
A Comprehensive Report of German Nationwide Inpatient Data on the Post-COVID-19 Syndrome Including Annual Direct Healthcare Costs
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patient-Led Research Collaborative Report. What Does COVID-19 Recovery Actually Look Like? An Analysis of the Prolonged COVID-19 Symptoms Survey by Patient-Led Research Team. Available online: https://patientresearchcovid19.com/research/report-1/ (accessed on 22 September 2022).
- NICE COVID-19 rapid guidelines. PharmacoEcon. Outcomes News 2021, 877, 33. [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. 2022, 74, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef]
- Havervall, S.; Rosell, A.; Phillipson, M.; Mangsbo, S.M.; Nilsson, P.; Hober, S.; Thålin, C. Symptoms and Functional Impairment Assessed 8 Months after Mild COVID-19 Among Health Care Workers. JAMA 2021, 325, 2015–2016. [Google Scholar] [CrossRef]
- Ziegler, S.; Raineri, A.; Nittas, V.; Rangelov, N.; Vollrath, F.; Britt, C.; Puhan, M.A. Long COVID Citizen Scientists: Developing a Needs-Based Research Agenda by Persons Affected by Long COVID. Patient 2022, 15, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Andrenelli, E.; Negrini, F.; Sire, A.D.; Arienti, C.; Patrini, M.; Negrini, S.; Ceravolo, M.G. Systematic rapid living review on rehabilitation needs due to COVID-19: Update to May 31st, 2020. Eur. J. Phys. Rehabil. Med. 2020, 56, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Sire, A.D.; Andrenelli, E.; Negrini, F.; Lazzarini, S.G.; Patrini, M.; Ceravolo, M.G. Rehabilitation and COVID-19: The Cochrane Rehabilitation 2020 rapid living systematic review. Update as of 31 August 2020. Eur. J. Phys. Rehabil. Med. 2020, 56, 839–845. [Google Scholar] [CrossRef]
- Sire, A.D.; Andrenelli, E.; Negrini, F.; Patrini, M.; Lazzarini, S.G.; Ceravolo, M.G. Rehabilitation and COVID-19: A rapid living systematic review by Cochrane Rehabilitation Field updated as of 31 December 2020 and synthesis of the scientific literature of 2020. Eur. J. Phys. Rehabil. Med. 2021, 57, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Alwan, N.A.; Johnson, L. Defining long COVID: Going back to the start. Med 2021, 2, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Nittas, V.; Gao, M.; West, E.A.; Ballouz, T.; Menges, D.; Wulf Hanson, S.; Puhan, M.A. Long COVID Through a Public Health Lens: An Umbrella Review. Public Health Rev. 2022, 43, 1604501. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2021, 27, 89–95. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months after COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. EClinicalMedicine 2020, 38, 101019. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2021, 76, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Mendiola-Pastrana, I.R.; López-Ortiz, E.; La Río de Loza-Zamora, J.G.; González, J.; Gómez-García, A.; López-Ortiz, G. SARS-CoV-2 Variants and Clinical Outcomes: A Systematic Review. Life 2022, 12, 170. [Google Scholar] [CrossRef] [PubMed]
- Santhosh, L. Beyond “In the Red”: Building the Business Case for a Post–COVID-19 Clinic. Ann. Am. Thorac. Soc. 2022, 19, 1257–1259. [Google Scholar] [CrossRef]
- Richards, F.; Kodjamanova, P.; Chen, X.; Li, N.; Atanasov, P.; Bennetts, L.; Patterson, B.J.; Yektashenas, B.; Mesa-Frias, M.; Tronczynski, K.; et al. Economic Burden of COVID-19: A Systematic Review. Clinicoecon. Outcomes Res. 2022, 14, 293–307. [Google Scholar] [CrossRef]
- Bartsch, S.M.; Ferguson, M.C.; McKinnell, J.A.; O’Shea, K.J.; Wedlock, P.T.; Siegmund, S.S.; Lee, B.Y. The Potential Health Care Costs And Resource Use Associated With COVID-19 In The United States. Health Aff. 2020, 39, 927–935. [Google Scholar] [CrossRef] [Green Version]
- Koumpias, A.M.; Schwartzman, D.; Fleming, O. Long-haul COVID: Healthcare utilization and medical expenditures 6 months post-diagnosis. BMC Health Serv. Res. 2022, 22, 1010. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Suri, R.; Suchyta, M.R.; Digrande, K.F.; Sherwood, K.D.; Colantuoni, E.; Dinglas, V.D.; Needham, D.M.; Hopkins, R.O. Return to work after critical illness: A systematic review and meta-analysis. Thorax 2020, 75, 17–27. [Google Scholar] [CrossRef]
- Cutler, D.M. The Costs of Long COVID. JAMA Health Forum 2022, 3, e221809. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; Koyanagi, A.; Smith, L.; Tanislav, C.; Konrad, M.; van der Beck, S.; Kostev, K. Prevalence of, and factors associated with, long-term COVID-19 sick leave in working-age patients followed in general practices in Germany. Int. J. Infect. Dis. 2021, 109, 203–208. [Google Scholar] [CrossRef]
- Sandmann, F.G.; Tessier, E.; Lacy, J.; Kall, M.; van Leeuwen, E.; Charlett, A.; Eggo, R.M.; Dabrera, G.; Edmunds, W.J.; Ramsay, M.; et al. Long-Term Health-Related Quality of Life in Non-Hospitalized Coronavirus Disease 2019 (COVID-19) Cases with Confirmed Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in England: Longitudinal Analysis and Cross-Sectional Comparison With Controls. Clin. Infect. Dis. 2022, 75, e962–e973. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Diagnosis | Total Numbers | Incidence/100,000 Inhabitants | % Male/ Female | % ≤65/>65 Years Old | ICU Treatment | In-House Mortality |
|---|---|---|---|---|---|---|
| COVID-19 | 543,789 | 801.3 | 51.1/48.9 | 43.5/56.5 | 123,082 (22.6%) | 69,293 (12.7%) |
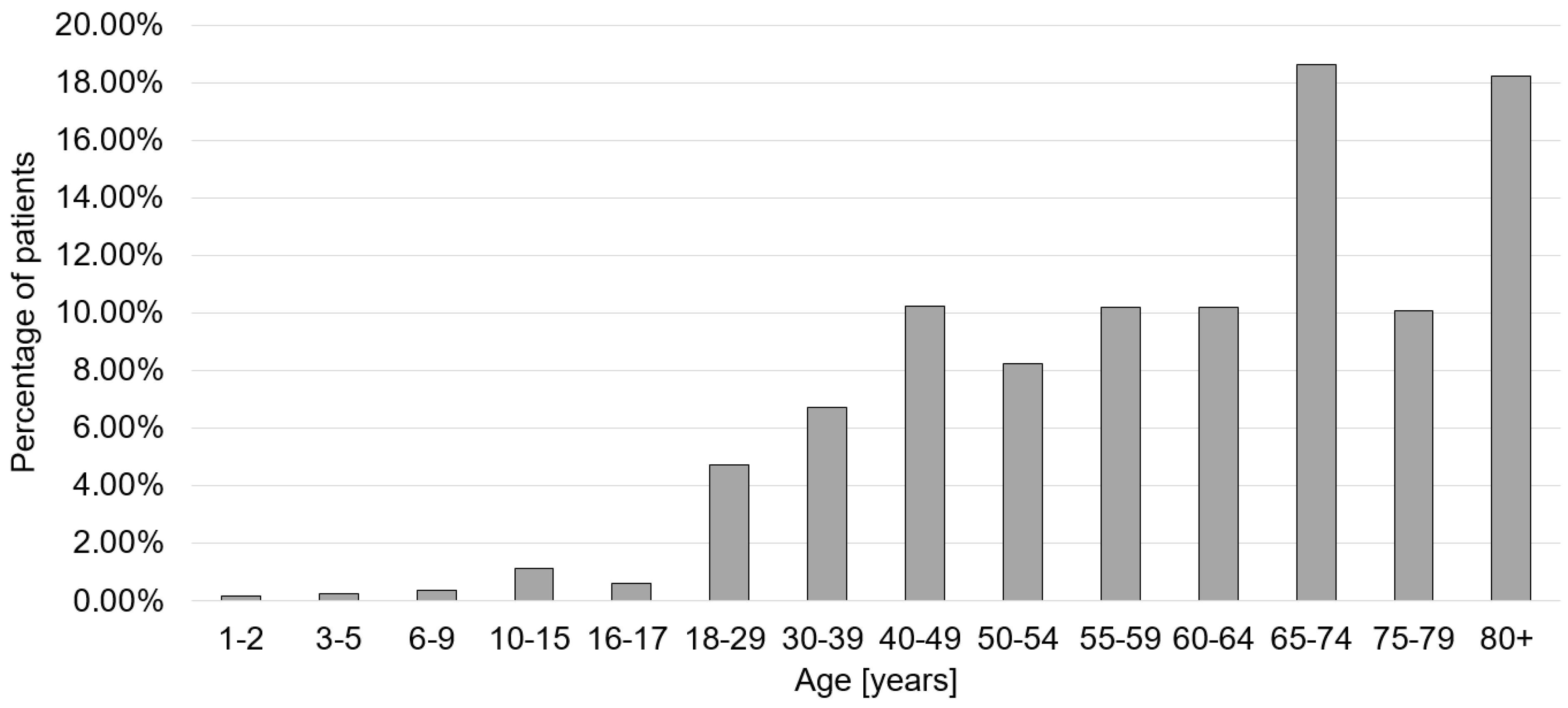
| Post-COVID | 29,808 | 43.9 | 51.8/48.2 | 53.1/46.9 | 5140 (17.2%) | 1330 (4.5%) |
| ICD-10 Code | Description | Number of Cases | Percentage |
|---|---|---|---|
| J12.8 | Pneumonia due to other viruses | 1771 | 5.94% |
| G62.80 | Critical-illness-Polyneuropathy | 1652 | 5.54% |
| R06.0 | Dyspnea | 1614 | 5.41% |
| G93.3 | Chronic fatigue syndrome | 703 | 2.36% |
| I26.9 | Pulmonary embolism without indication of acute cor pulmonale | 681 | 2.28% |
| J96.00 | Acute respiratory failure, not elsewhere classified: Type I (hypoxic) | 679 | 2.28% |
| J84.1 | Other interstitial lung disease with fibrosis | 494 | 1.66% |
| R53 | Malaise and fatigue | 492 | 1.65% |
| J96.10 | Chronic respiratory insufficiency, not elsewhere classified: Type I (hypoxic) | 393 | 1.32% |
| R26.8 | Other and unspecified disorders of gait and mobility | 351 | 1.18% |
| I50.14 | Left-sided heart failure: with symptoms at rest | 339 | 1.14% |
| I50.01 | Secondary right-sided heart failure | 328 | 1.10% |
| J18.9 | Pneumonia, unspecified | 276 | 0.93% |
| N39.0 | Urinary tract infection | 275 | 0.92% |
| I50.13 | Left-sided heart failure: with discomfort on mild exertion | 247 | 0.83% |
| J98.4 | Other changes in the lungs | 239 | 0.80% |
| J96.01 | Acute respiratory failure, not elsewhere classified: Type II (hypercapnic) | 236 | 0.79% |
| E86 | Volume deficiency | 229 | 0.77% |
| R07.3 | Other chest pain | 219 | 0.73% |
| J84.8 | Other interstitial lung disease not otherwise specified | 214 | 0.72% |
| J96.11 | Chronic respiratory insufficiency, not elsewhere classified: Type II (hypercapnic) | 204 | 0.68% |
| J18.8 | Other pneumonia, causative agent unspecified | 200 | 0.67% |
| R51 | Headache | 198 | 0.66% |
| J18.1 | Lobar pneumonia, unspecified | 197 | 0.66% |
| R07.4 | Chest pain, unspecified | 187 | 0.63% |
| F48.0 | Neurasthenia | 176 | 0.59% |
| I10.01 | Benign essential hypertension | 172 | 0.58% |
| J80.03 | Severe adult respiratory distress syndrome (ARDS). | 172 | 0.58% |
| G47.31 | Obstructive sleep apnoea syndrome | 167 | 0.56% |
| R42 | Immobility | 154 | 0.52% |
| CPT Code | Description | Number of Cases | Percentage |
|---|---|---|---|
| 3–222 | Computed tomography of the thorax with contrast medium | 5233 | 17.56% |
| 1–710 | Whole-body plethysmography | 4990 | 16.74% |
| 8–930 | Monitoring of respiration, heart, and circulation | 4968 | 16.67% |
| 3–990 | Computer-aided image data analysis with 3D evaluation | 4062 | 13.63% |
| 3–202 | Native computed tomography of the thorax | 3431 | 11.51% |
| 1–711 | Determination of CO diffusion capacity | 3329 | 11.17% |
| 3–200 | Native computed tomography of the skull | 3037 | 10.19% |
| 1–632.0 | Diagnostic esophagogastroduodenoscopy | 2379 | 7.98% |
| 1–620.00 | Diagnostic tracheobronchoscopy | 2118 | 7.11% |
| 3–225 | Computed tomography of the abdomen with contrast medium | 2043 | 6.85% |
| 8–831.0 | Placement of catheter in central venous vessels: | 1800 | 6.04% |
| 8–800.c0 | Whole blood transfusion, red blood cell concentrate, and platelet concentrate: Red blood cell concentrate: 1 TE to less than 6 TE | 1720 | 5.77% |
| 8–550.1 | Geriatric early rehabilitation complex treatment: at least 14 treatment days and 20 therapy units | 1554 | 5.21% |
| 1–620.01 | Diagnostic tracheobronchoscopy with bronchoalveolar lavage | 1518 | 5.09% |
| 1–207.0 | Electroencephalography | 1413 | 4.74% |
| 1–715 | Guyatt six-minute walk test | 1269 | 4.26% |
| 3–800 | Native magnetic resonance imaging of the skull | 1261 | 4.23% |
| 1–204.2 | Examination of the cerebrospinal fluid system: lumbar puncture for cerebrospinal fluid sampling | 1186 | 3.98% |
| 1–843 | Diagnostic aspiration from the bronchus | 1123 | 3.77% |
| 8–706 | Application of a mask for mechanical ventilation | 1089 | 3.65% |
| 1–206 | Neurography | 1075 | 3.61% |
| 9–320 | Therapy of organic and functional disorders of speech, language, voice, and swallowing | 978 | 3.28% |
| 3–052 | Transesophageal echocardiography (TEE) | 926 | 3.11% |
| 8–701 | Endotracheal intubation | 899 | 3.02% |
| 3–820 | Magnetic resonance imaging of the skull with contrast medium | 863 | 2.90% |
| G-DRG Code | Description | Number of Cases | Percentage | Mean Cost Per Case [Euro] | Standard Deviation [Euro] | Overall Costs [Euro] |
|---|---|---|---|---|---|---|
| E69C | Bronchitis and bronchial asthma, one day of occupancy or without extreme severe or severe CC or age < 56 years or respiratory complaints and symptoms or respiratory disorders with cause in the neonatal period, without certain extensive/highly extensive treatment | 1923 | 6.45% | 1192 | 476 | 2,292,216 |
| E79C | Infections and inflammations of the respiratory organs without complex diagnosis, without extremely serious CC or one day of occupancy, except in the case of para-/tetraplegia, without certain moderately complex treatments | 1534 | 5.15% | 1939 | 842 | 2,974,426 |
| Z65Z | Complaints, symptoms, other abnormalities, and aftercare | 1242 | 4.17% | 1483 | 752 | 1,841,886 |
| E64A | Respiratory failure, more than one day of occupancy, with extremely severe CC or pulmonary embolism | 814 | 2.73% | 2366 | 1153 | 1,925,924 |
| E74Z | Interstitial lung disease | 775 | 2.60% | 2070 | 1027 | 1,604,250 |
| E42Z | Geriatric early rehabilitative complex treatment for diseases and disorders of the respiratory organs | 725 | 2.43% | 4878 | 1418 | 3,536,550 |
| F62C | Heart failure and shock without severe CC or without dialysis, without complicated diagnosis, without complicated treatment | 636 | 2.13% | 2136 | 965 | 1,358,496 |
| E75C | Other diseases of the respiratory organs without extremely severe CC or respiratory complaints and symptoms with a complex diagnosis | 523 | 1.75% | 1633 | 740 | 854,059 |
| E64C | Respiratory failure, more than one day of occupancy, without extremely severe CC, age > 15 years. | 504 | 1.69% | 1846 | 964 | 930,384 |
| B43Z | Early rehabilitation for diseases and disorders of the nervous system, more than 27 days | 488 | 1.64% | 10,131 | 3359 | 4,943,928 |
| E63B | Sleep apnea syndrome or polysomnography or cardiorespiratory polygraphy, up to 2 days of occupancy, age > 17 years | 480 | 1.61% | 907 | 315 | 435,360 |
| B71D | Diseases of cranial nerves and peripheral nerves without complex diagnosis | 449 | 1.51% | 1693 | 878 | 760,157 |
| G67C | Esophagitis, gastroenteritis, gastrointestinal hemorrhage, ulcer disease, and various diseases of the digestive organs without specific or other complicating factors | 443 | 1.49% | 1284 | 522 | 568,812 |
| F71B | Nonsevere cardiac arrhythmia and conduction disorders | 439 | 1.47% | 1231 | 525 | 540,409 |
| F74Z | Thoracic pain and other unspecified diseases of the circulatory system | 421 | 1.41% | 1051 | 343 | 442,471 |
| A13H | Ventilation > 95 h with specific OR procedure or complicated constellation. | 376 | 1.26% | 7839 | 3112 | 2,947,464 |
| B81B | Other diseases of the nervous system without complex diagnosis | 345 | 1.16% | 1933 | 870 | 666,885 |
| E65C | Chronic obstructive pulmonary disease without extremely severe CC | 337 | 1.13% | 1780 | 798 | 599,860 |
| E41Z | Early rehabilitation for diseases and disorders of the respiratory organs | 316 | 1.06% | 8040 | 4134 | 2,540,640 |
| B77Z | Headache | 313 | 1.05% | 1467 | 572 | 459,171 |
| F75C | Other diseases of the circulatory system without extremely severe CC | 303 | 1.02% | 2087 | 1102 | 632,361 |
| F49G | Invasive cardiology diagnosis | 300 | 1.01% | 1804 | 648 | 541,200 |
| B42B | Early rehabilitation for diseases and disorders of the nervous system for up to 27 days without neurological complex treatment of acute stroke | 287 | 0.96% | 7913 | 2311 | 2,271,031 |
| K62C | Various metabolic diseases | 269 | 0.90% | 1581 | 773 | 425,289 |
| E40C | Diseases and disorders of the respiratory organs with ventilation > 24 h | 256 | 0.86% | 5243 | 2351 | 1,342,208 |
| B44B | Geriatric early rehabilitation complex treatment for diseases and disorders of the nervous system with other neurological complex treatment | 250 | 0.84% | 4948 | 1372 | 1,237,000 |
| L63E | Infections of the urinary organs | 236 | 0.79% | 1472 | 621 | 347,392 |
| F67C | Hypertension without complicating diagnosis | 227 | 0.76% | 1208 | 473 | 274,216 |
| A09F | Ventilation > 499 h | 225 | 0.75% | 27,472 | 8194 | 6,181,200 |
| B44C | Geriatric early rehabilitation complex treatment for diseases and disorders of the nervous system without complex treatment | 225 | 0.75% | 4262 | 972 | 958,950 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walter, N.; Rupp, M.; Lang, S.; Leinberger, B.; Alt, V.; Hinterberger, T.; Loew, T. A Comprehensive Report of German Nationwide Inpatient Data on the Post-COVID-19 Syndrome Including Annual Direct Healthcare Costs. Viruses 2022, 14, 2600. https://0-doi-org.brum.beds.ac.uk/10.3390/v14122600
Walter N, Rupp M, Lang S, Leinberger B, Alt V, Hinterberger T, Loew T. A Comprehensive Report of German Nationwide Inpatient Data on the Post-COVID-19 Syndrome Including Annual Direct Healthcare Costs. Viruses. 2022; 14(12):2600. https://0-doi-org.brum.beds.ac.uk/10.3390/v14122600
Chicago/Turabian StyleWalter, Nike, Markus Rupp, Siegmund Lang, Beate Leinberger, Volker Alt, Thilo Hinterberger, and Thomas Loew. 2022. "A Comprehensive Report of German Nationwide Inpatient Data on the Post-COVID-19 Syndrome Including Annual Direct Healthcare Costs" Viruses 14, no. 12: 2600. https://0-doi-org.brum.beds.ac.uk/10.3390/v14122600