
Low T Cell Responsiveness in the Early Phase of COVID-19 Associates with Progression to Severe Pneumonia in Kidney Transplant Recipients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, Data Collection
2.2. Collection of Blood Samples and Immunoassays
2.3. Statistical Analysis
2.3.1. Descriptive Statistics
2.3.2. Unsupervised Classification
2.3.3. Penalized Logistic Regression
3. Results
3.1. Characteristics of the Study Population and Outcomes
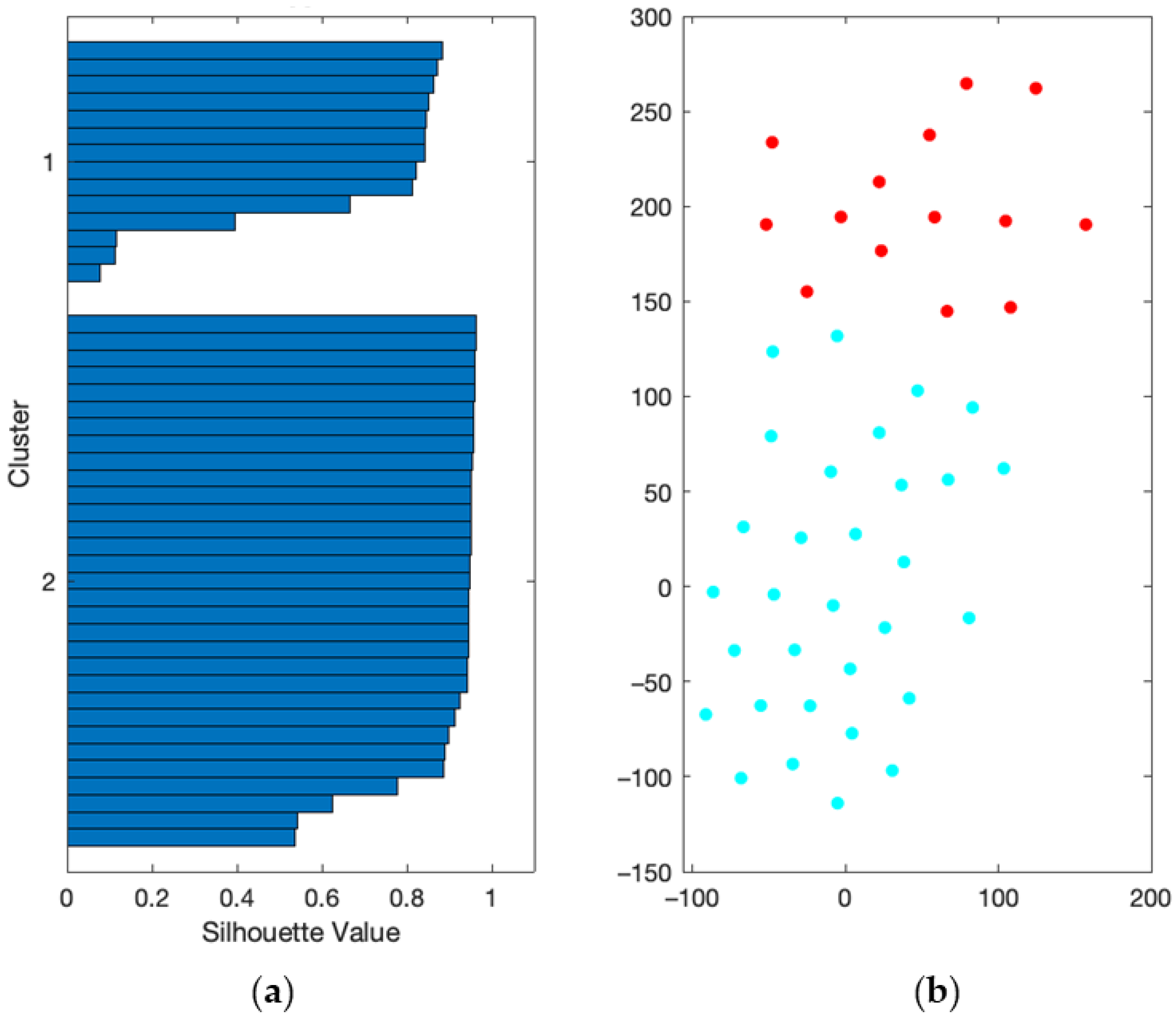
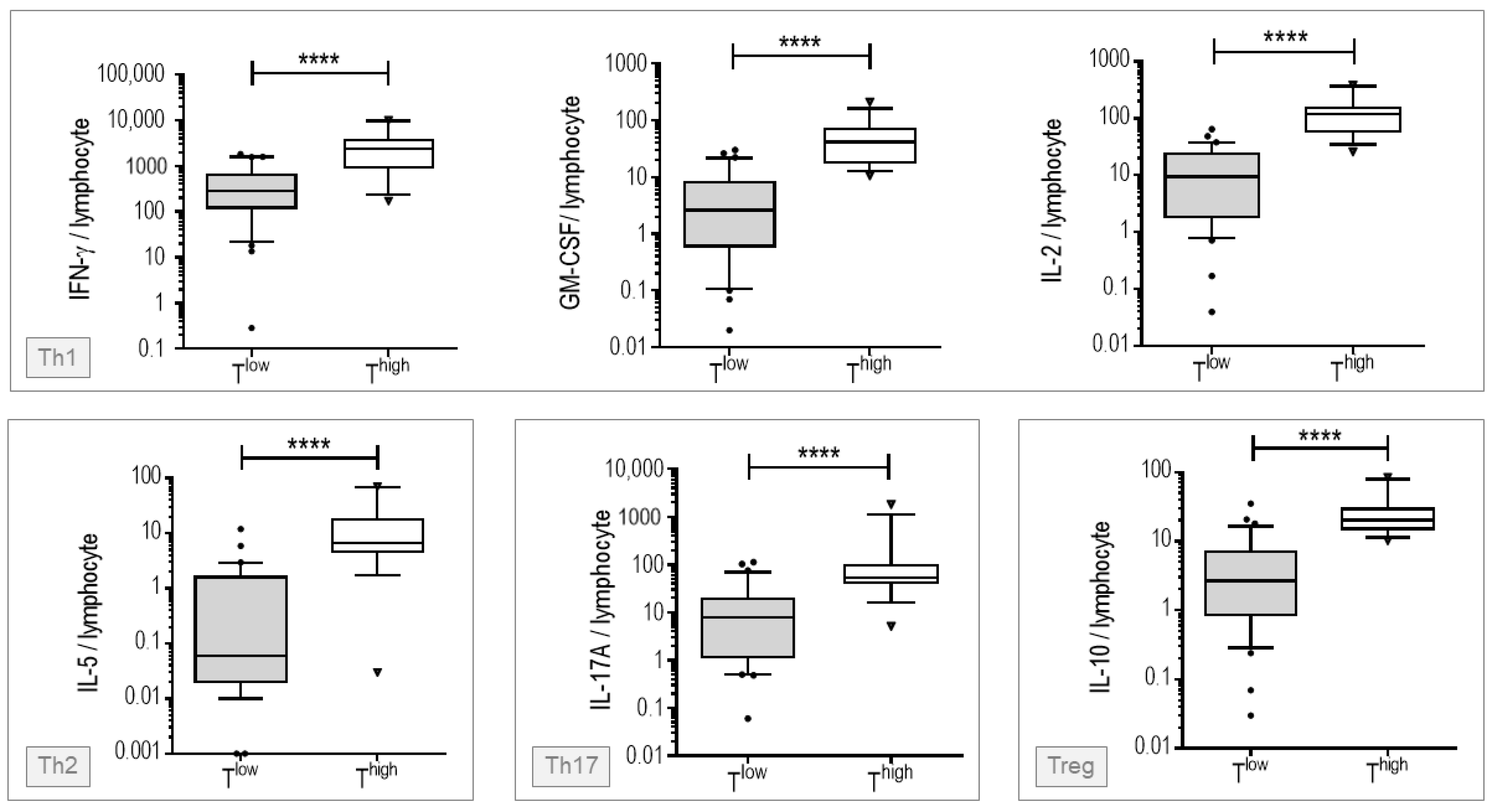
3.2. Patients Stratification Based on Early T Cells Responsiveness
3.3. Characteristics and Outcomes of Low and High T Cell Responders
3.4. Variables Associated with the Risk to Progression to Severe Pneumonia
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banerjee, D.; Popoola, J.; Shah, S.; Ster, I.C.; Quan, V.; Phanish, M. COVID-19 infection in kidney transplant recipients. Kidney Int. 2020, 97, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. COVID-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020, 20, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. UW COVID-19 SOT Study Team. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin. Infect. Dis. 2021, 73, e4090–e4099. [Google Scholar] [CrossRef]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Zambetti, N.; Moscato, M.; et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int. 2020, 97, 1083–1088. [Google Scholar] [CrossRef]
- Phanish, M.; Ster, I.C.; Ghazanfar, A.; Cole, N.; Quan, V.; Hull, R.; Banerjee, D. Systematic Review and Meta-analysis of COVID-19 and Kidney Transplant Recipients; the South West London Kidney Transplant Network Experience. Kidney Int. Rep. 2021, 6, 574–585. [Google Scholar] [CrossRef]
- Khairallah, P.; Aggarwal, N.; Awan, A.A.; Vangala, C.; Airy, M.; Pan, J.S.; Murthy, B.V.R.; Winkelmayer, W.C.; Ramanathan, V. The impact of COVID-19 on kidney transplantation and the kidney transplant recipient - One year into the pandemic. Transpl. Int. 2021, 612–621. [Google Scholar] [CrossRef]
- Coll, E.; Fernández-Ruiz, M.; Sánchez-Álvarez, J.E.; Martínez-Fernández, J.R.; Crespo, M.; Gayoso, J.; Bada-Bosch, T.; Oppenheimer, F.; Moreso, F.; López-Oliva, M.O.; et al. Spanish Group for the Study of COVID-19 in Transplant Recipients. COVID-19 in transplant recipients: The Spanish experience. Am. J. Transplant. 2021, 21, 1825–1837. [Google Scholar] [CrossRef]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. French SOT COVID Registry. Is COVID-19 infection more severe in kidney transplant recipients? Am. J. Transplant. 2021, 21, 1295–1303. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Invest. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed]
- Ruetsch, C.; Brglez, V.; Crémoni, M.; Zorzi, K.; Fernandez, C.; Boyer-Suavet, S.; Benzaken, S.; Demonchy, E.; Risso, K.; Courjon, J.; et al. Functional Exhaustion of Type I and II Interferons Production in Severe COVID-19 Patients. Front. Med. 2021, 7, 603961. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M. Building Predictive Models in R Using the caret Package. J. Stat. Soft. 2008, 28, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Soft. 2010, 33. [Google Scholar] [CrossRef] [Green Version]
- Bunea, F.; She, Y.; Ombao, H.; Gongvatana, A.; Devlin, K.; Cohen, R. Penalized least squares regression methods and applications to neuroimaging. Neuroimage 2011, 55, 1519–1527. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.P.; Chopin, N.; Rousseau, J. Harold Jeffreys’s Theory of Probability Revisited. Statist. Sci. 2009, 24, 141–172. [Google Scholar] [CrossRef]
- Cravedi, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Pérez-Sáez, M.J.; Redondo-Pachón, M.D.; Murphy, B.; Flor-man, S.; Cyrino, L.G.; et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020, 20, 3140–3148. [Google Scholar] [CrossRef]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Coates, P.T.; Wong, G.; Drueke, T.; Rovin, B.; Ronco, P.; Associate Editors; for the Entire Editorial Team. Early experience with COVID-19 in kidney transplantation. Kidney Int. 2020, 97, 1074–1075. [Google Scholar] [CrossRef]
- Mahalingasivam, V.; Craik, A.; Tomlinson, L.A.; Ge, L.; Hou, L.; Wang, Q.; Yang, K.; Fogarty, D.G.; Keenan, C. A Systematic Review of COVID-19 and Kidney Transplantation. Kidney Int Rep. 2021 Jan;6, 24-45. Kidney Int. Rep. 2021, 6, 24–45. [Google Scholar] [CrossRef] [PubMed]
- Brunet, L.R.; LaBrie, S.; Hagemann, T. Immune monitoring technology primer: Immunoprofiling of antigen-stimulated blood. J. Immunother. Cancer. 2016, 4, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, M.M.; Hrusch, C.L.; Gozdz, J.; Igartua, C.; Pivniouk, V.; Murray, S.E.; Ledford, J.G.; Marques, D.S.M.; Anderson, R.L.; Metwali, N.; et al. Innate Immunity and Asthma Risk in Amish and Hutterite Farm Children. N. Engl. J. Med. 2016, 375, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnjatic, S.; Bronte, V.; Brunet, L.R.; Butler, M.O.; Disis, M.L.; Galon, J.; Hakansson, L.G.; Hanks, B.A.; Karanikas, V.; Khleif, S.N.; et al. Identifying baseline immune-related biomarkers to predict clinical outcome of immunotherapy. J. Immunother. Cancer 2017, 16, 44. [Google Scholar] [CrossRef]
- Duffy, D.; Rouilly, V.; Braudeau, C.; Corbière, V.; Djebali, R.; Ungeheuer, M.N.; Josien, R.; LaBrie, S.T.; Lantz, O.; Louis, D.; et al. Multinational FOCIS Centers of Excellence. Standardized whole blood stimulation improves immunomonitoring of induced immune responses in multi-center study. Clin. Immunol. 2017, 183, 325–335. [Google Scholar] [CrossRef]
- Thervet, E.; Anglicheau, D.; King, B.; Schlageter, M.H.; Cassinat, B.; Beaune, P.; Legendre, C.; Daly, A.K. Impact of cytochrome p450 3A5 genetic polymorphism on tacrolimus doses and concentration-to-dose ratio in renal transplant recipients. Transplantation 2003, 76, 1233–1235. [Google Scholar] [CrossRef]
- Anglicheau, D.; Legendre, C.; Beaune, P.; Thervet, E. Cytochrome P450 3A polymorphisms and immunosuppressive drugs: An update. Pharmacogenomics 2007, 8, 835–849. [Google Scholar] [CrossRef]
- Thervet, E.; Anglicheau, D.; Legendre, C.; Beaune, P. Role of pharmacogenetics of immunosuppressive drugs in organ transplantation. Ther. Drug Monit. 2008, 30, 143–150. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Chen, Z.; John Wherry, E. T cell responses in patients with COVID-19. Nat. Rev. Immunol. 2020, 20, 529–536. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline characteristics | |
| Age, years | 51.7 (16.9) |
| Males | 33 (73%) |
| Comorbidities | |
| Diabetes | 9 (20%) |
| Hypertension | 41 (91%) |
| Cardiovascular events | 4 (9%) |
| BMI > 30 kg/m² | 10 (22%) |
| COPD | 1 (2%) |
| Time since transplantation, months | 35 (1–400) |
| Prior renal transplantation | 4 (9%) |
| Pretransplant Donor Specific Antibodies | 0 (0%) |
| Baseline creatininemia, µmol/L | 127.5 (79.6–460.0) |
| Baseline eGFR, mL/min/1.73 m² | 49.0 (13.0–120.0) |
| Immunosuppressive therapy at inclusion | |
| Corticosteroids | 34 (76%) |
| Calcineurin inhibitors | 43 (96%) |
| Antimetabolites | 37 (82%) |
| mTOR inhibitors | 3 (7%) |
| Presentation at inclusion | |
| Time since symptoms onset, days | 5.8 (2.1) |
| Fever | 11 (24%) |
| Cough | 16 (36%) |
| Dyspnea with normal oxygen saturation | 8 (18%) |
| Anosmia/ageusia | 11 (24%) |
| Diarrhea | 8 (18%) |
| Headache | 16 (36%) |
| Serum creatinine, µmol/L | 142.1 (79.5–398.0) |
| Lymphocytes count, ×109/L | 0.9 (0.2–3.7) |
| Residual tacrolemia, µg/L * | 7.19 (2.30–18.40) |
| Clinical course | |
| Progression to severe pneumonia | 11 (24%) |
| Subsequent ICU admission | 2 (4%) |
| Death | 1 (2%) |
| Low T cell responders (n = 31) | High T cell responders (n = 14) | p-value | |
|---|---|---|---|
| Baseline characteristics | |||
| Age, years | 53.0 (17.3) | 48.9 (16.1) | 0.45 |
| Males | 22 (71%) | 11 (79%) | 0.73 |
| Comorbidities | |||
| Diabetes | 7 (23%) | 2 (14%) | 0.70 |
| Hypertension | 27 (87%) | 14 (100%) | 0.29 |
| Cardiovascular events | 2 (6%) | 2 (14%) | 0.58 |
| BMI> 30 kg/m² | 7 (23%) | 3 (21%) | >0.99 |
| Time since transplantation, months | 21 (1–400) | 57 (10–186) | 0.13 |
| Prior renal transplantation | 2 (6%) | 2 (14%) | 0.58 |
| Baseline creatininemia, µmol/L | 120.0 (79.6–460.0) | 145.5 (94.0–195.0) | 0.42 |
| Baseline eGFR, mL/min/1.73 m² | 53.0 (13.0–64.0) | 43.5 (28.0–85.0) | 0.57 |
| Immunosuppressive therapy at inclusion | |||
| Corticosteroids | 23 (74%) | 11 (79%) | >0.99 |
| Calcineurin inhibitors | 30 (97%) | 13 (93%) | 0.53 |
| Antimetabolites | 28 (90%) | 9 (64%) | 0.08 |
| mTOR inhibitors | 2 (6%) | 1 (7%) | >0.99 |
| Presentation at inclusion | |||
| Time since symptoms onset, days | 5.8 (2.1) | 5.6 (2.2) | 0.78 |
| Fever | 9 (29%) | 2 (14%) | 0.46 |
| Cough | 11 (35%) | 5 (36%) | >0.99 |
| Dyspnea with normal oxygen saturation | 6 (19%) | 2 (14%) | >0.99 |
| Anosmia/ageusia | 7 (23%) | 4 (29%) | 0.72 |
| Diarrhea | 5 (16%) | 3 (21%) | 0.69 |
| Headache | 9 (29%) | 7 (50%) | 0.20 |
| Serum creatinine, µmol/L | 142.1 (79.5–398.0) | 141.4 (94.0–231.8) | 0.67 |
| Lymphocytes count, ×109/L | 0.8 (0.2–3.7) | 1.1 (0.3–2.9) | 0.31 |
| Residual tacrolemia, µg/L * | 9.05 (4.46) | 7.26 (1.66) | 0.50 |
| Immunosuppression management | |||
| Antimetabolites withdrawal | 16/28 (57%) | 4/9 (44%) | 0.70 |
| Clinical course | |||
| Progression to severe pneumonia | 11 (35%) | 0 (0%) | 0.01 |
| Median ORs | %95 CI | VIP | |
|---|---|---|---|
| High T cell responsiveness (cluster 1) | 0.43 | [0.05–1.00] | 0.85 |
| Low T cell responsiveness (cluster 2) | 3.00 | [1.53–39.10] | 0.98 |
| Age (years) | 0.86 | [0.12–1.87] | 0.58 |
| Sex (Female) | 0.63 | [0.13–2.31] | 0.65 |
| Sex (Male) | 1.49 | [0.47–6.72] | 0.62 |
| BMI (kg/m²) | 1.28 | [0.48–4.32] | 0.68 |
| Time since transplantation (years) | 0.69 | [0.14–1.40] | 0.68 |
| Basal creatinemia (µmoL/L) | 2.06 | [1.13–9.21] | 0.97 |
| Diabetes (No) | 0.43 | [0.02–1.49] | 0.84 |
| Diabetes (Yes) | 1.73 | [0.66–33.09] | 0.75 |
| Calcineurin inhibitor (No) | 0.52 | [0.08–0.95] | 0.57 |
| Calcineurin inhibitor (Yes) | 1.83 | [1.00–10.18] | 0.53 |
| mTOR inhibitor (No) | 1.13 | [0.32–3.58] | 0.37 |
| mTOR inhibitor (Yes) | 0.97 | [0.37–2.90] | 0.37 |
| Steroids (No) | 1.47 | [0.48–11.63] | 0.70 |
| Steroids (Yes) | 0.84 | [0.10–2.08] | 0.67 |
| Antimetabolites (No) | 0.42 | [0.06–0.91] | 0.95 |
| Antimetabolites (Yes) | 1.92 | [1.00–10.16] | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cremoni, M.; Cuozzo, S.; Martinuzzi, E.; Barbosa, S.; Ben Hassen, N.; Massa, F.; Demonchy, E.; Durand, M.; Thaunat, O.; Esnault, V.; et al. Low T Cell Responsiveness in the Early Phase of COVID-19 Associates with Progression to Severe Pneumonia in Kidney Transplant Recipients. Viruses 2022, 14, 542. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030542
Cremoni M, Cuozzo S, Martinuzzi E, Barbosa S, Ben Hassen N, Massa F, Demonchy E, Durand M, Thaunat O, Esnault V, et al. Low T Cell Responsiveness in the Early Phase of COVID-19 Associates with Progression to Severe Pneumonia in Kidney Transplant Recipients. Viruses. 2022; 14(3):542. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030542
Chicago/Turabian StyleCremoni, Marion, Sébastien Cuozzo, Emanuela Martinuzzi, Susana Barbosa, Nadia Ben Hassen, Filippo Massa, Elisa Demonchy, Matthieu Durand, Olivier Thaunat, Vincent Esnault, and et al. 2022. "Low T Cell Responsiveness in the Early Phase of COVID-19 Associates with Progression to Severe Pneumonia in Kidney Transplant Recipients" Viruses 14, no. 3: 542. https://0-doi-org.brum.beds.ac.uk/10.3390/v14030542