
Long-Term Outcomes after Vaccine-Induced Thrombotic Thrombocytopenia


Abstract
:1. Introduction
2. Materials and Methods
- Vaccination 4 to 21 days before symptom onset.
- Signs or symptoms of venous or arterial thrombosis.
- Thrombocytopenia < 150/nL.
- Positive anti-platelet factor 4 (PF4) antibody.
- Elevated D-Dimer > 4 times upper limit of normal.
3. Results
3.1. Presenting Characteristics
3.2. Details on Thromboembolic Events
3.3. Initial Therapy
3.4. Long-Term Therapy
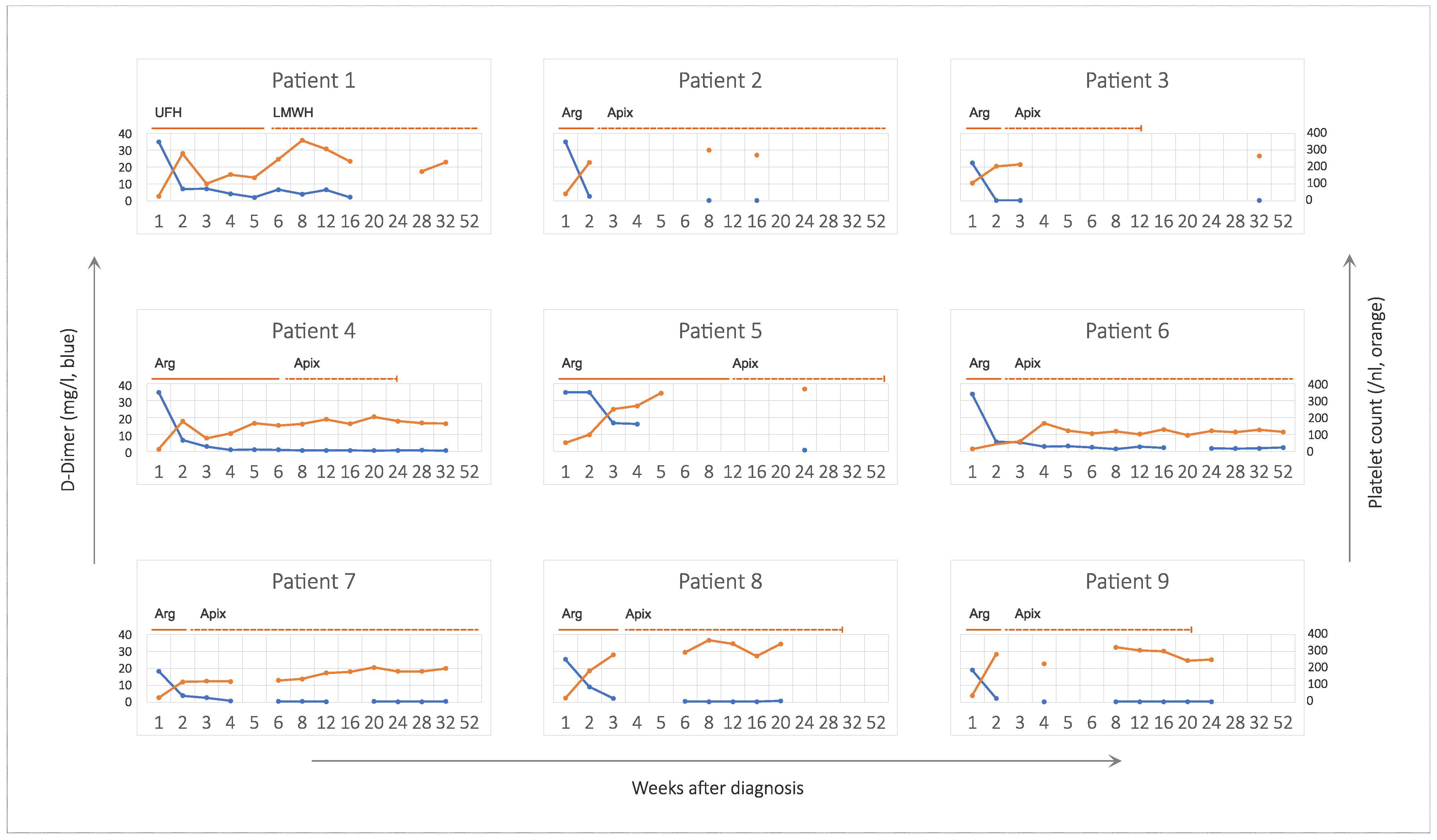
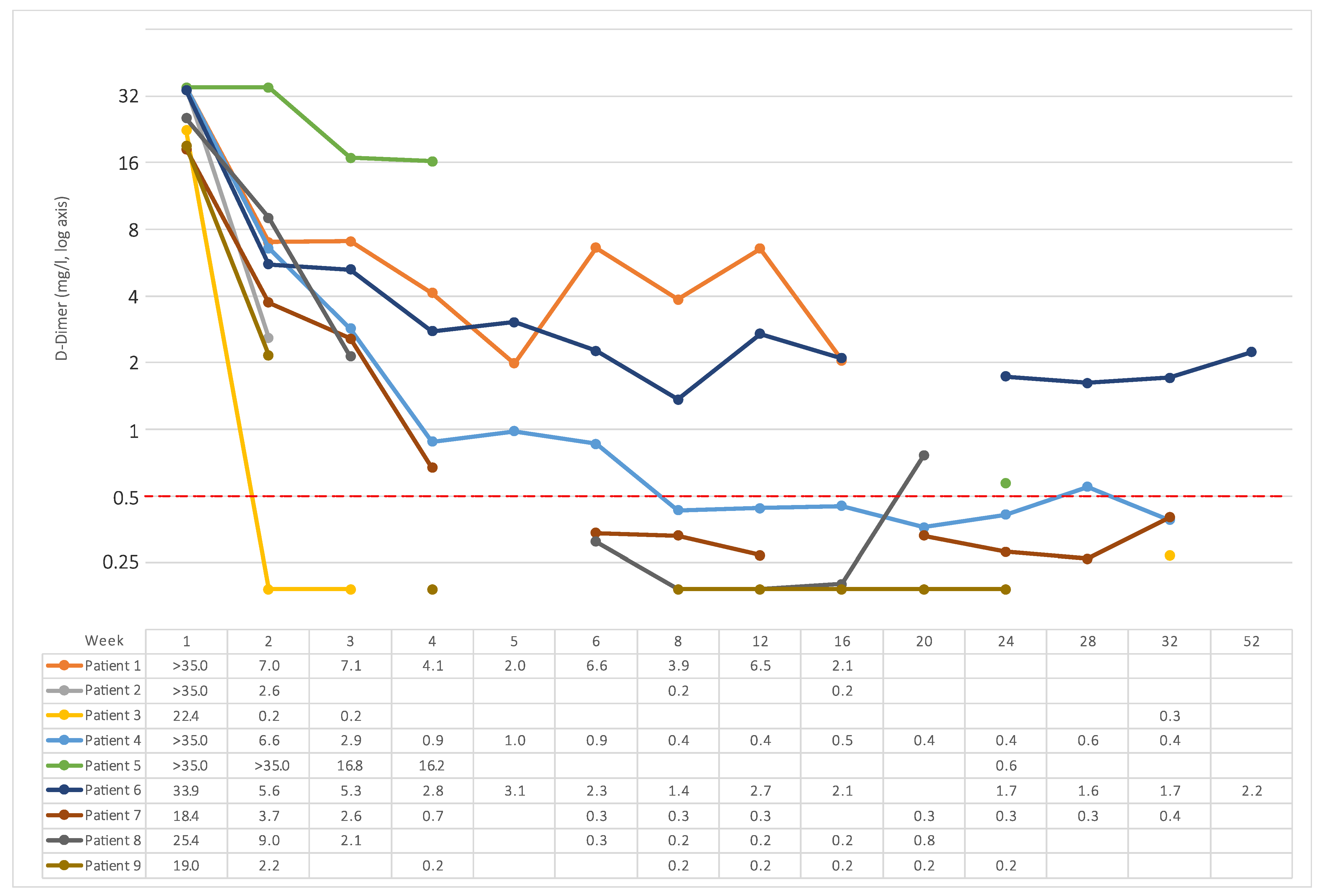
3.5. Platelet Count and D-Dimer
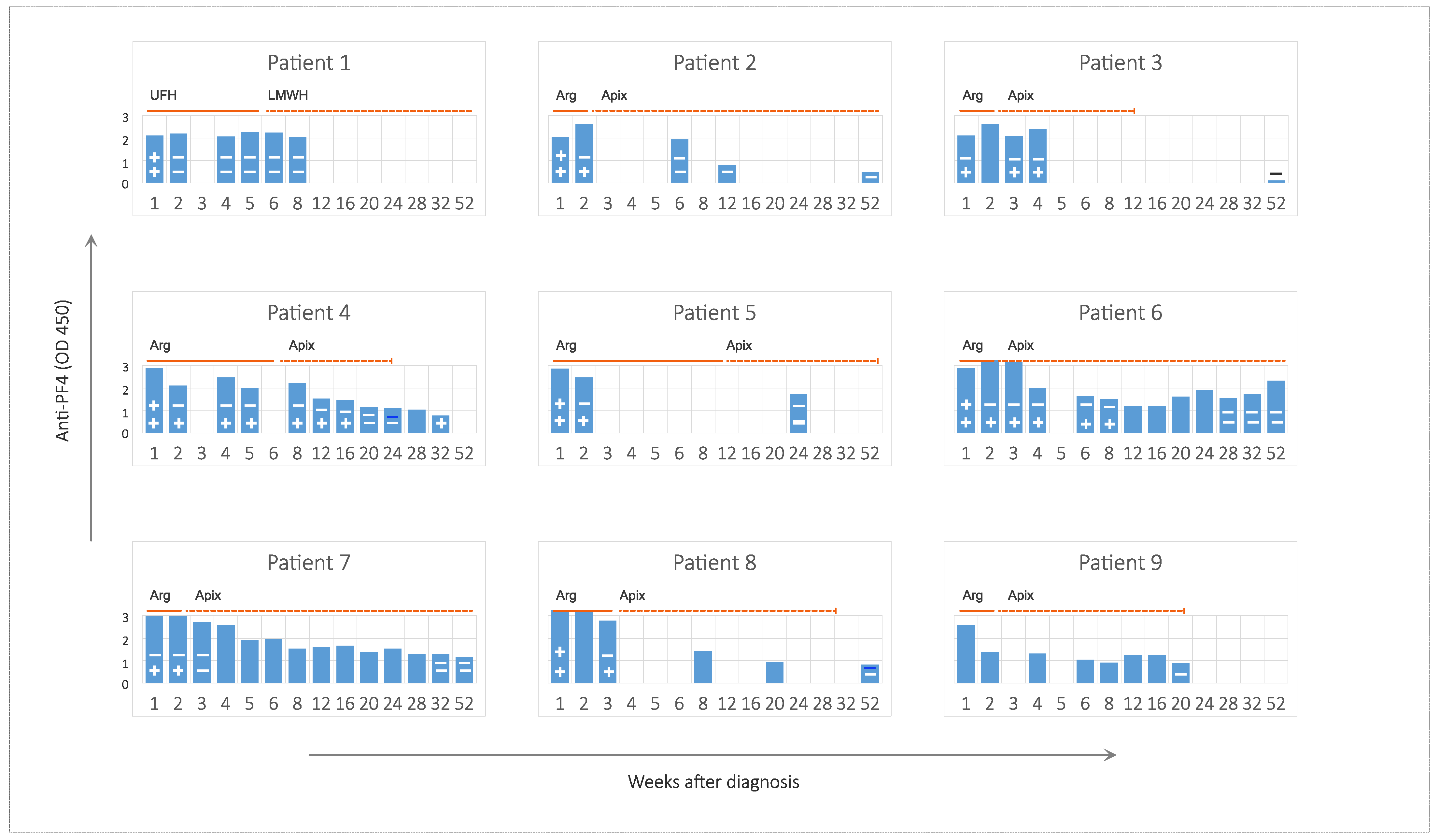
3.6. Anti-PF4 Antibodies and Platelet Binding
3.7. Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodes-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 27 June 2022).
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.H.; Sorvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattor, T.H.; Tjonnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Lale, A.; Marquez, P.; Streiff, M.B.; Wheeler, A.P.; Tepper, N.K.; Woo, E.J.; Broder, K.R.; Edwards, K.M.; Gallego, R.; et al. Case Series of Thrombosis With Thrombocytopenia Syndrome After COVID-19 Vaccination-United States, December 2020 to August 2021. Ann. Intern. Med. 2022, 175, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef] [PubMed]
- Tiede, A.; Sachs, U.J.; Czwalinna, A.; Werwitzke, S.; Bikker, R.; Krauss, J.K.; Donnerstag, F.; Weissenborn, K.; Hoglinger, G.; Maasoumy, B.; et al. Prothrombotic immune thrombocytopenia after COVID-19 vaccination. Blood 2021, 138, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, J.; Klamroth, R.; Langer, F.; Albisetti, M.; von Auer, C.; Ay, C.; Korte, W.; Scharf, R.E.; Potzsch, B.; Greinacher, A. Diagnosis and Management of Vaccine-Related Thrombosis following AstraZeneca COVID-19 Vaccination: Guidance Statement from the GTH. Hamostaseologie 2021, 41, 184–189. [Google Scholar] [PubMed]
- Oldenburg, J.; Klamroth, R.; Langer, F.; Pötzsch, B.; Greinacher, A. Updated GTH Statement on Vaccination with the AstraZeneca COVID-19 Vaccine, as of 22 March 2021. Available online: https://gth-online.org/wp-content/uploads/2021/03/GTH_Stellungnahme_AstraZeneca_engl._3_24_2021.pdf (accessed on 27 June 2022).
- Greinacher, A.; Selleng, K.; Warkentin, T.E. Autoimmune heparin-induced thrombocytopenia. J. Thromb. Haemost. 2017, 15, 2099–2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachs, U.J.; Cooper, N.; Czwalinna, A.; Muller, J.; Potzsch, B.; Tiede, A.; Althaus, K. PF4-Dependent Immunoassays in Patients with Vaccine-Induced Immune Thrombotic Thrombocytopenia: Results of an Interlaboratory Comparison. Thromb. Haemost. 2021, 121, 1622–1627. [Google Scholar] [PubMed]
- Bourguignon, A.; Arnold, D.M.; Warkentin, T.E.; Smith, J.W.; Pannu, T.; Shrum, J.M.; Al Maqrashi, Z.A.A.; Shroff, A.; Lessard, M.C.; Blais, N.; et al. Adjunct Immune Globulin for Vaccine-Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 385, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Uzun, G.; Althaus, K.; Singh, A.; Moller, P.; Ziemann, U.; Mengel, A.; Rosenberger, P.; Guthoff, M.; Petzold, G.C.; Muller, J.; et al. The use of IV immunoglobulin in the treatment of vaccine-induced immune thrombotic thrombocytopenia. Blood 2021, 138, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Thiele, T.; Ulm, L.; Holtfreter, S.; Schonborn, L.; Kuhn, S.O.; Scheer, C.; Warkentin, T.E.; Broker, B.M.; Becker, K.; Aurich, K.; et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood 2021, 138, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Cesari, F.; Sorrentino, S.; Gori, A.M.; Rogolino, A.; De Cristofaro, R.; Giusti, B.; Sticchi, E.; De Candia, E.; Marcucci, R. Detection of Platelet-Activating Antibodies Associated with Vaccine-Induced Thrombotic Thrombocytopenia by Flow Cytometry: An Italian Experience. Viruses 2022, 14, 1133. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Toma, F.; Uzun, G.; Wagner, T.R.; Pelzl, L.; Zlamal, J.; Freytag, V.; Weich, K.; Nowak-Harnau, S.; Rothbauer, U.; et al. The interaction between anti-PF4 antibodies and anticoagulants in vaccine-induced thrombotic thrombocytopenia. Blood 2022, 139, 3430–3438. [Google Scholar] [CrossRef] [PubMed]
- Pitkanen, H.H.; Jouppila, A.; Helin, T.; Dulipati, V.; Kotimaa, J.; Meri, S.; Kantele, A.; Jalkanen, P.; Julkunen, I.; Lassila, R. COVID-19 adenovirus vaccine triggers antibodies against PF4 complexes to activate complement and platelets. Thromb. Res. 2021, 208, 129–137. [Google Scholar] [CrossRef] [PubMed]
- de Buhr, N.; Baumann, T.; Werlein, C.; Fingerhut, L.; Imker, R.; Meurer, M.; Gotz, F.; Bronzlik, P.; Kuhnel, M.P.; Jonigk, D.D.; et al. Insights Into Immunothrombotic Mechanisms in Acute Stroke due to Vaccine-Induced Immune Thrombotic Thrombocytopenia. Front. Immunol. 2022, 13, 879157. [Google Scholar] [CrossRef] [PubMed]
- Major, A.; Carll, T.; Chan, C.W.; Christenson, C.; Aldarweesh, F.; Wool, G.D.; Cohen, K.S. Refractory vaccine-induced immune thrombotic thrombocytopenia (VITT) managed with delayed therapeutic plasma exchange (TPE). J. Clin. Apher. 2022, 37, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Scutelnic, A.; Krzywicka, K.; Mbroh, J.; van de Munckhof, A.; Sanchez van Kammen, M.; Aguiar de Sousa, D.; Lindgren, E.; Jood, K.; Gunther, A.; Hiltunen, S.; et al. Management of cerebral venous thrombosis due to adenoviral COVID-19 vaccination. Ann. Neurol. 2022. [Google Scholar] [CrossRef]
- The DVTENOX Study Group. Markers of hemostatic system activation in acute deep venous thrombosis-evolution during the first days of heparin treatment. Thromb. Haemost. 1993, 70, 909–914. [Google Scholar]
- Montague, S.J.; Smith, C.W.; Lodwick, C.S.; Stoneley, C.; Roberts, M.; Lowe, G.C.; Lester, W.A.; Watson, S.P.; Nicolson, P.L.R. Anti-platelet factor 4 immunoglobulin G levels in vaccine-induced immune thrombocytopenia and thrombosis: Persistent positivity through 7 months. Res. Pract. Thromb. Haemost. 2022, 6, e12707. [Google Scholar] [CrossRef] [PubMed]
- Thaler, J.; Jilma, P.; Samadi, N.; Roitner, F.; Mikuskova, E.; Kudrnovsky-Moser, S.; Rettl, J.; Preiss, R.; Quehenberger, P.; Pabinger, I.; et al. Long-term follow-up after successful treatment of vaccine-induced prothrombotic immune thrombocytopenia. Thromb. Res. 2021, 207, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Eudravigilance European Database of Suspected Adverse Reaction Reports. Available online: http://www.adrreports.eu/en/index.html (accessed on 27 June 2022).




{kind=link}
{kind=link}
{kind=link}
| Category | Characteristic | Data |
|---|---|---|
| Demographics | Female gender, n (%) | 8 (89) |
| Age in years, mean (SD) | 56.7 (12.4) | |
| Diagnosis of VITT | Days after vaccination, mean (SD) | 12 (5) |
| Received Vaxzevria, n (%) | 9 (100) | |
| Presenting after 1st vaccination, n (%) | 8 (89) | |
| Presenting after 2nd vaccination, n (%) | 1 (11) | |
| Clinical | Signs or symptoms of thromboembolic event, n (%) | 9 (100) |
| Confirmation of thromboembolic event, n (%) | 8 (89) | |
| Petechiae, n (%) | 6 (67) | |
| Laboratory data | Positive anti-PF4 antibodies (ELISA), n (%) | 9 (100) |
| Positive HIPA (with AZD1222), n (%) | 7 (78) | |
| Platelet count per nL, median (range) | 27 (12–105) | |
| D-Dimer in mg/L, median (range) | 33.9 (18.4–>35) |
| Patient Number | Clinical Events | Argatroban | Corticosteroids | IVIG | Eculizumab |
|---|---|---|---|---|---|
| 1 | Cerebral venous sinus thrombosis, thrombotic microangiopathy | − 1 | + | − | + (1st) |
| 2 | Arterial cerebral embolism | + | + | + | − |
| 3 | Transitory ischemic attack | + | + | − | − |
| 4 | Splanchnic vein thrombosis | + 2 | − | + (1st) | + (2nd) |
| 5 | Cerebral and popliteal artery thrombosis, DVT, pulmonary embolism | + | − | + | − |
| 6 | DVT | + | + | + (1st) | + (2nd) |
| 7 | None | + | + | − | − |
| 8 | Portal vein thrombosis, DVT | + | + | − | − |
| 9 | DVT | + | − | − | − |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panagiota, V.; Dobbelstein, C.; Werwitzke, S.; Ganser, A.; Cooper, N.; Sachs, U.J.; Tiede, A. Long-Term Outcomes after Vaccine-Induced Thrombotic Thrombocytopenia. Viruses 2022, 14, 1702. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081702
Panagiota V, Dobbelstein C, Werwitzke S, Ganser A, Cooper N, Sachs UJ, Tiede A. Long-Term Outcomes after Vaccine-Induced Thrombotic Thrombocytopenia. Viruses. 2022; 14(8):1702. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081702
Chicago/Turabian StylePanagiota, Victoria, Christiane Dobbelstein, Sonja Werwitzke, Arnold Ganser, Nina Cooper, Ulrich J. Sachs, and Andreas Tiede. 2022. "Long-Term Outcomes after Vaccine-Induced Thrombotic Thrombocytopenia" Viruses 14, no. 8: 1702. https://0-doi-org.brum.beds.ac.uk/10.3390/v14081702