
Hepatitis C Screening and Treatment Program in Hungarian Prisons in the Era of Direct Acting Antiviral Agents

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Screenings
2.2. Treatments
2.3. Data Collection
2.4. Ethics Committee Approval
3. Results
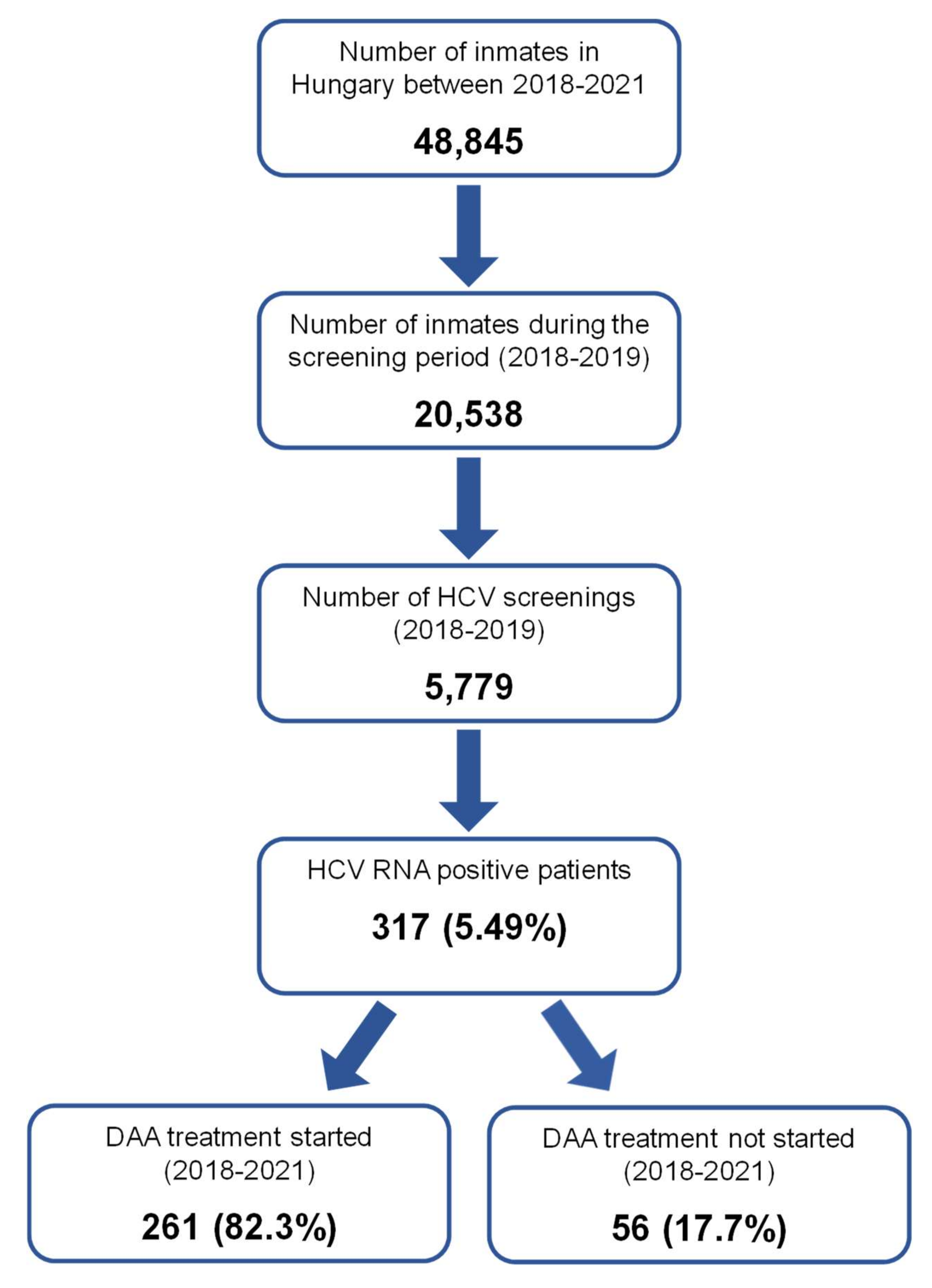
3.1. Screening Test Results
3.2. Patient Characteristics
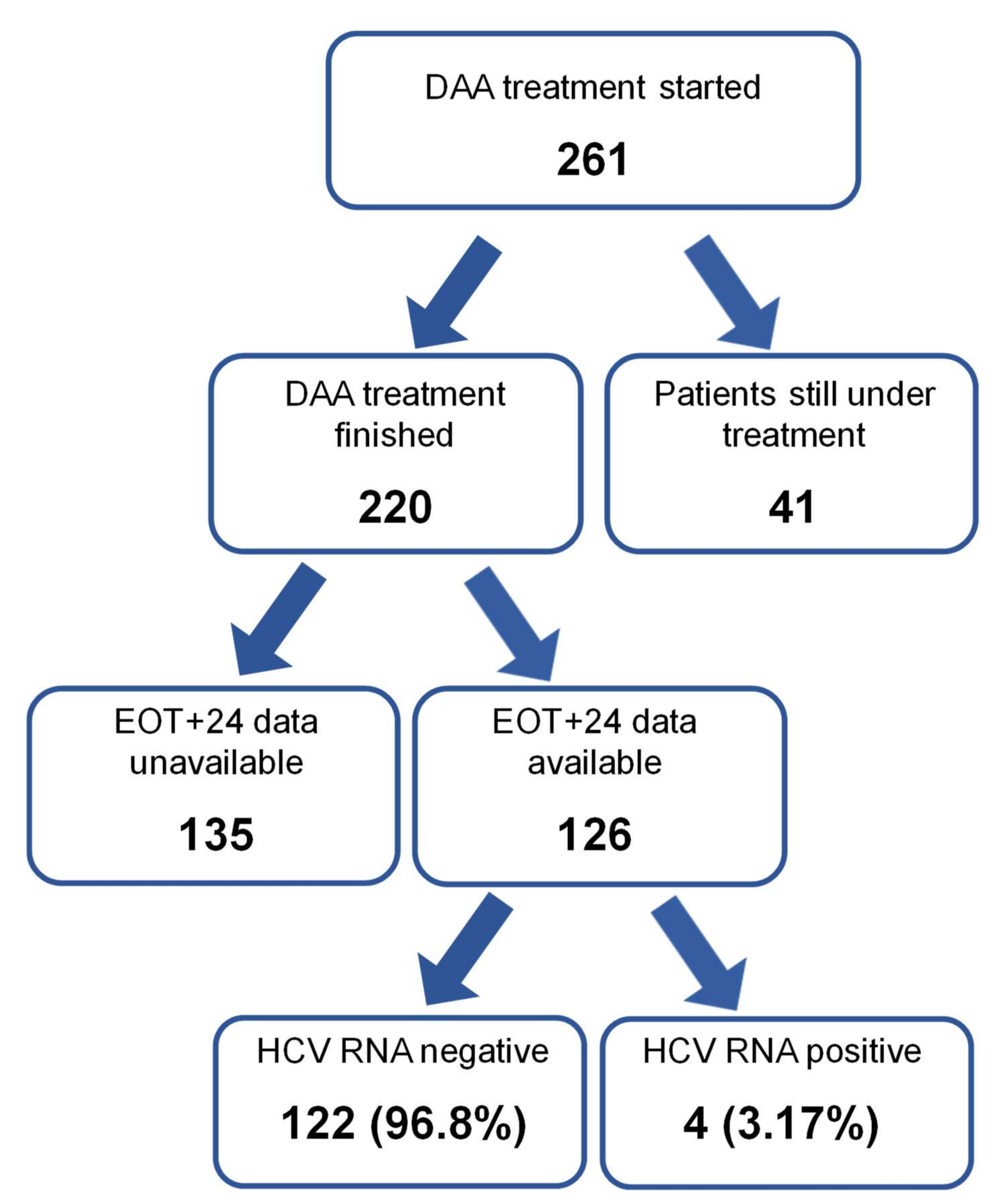
3.3. Treatment Outcome
3.4. Safety
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Alanine aminotransferase | (ALT) |
| Antibody | (Ab) |
| direct acting antiviral agent | (DAA) |
| hepatitis C virus | (HCV) |
| international normalized ratio | (INR) |
| intravenous | (iv.) |
| needle and syringe program | (NSP) |
| opioid substitution therapy | (OST) |
| pegylated interferon | (pegIFN) |
| person with intravenous drug use | (PWID) |
| polymerase chain reaction | (PCR) |
| ribavirin | (RBV) |
| ribonucleic acid | (RNA) |
| World Health Organization | (WHO). |
References
- Thrift, A.P.; El-Serag, H.B.; Kanwal, F. Global epidemiology and burden of HCV infection and HCV-related disease. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Hatzakis, A.; Cholongitas, E.; Baptista-Leite, R.; Baskozos, I.; Chhatwal, J.; Colombo, M.; Cortez-Pinto, H.; Craxi, A.; Goldberg, D.; et al. Hepatitis C: The beginning of the end-key elements for successful European and national strategies to eliminate HCV in Europe. J. Viral Hepat. 2018, 25, 6–17. [Google Scholar] [CrossRef] [PubMed]
- European Union HCV Collaborators. Hepatitis C virus prevalence and level of intervention required to achieve the WHO targets for elimination in the European Union by 2030: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 325–336. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. Available online: https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf (accessed on 20 December 2021).
- World Health Organization. Interim Guidance for Country Validation of Viral Hepatitis Elimination. 2021. Available online: https://www.who.int/publications/i/item/9789240028395 (accessed on 20 December 2021).
- Chen, C.P.; Cheng, C.Y.; Zou, H.; Cheng, C.H.; Cheng, S.H.; Chen, C.K.; Chen, C.H.; Bair, M.J. Evaluation of cost-effectiveness of peginterferon plus ribavirin for chronic hepatitis C treatment and direct-acting antiviral agents among HIV-infected patients in the prison and community settings. J. Microbiol. Immunol. Infect. 2019, 52, 556–562. [Google Scholar]
- Mason, L.M.K.; Duffel, E.; Veldhuijzen, I.K.; Petriti, U.; Bunge, E.M.; Tavoschi, L. Hepatitis B and C Prevalence and Incidence in Key Population Groups with Multiple Risk Factors in the EU/EEA: A Systematic Review. Euro. Surveill. 2019, 24, 1800614. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control, European Monitoring Centre for Drugs and Drug Addiction. Public Health Guidance on Active Case Finding of Communicable Diseases in Prison Settings. Stockholm and Lisbon: ECDC and EMCDDA. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Active-case-finding-communicable-diseases-in-prisons.pdf (accessed on 20 December 2021).
- Yang, T.H.; Fang, Y.-J.; Hsu, S.-J.; Lee, J.-Y.; Chiu, M.-C.; Yu, J.-J.; Kuo, C.-C.; Chen, C.-H. Microelimination of Chronic Hepatitis C by Universal Screening Plus Direct-Acting Antivirals for Incarcerated Persons in Taiwan. Open Forum Infect Dis. 2020, 7, 1–7. [Google Scholar] [CrossRef]
- Hariri, S.; Sharafi, H.; Sheikh, M.; Merat, S.; Hashemi, F.; Azimian, F.; Tamadoni, B.; Ramazani, R.; Gouya, M.M.; Abbasi, B.; et al. Continuum of Hepatitis C Care Cascade in Prison and Following Release in the Direct-Acting Antivirals Era. Harm Reduct. J. 2020, 17, 80. [Google Scholar] [CrossRef]
- Masarone, M.; Caruso, R.; Aglitti, A.; Izzo, C.; De Matteis, G.; Attianese, M.R.; Pagano, A.M.; Persico, M. Hepatitis C virus infection in jail: Difficult-to-reach, not to-treat. Results of a point-of-care screening and treatment program. Dig. Liver Dis. 2020, 52, 541–546. [Google Scholar]
- Makara, M.; Horváth, G.; Szalay, F.; Tornai, I.; Hunyady, B. Organizational characteristics of treatment for chronic hepatitis in Hungary: Hepatitis Registry and Priority Index. Orv. Hetil. 2013, 154, 1151–1155. (In Hungarian) [Google Scholar] [CrossRef] [Green Version]
- Hunyady, B.; Gerlei, Z.; Gervain, J.; Horváth, G.; Kiss, A.; Lengyel, G.; Pár, A.; Pár, G.; Péter, Z.; Rókusz, L.; et al. Screening, diagnosis, treatment, and follow up of hepatitis C virus infection. National consensus guideline in Hungary from 23 September 2020. Centr. Eur. J. Gastroenterol. Hepatol. 2021, 7, 7–21. (In Hungarian) [Google Scholar]
- Redman, J.S.; Sterling, R.K. Treating HCV in a Captive Audience: Eradication Efforts in the Prison Microenvironment. Am. J. Gastroenterol. 2018, 113, 1585–1587. [Google Scholar] [CrossRef] [PubMed]
- Negro, F. Epidemiology of hepatitis C in Europe. Dig. Liver Dis. 2014, 46, S158–S164. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.; Martin, N.K.; Hickman, M.; Hutchinson, S.J.; Aspinall, E.; Taylor, A.; Munro, A.; Dunleavy, K.; Peters, E.; Bramley, P.; et al. Modelling the impact of incarceration and prison-based hepatitis C virus (HCV) treatment on HCV transmission among people who inject drugs in Scotland: Modelling HCV prison-based interventions. Addiction 2017, 112, 1302–1314. [Google Scholar] [CrossRef] [PubMed]
- Bielen, R.; Stumo, S.R.; Halford, R.; Werling, K.; Reic, T.; Stöver, H.; Robaeys, G.; Lazarus, J.V. Harm reduction and viral hepatitis C in European prisons: A cross-sectional survey of 25 countries. Harm. Reduct. J. 2018, 15, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Aspinall, E.J.; Mitchell, W.; Schofield, J.; Cairns, A.; Lamond, S.; Bramley, P.; Peters, S.E.; Valerio, H.; Tomnay, J.; Goldberg, D.J.; et al. A matched comparison study of hepatitis C treatment outcomes in the prison and community setting, and an analysis of the impact of prison release or transfer during therapy. J. Viral Hepat. 2016, 23, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Hochstatter, K.R.; Stockman L., J.; Holzmacher, R.; Greer, J.; Seal, D.W.; Taylor, Q.A.; Gill, E.K.; Westergaard, R.P. The continuum of hepatitis C care for criminal justice involved adults in the DAA era: A retrospective cohort study demonstrating limited treatment uptake and inconsistent linkage to community-based care. Health Justice 2017, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuadrado, A.; Llerena, S.; Cobo, C.; Pallás, J.R.; Mateo, M.; Cabezas, J.; Fortea, J.I.; Alvarez, S.; Pellón, R.; Crespo, J.; et al. Microenvironment Eradication of Hepatitis C: A Novel Treatment Paradigm. Am. J. Gastroenterol. 2018, 113, 1639–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pontali, E.; Fiore, V.; Ialungo, A.M.; Ranieri, R.; Mollaretti, O.; Barbarini, G.; Marri, D.; Prestileo, T.; Dell’Isola, S.; Rastrelli, E.; et al. Treatment with direct-acting antivirals in a multicenter cohort of HCV-infected inmates in Italy. Int. J. Drug Policy 2018, 59, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, R.; Liberal, R.; Tavares, J.; Morgado, R.; Macedo, G. HIPPOCRATES® project: A proof of concept of a collaborative program for hepatitis C virus micro-elimination in a prison setting. World J. Hepatol. 2020, 12, 1314–1325. [Google Scholar] [CrossRef]
- Bhandari, R.; Morey, S.; Hamoodi, A.; Thompson, C.; Jones, D.; Hewett, M.; Hunter, E.; Taha, Y.; McPherson, S. High rate of hepatitis C reinfection following antiviral treatment in the North East England Prisons. Viral Hepat. 2020, 27, 449–452. [Google Scholar] [CrossRef]
- Tohme, R.A.; Holmberg, S.D. Transmission of Hepatitis C Virus Infection Through Tattooing and Piercing: A Critical Review. Clin. Infect. Dis. 2012, 54, 1167–1178. [Google Scholar] [CrossRef] [PubMed]
- Hellard, M.E.; Aitken, C.K.; Hocking, J.S. Tattooing in prisons—Not such a pretty picture. Am. J. Infect. Control. 2007, 35, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Poulin, C.; Courtemanche, Y.; Serhir, B.; Alary, M. Tattooing in prison: A risk factor for HCV infection among inmates in the Quebec’s provincial correctional system. Ann. Epidemiol. 2018, 28, 231–235. [Google Scholar] [CrossRef]
- Gervain, J. Analysis of hepatitis C virus type and subtype distribution in Hungary. Orv. Hetil. 2018, 159, 2–8. (In Hungarian) [Google Scholar] [CrossRef]
- Tresó, B.; Takács, M.; Dencs, Á.; Pár, A.; Rusvai, E. Molecular epidemiology of hepatitis C virus genotypes and subtypes among injecting drug users in Hungary. Eurosurveillance 2013, 18, 20639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazur, W.P. Management of Hepatitis C in Delaware Prisons. Del. J. Public Health 2019, 5, 20–27. [Google Scholar] [CrossRef]
- Palmateer, N.E.; McAuley, A.; Dillon, J.F.; McDonald, S.; Yeung, A.; Smith, S.; Barclay, S.; Hayes, P.; Shepherd, S.J.; Gunson, R.N.; et al. Reduction in the population prevalence of hepatitis C virus viraemia among people who inject drugs associated with scale-up of direct-acting anti-viral therapy in community drug services: Real-world data. Addict. Abingdon Engl. 2021, 116, 2893–2907. [Google Scholar] [CrossRef]
- Lim, A.G.; Stone, J.; Hajarizadeh, B.; Byrne, M.; Chambers, G.M.; Martin, N.K.; Grebely, J.; Dore, G.J.; Lloyd, A.R.; Vickerman, P. Evaluating the Prevention Benefit of HCV Treatment: Modeling the SToP-C Treatment as Prevention Study in Prisons. Hepatol. Baltim. Md. 2021, 74, 2366–2379. [Google Scholar] [CrossRef]
- Ocal, S.; Muir, A.J. Addressing Hepatitis C in the American Incarcerated Population: Strategies for Nationwide Elimination. Curr. HIV/AIDS Rep. 2020, 17, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Lau, G.K.K.; Wei, L.; Moriyama, M.; Yu, M.L.; Chuang, W.L.; Ibrahim, A.; Lesmana, C.R.A.; Sollano, J.; Kumar, M.; et al. APASL HCV guidelines of virus-eradicated patients by DAA on how to monitor HCC occurrence and HBV reactivation. Hepatol Int. 2019, 13, 649–661. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parameter | Data |
|---|---|
| Number of Patients Treated with DAA | 261 |
| Male/female, n/n | 220/41 |
| Age, median/mean (range), year, (number of available data) | 34/34.3 (17–64), (n = 261) |
| History of intravenous drug use, n (%), (number of available data) | 252 (99%), (n = 255) |
| ALT, median/mean (range), IU/L, (number of available data) | 74/94.0 (10–430), (n = 261) |
| AST, median/mean (range), IU/L, (number of available data) | 41/50.9 (12–189), (n = 261) |
| Serum bilirubin, median/mean, µmol/L, (number of available data) | 10/11.1 (2.2–29), (n = 261) * |
| Serum albumin, median/mean, g/L, (number of available data) | 47/46.7 (25.0–57.6), (n = 261) * |
| INR, median/mean, (number of available data) | 1.1/1.0 (0.8–1.5), (n = 261) |
| Hemoglobin, median/mean, g/L, (number of available data) | 155/153.6 (68–197), (n = 256) |
| Platelet count, median/mean, G/L, (number of available data) | 231/232.4 (73–497), (n = 256) |
| Absolute neutrophil cell count median/mean, G/L, (number of available data) | 4.2/4.5 (1.1–9.5), (n = 256) |
| Estimated glomerular filtration rate, median/mean, mL/min/1.73 m2, (number of available data) | 90/85.0 (6–137), (n = 201) * |
| Virus titer, median/mean (range), IU/L, (number of available data) | 160,583/1,286,636 (17–90,000,000), (n = 261) |
| Genotype distribution | |
| G1 with unknown subtype, n (%) | 10 (3.8%) |
| G1a, n (%) | 128 (49.0%) |
| G1b, n (%) | 93 (35.6%) |
| G1c, n (%) | 1 (0.4%) |
| G3, n (%) | 28 (10.7%) |
| G4, n (%) | 1 (0.4%) |
| FIB4 score median/mean (range), (number of available data) | 0.72/1.23 (0.24–35.28), (n = 261) |
| FIB4 < 1.45, n (%) | 232 (88.9%) |
| FIB4 1.45–3.25, n (%) | 25 (9.6%) |
| FIB4 > 3.25, n (%) | 4 (1.5%) |
| HBV coinfection, n, (number of available data) | 5 (n = 258) |
| HIV coinfection, n, (number of available data) | 0 (n = 245) |
| Status | Number of Patients |
|---|---|
| Naïve, n (%) | 219 (84.5%) |
| Partial responder, n (%) | 3 (1.1%) |
| Null responder, n (%) | 6 (2.3%) |
| Relapsed/re-infected, n (%) | 8 (3.1%) |
| Previous treatment suspended, n (%) | 25 (9.6%) |
| Reason | Number, n |
|---|---|
| Hepatocellular Carcinoma, n | 1 |
| Multiple hepatic metastases, n | 1 |
| Decompensation of non-hepatic disease, n | 1 |
| Passed away before treatment, n | 2 |
| COVID-19 pandemic-related, n | 1 |
| Refused treatment, n | 4 |
| Released or moved to another facility, n | 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werling, K.; Hunyady, B.; Makara, M.; Nemesi, K.; Horváth, G.; Schneider, F.; Enyedi, J.; Müller, Z.; Lesch, M.; Péterfi, Z.; et al. Hepatitis C Screening and Treatment Program in Hungarian Prisons in the Era of Direct Acting Antiviral Agents. Viruses 2022, 14, 308. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020308
Werling K, Hunyady B, Makara M, Nemesi K, Horváth G, Schneider F, Enyedi J, Müller Z, Lesch M, Péterfi Z, et al. Hepatitis C Screening and Treatment Program in Hungarian Prisons in the Era of Direct Acting Antiviral Agents. Viruses. 2022; 14(2):308. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020308
Chicago/Turabian StyleWerling, Klára, Béla Hunyady, Mihály Makara, Krisztina Nemesi, Gábor Horváth, Ferenc Schneider, Judit Enyedi, Zsófia Müller, Miklós Lesch, Zoltán Péterfi, and et al. 2022. "Hepatitis C Screening and Treatment Program in Hungarian Prisons in the Era of Direct Acting Antiviral Agents" Viruses 14, no. 2: 308. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020308