
Compartmental and COMSOL Multiphysics 3D Modeling of Drug Diffusion to the Vitreous Following the Administration of a Sustained-Release Drug Delivery System

 ,
,
Abstract
:1. Introduction
1.1. Ocular Drug Delivery
1.2. Drug Delivery Systems
1.3. Modeling Pharmacokinetics
2. Materials and Methods
2.1. Hydrogel Synthesis
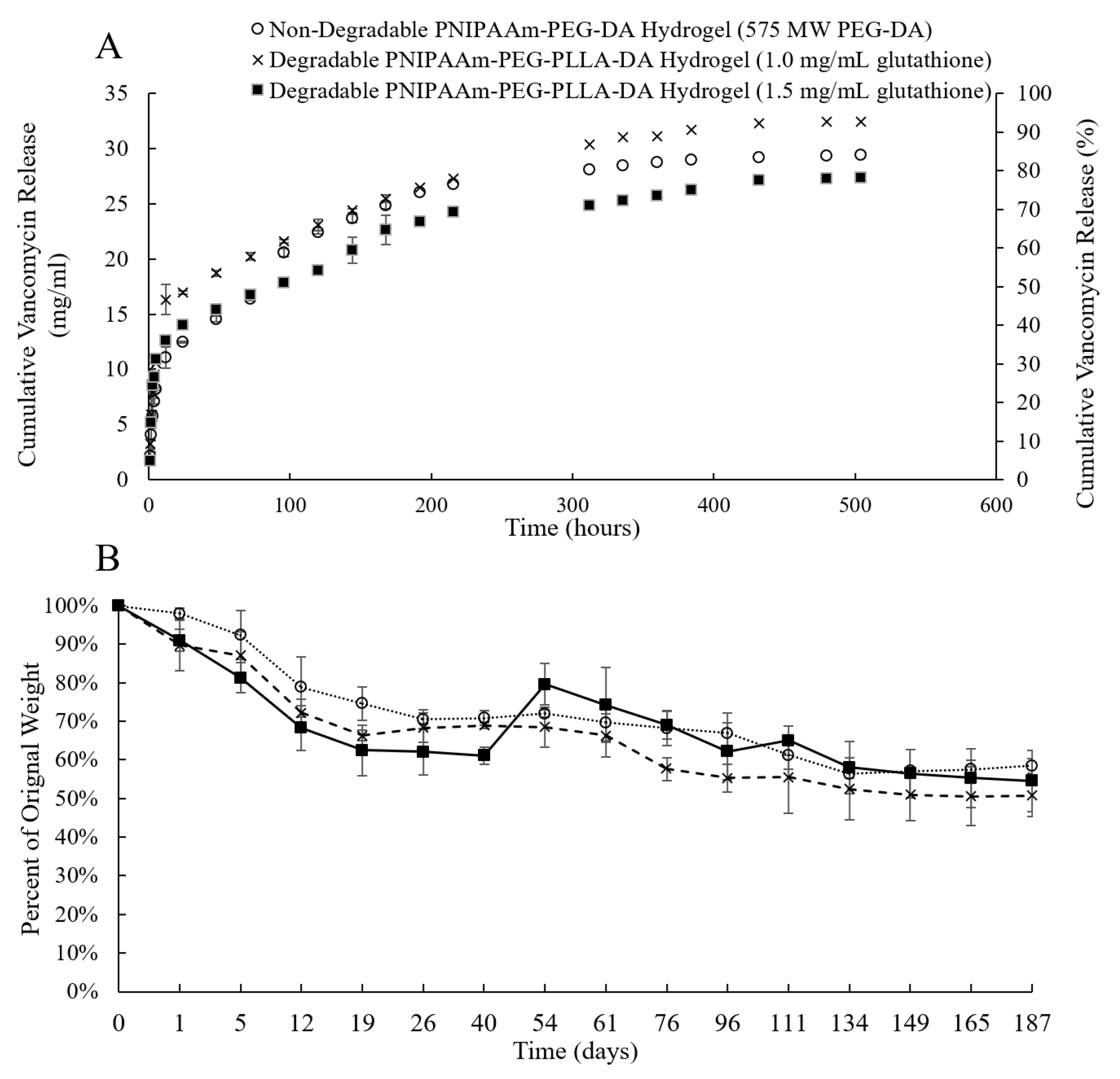
2.2. Effect of Glutathione on Thermo-Responsive Hydrogel Degradation
2.3. Hydrogel Encapsulation Efficiency
2.4. Hydrogel Release Profiles
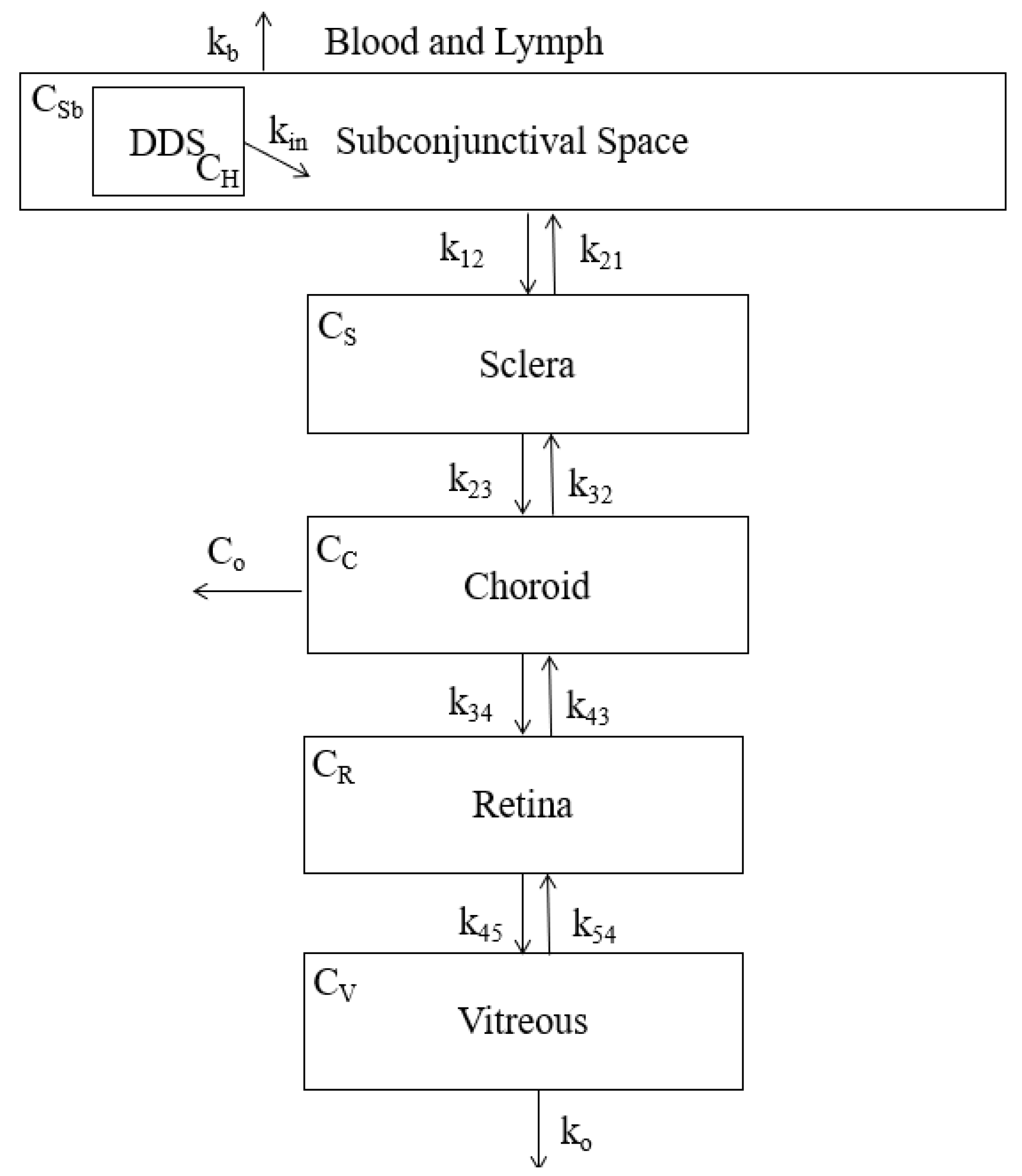
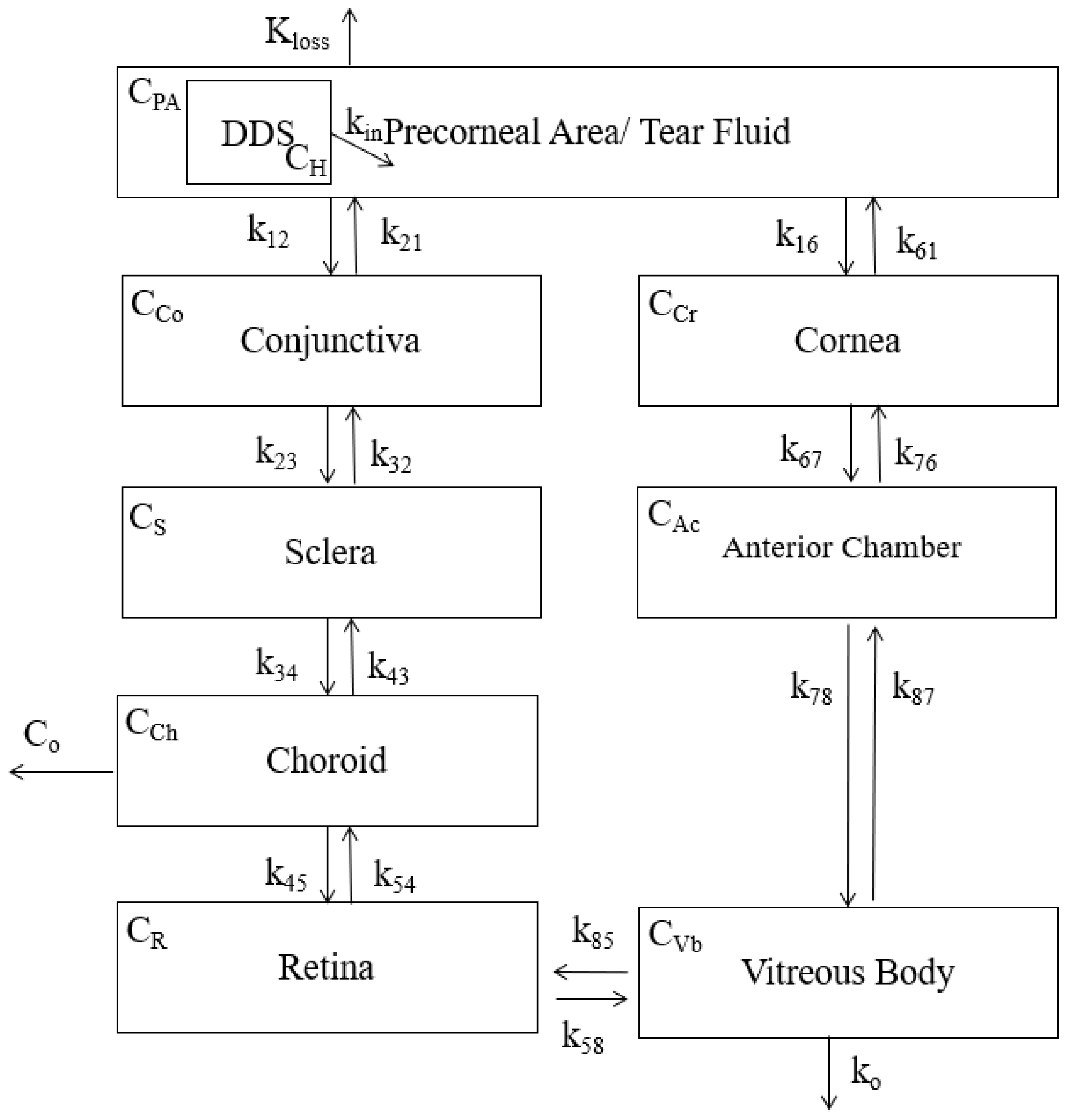
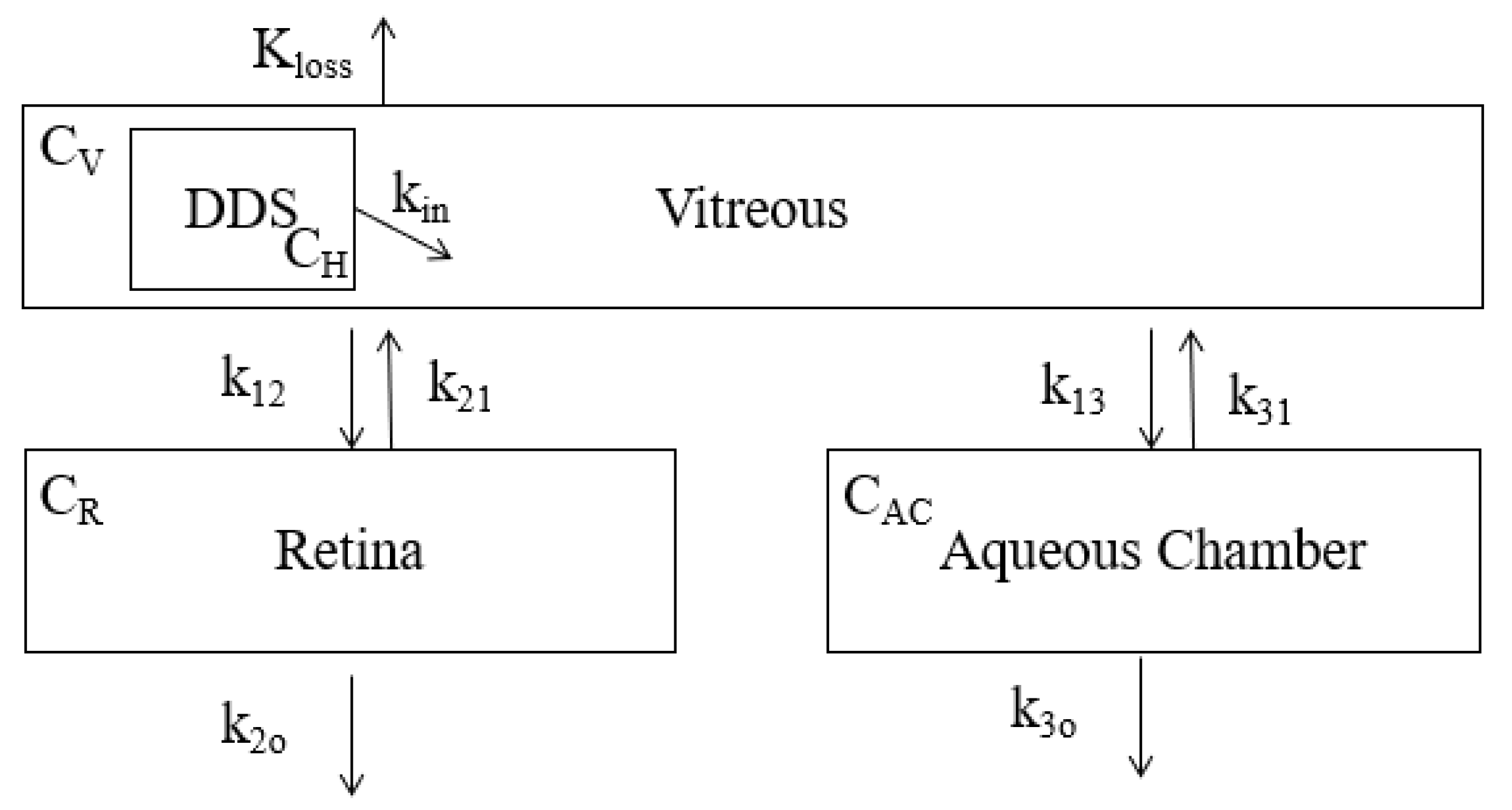
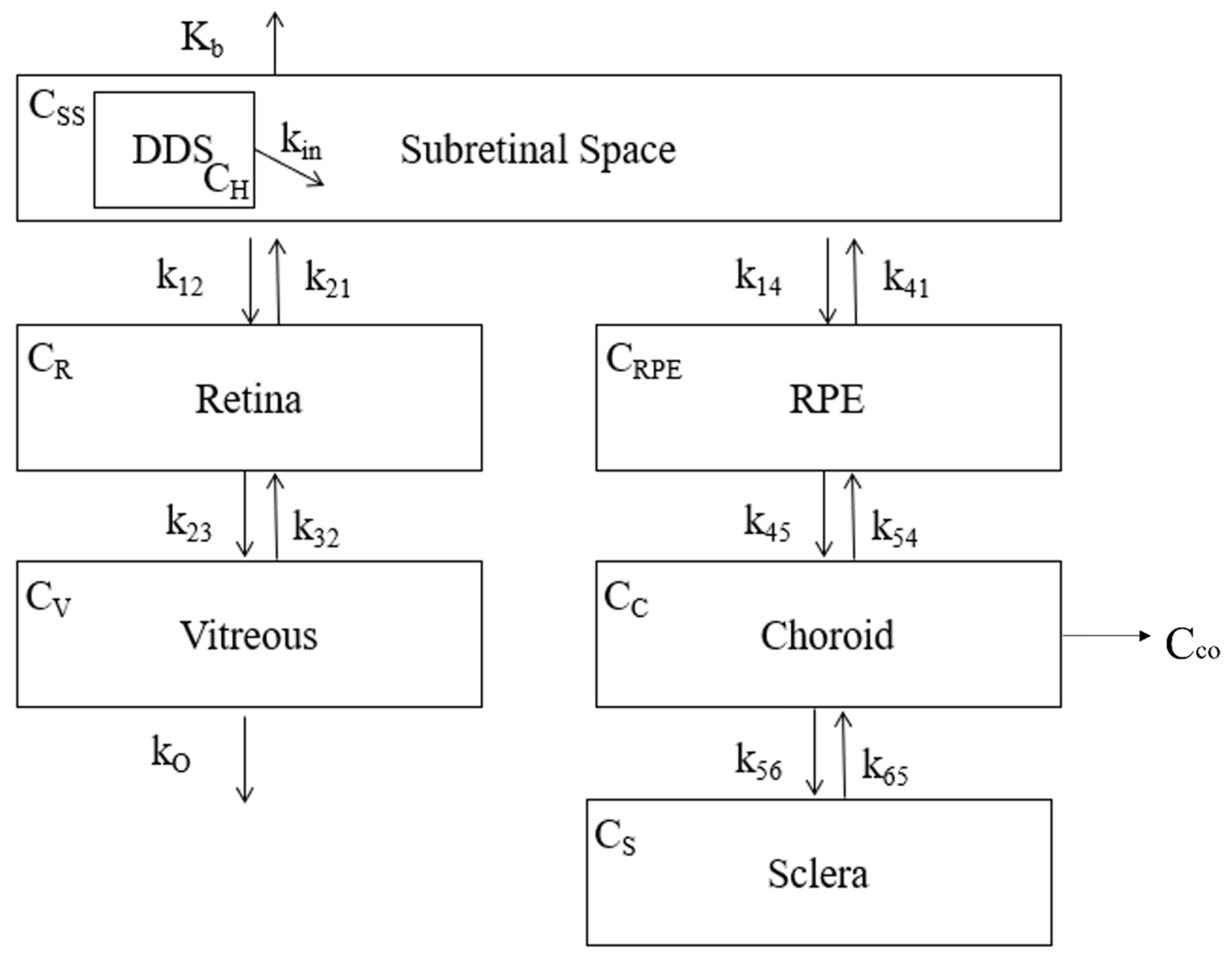
2.5. Compartmental Model
2.6. COMSOL Multiphysics Model
2.7. Statistical Analysis
3. Results
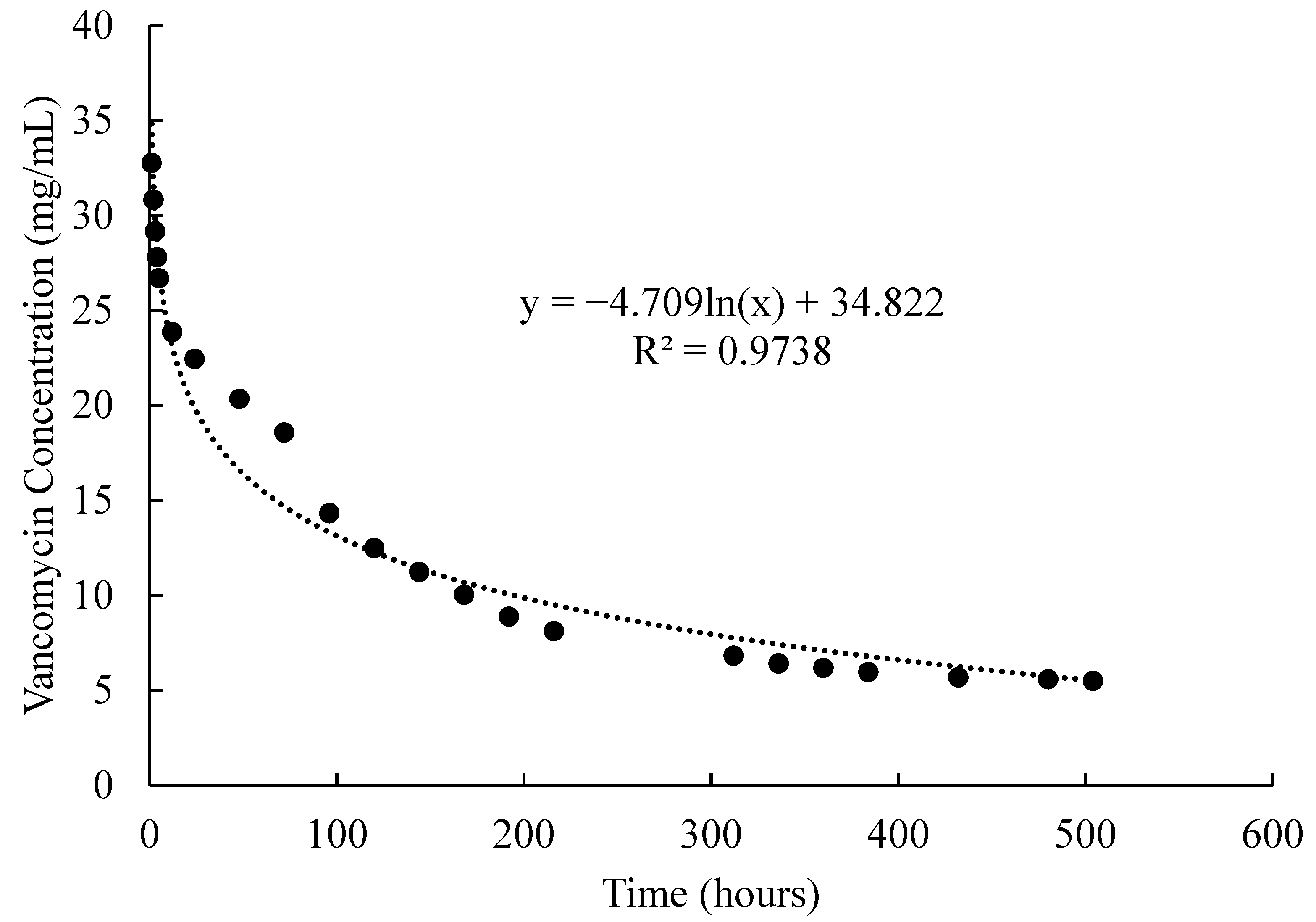
3.1. In Vitro Drug Delivery System Results
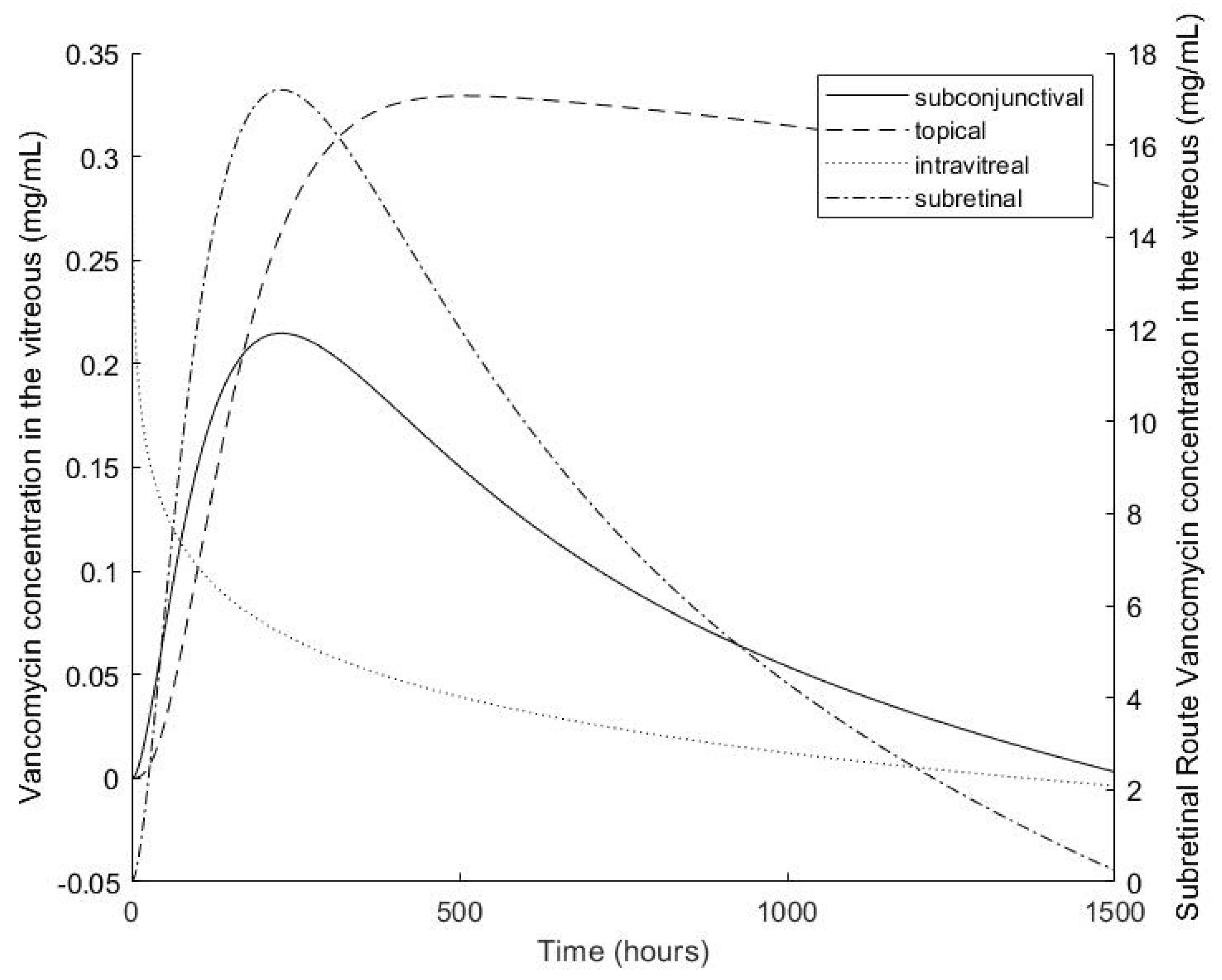
3.2. Compartmental Model
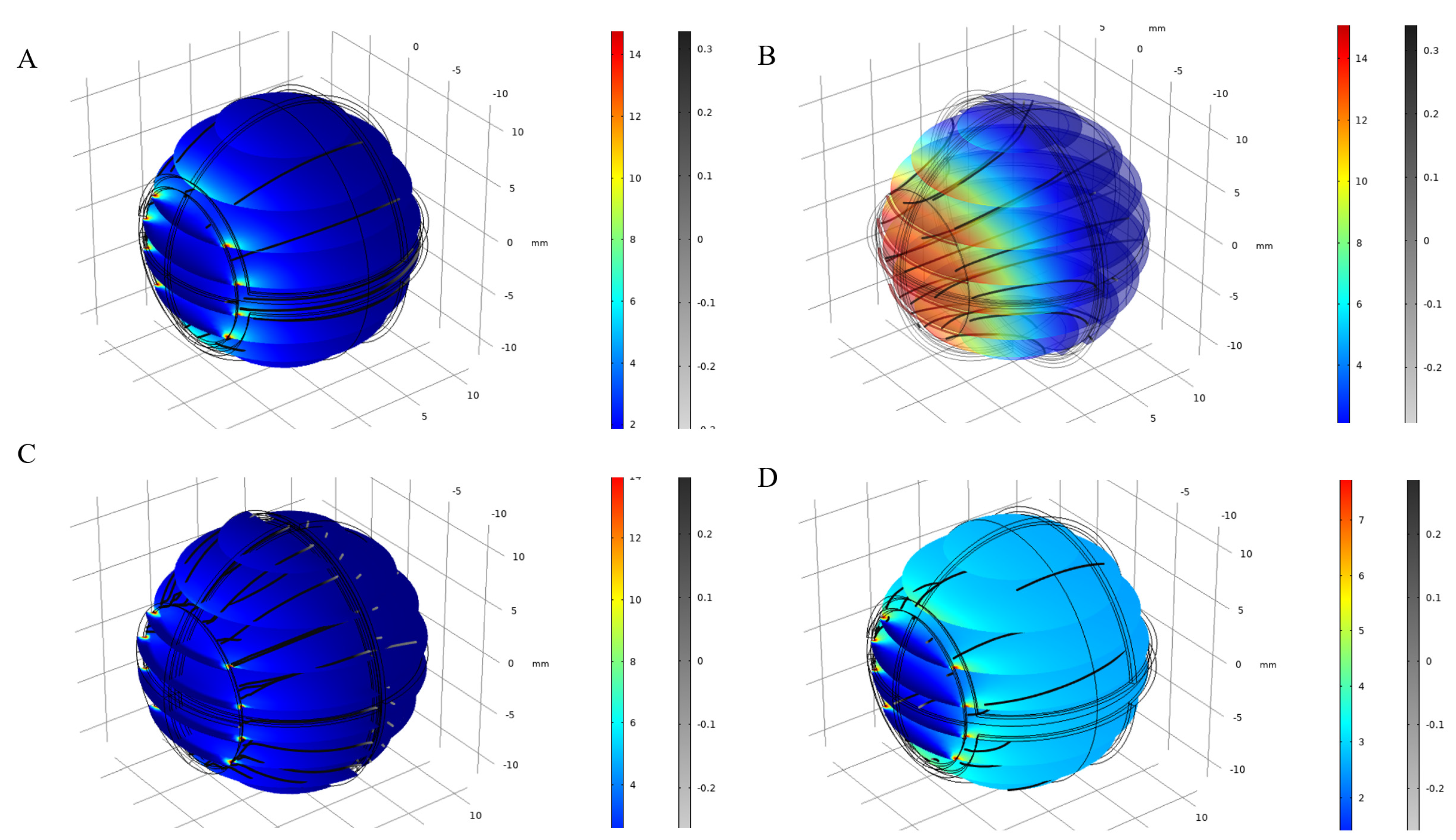
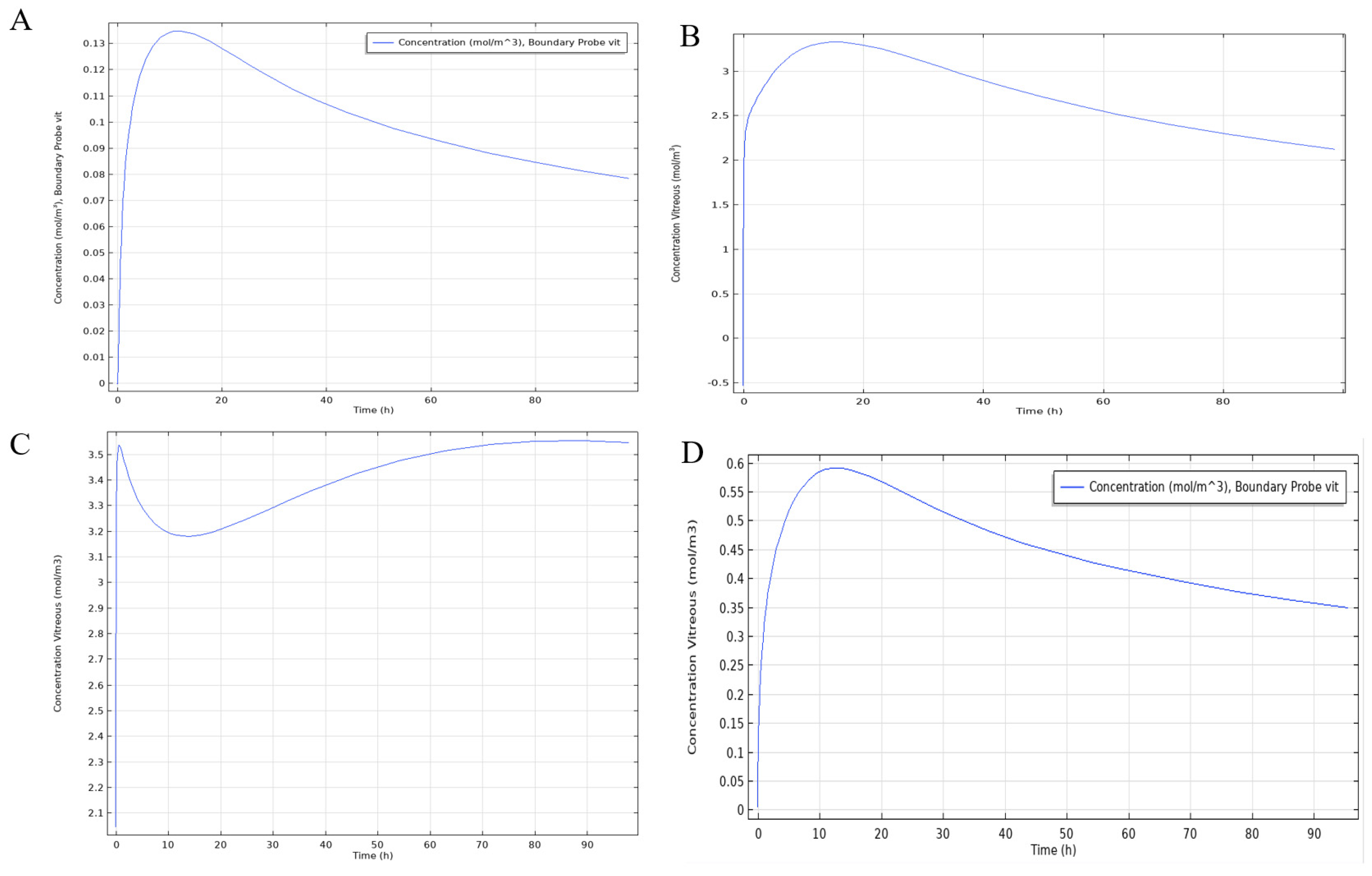
3.3. COMSOL Multiphysics Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang-Mieler, J.J.; Dosmar, E.; Liu, W.; Mieler, W.F. Extended ocular drug delivery systems for the anterior and posterior segments: Biomaterial options and applications. Expert Opin. Drug Deliv. 2016, 14, 611–620. [Google Scholar] [CrossRef]
- Geroski, D.H.; Edelhauser, H.F. Drug delivery for posterior segment eye disease. Investig. Ophthalmol. Vis. Sci. 2000, 41, 961–964. [Google Scholar]
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; et al. Ophthalmic Drug Delivery Systems for the Treatment of Retinal Diseases: Basic Research to Clinical Applications. Investig. Opthalmology Vis. Sci. 2010, 51, 5403–5420. [Google Scholar] [CrossRef]
- Ciolino, J.; Hoare, T.R.; Iwata, N.G.; Behlau, I.; Dohlman, C.H.; Langer, R.; Kohane, D.S. A Drug-Eluting Contact Lens. Investig. Opthalmology Vis. Sci. 2009, 50, 3346–3352. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M. Biopharmaceutical Considerations In Topical Ocular Drug Delivery. Clin. Exp. Pharmacol. Physiol. 2000, 27, 558–562. [Google Scholar] [CrossRef]
- Djebli, N.; Khier, S.; Griguer, F.; Coutant, A.-L.; Tavernier, A.; Fabre, G.; Leriche, C.; Fabre, D. Ocular Drug Distribution After Topical Administration: Population Pharmacokinetic Model in Rabbits. Eur. J. Drug Metab. Pharmacokinet. 2016, 42, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barza, M.; Kane, A.; Baum, J. The difficulty of determining the route of intraocular penetration of gentamicin after subconjunctival injection in the rabbit. Investig. Ophthalmol. Vis. Sci. 1981, 20, 509–514. [Google Scholar] [CrossRef]
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef]
- Lee, S.J.; He, W.; Robinson, S.B.; Robinson, M.R.; Csaky, K.G.; Kim, H. Evaluation of Clearance Mechanisms with Transscleral Drug Delivery. Investig. Opthalmology Vis. Sci. 2010, 51, 5205–5212. [Google Scholar] [CrossRef]
- Souli, M.; Kopsinis, G.; Kavouklis, E.; Gabriel, L.; Giamarellou, H. Vancomycin levels in human aqueous humour after intravenous and subconjunctival administration. Int. J. Antimicrob. Agents 2001, 18, 239–243. [Google Scholar] [CrossRef]
- Goel, M.; Picciani, R.G.; Lee, R.K.; Bhattacharya, S.K. Aqueous Humor Dynamics: A Review. Open Ophthalmol. J. 2010, 4, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choonara, Y.E.; Pillay, V.; Danckwerts, M.P.; Carmichael, T.R.; du Toit, L.C. A review of implantable intravitreal drug delivery technologies for the treatment of posterior segment eye diseases. J. Pharm. Sci. 2010, 99, 2219–2239. [Google Scholar] [CrossRef]
- Osswald, C.R.; Kang-Mieler, J.J. Controlled and Extended Release of a Model Protein from a Microsphere-Hydrogel Drug Delivery System. Ann. Biomed. Eng. 2015, 43, 2609–2617. [Google Scholar] [CrossRef]
- Peng, Y.; Tang, L.; Zhou, Y. Subretinal Injection: A Review on the Novel Route of Therapeutic Delivery for Vitreoretinal Diseases. Ophthalmic Res. 2017, 58, 217–226. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peynshaert, K.; Devoldere, J.; De Smedt, S.C.; Remaut, K. In vitro and ex vivo models to study drug delivery barriers in the posterior segment of the eye. Adv. Drug Deliv. Rev. 2018, 126, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.K.; Lee, D.S. Injectable Biodegradable Hydrogels. Macromol. Biosci. 2010, 10, 563–579. [Google Scholar] [CrossRef]
- West, J.L.; Hubbell, J. Photopolymerized hydrogel materials for drug delivery applications. React. Polym. 1995, 25, 139–147. [Google Scholar] [CrossRef]
- Zustiak, S.P.; Pubill, S.; Ribeiro, A.; Leach, J.B. Hydrolytically degradable poly(ethylene glycol) hydrogel scaffolds as a cell delivery vehicle: Characterization of PC12 cell response. Biotechnol. Prog. 2013, 29, 1255–1264. [Google Scholar] [CrossRef] [Green Version]
- Kumar, M.N.V.R.; Kumar, N. Polymeric Controlled Drug-Delivery Systems: Perspective Issues and Opportunities. Drug Dev. Ind. Pharm. 2001, 27, 1–30. [Google Scholar] [CrossRef]
- Bal, T.; Kepsutlu, B.; Kizilel, S. Characterization of protein release from poly(ethylene glycol) hydrogels with crosslink density gradients. J. Biomed. Mater. Res. Part A 2013, 102, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Akar, B.; Waller, T.; Larson, J.; Appel, A.; Brey, E. Design of a composite biomaterial system for tissue engineering applications. Acta Biomater. 2014, 10, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Drapala, P.W.; Jiang, B.; Chiu, Y.-C.; Mieler, W.F.; Brey, E.M.; Kang-Mieler, J.J.; Pérez-Luna, V.H. The Effect of Glutathione as Chain Transfer Agent in PNIPAAm-Based Thermo-responsive Hydrogels for Controlled Release of Proteins. Pharm. Res. 2013, 31, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.W.-Y.; Robinson, J.R. Drug Delivery to the Posterior Segment of the Eye IV: Theoretical Formulation of a Drug Delivery System for Subconjunctival Injection. J. Ocul. Pharmacol. Ther. 2009, 25, 29–38. [Google Scholar] [CrossRef]
- Lee, T.W.-Y.; Robinson, J.R. Drug Delivery to the Posterior Segment of the Eye III: The Effect of Parallel Elimination Pathway on the Vitreous Drug Level After Subconjunctival Injection. J. Ocul. Pharmacol. Ther. 2004, 20, 55–64. [Google Scholar] [CrossRef]
- Lee, T.W.-Y.; Robinson, J.R. Drug Delivery to the Posterior Segment of the Eye II: Development and Validation of a Simple Pharmacokinetic Model for Subconjunctival Injection. J. Ocul. Pharmacol. Ther. 2004, 20, 43–53. [Google Scholar] [CrossRef]
- Lee, T.W.-Y.; Robinson, J.R. Drug Delivery to the Posterior Segment of the Eye: Some Insights on the Penetration Pathways after Subconjunctival Injection. J. Ocul. Pharmacol. Ther. 2001, 17, 565–572. [Google Scholar] [CrossRef]
- Derwent, J.J.K.; Mieler, W.F. Thermoresponsive Hydrogels as a New Ocular Drug Delivery Platform to The Posterior Segment of the Eye. Trans. Am. Ophthalmol. Soc. 2008, 106, 206–214. [Google Scholar]
- Brey, H.H.E.; Kang-Mieler, J.J. Thermo-Responsive Hydrogel Compositions. U.S. Patent US20140065226A1, 5 March 2012. [Google Scholar]
- Drapala, P.W.; Brey, E.M.; Mieler, W.F.; Venerus, D.C.; Derwent, J.J.K.; Pérez-Luna, V.H. Role of Thermo-responsiveness and Poly(ethylene glycol) Diacrylate Cross-link Density on Protein Release from Poly(N-isopropylacrylamide) Hydrogels. J. Biomater. Sci. Polym. Ed. 2011, 22, 59–75. [Google Scholar] [CrossRef]
- Deshmukh, M.; Singh, Y.; Gunaseelan, S.; Gao, D.; Stein, S.; Sinko, P.J. Biodegradable poly(ethylene glycol) hydrogels based on a self-elimination degradation mechanism. Biomaterials 2010, 31, 6675–6684. [Google Scholar] [CrossRef] [Green Version]
- Honary, S.; Ebrahimi, P.; Hadianamrei, R. Optimization of size and encapsulation efficiency of 5-FU loaded chitosan nanoparticles by response surface methodology. Curr. Drug Deliv. 2013, 10, 742–752. [Google Scholar] [CrossRef]
- Honary, S.; Ebrahimi, P.; Hadianamrei, R. Optimization of particle size and encapsulation efficiency of vancomycin nanoparticles by response surface methodology. Pharm. Dev. Technol. 2013, 19, 987–998. [Google Scholar] [CrossRef] [PubMed]
- Ranta, V.-P.; Mannermaa, E.; Lummepuro, K.; Subrizi, A.; Laukkanen, A.; Antopolsky, M.; Murtomäki, L.; Hornof, M.; Urtti, A. Barrier analysis of periocular drug delivery to the posterior segment. J. Control. Release 2010, 148, 42–48. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Noonan, J.S. Permeability of cornea, sclera, and conjunctiva: A literature analysis for drug delivery to the eye. J. Pharm. Sci. 1998, 87, 1479–1488. [Google Scholar] [CrossRef]
- Ambati, J.; Canakis, C.S.; Miller, J.W.; Gragoudas, E.S.; Edwards, A.; Weissgold, D.J.; Kim, I.; Delori, F.C.; Adamis, A.P. Diffusion of high molecular weight compounds through sclera. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1181–1185. [Google Scholar]
- Maurice, D.; Polgar, J. Diffusion across the sclera. Exp. Eye Res. 1977, 25, 577–582. [Google Scholar] [CrossRef]
- Olsen, T.W.; Edelhauser, H.F.; Lim, J.I.; Geroski, D.H. Human scleral permeability: Effects of age, cryotherapy, transscleral diode laser, and surgical thinning. Investig. Ophthalmol. Vis. Sci. 1995, 39, 1893–1903. [Google Scholar] [CrossRef] [Green Version]
- Pitkänen, L.; Ranta, V.-P.; Moilanen, H.; Urtti, A. Permeability of Retinal Pigment Epithelium: Effects of Permeant Molecular Weight and Lipophilicity. Investig. Opthalmology Vis. Sci. 2005, 46, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.E.; Pridgen, T.A.; Csaky, K.G. Episcleral clearance of sodium fluorescein from a bioerodible sub-tenon’s implant in the rat. Exp. Eye Res. 2010, 90, 501–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, M.R.; Lee, S.S.; Kim, H.; Kim, S.; Lutz, R.J.; Galban, C.; Bungay, P.M.; Yuan, P.; Wang, N.S.; Kim, J.; et al. A rabbit model for assessing the ocular barriers to the transscleral delivery of triamcinolone acetonide. Exp. Eye Res. 2006, 82, 479–487. [Google Scholar] [CrossRef]
- Le Merdy, M.; Fan, J.; Bolger, M.B.; Lukacova, V.; Spires, J.; Tsakalozou, E.; Patel, V.; Xu, L.; Stewart, S.; Chockalingam, A.; et al. Application of Mechanistic Ocular Absorption Modeling and Simulation to Understand the Impact of Formulation Properties on Ophthalmic Bioavailability in Rabbits: A Case Study Using Dexamethasone Suspension. AAPS J. 2019, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular Drug Delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Dosmar, E.; Liu, W.; Patel, G.; Rogozinski, A.; Mieler, W.F.; Kang-Mieler, J.J. Controlled Release of Vancomycin from a Thermoresponsive Hydrogel System for the Prophylactic Treatment of Postoperative Acute Endophthalmitis. Transl. Vis. Sci. Technol. 2019, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Hutton-Smith, L.A.; Gaffney, E.; Byrne, H.M.; Maini, P.K.; Schwab, D.; Mazer, N.A. A Mechanistic Model of the Intravitreal Pharmacokinetics of Large Molecules and the Pharmacodynamic Suppression of Ocular Vascular Endothelial Growth Factor Levels by Ranibizumab in Patients with Neovascular Age-Related Macular Degeneration. Mol. Pharm. 2016, 13, 2941–2950. [Google Scholar] [CrossRef]
- Barry, S.G.P.; Cordoves, L. ESCRS Guidelines for Prevention and Treatment of Endophthalmitis Following Cataract Surgery: Data, Dilemmas and Conclusions; Temple House: Dublin, UK, 2013; p. 52. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Values (hr−1) | Rationale |
|---|---|---|
| Drug permeation across the cornea | 0.0216 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the conjunctiva | 0.0018 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the aqueous chamber | 0.0189 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the iris and ciliary | 3.6 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the sclera | 0.05472 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the choroid | 1.782 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the retina | 1.782 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the vitreous humor | 0.0234 | Parameter values implemented in an ocular compartmental absorption and transmit model of dexamethasone [42] |
| Drug permeation across the RPE | 0.000936 | Derived values used in modeling the intravitreal pharmacokinetics of antibody fragments [45] |
| Drug elimination from the vitreous | 0.008208 | Derived values used in modeling the intravitreal pharmacokinetics of antibody fragments [45] |
| Drug elimination from systemic absorption | 0.0329 | Parameter values implemented in am ocular compartmental absorption and transmit model of dexamethasone [42] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dosmar, E.; Vuotto, G.; Su, X.; Roberts, E.; Lannoy, A.; Bailey, G.J.; Mieler, W.F.; Kang-Mieler, J.J. Compartmental and COMSOL Multiphysics 3D Modeling of Drug Diffusion to the Vitreous Following the Administration of a Sustained-Release Drug Delivery System. Pharmaceutics 2021, 13, 1862. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13111862
Dosmar E, Vuotto G, Su X, Roberts E, Lannoy A, Bailey GJ, Mieler WF, Kang-Mieler JJ. Compartmental and COMSOL Multiphysics 3D Modeling of Drug Diffusion to the Vitreous Following the Administration of a Sustained-Release Drug Delivery System. Pharmaceutics. 2021; 13(11):1862. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13111862
Chicago/Turabian StyleDosmar, Emily, Gabrielle Vuotto, Xingqi Su, Emily Roberts, Abigail Lannoy, Garet J. Bailey, William F. Mieler, and Jennifer J. Kang-Mieler. 2021. "Compartmental and COMSOL Multiphysics 3D Modeling of Drug Diffusion to the Vitreous Following the Administration of a Sustained-Release Drug Delivery System" Pharmaceutics 13, no. 11: 1862. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13111862