
Enhanced Transdermal Delivery of Bisoprolol Hemifumarate via Combined Effect of Iontophoresis and Chemical Enhancers: Ex Vivo Permeation/In Vivo Pharmacokinetic Studies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Determination of BH Using HPLC
2.2.2. Preparation of BH Hydrogels
3. Evaluation of BH Gels
3.1. Physical Appearance
3.2. Drug Content Determination of BH Hydrogels
3.3. pH Determination of BH Hydrogels
3.4. Rheological Measurements
4. Preparation of Skin Membranes
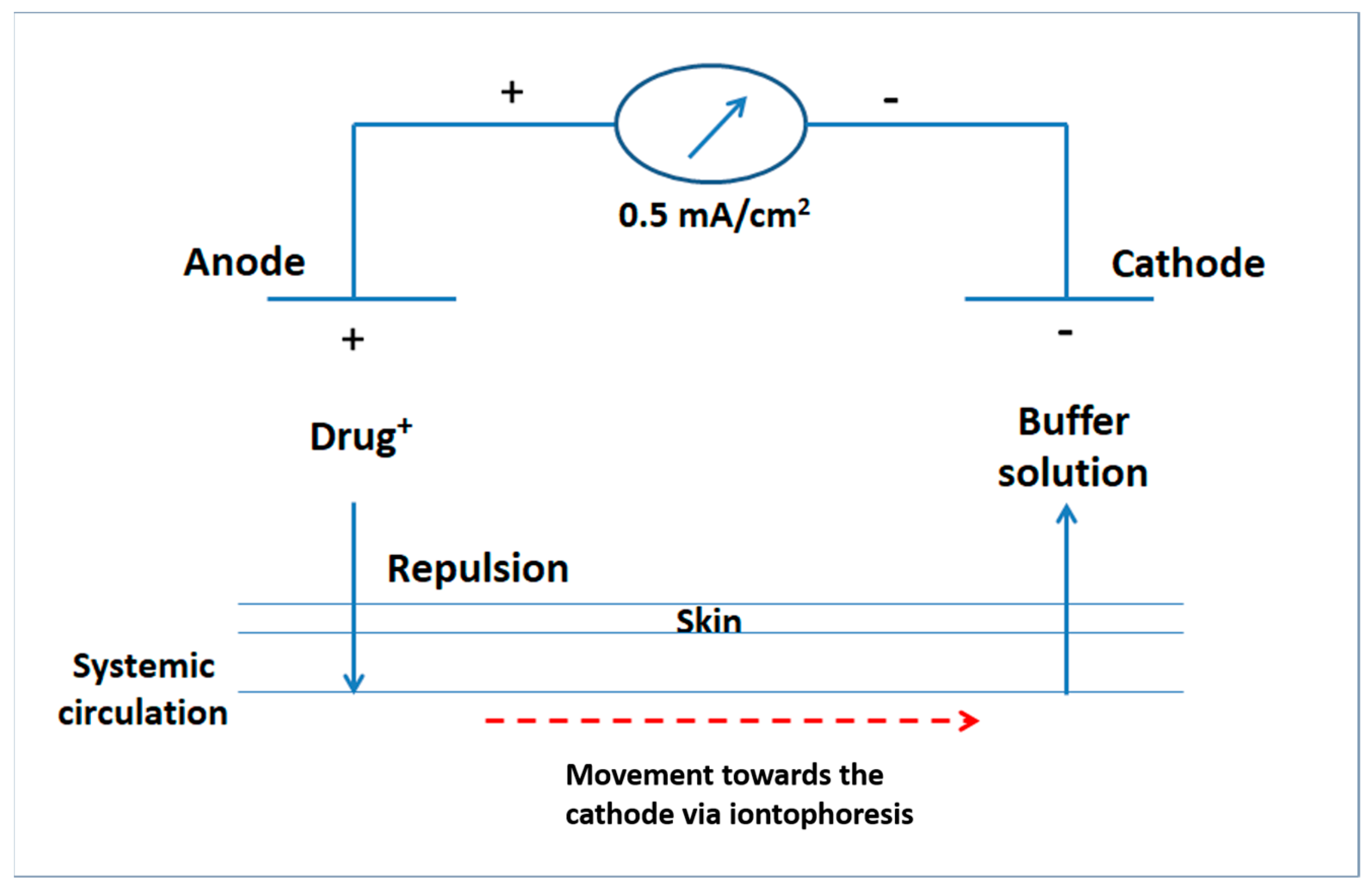
5. Custom-Made Iontophoretic Device
6. Ex Vivo Permeation Studies
7. Pharmacokinetic Study
7.1. Study Design and Subjects
7.2. Sample Collection
7.3. Sample Preparation
7.4. LC-ESI/MS Assay of BH
7.5. Pharmacokinetic and Statistical Analysis
8. Results and Discussion
8.1. Physical Appearance, Drug Content and pH
8.2. Rheological Properties of BH Hydrogels
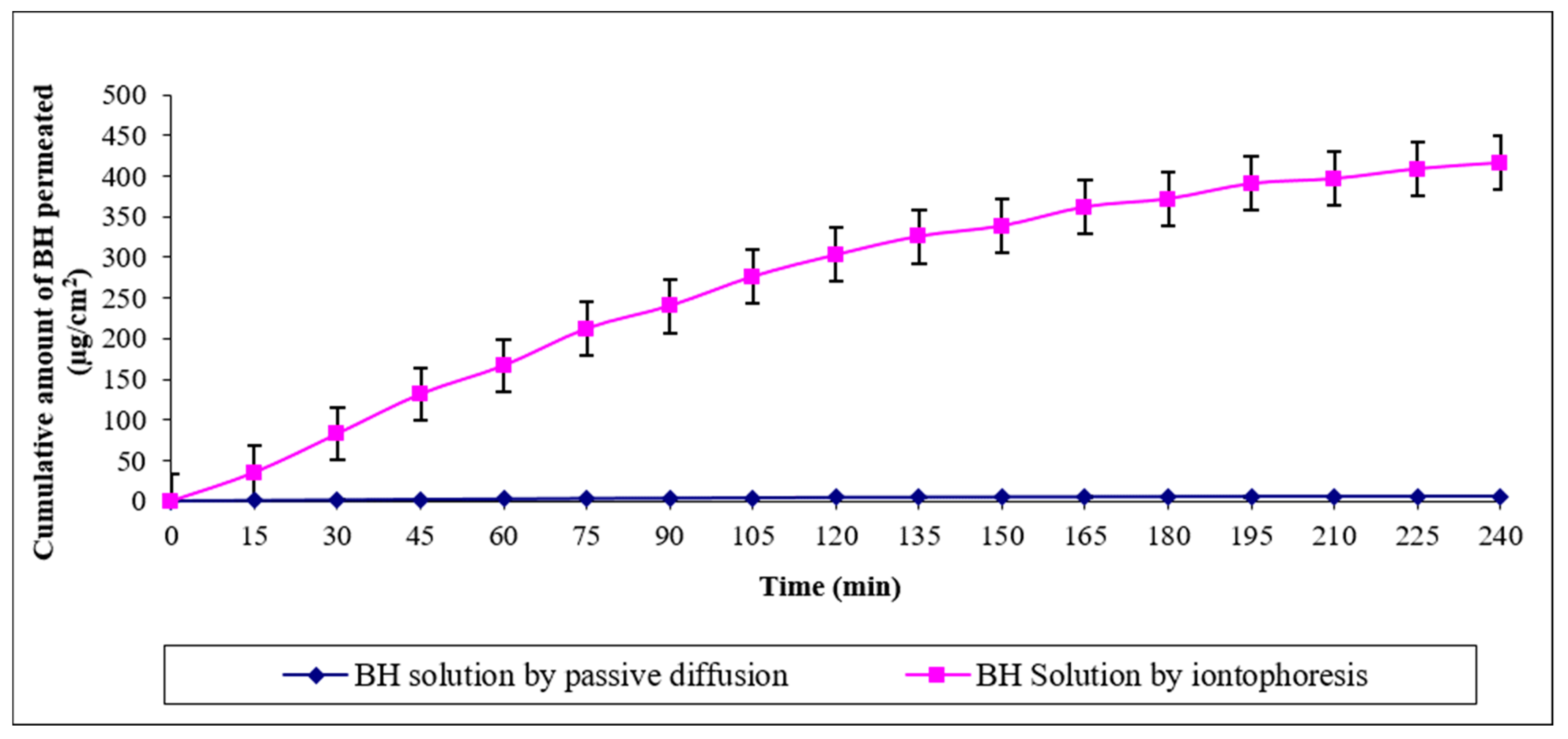
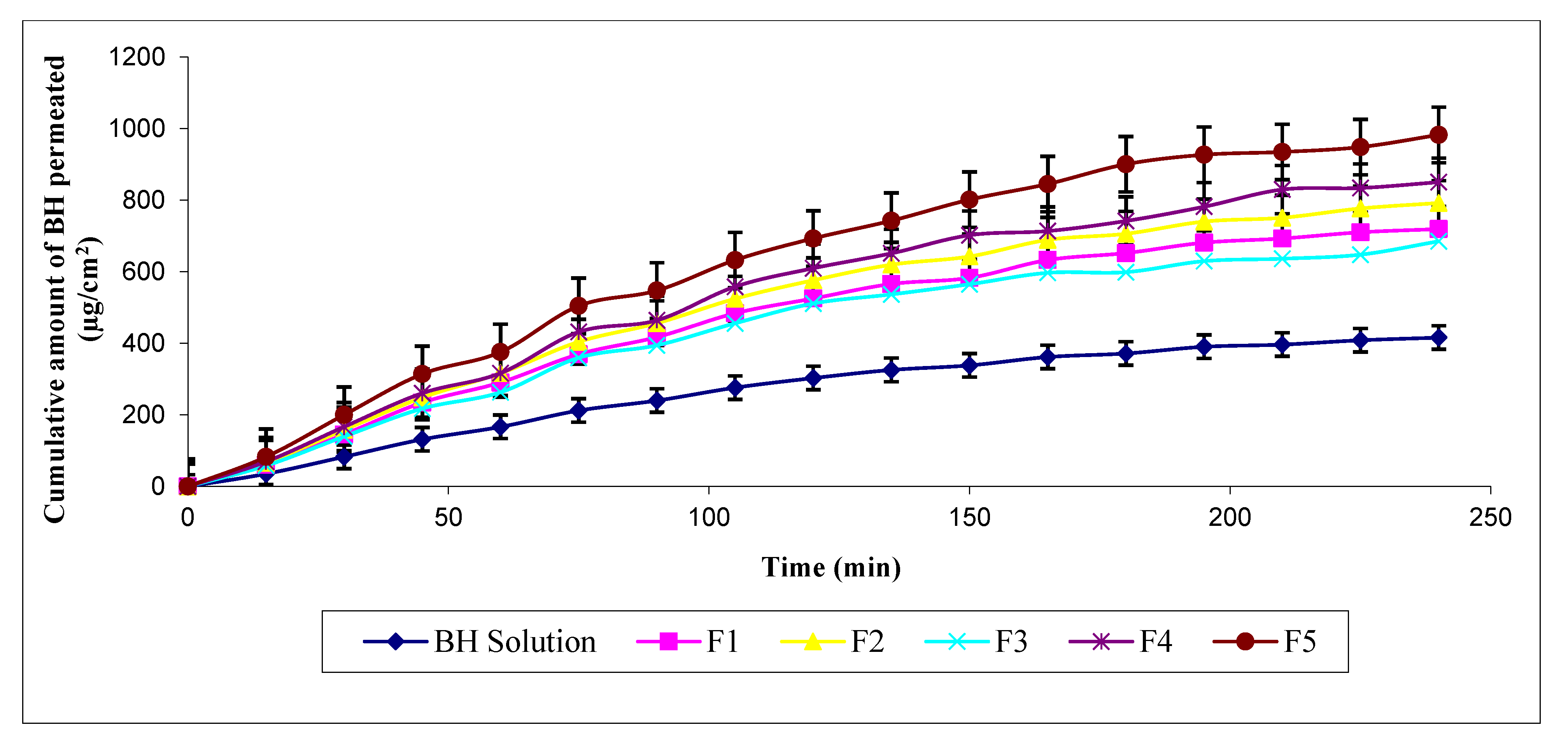
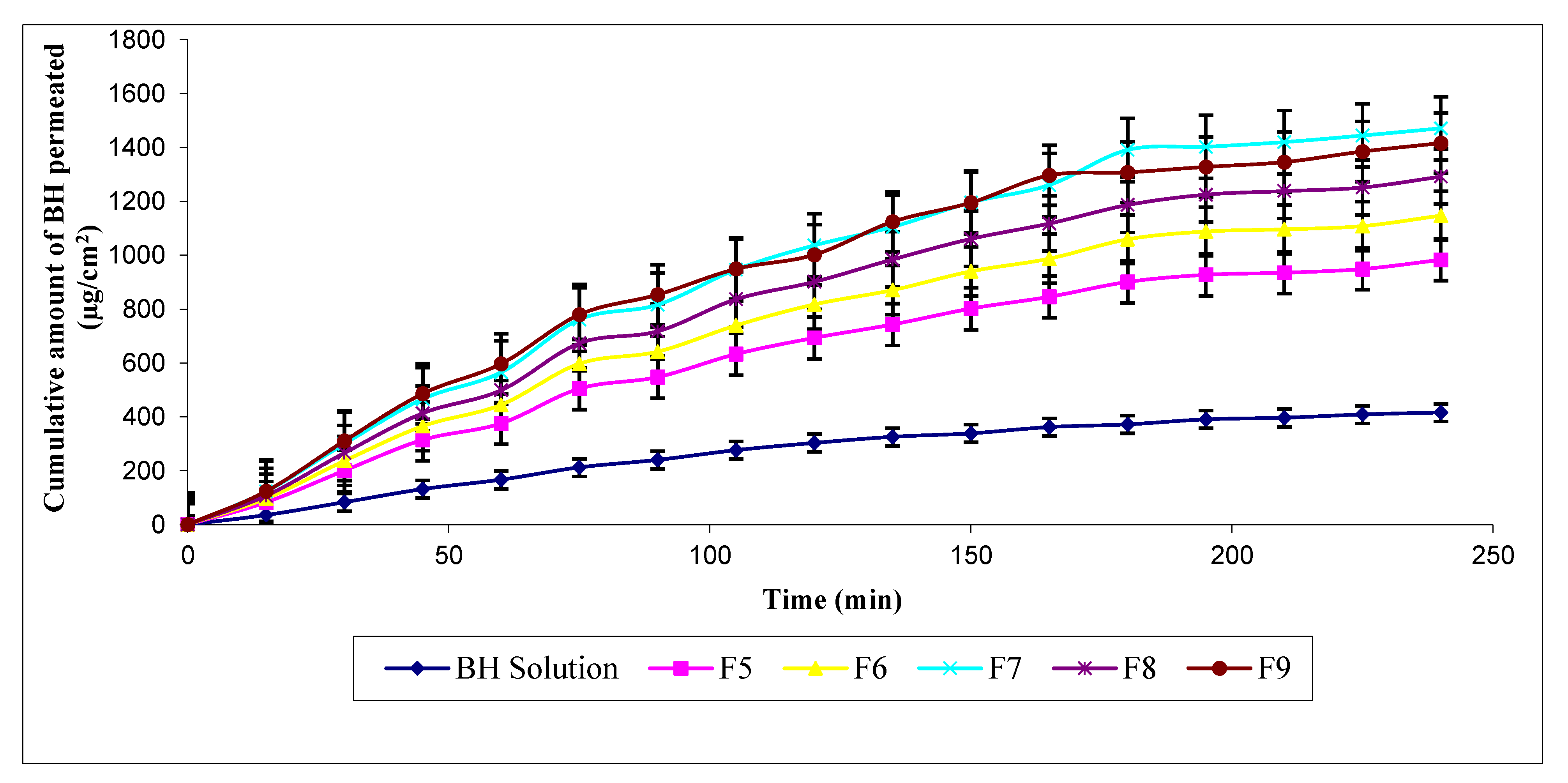
8.3. Ex Vivo Permeation of BH through Rat Skin
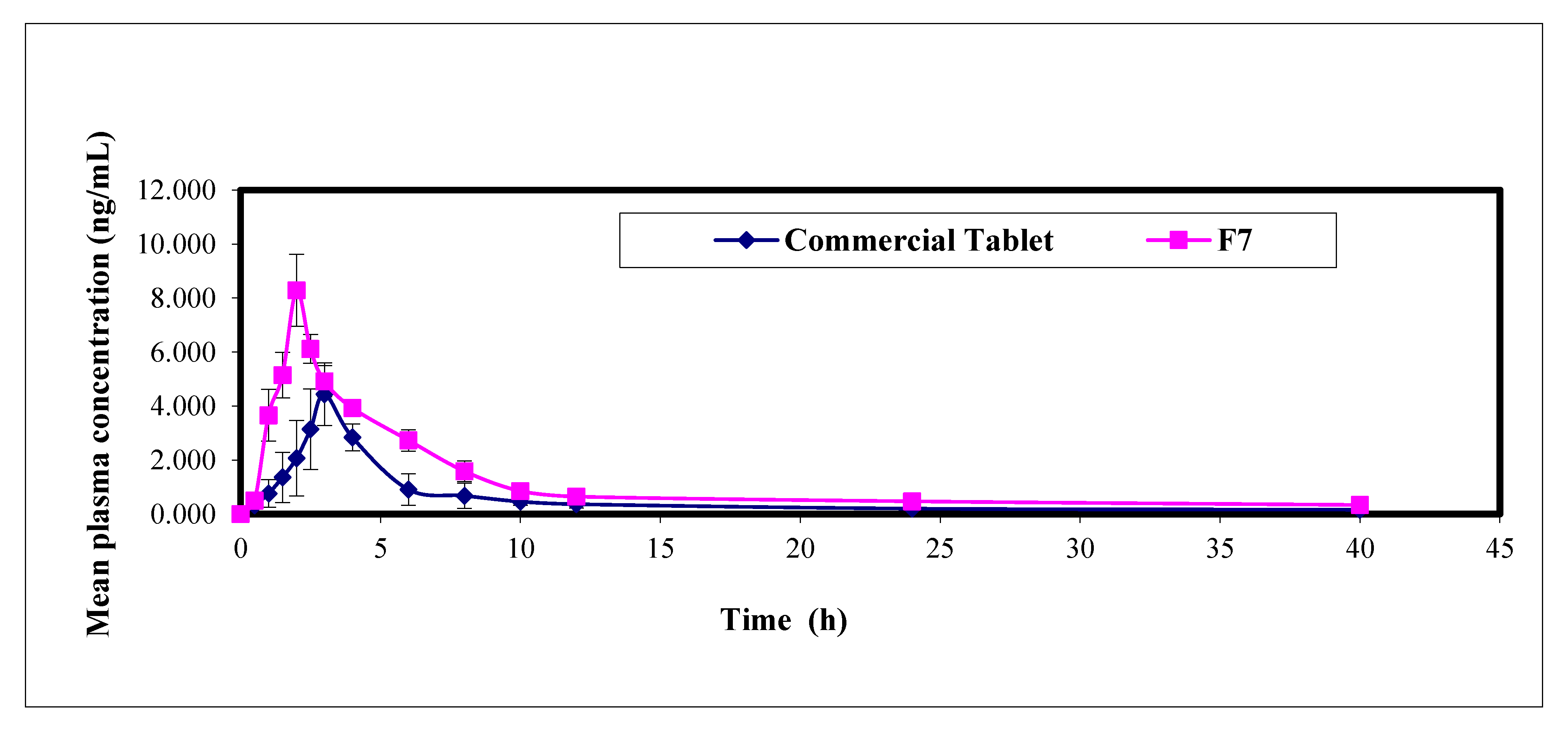
9. Pharmacokinetic Study in Healthy Human Volunteers
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lionakis, N.; Mendrinos, D.; Sanidas, E.; Favatas, G.; Georgopoulou, M. Hypertension in the elderly. World J. Cardiol. 2012, 4, 135. [Google Scholar] [CrossRef]
- Nicolas, R.R.; Juan, F.M. Hypertension in the elderly. Cardiovasc. Hematol. Agents Med. Chem. Former. Curr. Med. Chem. Cardiovasc. Hematol. Agents 2014, 12, 136–145. [Google Scholar] [CrossRef]
- Malakar, J.; Nayak, A.K.; Goswami, S. Use of response surface methodology in the formulation and optimization of bisoprolol fumarate matrix tablets for sustained drug release. Int. Sch. Res. Not. 2012, 2012, 730624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Nabarawi, M.A.; Tayel, S.A.; Soliman, N.A.; Enin, H.A.A. Development and evaluation of fixed dose bi therapy sublingual tablets for treatment stress hypertension and anxiety. J. Pharm. Bioallied Sci. 2013, 5, 191. [Google Scholar] [PubMed]
- Tayel, S.A.; Foda, N.; Louis, D. Bisoprolol Hemifumarate Matrix Tablets for Sustained Release: Preparation and Evaluation; Inventi Journals Pvt.Ltd: Bhopal, India, 2018; Volume 2018. [Google Scholar]
- Malaak, F.A.; Abu Zeid, K.; Fouad, S.A.; El-Nabarawi, M.A. Orodispersible Tablets: Novel Strategies and future challenges in Drug Delivery. Res. J. Pharm. Technol. 2019, 12, 5575–5582. [Google Scholar] [CrossRef]
- Elshafeey, A.H.; Kamel, A.O.; Fathallah, M.M. Utility of nanosized microemulsion for transdermal delivery of tolterodine tartrate: Ex-vivo permeation and in-vivo pharmacokinetic studies. Pharm. Res. 2009, 26, 2446–2453. [Google Scholar] [CrossRef]
- Rastogi, V.; Yadav, P. Transdermal drug delivery system: An overview. AJP Free Full Text Artic. Asian J. Pharm. 2014, 6. [Google Scholar] [CrossRef]
- Panchagnula, R.; Desu, H.; Jain, A.; Khandavilli, S. Effect of lipid bilayer alteration on transdermal delivery of a high-molecular-weight and lipophilic drug: Studies with paclitaxel. J. Pharm. Sci. 2004, 93, 2177–2183. [Google Scholar] [CrossRef] [PubMed]
- Funke, A.P.; Schiller, R.; Motzkus, H.W.; Günther, C.; Müller, R.H.; Lipp, R. Transdermal delivery of highly lipophilic drugs: In vitro fluxes of antiestrogens, permeation enhancers, and solvents from liquid formulations. Pharm. Res. 2002, 19, 661–668. [Google Scholar] [CrossRef]
- Kharshoum, R.M.; Ali, A.A. Development of Sublingual tablets of Bisoprolol Hemifumarate/Hydroxypropyl-[beta]-Cyclodextrin Complex for Potential treatment of Angina Pectoris. Int. J. Drug Deliv. 2012, 4, 484. [Google Scholar]
- Hadgraft, J. Recent developments in topical and transdermal delivery. Eur. J. Drug Metab. Pharmacokinet. 1996, 21, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Kankkunen, T.; Sulkava, R.; Vuorio, M.; Kontturi, K.; Hirvonen, J. Transdermal iontophoresis of tacrine in vivo. Pharm. Res. 2002, 19, 704. [Google Scholar] [CrossRef] [PubMed]
- Dhote, V.; Bhatnagar, P.; Mishra, P.K.; Mahajan, S.C.; Mishra, D.K. Iontophoresis: A potential emergence of a transdermal drug delivery system. Sci. Pharm. 2012, 80, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cázares-Delgadillo, J.; Balaguer-Fernandez, C.; Calatayud-Pascual, A.; Ganem-Rondero, A.; Quintanar-Guerrero, D.; Lopez-Castellano, A.C.; Merino, V.; Kalia, Y.N. Transdermal iontophoresis of dexamethasone sodium phosphate in vitro and in vivo: Effect of experimental parameters and skin type on drug stability and transport kinetics. Eur. J. Pharm. Biopharm. 2010, 75, 173–178. [Google Scholar] [CrossRef]
- Hegde, A.R.; Rewatkar, V.P.; Manikkath, J.; Tupally, K.; Parekh, H.S.; Mutalik, S. Peptide dendrimer-conjugates of ketoprofen: Synthesis and ex vivo and in vivo evaluations of passive diffusion, sonophoresis and iontophoresis for skin delivery. Eur. J. Pharm. Sci. 2017, 102, 237–249. [Google Scholar] [CrossRef] [Green Version]
- Manjunatha, R.G.; Prasad, R.; Sharma, S.; Narayan, R.P.; Koul, V. Iontophoretic delivery of lidocaine hydrochloride through ex-vivo human skin. J. Dermatol. Treat. 2019, 31, 191–199. [Google Scholar] [CrossRef]
- Sklenář, Z.; Vitková, Z.; Herdová, P.; Horáčková, K.; Šimunková, V. Formulation and release of alaptide from cellulose-based hydrogels. Acta Vet. Brno 2013, 81, 301–306. [Google Scholar] [CrossRef] [Green Version]
- El-Assal, M. Proniosomes as nano-carrier for transdermal delivery of atenolol niosomal gel. Int. J. Drug Deliv. Technol. 2017, 7, 283–297. [Google Scholar]
- Fouad, S.A.; Basalious, E.B.; El-Nabarawi, M.A.; Tayel, S.A. Microemulsion and poloxamer microemulsion-based gel for sustained transdermal delivery of diclofenac epolamine using in-skin drug depot: In vitro/in vivo evaluation. Int. J. Pharm. 2013, 453, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.B.; Udupa, N. Investigation into the potential of iontophoresis facilitated delivery of ketorolac. Int. J. Pharm. 2003, 260, 93–103. [Google Scholar] [CrossRef]
- Teaima, M.H.; Abd El-Rehim, R.A.; El-Setouhy, D.A.; El-Nabarawi, M.A.; Jasti, B.R. Electrically assisted transdermal delivery of escin. Int. J. Pharm. Pharm. Sci. 2012, 4, 663–672. [Google Scholar]
- Fouad, S.A.; Shamma, R.N.; Basalious, E.B.; El-Nabarawi, M.A.; Tayel, S.A. Novel instantly-soluble transmucosal matrix (ISTM) using dual mechanism solubilizer for sublingual and nasal delivery of dapoxetine hydrochloride: In-vitro/in-vivo evaluation. Int. J. Pharm. 2016, 505, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Panzade, P.; Heda, A.; Puranik, P.; Patni, M.; Mogal, V. Enhanced transdermal delivery of granisetron by using iontophoresis. Iran. J. Pharm. Res. 2012, 11, 503. [Google Scholar]
- Karavasili, C.; Komnenou, A.; Katsamenis, O.L.; Charalampidou, G.; Kofidou, E.; Andreadis, D.; Koutsopoulos, S.; Fatouros, D.G. Self-assembling peptide nanofiber hydrogels for controlled ocular delivery of timolol maleate. ACS Biomater. Sci. Eng. 2017, 3, 3386–3394. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Zhou, X.; Guo, X.; Song, Q.; He, J.; Xu, G. LC–ESI-MS method for the determination of bisoprolol in human plasma. J. Pharm. Biomed. Anal. 2007, 44, 520–525. [Google Scholar] [CrossRef]
- Basalious, E.B.; El-Sebaie, W.; El-Gazayerly, O. Rapidly absorbed orodispersible tablet containing molecularly dispersed felodipine for management of hypertensive crisis: Development, optimization and in vitro/in vivo studies. Pharm. Dev. Technol. 2013, 18, 407–416. [Google Scholar] [CrossRef]
- Nair, V.B.; Panchagnula, R. Effect of iontophoresis and fatty acids on permeation of arginine vasopressin through rat skin. Pharmacol. Res. 2003, 47, 563–569. [Google Scholar] [CrossRef]
- Jadoul, A.; Doucet, J.; Durand, D.; Préat, V. Modifications induced on stratum corneum structure after in vitro iontophoresis: ATR-FTIR and X-ray scattering studies. J. Control. Release 1996, 42, 165–173. [Google Scholar] [CrossRef]
- Al-Khalili, M.; Meidan, V.M.; Michniak, B.B. Iontophoretic transdermal delivery of buspirone hydrochloride in hairless mouse skin. AAPS Pharmsci. 2003, 5, 61–71. [Google Scholar] [CrossRef]
- El Fawal, G.; Hong, H.; Song, X.; Wu, J.; Sun, M.; He, C.; Mo, X.; Jiang, Y.; Wang, H. Fabrication of antimicrobial films based on hydroxyethylcellulose and ZnO for food packaging application. Food Packag. Shelf Life 2020, 23, 100462. [Google Scholar] [CrossRef]
- Raghavan, S.; Trividic, A.; Davis, A.F.; Hadgraft, J. Effect of cellulose polymers on supersaturation and in vitro membrane transport of hydrocortisone acetate. Int. J. Pharm. 2000, 193, 231–237. [Google Scholar] [CrossRef]
- Gannu, R.; Vishnu, Y.V.; Kishan, V.; Rao, Y.M. Development of nitrendipine transdermal patches: In vitro and ex vivo characterization. Curr. Drug Deliv. 2007, 4, 69–76. [Google Scholar] [CrossRef]
- Fiume, M.M.; Bergfeld, W.M.; Belsito, D.V.; Hill, R.A.; Klaassen, C.D.; Liebler, D.C.; Marks, J.G.; Shank, R.C.; Slaga, T.J.; Synder, P.W.; et al. Safety assessment of pegylated alkyl glycerides as used in cosmetics. Int. J. Toxicol. 2020, 39 (Suppl. 2), 26S–58S. [Google Scholar] [CrossRef]
- Kreilgaard, M.; Pedersen, E.J.; Jaroszewski, J.W. NMR characterisation and transdermal drug delivery potential of microemulsion systems. J. Control. Release 2000, 69, 421–433. [Google Scholar] [CrossRef]
- Gannu, R.; Vishnu, Y.V.; Kishan, V.; Rao, Y.M. In vitro permeation of carvedilol through porcine skin: Effect of vehicles and penetration enhancers. PDA J. Pharm. Sci. Technol. 2008, 62, 256–263. [Google Scholar]
- Shah, P.P.; Desai, P.R.; Patlolla, R.; Klevans, L.; Singh, M. Effect of combination of hydrophilic and lipophilic permeation enhancers on the skin permeation of kahalalide F. J. Pharm. Pharmacol. 2014, 66, 760–768. [Google Scholar] [CrossRef]
- Pandey, A.; Mittal, A.; Chauhan, N.; Alam, S. Role of surfactants as penetration enhancer in transdermal drug delivery system. J. Mol. Pharm. Org. Process. Res. 2014, 2, 2–7. [Google Scholar] [CrossRef]
- Mariani, E.; Villa, C.; Neuhoff, C. Derivatization Procedure and HPLC Determination of 2-Ethoxyethanol in Cosmetic Samples. Int. J. Cosmet. Sci. 1999, 21, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Copestake, P.; World Health Organization. Selected 2-Alkoxyethanols; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Mura, P.; Faucci, M.T.; Bramanti, G.; Corti, P. Evaluation of transcutol as a clonazepam transdermal permeation enhancer from hydrophilic gel formulations. Eur. J. Pharm. Sci. 2000, 9, 365–372. [Google Scholar] [CrossRef]
- Manconi, M.; Caddeo, C.; Sinico, C.; Valenti, D.; Mostallino, M.C.; Biggio, G.; Fadda, A.M. Ex vivo skin delivery of diclofenac by transcutol containing liposomes and suggested mechanism of vesicle–skin interaction. Eur. J. Pharm. Biopharm. 2011, 78, 27–35. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, K.; Guo, T.; Li, Y.; Zhu, C.; Feng, N. Transdermal baicalin delivery using diethylene glycol monoethyl ether-mediated cubic phase gel. Int. J. Pharm. 2015, 479, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Osborne, D.W.; Musakhanian, J. Skin penetration and permeation properties of Transcutol®—neat or diluted mixtures. Aaps Pharmscitech 2018, 19, 3512–3533. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hydrogels * | Gelling Agents | Permeation Enhancers | ||||
|---|---|---|---|---|---|---|
| Cp940 | HEC | SCMC | DermarolTM 6CC | Cellosolve® | Tween® 80 | |
| F1 | 1.00 g | - | - | - | - | - |
| F2 | - | 1.00 g | - | - | - | - |
| F3 | - | - | 1.00 g | - | - | - |
| F4 | - | 0.75 g | - | - | - | - |
| F5 | - | 0.50 g | - | - | - | - |
| F6 | - | 0.50 g | - | 5.00 mL | - | - |
| F7 | - | 0.50 g | - | - | 5.00 mL | - |
| F8 | - | 0.50 g | - | - | - | 5.00 mL |
| F9 | - | 0.50 g | - | - | 7.50 mL | - |
| Hydrogels | Physical Appearance | Drug Content (%) (n = 3 ± SD) | pH (n = 3 ± SD) | ||
|---|---|---|---|---|---|
| Color | Clarity | Homogeneity | |||
| F1 | Colorless | Turbid | Homogenous | 98.00 ± 0.13 | 7.42 + 0.01 |
| F2 | Colorless | Clear | Homogenous | 99.80 ± 0.94 | 7.44 + 0.03 |
| F3 | Colorless | Clear | Homogenous | 101.43 ± 1.13 | 7.39 + 0.04 |
| F4 | Colorless | Clear | Homogenous | 101.92 ± 0.93 | 7.42 + 0.02 |
| F5 | Colorless | Turbid | Homogenous | 101.67 ± 1.18 | 7.41 + 0.01 |
| F6 | Colorless | Turbid | Homogenous | 99.32 ± 0.72 | 7.38 + 0.04 |
| F7 | Colorless | Clear | Homogenous | 99.57 ± 1.01 | 7.36 + 0.01 |
| F8 | Slightly yellow | Clear | Homogenous | 101.51 ± 1.16 | 7.43 + 0.03 |
| F9 | colorless | Clear | Homogenous | 103.00 ± 0.76 | 7.37 + 0.02 |
| Hydrogels | Viscosity at 50 rpm (cp) | Farrow’s Constant (N) | Flow Behavior |
|---|---|---|---|
| F1 | 2976 | 1.86 | Pseudoplastic |
| F2 | 1027 | 1.72 | Pseudoplastic |
| F3 | 681 | 1.12 | Pseudoplastic |
| F4 | 645 | 2.46 | Pseudoplastic |
| F5 | 3765 | 1.04 | Pseudoplastic |
| F6 | 5361 | 1.21 | Pseudoplastic |
| F7 | 675 | 2.58 | Pseudoplastic |
| F8 | 978 | 3.20 | Pseudoplastic |
| F9 | 981 | 1.12 | Pseudoplastic |
| Formulations * | Q180 (µg/cm2) | Q240 (µg/cm2) | Jss (µg·h/cm2) | KP (cm/h) | FER |
|---|---|---|---|---|---|
| BH solution by passive diffusion | 5.24 ± 0.06 | 5.77 ± 0.05 | 1.44 ± 0.01 | 0 | 1 |
| BH solution by iontophoresis | 371.68 ± 3.78 | 415.92 ± 4.44 | 103.98 ± 1.11 | 0.01040 ± 0.00011 | 72.09 ± 0.69 |
| F1 | 652.00 ± 8.06 | 719.43 ± 0.62 | 179.86 ± 0.16 | 0.01799 ± 0.00002 | 124.70 ± 1.03 |
| F2 | 706.41 ± 5.14 | 792.38 ± 9.43 | 198.10 ± 2.36 | 0.01981 ± 0.00024 | 137.34 ± 1.12 |
| F3 | 598.99 ± 5.24 | 685.12 ± 6.56 | 171.28 ± 1.64 | 0.01713 ± 0.00016 | 118.75 ± 1.35 |
| F4 | 742.04 ± 5.67 | 850.49 ± 5.35 | 212.62 ± 1.34 | 0.02126 ± 0.00013 | 147.42 ± 1.22 |
| F5 | 900.57 ± 8.79 | 982.61 ± 7.04 | 245.65 ± 1.76 | 0.02457 ± 0.00018 | 170.31 ± 0.33 |
| F6 | 1058.78 ± 18.37 | 1146.67 ± 5.03 | 286.67 ± 1.26 | 0.02867 ± 0.00013 | 198.75 ± 1.12 |
| F7 | 1390.68 ± 3.65 | 1470.84 ± 9.49 | 367.71 ± 2.37 | 0.03677 ± 0.00024 | 254.94 ± 1.32 |
| F8 | 1186.55 ± 12.00 | 1292.02 ± 6.67 | 323.00 ± 1.67 | 0.03230 ± 0.00017 | 223.94 ± 1.25 |
| F9 | 1307.44 ± 4.26 | 1415.93 ± 4.70 | 353.98 ± 1.18 | 0.03540 ± 0.00012 | 245.43 ± 2.65 |
| PK Parameters * | F7 | Concor® Tablet | Statistical p-Values |
|---|---|---|---|
| Cmax (ng/mL) | 8.28 ± 1.34 | 4.46 ± 1.13 | p = 0.0001 |
| Tmax (h) a | 2.00 ± 2.00 | 2.92 ± 3.00 | p = 0.0020 |
| AUC0–40 (ng·h/mL) | 43.19 ± 3.31 | 21.44 ± 3.60 | p = 0.0001 |
| MRT (h) | 8.69 ± 1.86 | 8.59 ± 2.77 | p > 0.0500 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teaima, M.H.; Mohamed, M.A.A.; Abd El Rehem, R.T.; Tayel, S.A.; El-Nabarawi, M.A.; Fouad, S.A. Enhanced Transdermal Delivery of Bisoprolol Hemifumarate via Combined Effect of Iontophoresis and Chemical Enhancers: Ex Vivo Permeation/In Vivo Pharmacokinetic Studies. Pharmaceutics 2021, 13, 682. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13050682
Teaima MH, Mohamed MAA, Abd El Rehem RT, Tayel SA, El-Nabarawi MA, Fouad SA. Enhanced Transdermal Delivery of Bisoprolol Hemifumarate via Combined Effect of Iontophoresis and Chemical Enhancers: Ex Vivo Permeation/In Vivo Pharmacokinetic Studies. Pharmaceutics. 2021; 13(5):682. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13050682
Chicago/Turabian StyleTeaima, Mahmoud H., Mohamed Azmi Ahmed Mohamed, Randa Tag Abd El Rehem, Saadia A. Tayel, Mohamed A. El-Nabarawi, and Shahinaze A. Fouad. 2021. "Enhanced Transdermal Delivery of Bisoprolol Hemifumarate via Combined Effect of Iontophoresis and Chemical Enhancers: Ex Vivo Permeation/In Vivo Pharmacokinetic Studies" Pharmaceutics 13, no. 5: 682. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13050682