
One Health Investigation of SARS-CoV-2 Infection and Seropositivity among Pets in Households with Confirmed Human COVID-19 Cases—Utah and Wisconsin, 2020

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Enrollment
2.2. Household Visits
2.3. rRT-PCR and Serology of Animal Specimens
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
Appendix C
Appendix C.1. RNA Extraction and rRT-PCR of Animal Specimens
Appendix C.2. Virus Neutralization
Appendix C.3. Genome Sequencing and Analysis
Appendix C.4. Viral Culture of Fur Swab
Appendix D
Appendix D.1. Unique Medical Histories and Clinical Signs
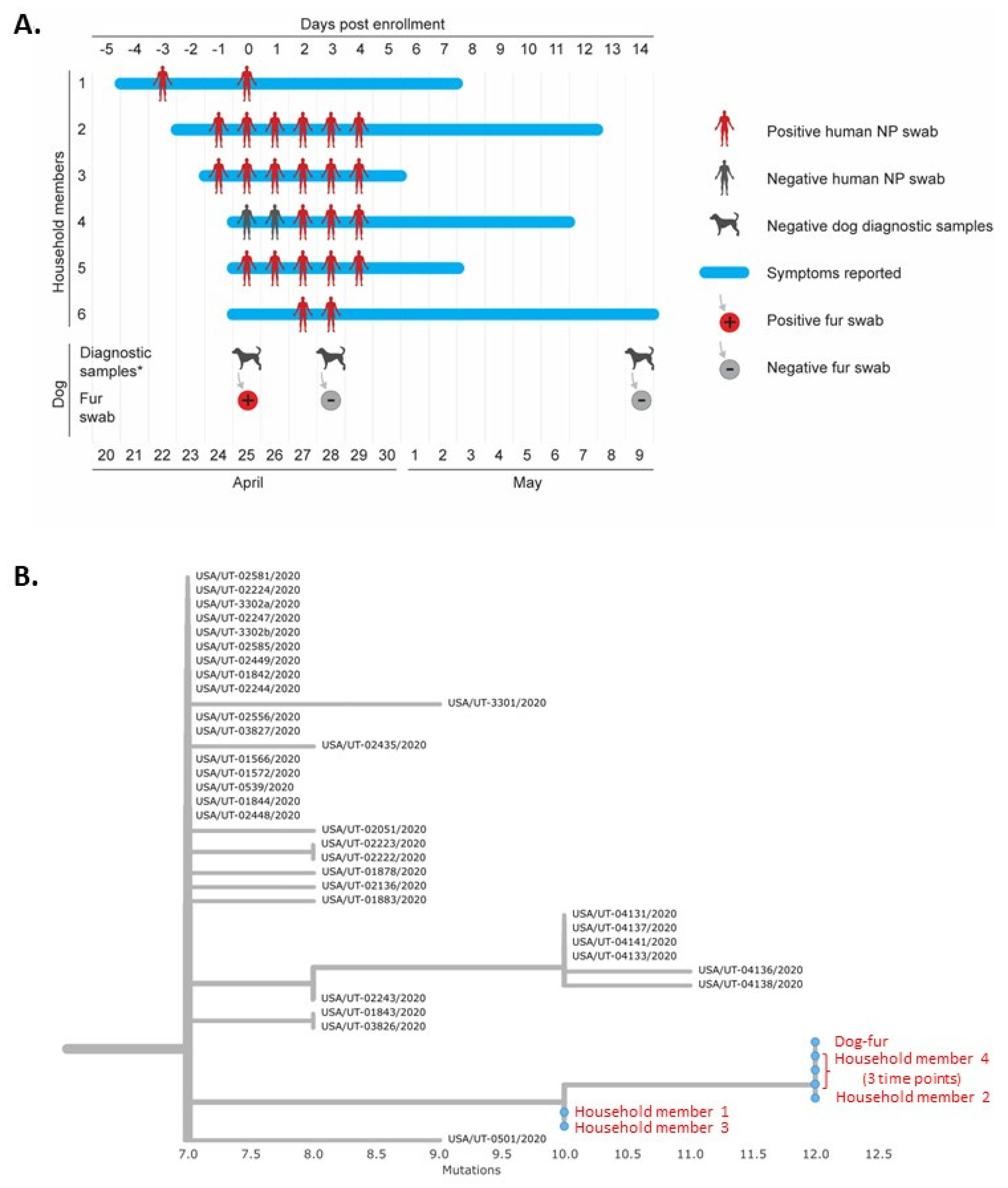
Appendix D.2. Sequence Analysis of Household UT-36 Human Samples and Dog Fur Swab
Appendix D.3. Presumptive Positive Sample
References
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of sars-cov-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [Green Version]
- El Zowalaty, M.E.; Järhult, J.D. From sars to covid-19: A previously unknown sars- related coronavirus (sars-cov-2) of pandemic potential infecting humans—Call for a one health approach. One Health 2020, 9, 100124. [Google Scholar] [CrossRef]
- American Pet Products Association. 2019–2020 Appa National Pet Owners Survey; American Pet Products Association: Stamford, CT, USA, 2019. [Google Scholar]
- Bowen, J.; García, E.; Darder, P.; Argüelles, J.; Fatjó, J. The effects of the spanish covid-19 lockdown on people, their pets, and the human-animal bond. J. Vet. Behav. 2020, 40, 75–91. [Google Scholar] [CrossRef]
- Duncan, S.L.; Allen, K.J.H. Service animals and their roles in enhancing independence, quality of life, and employment for people with disabilities. In Handbook on Animal-Assisted Therapy: Theoretical Foundations and Guidelines for Practice; Acadmic Press: San Diego, CA, USA, 2000; pp. 303–323. [Google Scholar]
- Sit, T.H.C.; Brackman, C.J.; Ip, S.M.; Tam, K.W.S.; Law, P.Y.T.; To, E.M.W.; Yu, V.Y.T.; Sims, L.D.; Tsang, D.N.C.; Chu, D.K.W.; et al. Infection of dogs with sars-cov-2. Nature 2020, 586, 776–778. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhang, H.; Huang, K.; Yang, Y.; Hui, X.; Gao, J.; He, X.; Li, C.; Gong, W.; Zhang, Y.; et al. Sars-cov-2 neutralizing serum antibodies in cats: A serological investigation. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- World Organisation for Animal Health. Events in Animals. Available online: https://www.oie.int/en/scientific-expertise/specific-information-and-recommendations/questions-and-answers-on-2019novel-coronavirus/events-in-animals/ (accessed on 8 September 2021).
- Shi, J.; Wen, Z.; Zhong, G.; Yang, H.; Wang, C.; Huang, B.; Liu, R.; He, X.; Shuai, L.; Sun, Z.; et al. Susceptibility of ferrets, cats, dogs, and other domesticated animals to sars–coronavirus 2. Science 2020, 368, 1016–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.F.; Zhang, A.J.; Yuan, S.; Poon, V.K.; Chan, C.C.; Lee, A.C.; Chan, W.M.; Fan, Z.; Tsoi, H.W.; Wen, L.; et al. Simulation of the clinical and pathological manifestations of coronavirus disease 2019 (covid-19) in golden syrian hamster model: Implications for disease pathogenesis and transmissibility. Clin. Infect. Dis. 2020, 17, 2139–2149. [Google Scholar] [CrossRef] [PubMed]
- Mykytyn, A.Z.; Lamers, M.M.; Okba, N.M.A.; Breugem, T.I.; Schipper, D.; van den Doel, P.B.; van Run, P.; van Amerongen, G.; Waal, L.d.; Koopmans, M.P.G.; et al. Susceptibility of rabbits to sars-cov-2. bioRxiv 2020. [Google Scholar] [CrossRef]
- Bosco-Lauth, A.M.; Hartwig, A.E.; Porter, S.M.; Gordy, P.W.; Nehring, M.; Byas, A.D.; VandeWoude, S.; Ragan, I.K.; Maison, R.M.; Bowen, R.A. Pathogenesis, transmission and response to re-exposure of sars-cov-2 in domestic cats. BioRxiv 2020. [Google Scholar] [CrossRef]
- Halfmann, P.J.; Hatta, M.; Chiba, S.; Maemura, T.; Fan, S.; Takeda, M.; Kinoshita, N.; Hattori, S.-i.; Sakai-Tagawa, Y.; Iwatsuki-Horimoto, K.; et al. Transmission of sars-cov-2 in domestic cats. N. Engl. J. Med. 2020, 383, 592–594. [Google Scholar] [CrossRef]
- Kim, Y.I.; Kim, S.G.; Kim, S.M.; Kim, E.H.; Park, S.J.; Yu, K.M.; Chang, J.H.; Kim, E.J.; Lee, S.; Casel, M.A.B.; et al. Infection and rapid transmission of sars-cov-2 in ferrets. Cell Host Microbe 2020, 27, 704–709.e702. [Google Scholar] [CrossRef] [PubMed]
- Hamer, S.A.; Ghai, R.R.; Zecca, I.B.; Auckland, L.D.; Roundy, C.M.; Davila, E.; Busselman, R.E.; Tang, W.; Pauvolid-Corrêa, A.; Killian, M.L.; et al. Sars-cov-2 b.1.1.7 variant of concern detected in a pet dog and cat after exposure to a person with covid-19, USA. Transbound. Emerg. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hamer, S.A.; Pauvolid-Corrêa, A.; Zecca, I.B.; Davila, E.; Auckland, L.D.; Roundy, C.M.; Tang, W.; Torchetti, M.K.; Killian, M.L.; Jenkins-Moore, M.; et al. Sars-cov-2 infections and viral isolations among serially tested cats and dogs in households with infected owners in texas, USA. Viruses 2021, 13, 938. [Google Scholar] [CrossRef] [PubMed]
- Lewis, N.M.; Chu, V.T.; Ye, D.; Conners, E.E.; Gharpure, R.; Laws, R.L.; Reses, H.E.; Freeman, B.D.; Fajans, M.; Rabold, E.M.; et al. Household transmission of sars-cov-2 in the united states. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. What To Do If You Are Sick. Available online: https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/steps-when-sick.html (accessed on 8 September 2021).
- Wang, L.; Mitchell, P.K.; Calle, P.P.; Bartlett, S.L.; McAloose, D.; Killian, M.L.; Yuan, F.; Fang, Y.; Goodman, L.B.; Fredrickson, R.; et al. Complete genome sequence of sars-cov-2 in a tiger from a u.S. Zoological collection. Microbiol. Resour. Announc. 2020, 9, e00468-20. [Google Scholar] [CrossRef]
- United States Department of Agriculture. Confirmed Cases of Sars-Cov-2 in Animals in the United States. Available online: https://www.aphis.usda.gov/aphis/ourfocus/animalhealth/sa_one_health/sars-cov-2-animals-us (accessed on 8 September 2021).
- Patterson, E.I.; Elia, G.; Grassi, A.; Giordano, A.; Desario, C.; Medardo, M.; Smith, S.L.; Anderson, E.R.; Prince, T.; Patterson, G.T.; et al. Evidence of exposure to sars-cov-2 in cats and dogs from households in Italy. Nat. Commun. 2020, 11, 6231. [Google Scholar] [CrossRef] [PubMed]
- Temmam, S.; Barbarino, A.; Maso, D.; Behillil, S.; Enouf, V.; Huon, C.; Jaraud, A.; Chevallier, L.; Backovic, M.; Pérot, P.; et al. Absence of sars-cov-2 infection in cats and dogs in close contact with a cluster of covid-19 patients in a veterinary campus. One Health 2020, 10, 100164. [Google Scholar] [CrossRef]
- Barrs, V.R.; Peiris, M.; Tam, K.W.S.; Law, P.Y.T.; Brackman, C.J.; To, E.M.W.; Yu, V.Y.T.; Chu, D.K.W.; Perera, R.; Sit, T.H.C. Sars-cov-2 in quarantined domestic cats from covid-19 households or close contacts, Hong Kong, China. Emerg. Infect. Dis. 2020, 26. [Google Scholar] [CrossRef]
- Spada, E.; Vitale, F.; Bruno, F.; Castelli, G.; Reale, S.; Perego, R.; Baggiani, L.; Proverbio, D. A pre- and during pandemic survey of sars-cov-2 infection in stray colony and shelter cats from a high endemic area of northern Italy. Viruses 2021, 13, 618. [Google Scholar] [CrossRef]
- Stranieri, A.; Lauzi, S.; Giordano, A.; Galimberti, L.; Ratti, G.; Decaro, N.; Brioschi, F.; Lelli, D.; Gabba, S.; Amarachi, N.L.; et al. Absence of sars-cov-2 rna and anti-sars-cov-2 antibodies in stray cats. Transbound. Emerg. Dis. 2021. [Google Scholar] [CrossRef]
- Villanueva-Saz, S.; Giner, J.; Tobajas, A.P.; Pérez, M.D.; González-Ramírez, A.M.; Macías-León, J.; González, A.; Verde, M.; Yzuel, A.; Hurtado-Guerrero, R.; et al. Serological evidence of sars-cov-2 and co-infections in stray cats in Spain. Transbound. Emerg. Dis. 2021. [Google Scholar] [CrossRef]
- Gaudreault, N.N.; Trujillo, J.D.; Carossino, M.; Meekins, D.A.; Morozov, I.; Madden, D.W.; Indran, S.V.; Bold, D.; Balaraman, V.; Kwon, T.; et al. Sars-cov-2 infection, disease and transmission in domestic cats. bioRxiv 2020. [Google Scholar] [CrossRef]
- Lauzi, S.; Stranieri, A.; Giordano, A.; Lelli, D.; Elia, G.; Desario, C.; Ratti, G.; Decaro, N.; Paltrinieri, S. Do dogs and cats passively carry sars-cov-2 on hair and pads? Viruses 2021, 13, 1357. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. If You Have Pets. Available online: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/pets.html (accessed on 8 September 2021).
- Garigliany, M.; Van Laere, A.S.; Clercx, C.; Giet, D.; Escriou, N.; Huon, C.; van der Werf, S.; Eloit, M.; Desmecht, D. Sars-cov-2 natural transmission from human to cat, Belgium, March 2020. Emerg. Infect. Dis. 2020, 26, 3069. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.; Smith, D.; Ghai, R.R.; Wallace, R.M.; Torchetti, M.K.; Loiacono, C.; Murrell, L.S.; Carpenter, A.; Moroff, S.; Rooney, J.A.; et al. First reported cases of sars-cov-2 infection in companion animals—New York, March–April 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Leroy, E.M.; Ar Gouilh, M.; Brugère-Picoux, J. The risk of sars-cov-2 transmission to pets and other wild and domestic animals strongly mandates a one-health strategy to control the covid-19 pandemic. One Health 2020, 10, 100133. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Cdc 2019-Novel Coronavirus (2019-ncov) Real-Time Rt-Pcr Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 8 September 2021).
- Mercatelli, D.; Giorgi, F.M. Geographic and genomic distribution of sars-cov-2 mutations. Front. Microbiol. 2020, 11, 1800. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total N (Column %) | Blood Sample Collected | No Blood Sample Collected n (Row %) | |
|---|---|---|---|---|
| Seropositive 1 n (Row %) | Seronegative n (Row %) | |||
| Total | 56 | 8 (14) | 39 (70) | 9 (16) |
| Study site | ||||
| Utah | 38 (68) | 6 (16) | 31 (82) | 1 (3) |
| Wisconsin | 18 (32) | 2 (11) | 8 (44) | 8 (44) |
| Species | ||||
| Dog | 37 (66) | 4 (11) | 30 (81) | 3 (8) |
| Cat | 19 (34) | 4 (21) | 9 (47) | 6 (32) |
| Age (years) | ||||
| <2 | 11 (20) | 1 (9) | 7 (64) | 3 (27) |
| 2–9 | 33 (59) | 5 (15) | 23 (70) | 5 (15) |
| ≥10 | 12 (21) | 2 (17) | 9 (75) | 1 (8) |
| Sex and reproductive status | ||||
| Male | 29 (52) | 4 (14) | 19 (66) | 6 (21) |
| Neutered | 23 (79) | 3 (13) | 16 (70) | 4 (17) |
| Female | 27 (48) | 4 (15) | 20 (74) | 3 (11) |
| Spayed | 22 (81) | 4 (18) | 15 (68) | 3 (14) |
| Indoor/outdoor housing environment | ||||
| Primarily indoors | 55 (98) | 7 (13) | 39 (71) | 9 (16) |
| Primarily outdoors 2 | 1 (2) | 1 (100) | 0 | 0 |
| Exposures outside of the household setting 3 | ||||
| Spent any time free-roaming in the yard or the neighborhood | 29 (52) | 5 (17) | 21 (72) | 3 (10) |
| Attended a social setting (e.g., dog park, daytime boarding facility, veterinary clinic) | 5 (9) | 0 | 5 (100) | 0 |
| Characteristics | Total Households N = 34 | Households with ≥1 Seropositive 1 Pet n = 6 | Households with Seronegative Pet(s) Only n = 24 | Households with No Pet Blood Sample Collected n= 4 | p-Value 2 |
|---|---|---|---|---|---|
| Human SARS-CoV-2 infection and timing | |||||
| Median (range) | |||||
| Proportion of human household members 3 with laboratory evidence of SARS-CoV-2 infection 4 | 0.45 (0.13–1.00) | 0.79 (0.40–1.00) | 0.37 (0.13–1.00) | 0.63 (0.25–1.00) | 0.01 |
| Days from symptom onset in the human index patient to first date of pet sampling | 27 (3–46) | 28 (22–39) | 24 (3–46) | 32.5 (24–42) | 0.30 |
| Days from first positive diagnostic result of the human index patient to first date of pet sampling | 20.5 (3–42) | 21.5 (18–38) | 20 (3–41) | 25.5 (21–42) | 0.37 |
| Household members and size | |||||
| Median (range) | |||||
| No. persons 5 | 4 (2–8) | 4·5 (3–6) | 4 (2–8) | 3 (2–4) | 0.70 |
| No. dogs and cats 6 | 1 (1–5) | 1·5 (1–3) | 1 (1–5) | 1 (1–2) | 0.47 |
| Total square meters | 213.68 (55.74–706.06) | 181.16 (90.95–315.87) | 241.55 (55.74–706.06) | 192.40 (130.06–260.13) | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goryoka, G.W.; Cossaboom, C.M.; Gharpure, R.; Dawson, P.; Tansey, C.; Rossow, J.; Mrotz, V.; Rooney, J.; Torchetti, M.; Loiacono, C.M.; et al. One Health Investigation of SARS-CoV-2 Infection and Seropositivity among Pets in Households with Confirmed Human COVID-19 Cases—Utah and Wisconsin, 2020. Viruses 2021, 13, 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091813
Goryoka GW, Cossaboom CM, Gharpure R, Dawson P, Tansey C, Rossow J, Mrotz V, Rooney J, Torchetti M, Loiacono CM, et al. One Health Investigation of SARS-CoV-2 Infection and Seropositivity among Pets in Households with Confirmed Human COVID-19 Cases—Utah and Wisconsin, 2020. Viruses. 2021; 13(9):1813. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091813
Chicago/Turabian StyleGoryoka, Grace W., Caitlin M. Cossaboom, Radhika Gharpure, Patrick Dawson, Cassandra Tansey, John Rossow, Victoria Mrotz, Jane Rooney, Mia Torchetti, Christina M. Loiacono, and et al. 2021. "One Health Investigation of SARS-CoV-2 Infection and Seropositivity among Pets in Households with Confirmed Human COVID-19 Cases—Utah and Wisconsin, 2020" Viruses 13, no. 9: 1813. https://0-doi-org.brum.beds.ac.uk/10.3390/v13091813