.71 (0.22–2.28) | 6 (4) | 45 (46.9) | 0.63 (0.26–1.56) | 3 (1.5) |
| Missing | 19 (9.4) | 0.88 (0.27–2.83) | 7 (3) | 11 (11.5) | 0.70 (0.28–1.72) | 2 (1) |
| Number of sexual partners (total) | ||||||
| 1 | 50 (24.6) | ref. | 6 (4) | 25 (26.0) | ref. | 3 (1) |
| 2–5 | 92 (45.3) | 0.48 (0.16–1.43) | 7 (5) | 44 (45.8) | 1.32 (0.57–3.03) | 3 (2) |
| ≥6 | 26 (12.8) | 0.47 (0.17–1.31) | 7.5 (4) | 14 (14.6) | 1.24 (0.58–2.66) | 4 (2.3) |
| Missing | 35 (17.2) | 0.74 (0.19–2.83) | 6 (4) | 13 (13.5) | 1.75 (0.66–4.66) | 2 (1.5) |
| Number of sexual partners (in last 3 months) | ||||||
| 0 | 10 (4.9) | ref. | 6 (4) | 5 (5.2) | ref. | 5 (3.5) |
| 1 | 165 (81.3) | 0.50 (0.13–1.94) | 7 (5) | 76 (79.2) | 0.70 (0.19–2.55) | 3 (2) |
| 2–5 | 0 (0.0) | / | / | 0 (0.0) | / | / |
| ≥6 | 0 (0.0) | / | / | 0 (0.0) | / | / |
| Missing | 28 (13.8) | 1.01 (0.41–2.46) | 7 (3) | 15 (15.6) | 0.78 (0.37–1.63) | 2 (1) |
| HPV Knowledge Item (Correct Answer) | Yes | No | I Don’t Know | Total Number of Answers |
|---|---|---|---|---|
| Total Women Included 203 | n (%) | n (%) | n (%) | n (%) |
| Is there more than one type of human papilloma virus? (yes) | 120 (59.1) | 5 (2.5) | 75 (36.9) | 200 (98.5) |
| Can HPV be transmitted by sexual contact? (yes) | 175 (86.2) | 3 (1.5) | 22 (10.8) | 200 (98.5) |
| Can human papillomaviruses be transmitted through towels, toilets, swimming pools, etc.? (no) | 67 (33.0) | 54 (26.6) | 81 (39.9) | 202 (99.5) |
| If a pregnant woman is infected with human papilloma viruses, can they be transmitted to the newborn during childbirth? (yes) | 102 (50.2) | 13 (6.4) | 85 (41.9) | 200 (98.5) |
| Can person infected by HPV have no symptoms? (yes) | 107 (52.7) | 24 (11.8) | 69 (34.0) | 200 (98.5) |
| Does the risk of human papillomavirus infection increase with the number of sexual partners? (yes) | 147 (72.4) | 11 (5.4) | 42 (20.7) | 200 (98.5) |
| Can HPV cause infection in men? (yes) | 137 (67.5) | 10 (4.9) | 54 (26.6) | 201 (99.0) |
| Can infections caused by HPV be cured spontaneously? (yes) | 28 (13.8) | 121 (59.6) | 50 (24.6) | 199 (98.0) |
| Can HPV cause genital warts? (yes) | 146 (71.9) | 4 (2.0) | 52 (25.6) | 202 (99.5) |
| Can HPV cause cervical carcinoma? (yes) | 131 (68.2) | 4 (2.1) | 57 (29.7) | |
| Do most sexually active people get human papillomaviruses at some time in their lifetime? (yes) | 93 (45.8) | 27 (13.3) | 81 (39.9) | 201 (99.0) |
| Can condoms prevent occurrence of infection caused by HPV? (no) | 158 (77.8) | 20 (9.9) | 24 (11.8) | 202 (99.5) |
| Median (IQR) knowledge score | 7.0 (5.0) | |||
| HPV vaccine knowledge item (correct answer) | ||||
| Total women included 96 | ||||
| Is the vaccine available in Serbia? (yes) | 62 (64.6) | 5 (5.2) | 29 (30.2) | 96 (100.0) |
| Is the vaccine recommended before first sexual intercourse? (yes) | 68 (70.8) | 1 (1.0) | 27 (28.1) | 96 (100.0) |
| Whether vaccinated women should go for cervical cancer screening? (yes) | 70 (72.9) | 0 (0.0) | 25 (26.0) | 95 (99.0) |
| Whether the vaccine can cause cervical cancer? (no) | 14 (14.6) | 54 (56.3) | 28 (29.2) | 96 (100.0) |
| Is the vaccine also recommended for men? (yes) | 31 (32.3) | 16 (16.7) | 49 (51.0) | 96 (100.0) |
| Median (IQR) knowledge score | 3.0 (2.0) |
| Attitudes towards Vaccination | Total (n = 237) | Total Vaccine Aware (n = 96) | HPV Vaccine Knowledge Score ≤ 3 (n = 61) | Score of HPV Vaccine Knowledge > 3 (n = 35) | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | OR (95% CI) | |
| Would be vaccinated | 66 (25.8) | 43 (44.8) | 23 (38.3) | 20 (57.1) | 2.14 (0.92–5.01) |
| Would vaccinate her female child | 101 (39.5) | 62 (64.6) | 33 (54.1) | 29 (82.9) | 4.10 (1.50–11.29) |
| Would vaccinate her male child | 77 (30.1) | 45 (46.9) | 22 (36.1) | 23 (67.6) | 3.71 (1.52–9.01) |
| Will she vaccinate her child against diseases for which vaccination is mandatory | 204 (79.7) | 84 (87.5) | 51 (87.9) | 33 (97.1) | 4.53 (0.53–38.52) |
| Variable | Multivariate Logistic Regression |
|---|---|
| OR (95% CI) | |
| Age | 1.05 (0.98–1.13) |
| High education (>12 years of schooling) | 2.47 (0.70–8.65) |
| Employed vs. not employed | 0.68 (0.17–2.66) |
| Number of children | 1.32 (1.04–1.67) |
| HPV vaccine knowledge score | 1.64 (1.13–2.39) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markovic-Denic, L.; Milicevic, S.; Todorovic, J.; Nikolic, V.; Djuric, O.; Marusic, V.; Dugalic, S.; Vasiljevic, B.; Gojnic-Dugalic, M. Uptake of Human Papillomavirus Vaccine and Intention to Vaccinate among Healthy Pregnant Women in Serbia: A Cross-Sectional Study on Awareness, Knowledge, and Attitudes. Viruses 2021, 13, 727. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050727
Markovic-Denic L, Milicevic S, Todorovic J, Nikolic V, Djuric O, Marusic V, Dugalic S, Vasiljevic B, Gojnic-Dugalic M. Uptake of Human Papillomavirus Vaccine and Intention to Vaccinate among Healthy Pregnant Women in Serbia: A Cross-Sectional Study on Awareness, Knowledge, and Attitudes. Viruses. 2021; 13(5):727. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050727
Chicago/Turabian StyleMarkovic-Denic, Ljiljana, Srboljub Milicevic, Jovana Todorovic, Vladimir Nikolic, Olivera Djuric, Vuk Marusic, Stefan Dugalic, Brankica Vasiljevic, and Miroslava Gojnic-Dugalic. 2021. "Uptake of Human Papillomavirus Vaccine and Intention to Vaccinate among Healthy Pregnant Women in Serbia: A Cross-Sectional Study on Awareness, Knowledge, and Attitudes" Viruses 13, no. 5: 727. https://0-doi-org.brum.beds.ac.uk/10.3390/v13050727