
Current Trend in Antiviral Therapy for Chronic Hepatitis B


Liver Research Unit, Chang Gung Memorial Hospital and University College of Medicine, 199 Tung Hwa North Road, Taipei 105, Taiwan
*
Authors to whom correspondence should be addressed.
Viruses 2022, 14(2), 434; https://0-doi-org.brum.beds.ac.uk/10.3390/v14020434
Submission received: 12 January 2022
/
Revised: 13 February 2022
/
Accepted: 16 February 2022
/
Published: 21 February 2022
(This article belongs to the Special Issue State-of-the-Art Chronic Hepatitis Viruses Research in Asia)
Abstract
:Since active hepatitis B virus (HBV) replication is the key driver of hepatic necroinflammation and disease progression, the treatment aim of chronic hepatitis B (CHB) is to suppress HBV replication permanently to prevent hepatic decompensation, liver cirrhosis and/or hepatocellular carcinoma and prolong survival. Currently, pegylated interferon (Peg-IFN), entecavir (ETV), tenofovir disoproxil fumarate (TDF) and tenofovir alafenamide (TAF) are the first-line drugs of choice. Peg-IFN therapy has been used rarely due to its subcutaneous injection and significant side effect profile. Once daily oral ETV, TDF and TAF can suppress HBV DNA profoundly but have no direct action on cccDNA of the HBV-infected hepatocytes, hence continuing long-term therapy is usually needed to maintain HBV suppression, but the ultimate goal of HBsAg loss was rarely achieved (10 year 2%). In addition, long-term NUC therapy comes with several concerns such as increasing cost, medication adherence and loss-to-follow-up. Studies, mainly from Taiwan, have shown that finite NUCs therapy of two to three years in HBeAg-negative patients is feasible, safe and has a great benefit of much increasing HBsAg loss rate up to 30%/5 year. These have led an emerging paradigm shift to finite NUC therapy in HBeAg-negative patients globally. However, off-NUC relapse with hepatitis B flares may occur and have a risk of decompensation or even life-threatening outcomes. Therefore, proper monitoring, assessment, and retreatment decisions are crucial to ensure safety. Ideally, retreatment should be not too late to ensure safety and also not too early to allow further immune response for further HBsAg decline toward HBsAg loss. Assessment using combined HBsAg/ALT kinetics during hepatitis flare is better than biochemical markers alone to make a right retreatment decision. The strategy of finite NUC therapy has set a benchmark of high HBsAg loss rate to be achieved by the new anti-HBV drugs which are under preclinical or early phase study.
1. Introduction
Chronic infection with Hepatitis B virus (HBV) is a major global health problem, an important cause of morbidity and mortality sequelae such as hepatic decompensation, liver cirrhosis (LC) and/or hepatocellular carcinoma (HCC) development [1]. It affects ~290 million people worldwide; 64% of them reside in the Asia Pacific region, and approximately 2 billion people have been infected worldwide and about 1 million die from it annually [2]. In the past decades, basic and clinical studies have provided a better understanding of the virus, its natural history and the immunopathogenesis of chronic HBV infection [1,2,3]. Furthermore, primary prevention of HCC by universal HBV vaccination program was conducted globally and was successful in achieving declining HBV infection rates [3,4]. In addition, treatment of patients with chronic Hepatitis B (CHB) has been evolving rapidly in the past decades, with an increasing range of treatment options and the availability of multiple antiviral agents [2,3,5]. The long-term goal of antiviral therapy has partly achieved by effectively reducing the incidence of HCC development [6]; however, the existing antiviral therapy is still far from satisfactory now that new strategies and/or new drugs are emerging. This review aims to assess and discuss current and evolving trends in the antiviral therapy of chronic HBV infection.
2. Natural History and Treatment Considerations
Chronic HBV infection is a dynamic process of the interactions between HBV and host immune response on hepatocytes. The hepatitis activity with the rising of serum alanine aminotransferase (ALT) is reflecting the host endogenous immune ability against HBV. The classical natural course of chronic HBV infection is divided into the immune tolerance phase (high levels of HBsAg quantification [qHBsAg], seropositive for Hepatitis B e antigen [HBeAg], high levels of serum HBV DNA, normal ALT and minimal hepatic histological changes), the immune clearance phase (declining levels of qHBsAg, HBeAg seropositive, declining levels of serum HBV DNA, fluctuation of ALT and increased hepatic lobular and/or periportal activity), and followed by HBeAg seroconversion to the residual integration phase (lower levels of qHBsAg, seropositive for antibody against HBeAg [anti-HBe], lower levels of serum HBV DNA, normal ALT and minimal hepatic histological activity [7], which may reactive to HBeAg-negative CHB (reactive phase: HBeAg-negative, elevated ALT with increased hepatitis activity and higher HBV DNA level) [1]. The severity, extent, duration and frequency of hepatic lobular alterations during hepatitis flares are determinants of disease progression (LC and/or HCC), remission or clearance of HBV antigens [1].
Obviously, active HBV replication is the key driver leading to hepatic necroinflammation and disease progression. Therefore, HBeAg-positive and HBeAg-negative patients with CHB are candidates of anti-HBV therapy with an aim of permanent suppression of HBV replication. The short-term goal of treatment is profound HBV DNA suppression, ALT normalization, the prevention of hepatic decompensation and the achievement of HBeAg seroconversion in HBeAg-positive patients. The long-term goal of therapy is to prevent hepatic decompensation, reduce progression to LC and/or HCC and prolong survival [8]. The ultimate goal of antiviral therapy is HBsAg loss, considered as a functional cure, with or without seroconversion to its antibody (anti-HBs).
3. Currently Available Antivirals
Currently, two subcutaneous interferon (IFN)-based drugs and seven oral nucleos(t)ide analogues (NUC) have been approved for the treatment of CHB. Lamivudine (LAM), adefovir (ADV) and telbivudine (LdT) have been rendered almost obsolete because of issues of drug resistance, whereas entecavir (ETV), tenofovir disoproxil fumarate (TDF), tenofovir alafenamide (TAF) and pegylated interferon (Peg-IFN) are the first-line drugs of choice for anti-HBV therapy [5,9,10,11].
3.1. IFN-Based Therapy
Peg-IFN has the benefit of both antiviral and immunomodulatory effects after a finite course of therapy in HBeAg-positive and -negative CHB patients. Studies showed that HBeAg-positive CHB patients treated with subcutaneous Peg-IFN 180 μg per week for 48 weeks achieved ALT normalization in 41%, HBeAg seroconversion with HBV DNA <400 copies/mL in 32% and HBsAg seroconversion in 3%, assessed at 24 weeks post-treatment [12]. The responses of Peg-IFN therapy at shorter duration (24 weeks) and/or lower weekly dose (90 μg) were inferior to the recommended 180 μg/week for 48 weeks regimen [13]. In addition, a mean three years interval follow-up study in those HBeAg-seropositive patients after 52 weeks Peg-IFN ± LAM treatment has revealed that 81% of those initial HBeAg loss had sustained its response and 27% of those initial HBeAg non-responders had achieved delayed HBeAg loss. Of note is that 30% of the initial responders or 11% of overall patients achieved HBsAg loss thereafter [14]. Wong et al. further reported the durability at five years post-therapy, showing 69% of the initial HBeAg non-responders followed by delayed HBeAg seroconversion with a 60% overall HBeAg seroconversion rate [15]. Concerning HBeAg-negative CHB patients, the phase III global trial have demonstrated that ALT normalization, HBV DNA <20,000 copies/mL, HBV DNA <400 copies/mL and HBsAg loss were 59%, 43%, 19% and 3%, respectively, after six months post-treatment (Peg-IFN therapy at 180 μg/week for 48 weeks) assessment [16]. Upon long-term follow-up, 31% and 23% of patients treated with 1-year Peg-IFN ± LAM achieved HBV DNA <2000 IU/mL at 1- and 5-years post-therapy, respectively, and HBsAg loss in 5% and 12% at one and five years post-therapy, respectively [17].
3.2. NUCs Therapy
3.2.1. Entecavir
ETV, a cyclopentyl guanosine analogue, is a potent inhibition of the HBV polymerase, achieving a mean 6.9 log decline of serum HBV DNA. An international collaborative ETV treatment in HBeAg-positive patients showed a five-year cumulative probability of HBV DNA < 300 copies/mL of 94% [18]. Another report from Hong Kong involving 222 treatment-naïve patients treated with five-year ETV showed undetectable HBV DNA in 97%, achieving HBeAg seroconversion in 66.9% and HBsAg loss in one patient [19]. Other studies also demonstrated undetectable HBV DNA of 83–90%, and HBeAg seroconversion of 24–44% at year three of treatment [20,21,22]. But HBsAg loss was rare, and this was reported in only 0–1.4% of HBeAg-positive patients after three to five years of ETV therapy [20,21]. In addition, improvement of hepatic activity and fibrosis could be achieved after continuous ETV treatment [23]. However, Papatheodoris et al. had demonstrated that the calculated HBsAg decline is only 0.09 log IU/mL per year, which explains why long-term therapy is needed and the HBsAg loss rate in ETV-treated patients is low [24]. Paired histologic studies showed fibrosis regression and cirrhosis remission in 85% and 100%, respectively, of patients after 3–7 years ETV therapy [23,25]. Compared with historical untreated controls among patients with or without liver cirrhosis, several long-term cohort studies from Asia have demonstrated that ETV-treated patients could reduce the incidence of liver related complications and improve their survival [26,27,28]. Moreover, a multicenter collaborative study from Taiwan also showed a significant reduction in the risk of cirrhotic complications, HCC and mortality in patients with HBV-related cirrhosis after four-year ETV therapy [29].
3.2.2. Tenofovir Disoproxil Fumarate
TDF is an acyclic adenine nucleotide analogue effective for both HBV and human immune deficiency virus (HIV). In a phase III randomized trial, TDF 300 mg daily, compared to ADV 10 mg daily, has been shown to have superior HBV DNA suppression in both HBeAg-positive and HBeAg-negative patients [30]. TDF treatment for seven years achieved undetectable HBV DNA in 99.3%, ALT normalization in 80%, HBeAg loss of 54.5% and HBsAg loss in 11.8% of patients with HBeAg loss [31]. In HBeAg-negative patients, the calculated HBsAg decline was only −0.09 log10 IU/mL [32] and only one (0.3%) of 375 patients was reported to achieve HBsAg loss after seven years TDF therapy [31]. More importantly, Marcellin et al. had reported that 74% of cirrhotic patients showed regression of liver cirrhosis and 87% of patients improved histological activity of liver on paired liver biopsy at five years, [33]. Based on the REACH-B risk calculator, Kim et al. showed a reduced incidence of HCC after TDF long-term therapy among patients without cirrhosis [34].
3.2.3. Tenofovir Alafenamide
Recently, a small molecular weight oral prodrug of tenofovir, TAF, has been approved for the treatment of chronic HBV infection to replace long-term TDF therapy because of some concerns with regard to renal injury and decreased bone mineral density. Compared to a 300 mg dose of TDF administration, a 25 mg dose of TAF has showed more than 90% lower systemic tenofovir concentration and higher intracellular concentration during pharmacokinetic study [35]. A randomized, double-blind non-inferior trial in both HBeAg-positive and HBeAg-negative patients receiving TAF or TDF therapy have demonstrated similar rates of achieving an HBV DNA levels <29 IU/mL at week 48 [36,37]. However, using AASLD ALT normal criteria (male: ALT ≤ 30 U/L and female: ALT ≤ 19 U/L), TAF is associated with higher rate of ALT normalization than TDF (p < 0.05) [37]. Concerning the renal safety using the estimated glomerular filtration rate (eGFR) analysis, patients with TAF had a smaller reduction than those with TDF therapy. In comparison with decreased in bone mineral density at the hip and spine, patients with TAF also showed smaller than those with TDF therapy significantly in both HBeAg-positive and HBeAg-negative patients [36,37].
4. Problems of Current Therapy
4.1. IFN-Based Therapy
Although it is recommended as one of the first line treatments by all therapeutic guidelines, it has been limited by its subcutaneous injection, poor tolerability and significant side effect profile. In addition, it is also contraindicated in patients with hepatic decompensation, immunosuppressed states, major comorbid diseases, and pregnancy. Hence, Peg-IFN has been used in only <5% of the real world patients and is only preferred by young patients who wish to have children in the near future and those who refuse long-term NUCs treatment.
4.2. NUCs Therapy
Since NUCs can suppress HBV DNA profoundly but have no direct action on cccDNA of the HBV-infected hepatocytes, the indefinite continuation of long-term NUCs therapy is usually necessary to maintain a virological response [5,9,10,11]. A mathematic modelling study has estimated that three to four decades of continuous NUC therapy would be needed to achieve a functional cure [38]. However, several concerns and disadvantages of life-long NUC therapy have emerged and been extensively discussed [39], as summarized in the following subsections.
4.2.1. Ultimate Goal of HBsAg Loss Rarely Achieved
A large multinational multicenter long-term ETV/TDF therapy cohort study in 4769 patients demonstrated a 10-year HBsAg loss rate of 2.1% and an annual incidence of only 0.22% [40].
4.2.2. Cost and Drug-Resistance Issues
Earlier reports of low genetic barrier NUCs therapy such as LAM, ADV or LdT, showed that resistance mutants may emerge [5], and may cause hepatitis, hepatitis flare, and even life-threatening hepatic decompensation [41]. In addition, peoples from resource limited countries or regions such as Asia could not afford the financial burden of long-term NUC therapy [42].
4.2.3. Adherence and Other Additional Concerns
Even though ETV, TDF or TAF shows a high genetic barrier, and drug resistance is no longer a concern during monotherapy, drug adherence and compliance issues are emerging concerns to a physician [43]. Ford et al. performed a systematic review involving 30 studies with meta-analysis [44], and had showed an overall adherence of 74.6%, which is far from the optimal adherence of 95%. Another important study by Shin et al. from Korea involving 894 patients further showed patients with poor adherence (<70%) in 10.5% and moderate adherence (70–90%) in 20.5% during 5-year ETV therapy, respectively. More important is that such patients showed increased incidence of cirrhotic complications, HCC, and mortality significantly in a dose-dependent manner [45]. Furthermore, Ahn et al. also demonstrated that 7.3% of 658 patients (Asians: 83.3%) stopped therapy by themselves or were lost to follow-up during a five-year ETV study [46]. It is very clear, without off-therapy monitoring, that such patients may encounter some risk of severe ALT relapse, hepatic decompensation, even hepatic failure and mortality [47].
Together with the financial issue, these human nature related inevitable problems may get worse upon longer duration of therapy. In addition, the safety issues of NUC therapy beyond 10 years are largely unknown and is also one of the concerns.
5. Current Trend of NUC Therapy
5.1. Finite NUC Therapy
All guidelines of major liver association have recommended that NUC therapy in HBeAg-positive CHB can be stopped after HBeAg loss with undetectable HBV DNA and consolidation therapy >12 months [9,10,11]. Along this line and against other guidelines, the APASL guidelines recommended to consider stopping NUC therapy in HBeAg-negative patients after treatment of at least two years with undetectable HBV DNA documented on three separate occasions each >6 months apart (total >12 months) with off-therapy ALT monitoring monthly in the first three months and then every three months along with an HBV DNA assay, the so called APASL stopping rule [8] Planned NUCs cessation in HBeAg-negative patients with maintained HBV suppression over one to three years may encounter virologic relapse (VR: HBV DNA > 2000 IU/mL), which may coincide with or be followed by clinical relapse (CR: VR + ALT > 2 × ULN) and hepatitis flare (ALT > 5 × ULN). The one-year rate of hepatitis flare was around 36% and the rate of ALT > 10 × ULN was around 21% in small studies (<100 patients) [39]. Our large study involving 691 patients (308 with cirrhosis), so far the largest on this issue, showed clinical relapse in 419 (61%), hepatitis flare (ALT > 5 × ULN) in 280 (41%), total bilirubin >2 mg/dL in 72 (10%), prolongation of prothrombin time with international normalized ratio (INR) > 1.5 in 16 (2%) during a median follow-up of three years after end-of-treatment (EOT), and the calculated annular incidence of hepatic decompensation was 0.28%, with a five-year cumulative incidence of 0% in 383 patients with CHB and 2.95% in 308 patients with cirrhosis, during a median follow-up of 155 (2–614) weeks [48]. These studies have shown that finite NUC therapy in HBeAg-negative patients is feasible and reasonably safe, even in patients with cirrhosis [39].
Of note is that earlier report by Hadziyannis et al. [49] that demonstrated ALT flares in 25 (76%) of the 33 patients after cessation of four-to-five-year ADV treatment with a 39% of HBsAg loss rate subsequently during a 5.5 year follow-up. Also noteworthy is that “no-retreatment “is the most important determinant for HBsAg loss. Furthermore, Honer zu Siederdissen C et al. [50] has reported a 20% HBsAg loss rate after discontinuation of NUC treatment in HBeAg-negative CHB patients during a median of 33 months follow-up. Recently, Berg et al. reported an important result of a randomized controlled trial (FINITE study). It showed HBsAg loss in 19% within three-years after cessation of TDF therapy in comparison to 0% in those who continued TDF treatment [51]. Although this is a small number study, it has provided a meaningful data of well controlled head-to-head comparison, and further confirms the pivotal findings of Hadziyannis et al. [49] that discontinuation of NUC therapy in HBeAg-negative patients with HBV DNA suppression may subsequently increase HBsAg loss rate. In addition, there were several reports worldwide showing higher HBsAg loss rate after finite NUC treatment [52,53,54,55], as summarized in Table 1. We also reported a large-scale study involving 691 HBeAg-negative patients and demonstrated that the incidence of HBsAg loss was highest in patients with sustained response (6-year: 36%) off-NUC treatment. It is worth to note that patients with clinical relapse but were not retreated had a 7.34 times higher incidence of HBsAg loss than those who received retreatment (six-year: 19% vs. 1%), confirming that “no-retreatment” is an important factor for HBsAg loss [48], as compared in Table 2. The strategy of finite NUC therapy in HBeAg-negative patients has been increasingly accepted by non-APASL countries since 2016 [10,11]. Clearly, a paradigm shift from indefinite long-term/life-long NUC therapy to finite therapy in HBeAg-negative patients is emerging [39]. European experts even consider that the strategy of finite therapy is not only an option but also becoming a more specific recommendation in future guidelines [56].
5.2. Off-Therapy Management and Re-Treatment Decision
Although finite NUC therapy in HBeAg-negative patients may minimize the concerns/problems of indefinite long-term therapy and much increased HBsAg loss, CR may occur in about 60% and hepatitis flare in 40% of HBeAg-negative patients after cessation of NUC therapy, and may sometimes deteriorate to hepatic decompensation and even death [48,55]. Hence, off-therapy monitoring is of paramount importance, and timely retreatment is required in some patients with hepatitis flare to prevent hepatic decompensation. It is therefore pertinent to follow the patients with rising ALT or ALT > 5 × ULN either weekly or biweekly with assays of ALT, bilirubin and INR to detect hepatic decompensation and start treatment/retreatment in time to ensure safety [57]. Given that “no-retreatment” is an important determinant for subsequent HBsAg loss [48,49], this monitoring plan can avoid unnecessary retreatment [58]. Therefore, the decision of retreatment is crucial for the best result of finite NUC therapy. Ideally, it should be not too late to prevent/rescue hepatic decompensation and not too early to allow further HBsAg decline toward HBsAg loss [39].
5.2.1. Biochemical Markers for Retreatment Decision
In principle, the indications of retreatment are similar to the indications of treatment for treatment-naïve patients, such as viremic patients with persistent/intermittent ALT elevation >3 months [9,10,11]. However, patients with hepatitis flare are at risk of hepatic decompensation and hence require special consideration. Various biochemical criteria have been applied in studies on off-NUC retreatment [51,59,60,61], as shown in Table 3. Retreatment decisions by these criteria determined at one single time point may include patients destined to have spontaneous beneficial outcomes. In contrast, retreatment decisions by criteria determined at time points >four weeks apart may be too late to detect deterioration for timely retreatment [58]. It seems that biochemical markers are still not ideal for optimal retreatment decisions.
5.2.2. Combined HBsAg/ALT Kinetics for Retreatment Decision
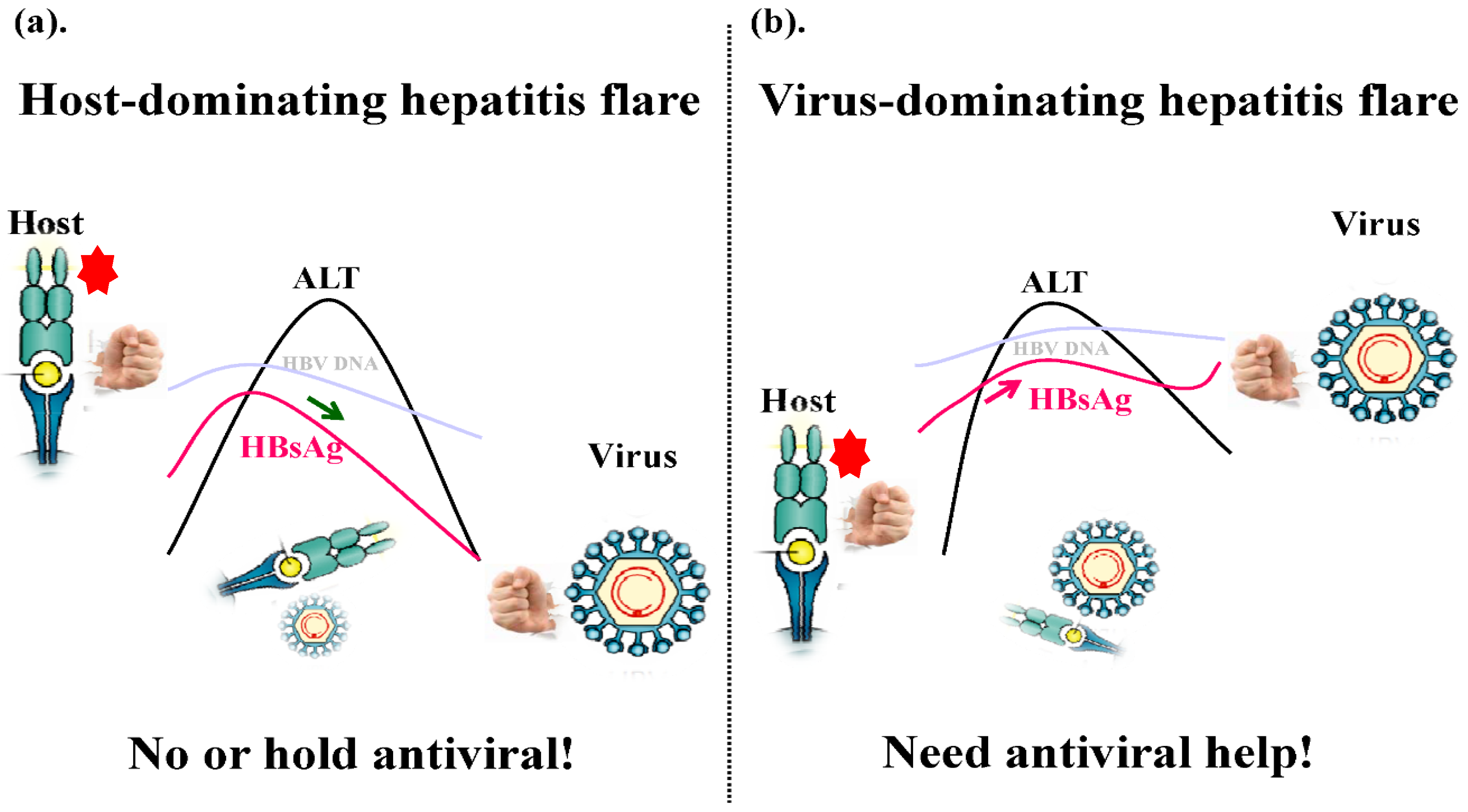
The quantitative HBsAg (qHBsAg) has been considered as a surrogate marker of transcriptionally active cccDNA or a marker of HBV-infected hepatocytes, and sensitive and reproducible qHBsAg assays have been available commercially and used widely in clinical practice and research [62]. Along with HBV DNA levels, serum HBsAg levels also upsurge prior to ALT elevation to its peak but may start to decline successively prior to the peak of ascending ALT in some hepatitis flares, which may resolve spontaneously [57]. Hepatitis flares with such a profile of combined HBsAg/ALT kinetics may reflect that the host immune response is dominating over the virus and the effective immune clearance of HBV is ongoing (host-dominating flare; HDF) (Figure 1a). In contrast, flares with qHBsAg increasing along with ascending ALT or remaining high after the peak of ALT may reflect that the virus is dominating over the host and the immune response is failing or being ineffective (virus-dominating flare; VDF) (Figure 1b) [58]. A proof-of-concept case study has shown that retreatment may be unnecessary or can be held in a patient with HDF, whereas timely retreatment was required for a patient with VDF [63]. This has been further confirmed by another study involving 48 patients who remained un-retreated, of whom five patients with off-NUC hepatitis flare have demonstrated off-NUC qHBsAg kinetics from EOT to HBsAg loss [64]. Furthermore, a retrospective appraisal study conducted by us using pre-retreatment combined HBsAg/ALT kinetics in 22 patients with off-NUC severe ALT flare (ALT > 30 × ULN), showing much greater and faster HBsAg decline (>1–3 log10 IU/mL decline in 12 months) during NUC retreatment in patients with VDF (bad flare but good response to NUC therapy), in contrast to minimal HBsAg decline or even HBsAg increase or rebound in patients with HDF (good flare but bad response to NUC therapy) [65]. An extension study using retrospective appraisal in 220 patients with off-NUC flare has further demonstrated that retreatment in patients with VDF achieved 1-year HBsAg decline of −0.91 log10 IU/mL in contrast to a decline of −0.07 log10 IU/mL in patients with HDF, while un-retreated patients with HDF showed greater HBsAg decline and a three-year HBsAg loss rate >20% (Jeng and Liaw, 2021, unpublished data). It is conceivable that patients with off-NUC VDF do need timely NUC retreatment to prevent severe ALT flare and help their ineffective immune response to fight the virus. In contrast, patients with off-NUC HDF which may overcome HBV and lead to further HBsAg decline and NUC retreatment should be withheld because it may halt or interrupt the strong endogenous immune clearance response of host. [66].
6. Conclusions and Perspective
Most real-world CHB patients preferred NUCs therapy. It is estimated that >90–95% of the patients were treated with NUCs. Most importantly, a paradigm shift from indefinite long-term or even lifelong to finite NUC therapy has been emerging globally. To identify the factors that can reliably predict the outcomes of CHB patients who stop NUCs therapy is quite important. Unfortunately, although there have been many studies trying to identify predictors of post-NUC events, accurate predictors have not been reliably identified [67]. So far, the best predictor is EOT qHBsAg <100 IU/mL, which showed a significantly lower relapse rate and higher probability of HBsAg loss after NUC discontinuation [48,68].
Proper monitoring is of paramount importance to ensure off-NUC safety. Patients with impending or overt hepatic decompensation definitely require immediate retreatment. Otherwise, “no retreatment” is an important determinant for off-NUC HBsAg loss. Hence, how to assess patients and decide whether to retreat or not are crucial in the strategy of finite NUC therapy. Of note is that patients with hepatitis flare with normal serum bilirubin and prothrombin time, a decision based on current biochemical markers, is not ideal, whereas combined HBsAg/ALT kinetics may help differentiate flares that need timely retreatment from those retreatment that can be held off or even deemed to be unnecessary.
Finally, the development of new drugs that target different steps of the HBV life cycle, such as entry inhibitors, targeting cccDNAs, capsid inhibitors, or HBsAg excretion blockers, and focusing on improving host innate immunity such as lymphotoxin-B receptor agonist or Toll-like receptor agonist; or improving host adaptive immunity such as therapeutic vaccine or immune checkpoint inhibitors, is strongly anticipated. Most of the investigation agents are still in the preclinical or early phases of study. The strategy of finite NUC therapy has set a benchmark of high HBsAg loss rate. To be applicable, future drugs have to achieve an even higher HBsAg loss rate.
Author Contributions
Conceptualization, Y.-F.L. and R.-N.C.; writing—original draft preparation, R.-N.C.; writing—review and editing, Y.-F.L.; visualization, R.-N.C.; supervision, Y.-F.L.; funding acquisition, Y.-F.L. and R.-N.C. All authors have read and agreed to the published version of the manuscript.
Funding
The author has been supported by grants from Chang Gung Medical Research Fund (CMRPG1K0101, CMRPG1K0111), Ministry of Science and Technology, Taiwan (MOST109-2314-B-182A-063) and the Prosperous Foundation, Taipei, Taiwan.
Acknowledgments
The authors thank Su-Chiung Chu for secretary assistance and preparation of the manuscript and figures.
Conflicts of Interest
The authors have no financial or personal relationships with other people or organizations that could inappropriately influence the work.
Abbreviations
ADV: adefovir; ALT: alanine aminotransferase; CHB: chronic hepatitis B; CR: clinical relapse; eGFR: estimated glomerular filtration rate; EOT: end-of-treatment; ETV: entecavir; HBV: hepatitis B virus; HBeAg: hepatitis B e antigen; HCC: hepatocellular carcinoma; HDF: host-dominating flare; HIV: human immunodeficiency virus; IFN: interferon; INR: international normalized ratio; LAM: Lamivudine; LC: liver cirrhosis; LdT: telbividine; NUC: nucleos(t)ide analogues; Peg-IFN: pegylated interferon; qHBsAg: quantitative HBsAg; TAF: tenofovir alafenamide; TDF: tenofovir disoproxil fumarate; VDF: virus-dominating flare; VR: virologic relapse.
References
- Liaw, Y.F.; Chu, C.M. Hepatitis B virus infection. Lancet 2009, 373, 582–592. [Google Scholar] [CrossRef]
- Polaris Observatory Collaborators. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar] [CrossRef]
- Maini, M.K.; Burton, A.R. Restoring, releasing or replacing adaptive immunity in chronic hepatitis B. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 662–675. [Google Scholar] [CrossRef] [PubMed]
- Mastrodomenico, M.; Muselli, M.; Provvidenti, L.; Scatigna, M.; Bianchi, S.; Fabian, L. Long-term immune protection against HBV: Associated factors and determinants. Hum. Vaccines Immunother. 2021, 17, 2268–2272. [Google Scholar] [CrossRef]
- Chien, R.N.; Kao, J.H.; Peng, C.Y.; Chen, C.H.; Liu, C.J.; Huang, Y.H.; Hu, T.H.; Yang, H.-I.; Lu, S.-N.; Liaw, Y.F.; et al. Taiwan consensus statement on the management of chronic hepatitis B. J. Formos. Med. Assoc. 2019, 118, 7–38. [Google Scholar] [CrossRef]
- Tseng, C.H.; Hsu, Y.C.; Chen, T.H.; Ji, F.; Chen, I.S.; Tsai, Y.N.; Hai, H.; Thanh Thuy, L.T.; Hosaka, T.; Nguyen, M.H.; et al. Hepatocellular carcinoma incidence with tenofovir versus entecavir in chronic hepatitis B: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1039–1053. [Google Scholar] [CrossRef]
- Chu, C.M.; Karayiannis, P.; Fowler, M.J.F.; Monjardino, J.; Liaw, Y.F.; Thomas, H.C. Natural history of chronic hepatitis B virus infection in Taiwan: Studies of hepatitis B virus DNA in serum. Hepatology 1985, 5, 431–434. [Google Scholar] [CrossRef]
- Liaw, Y.F.; Kao, J.H.; Piratvisuth, T.; Chan, H.L.Y.; Chien, R.N.; Liu, C.J.; Gane, E.; Locarnini, S.; Lim, S.G.; Han, K.H.; et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2012 update. Hepatol. Int. 2012, 6, 531–561. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.P.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.-S.; Chen, H.L.; Chien, R.N.; Dokmeci, A.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.V.; Zoulim, F.; Tacke, F. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S.B., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- Lau, G.K.; Piratvisuth, T.; Luo, K.X.; Marcellin, P.; Thongsawat, S.; Cooksley, G.; Gane, E.; Fried, M.W.; Chow, W.C.; Paik, S.W.; et al. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N. Engl. J. Med. 2005, 352, 2682–2695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liaw, Y.F.; Jia, J.D.; Chan, H.L.; Han, K.H.; Tanwandee, T.; Chuang, W.L.; Tan, D.M.; Chen, X.Y.; Gane, E.; Piratvisuth, T.; et al. Shorter durations and lower doses of peginterferon alfa-2a are associated with inferior hepatitis B e antigen seroconversion rates in hepatitis B virus genotypes B or C. Hepatology 2011, 54, 1591–1599. [Google Scholar] [CrossRef] [PubMed]
- Buster, E.H.; Flink, H.J.; Cakaloglu, Y.; Simon, K.; Trojan, J.; Tabak, F.; So, T.M.; Feinman, S.V.; Mach, T.; Akarca, U.S.; et al. Sustained HBeAg and HBsAg loss after long-term follow-up of HBeAg-positive patients treated with peginterferon alpha-2b. Gastroenterology 2008, 135, 459–467. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Yan, K.K.-L.; Chim, A.M.-L.; Chan, H.-Y.; Tse, C.-H.; Choi, P.C.-L.; Chan, A.W.-H.; Sung, J.J.-Y.; Chan, H.L.-Y. Durability of peginterferon alfa-2b treatment at 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2010, 51, 1945–1953. [Google Scholar] [CrossRef]
- Marcellin, P.; George, K.K.; Lau Bonino, F.; Farci, P.; Hadziyannis, S.; Jin, R.; Lu, Z.M.; Piratvisuth, T.; Germanidis, G.; Yurdaydin, C.; et al. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N. Engl. J. Med. 2004, 351, 1206–1217. [Google Scholar] [CrossRef] [Green Version]
- Marcellin, P.; Bonino, F.; Yurdaydin, C.; Hadziyannis, S.; Moucari, R.; Kapprell, H.-P.; Rothe, V.; Popescu, M.; Brunetto, M.R. Hepatitis B surface antigen levels: Association with 5-year response to peginterferon alfa-2a in hepatitis B e-antigen-negative patients. Hepatol. Int. 2013, 7, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Chang, T.T.; Lai, C.L.; Yoon, S.K.; Lee, S.S.; Coelho, H.S.M.; Carrilho, F.J.; Poordad, F.; Halota, W.; Horsmans, Y.; Tsai, N.; et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology 2010, 51, 422–433. [Google Scholar] [CrossRef]
- Seto, W.K.; Lam, Y.F.; Fung, J.; Wong, D.K.; Huang, F.V.; Hung, I.F.; Lai, C.L.; Yuen, M.F. Changes of HBsAg and HBV DNA levels in Chinese chronic hepatitis B patients after 5 years of entecavir treatment. J. Gastroenterol. Hepatol. 2014, 29, 1028–1034. [Google Scholar] [CrossRef]
- Yuen, M.F.; Seto, W.K.; Fung, J.; Wong, D.K.; Yuen, J.C.; Lai, C.L. Three years of continuous entecavir therapy in treatment-naı¨ve chronic hepatitis B patients: Viral suppression, viral resistance and clinical safety. Am. J. Gastroenterol. 2011, 106, 1264–1271. [Google Scholar] [CrossRef]
- Zoutendijk, R.; Peijnders, J.G.; Brown, A.; Zoulim, F.; Mutimer, D.; Deterding, K.; Petersen, J.; Hofmann, W.P.; Buti, M.; Santantonio, T.; et al. Entecavir treatment for chronic hepatitis B: Adaptation is not needed for the majority of naïve patients with a partial virological response. Hepatology 2011, 54, 443–451. [Google Scholar] [CrossRef]
- Yokosuka, O.; Takaguchi, K.; Fujioka, S.; Shindo, M.; Chayama, K.; Kobashi, H.; Hayashi, N.; Sato, C.; Kiyosawa, K.; Tanikawa, K.; et al. Long-term use of entecavir in nucleoside-naïve Japanese patients with chronic hepatitis B infection. J. Hepatol. 2010, 52, 791–799. [Google Scholar] [CrossRef]
- Chang, T.-T.; Liaw, Y.-F.; Wu, S.-S.; Schiff, E.; Han, K.-H.; Lai, C.-L.; Safadi, R.; Lee, S.S.; Halota, W.; Goodman, Z.; et al. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology 2010, 52, 886–893. [Google Scholar] [CrossRef]
- Papatheodoridis, G.; Goulis, J.; Manolakopoulos, S.; Margariti, A.; Exarchos, X.; Kokkonis, G.; Hadziyiannis, E.; Papaioannou, C.; Manesis, E.; Pectasides, D.; et al. Changes of HBsAg and interferon-inducible protein 10 serum levels in naive HBeAg-negative chronic hepatitis B patients under 4-year entecavir therapy. J. Hepatol. 2014, 60, 62–68. [Google Scholar] [CrossRef]
- Liaw, Y.F. Reversal of cirrhosis: An achievable goal of hepatitis B antiviral therapy. J. Hepatol. 2013, 59, 880–881. [Google Scholar] [CrossRef] [Green Version]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef]
- Kumada, T.; Toyoda, H.; Tada, T.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Niinomi, T.; Yasuda, S.; Andou, Y.; et al. Effect of nucleos(t)ide analogue therapy on hepatocarcinogenesis in chronic hepatitis B paients: A propensity score analysis. J. Hepatol. 2013, 58, 427–433. [Google Scholar] [CrossRef]
- Wong, G.L.-H.; Chan, H.L.-Y.; Mak, C.W.-H.; Lee, S.K.-Y.; Ip, Z.M.-Y.; Lam, A.T.-H.; Iu, H.W.-H.; Leung, J.M.-S.; Lai, J.W.-Y.; Lo, A.O.-S.; et al. Entecavir treatment reduces hepatic events and deaths in chronic hepatitis B patients with liver cirrhosis. Hepatology 2013, 58, 1537–1547. [Google Scholar] [CrossRef]
- Su, T.-H.; Hu, T.-H.; Chen, C.-Y.; Huang, Y.-W.; Chuang, W.-L.; Lin, C.-C.; Wang, C.-C.; Su, W.-W.; Chen, M.-Y.; Peng, C.-Y.; et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016, 36, 1755–1764. [Google Scholar] [CrossRef]
- Marcellin, P.; Heathcote, E.J.; Buti, M.; Gane, E.; de Man, R.A.; Krastev, Z.; Germanidis, G.; Lee, S.S.; Flisiak, R.; Kaita, K.; et al. Tenofovir disoproxilfumarate versus adefovir dipivoxil for chronic hepatitis B. N. Engl. J. Med. 2008, 359, 2442–2455. [Google Scholar] [CrossRef]
- Buti, M.; Tsai, N.; Petersen, J.; Flisiak, R.; Gurel, S.; Krastev, Z.; Schall, R.A.; Flaherty, J.F.; Martins, E.B.; Charuworn, P.; et al. Seven-year efficacy and safety of treatment with tenofovir disoproxil fumarate for chronic hepatitis B virus infection. Dig. Dis. Sci. 2015, 60, 1457–1464. [Google Scholar] [CrossRef] [Green Version]
- Papatheodoridis, G.; Triantos, C.; Hadziyannis, E.; Zisimopoulos, K.; Georgiou, A.; Voulgaris, T.; Vlachogiannakos, I.; Nikolopoulou, V.; Manolakopoulos, S. Serum HBsAg kinetics and usefulness of interferon-inducible protein 10 serum in HBeAg-negative chronic hepatitis B patients treated with tenofovir disoproxil fumarate. J. Viral Hepat. 2015, 22, 1079–1087. [Google Scholar] [CrossRef]
- Marcellin, P.; Gane, E.; Buti, M.; Afdhal, N.; Sievert, W.; Jacobson, M.; Washington, M.K.; Germanidis, G.; Flaherty, J.F.; Schall, R.A.; et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumerate for chronic hepatitis B: A 5-year open-label follow-up study. Lancet 2013, 381, 468–475. [Google Scholar] [CrossRef]
- Kim, W.R.; Loomba, R.; Berg, T.; Schall, R.E.A.; Yee, L.J.; Dinh, P.V.; Flaherty, J.F.; Martins, E.B.; Therneau, T.M.; Jacobson, I.; et al. Impact of long-term tenofovir disoproxil fumarate on incidence of hepatocellular carcinoma in patients with chronic hepatitis B. Cancer 2015, 121, 3631–3638. [Google Scholar] [CrossRef]
- Agarwal, K.; Fung, S.K.; Nguyen, T.T.; Cheng, W.; Sicard, E.; Ryder, S.; Flaherty, J.F.; Lawson, E.; Zhao, S.; Subramanian, G.M.; et al. Twenty-eight day safety, antiviral activity, and pharmacokinetics of tenofovir alafenamide for treatment of chronic hepatitis B infection. J. Hepatol. 2015, 62, 533–540. [Google Scholar] [CrossRef]
- Chan, H.L.; Fung, S.; Seto, W.K.; Chuang, W.L.; Chen, C.Y.; Kim, H.J.; Hui, A.J.; Janssen, H.L.A.; Chowdhury, A.; Tsang, T.Y.O.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of HBeAg-positive chronic hepatitis B virus infection: A randomised, double-blind, Phase 3, non-inferiority trial. Lancet Gastroenterol. Hepatol. 2016, 1, 185–195. [Google Scholar] [CrossRef]
- Buti, M.; Gane, E.; Seto, W.K.; Chan, H.L.; Chuang, W.L.; Stepanova, T.; Hui, A.J.; Lim, Y.S.; Mehta, R.; Janssen, H.L.A.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of patients with HBeAg-negative chronic hepatitis B virus infection: A randomised, double-blind, Phase 3, non-inferiority trial. Lancet Gastroenterol. Hepatol. 2016, 1, 196–206. [Google Scholar] [CrossRef]
- Chevaliez, S.; Hezode, C.; Bahrami, S.; Grare, M.; Pawlotsky, J.M. Long-term hepatitis B surface antigen (HBsAg) kinetics during nucleoside/nucleotide analogue therapy: Finite treatment duration unlikely. J. Hepatol. 2013, 58, 676–683. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.F. Finite nucoleos(t)ide anaolog therapy in HBeAg-negative chronic hepatitis B: An emerging paradigm shift. Hepatol. Int. 2019, 13, 665–673. [Google Scholar] [CrossRef]
- Hsu, Y.C.; Yeh, M.L.; Wong, G.L.; Chen, C.H.; Peng, C.Y.; Buti, M.; Enomoto, M.; Xie, Q.; Trinh, H.; Preda, C.; et al. Incidences and Determinants of Functional Cure during Entecavir or Tenofovir Disoproxil Fumarate for Chronic Hepatitis, B. J. Infect. Dis. 2021, 224, 1890–1899. [Google Scholar] [CrossRef]
- Liaw, Y.F.; Chien, R.N.; Yeh, C.T.; Tsai, S.L.; Chu, C.M. Acute exacerbation and hepatitis B virus clearance after emergence of YMDD motif mutation during lamivudine therapy. Hepatology 1999, 30, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F. Antiviral therapy of chronic hepatitis B: Opportunities and challenges in Asia. J. Hepatol. 2009, 51, 403–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chotiyaputta, W.; Peterson, C.; Ditah, F.A.; Goodwin, D.; Lok, A.S. Persistence and adherence to necleos(t)ide analogue treatment for chronic hepatitis B. J. Hepatol. 2011, 54, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Ford, N.; Scourse, R.; Lemoine, M.; Hutin, Y.; Bulterys, M.; Shubber, Z.; Donchuk, D.; Wandeler, G. Adherence to necleos(t)ide analogues therapies for chronic hepatitis B infection: A systematic review and meta-analysis. Hepatol. Commun. 2018, 2, 1160–1167. [Google Scholar] [CrossRef]
- Shin, J.W.; Jung, S.W.; Lee, S.B.; Lee, B.U.; Park, B.R.; Park, E.J.; Park, N.H. Medication nonadherence increases hepatocellular carcinoma, cirrhotic complications, and mortality in chronic hepatitis B patients treated with entecavir. Am. J. Gastroenterol. 2018, 13, 998–1008. [Google Scholar] [CrossRef]
- Ahn, J.; Lee, H.M.; Lim, J.K.; Pan, C.Q.; Nguyen, M.H.; Ray Kim, W.; Mannalithara, A.; Trinh, H.; Chu, D.; Tran, T.; et al. Entecavir safety and effectiveness in a national cohort of treatment-naïve chronic hepatitis B patients in the US-the ENUMERATE study. Aliment. Pharmacol. Ther. 2016, 43, 134–144. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.G.; Wai, C.T.; Rajnakova, A.; Kajiji, T.; Guan, R. Fatal hepatitis B reactivation following discontinuation of nucleoside analogues for chronic hepatitis B. Gut 2002, 51, 597–599. [Google Scholar] [CrossRef]
- Jeng, W.J.; Chen, Y.C.; Chien, R.N.; Sheen, I.S.; Liaw, T.F. Incidence and predictors of HBsAg seroclearance after cessation of nucleos(t)ide analogue therapy in HBeAg negative chronic hepatitis B. Hepatology 2018, 68, 425–434. [Google Scholar] [CrossRef]
- Hadziyannis, S.J.; Sevastianos, V.; Rapti, I.; Vassilopoulos, D.; Hadziyannis, E. Sustained responses and loss of HBsAg in HBeAg-negative patients with chronic hepatitis B who stop long-term treatment with adefovir. Gastroenterology 2012, 143, 629–636. [Google Scholar] [CrossRef]
- Honer zu Siederdissen, C.; Rinker, F.; Maasoumy, B.; Wiegand, S.B.; Filmann, N.; Falk, C.S.; Deterding, K.; Deterding, K.; Port, K.; Mix, C.; et al. Viral and host responses after stopping long-term nucleos(t)ide analogue therapy in HBeAg-negative chronic hepatitis B. J. Infect. Dis. 2016, 214, 1492–1497. [Google Scholar] [CrossRef] [Green Version]
- Berg, T.; Simon, K.G.; Mauss, S.; Schott, E.; Heyne, R.; Klass, D.M.; Eisenbach, C.; Welzel, T.M.; Zachoval, R.; Felten, G.; et al. Long-term response after stopping tenofovir disoproxil fumarate in non-cirrhosis HBeAg-negative patients-FINITE study. J. Hepatol. 2017, 67, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Rigopoulou, E.I.; Papatheodoridis, M.; Zachou, K.; Xourafas, V.; Gatselis, N.; Hadziyannis, E.; Vlachogiannakos, J.; Manolakopoulos, S.; Dalekos, G.N. DARING-B: Discontinuation of effective entecavir or tenofovir disoproxil fumarate long-term therapy before HBsAg loss in non-cirrhotic HBeAg-negative chronic hepatitis B. Antivir. Ther. 2018, 23, 677–695. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Wong, G.L.; Chim, A.M.; Chan, H.Y.; Chu, S.H.; Wong, V.W. Prediction of off-treatment response to lamivudine by serum hepatitis B surface antigen quantification in hepatitis B e antigen-negative patients. Antivir. Ther. 2011, 16, 1249–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, H.; Hansen, B.E.; Yim, C.; Arends, P.; Abu-Amara, M.; van der Eijk, A.A.; Feld, J.J.; de Knegt, R.J.; Wong, D.K.H.; Janssen, H.L.A. Reduce risk of relapse after long-term nucleos(t)ide analogue consolidation therapy for chronic hepatitis B. Aliment. Pharmacol. Ther. 2015, 41, 867–876. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Hung, C.H.; Wang, J.H.; Lu, S.N.; Lai, H.C.; Hu, T.H.; Lin, C.H.; Peng, C.Y. The incidence of hepatitis B surface antigen loss between hepatitis B e antigen-negative noncirrhotic patients who discontinued or continued entecavir therapy. J. Infect. Dis. 2019, 219, 1624–1633. [Google Scholar] [CrossRef] [PubMed]
- Berg, T.; Lampertico, P. The times they are a-changing—A refined proposal for finite HBV nucleos(t)ide analog therapy. J. Hepatol. 2021, 75, 474–480. [Google Scholar] [CrossRef]
- Chang, M.L.; Liaw, Y.F. Hepatitis B flares in chronic hepatitis B: Pathogenesis, natural course and management. J. Hepatol. 2014, 61, 1407–1417. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.F. Hepatitis B Flare After Cessation of Nucleos(t)ide Analogue Therapy in HBeAg-Negative Chronic Hepatitis B: To Retreat or Not to Retreat. Hepatology 2021, 73, 843–852. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Manolakopoulos, S.; Su, T.H.; Siakavellas, S.; Liu, C.J.; Kourikou, A.; Yang, H.C.; Kao, J.H. Significance of definitions of relapse after discontinuation of oral antivirals in HBeAg-negative chronic hepatitis B. Hepatology 2018, 68, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Liem, K.S.; Fung, S.; Wong, D.K.; Yim, C.; Noureldin, S.; Chen, J.; Feld, J.J.; Hansen, B.E.; A Janssen, H.L. Limited sustained response after stopping nucleos(t)ide analogues in patients with chronic hepatitis B: Results from a randomised controlled trial (Toronto STOP study). Gut 2019, 68, 2206–2213. [Google Scholar] [CrossRef]
- García-López, M.; Lens, S.; Pallett, L.J.; Testoni, B.; Rodríguez-Tajes, S.; Mariño, Z.; Bartres, C.; Garcia-Pras, E.; Leonel, T.; Perpinan, E.; et al. Viral and immune factors associated with successful treatment withdrawal in HBeAg-negative chronic hepatitis B patients. J. Hepatol. 2021, 74, 1064–1074. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F. Clinical utility of HBV surface antigen quantification in HBV e antigen-negative chronic HBV infection. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F.; Jeng, W.J.; Chang, M.L. HBsAg kinetics in re-treatment decision for off-therapy hepatitis B flare in HBeAg-negative patients. Gastroenterology 2018, 154, 2280–2281. [Google Scholar] [CrossRef]
- Jeng, W.J.; Chang, M.L.; Liaw, Y.F. Off-therapy precipitous HBsAg decline predicts HBsAg loss after finite entecavir therapy in HBeAg-negative patients. J. Viral Hepat. 2019, 26, 1019–1026. [Google Scholar] [CrossRef]
- Chien, R.N.; Liaw, Y.F. Re-treatment for severe hepatitis flare in HBeAg-negative chronic hepatitis B: An appraisal with combined HBsAg/ALT kinetics. J. Viral Hepat. 2020, 27, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Jeng, W.J.; Kiu, Y.C.; Chien, R.N.; Liaw, Y.F. Remarkable difference in re-treatment response in patients with difference HBsAg/ALT kinetics during off-NUC hepatitis B flare. Hepatology 2019, 70, 303A. [Google Scholar]
- Papatheodoridi, M.; Papatheodoridis, G. Emerging diagnostic tools to decide when to discontinue nucleos(t)ide analogues in chronic hepatitis B. Cells 2020, 9, 493. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.G.; Phyo, W.W.; Ling, J.Z.J.; Cloherty, G.; Butler, E.K.; Kuhns, M.C.; McNamara, A.L.; Holzmayer, V.; Gersch, J.; Yang, W.L.; et al. Comparative biomarkers for HBsAg loss with antiviral therapy shows dominant influence of quantitative HBsAg (qHBsAg). Aliment. Pharmacol. Ther. 2021, 53, 172–182. [Google Scholar] [CrossRef]
Figure 1.
The cartoons demonstrated two types of combined qHBsAg/ALT kinetics during ALT flare in HBeAg-negative patients after end of NUC therapy. (a). “Host-dominating flare”: qHBsAg upsurged to peak levels and began to decline successively before or shortly after ALT peak. The flare was followed by a decline of HBV DNA and HBsAg levels with ALT normalization. (b). “Virus-dominating flare”: qHBsAg upsurged along with the ascending to the ALT to its peak and remained high after minor HBsAg decline. Patients may require antiviral therapy or hepatitis may persist or encounter another ALT flare later requiring antiviral(s) eventually. ![Viruses 14 00434 i001]() : representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
: representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
 : representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
: representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
Figure 1.
The cartoons demonstrated two types of combined qHBsAg/ALT kinetics during ALT flare in HBeAg-negative patients after end of NUC therapy. (a). “Host-dominating flare”: qHBsAg upsurged to peak levels and began to decline successively before or shortly after ALT peak. The flare was followed by a decline of HBV DNA and HBsAg levels with ALT normalization. (b). “Virus-dominating flare”: qHBsAg upsurged along with the ascending to the ALT to its peak and remained high after minor HBsAg decline. Patients may require antiviral therapy or hepatitis may persist or encounter another ALT flare later requiring antiviral(s) eventually. ![Viruses 14 00434 i001]() : representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
: representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.
: representative of host antiviral immune power including cytolytic (HLA class-I restricted CD8 mediated hepatocytolysis) and non-cytolytic (IL-2; IFN-γ; TNF-α) antiviral immune ability.

{kind=link}
Table 1.
Comparison of HBsAg loss between finite and indefinite long-term NUC therapy.
| Source [Reference] | (Country/Year) | No. of Patient | NUC Therapy | HBsAg Loss | Annular HBsAg Loss Rate |
|---|---|---|---|---|---|
| Finite Therapy | |||||
| Chan H.L., et al. [53] | (Hong Kong/2011) | 53 | LAM 3 Yr | 23%/5 Yr | 4.6% |
| Hadziyannis S.J., et al. [49] | (Greece/2012) | 33 | ADV 4–5 Yr | 39%/5 Yr | 7.8% |
| Chi H., et al. [54] | (Canada/2015) | 59 | NUC 5 Yr | 14%/3 Yr | 4.7% |
| Honer Zu Siederdissen C., et al. [50] | (Germany/2016) | 15 | NUC > 3 Yr | 20%/4 Yr | 5.0% |
| Berg T., et al. [51] | (Germany/2017) | 21 | TDF > 4 Yr | 19%/3 Yr | 6.3% |
| Papatheodoridis G.V., et al. [52] | (Greece/ 2018) | 57 | ETV/TDF 5 Yr | 16%/1 Yr | 16% |
| Jeng W.J., et al. [48] | (Taiwan/2018) | 383 (CHB) | ETV/TDF 3 Yr | 16%/6 Yr | 2.7% |
| 308 (LC) | 9%/6 Yr | 1.5% | |||
| Chen C.H., et al. [55] | (Taiwan/2019) | 234 | ETV 3 Yr | 13%/5 Yr | 2.6% |
| Indefinite long-term therapy | |||||
| Chen C.H., et al. [55] | (Taiwan/2019) | 226 | ETV 7 Yr | 1.8%/7 Yr | 0.25% |
| Hsu Y.C., et al. [40] | (Multination/2021) | 4769 | ETV/TDF 5.2Yr | 2%/10 Yr | 0.22% |
NUC: nucleos(t)ige analogue; LAM: Lamivudine; ADV: Adefovir; TDF: Tenofovir disoproxil fumarate; ETV: Entecavir; TAF: Tenofovir alafenamide; Yr: Years.
Table 2.
HBsAg loss rate related to off-NUC events.
| Event | HBV DNA (IU/mL) | ALT (U/L) | No of Patient | HBsAg Loss 6-Year Rate |
|---|---|---|---|---|
| Sustained response | <2000 | N | 144 | 36% |
| Virologic relapse | >2000 | N | 128 | 13% |
| Clinical relapse | >2000 | >2 × ULN | ||
| No-retreatment | 150 | 19% | ||
| Re-treatment | 269 | 1% | ||
| Total | 691 | 13% |
N: normal; ULN: upper limit of normal; data adapted from reference [48].
Table 3.
Biochemical criteria for retreatment decisions.
| Source [Reference] | Monitoring | Criteria to Retreat |
|---|---|---|
| Berg T., et al. [51] | 2-weekly × 3 months 4-weekly~ * | ALT > 10 × ULN > 2 visit * 5–10 × ULN > 4 weeks * Bilirubin >1.5 mg/dL or INR >1.5 |
| Papatheodoridis G.V., et al. [59] | Monthly × 3 months 3-monthly~ | ALT > 10 × ULN # ALT > 5 × ULN + bilirubin > 2 mg ALT > 3 × ULN+ HBV DNA > 105 IU/mL # |
| Liem K.S., et al. [60] | Week 4 and 6 then 6–8 weeks * | ALT > 15 × ULN # ALT >5 × ULN > 2 visits * ALT, 200–600 U/L for 6–8 weeks * |
| Garcia-Lopez M., et al. [61] | Week 3, 6, 12, 18, 24 * | ALT > 10 × ULN × 2 * ALT > 5–10 × ULN > 4 weeks * ALT > 2–5 × ULN > 6 months * |
#: at one time point may be too early; *: follow-up >four-weeks may be too late.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chien, R.-N.; Liaw, Y.-F. Current Trend in Antiviral Therapy for Chronic Hepatitis B. Viruses 2022, 14, 434. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020434
AMA Style
Chien R-N, Liaw Y-F. Current Trend in Antiviral Therapy for Chronic Hepatitis B. Viruses. 2022; 14(2):434. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020434
Chicago/Turabian StyleChien, Rong-Nan, and Yun-Fan Liaw. 2022. "Current Trend in Antiviral Therapy for Chronic Hepatitis B" Viruses 14, no. 2: 434. https://0-doi-org.brum.beds.ac.uk/10.3390/v14020434
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.