
Enhancement of Rotator Cuff Healing with Farnesol-Impregnated Gellan Gum/Hyaluronic Acid Hydrogel Membranes in a Rabbit Model

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
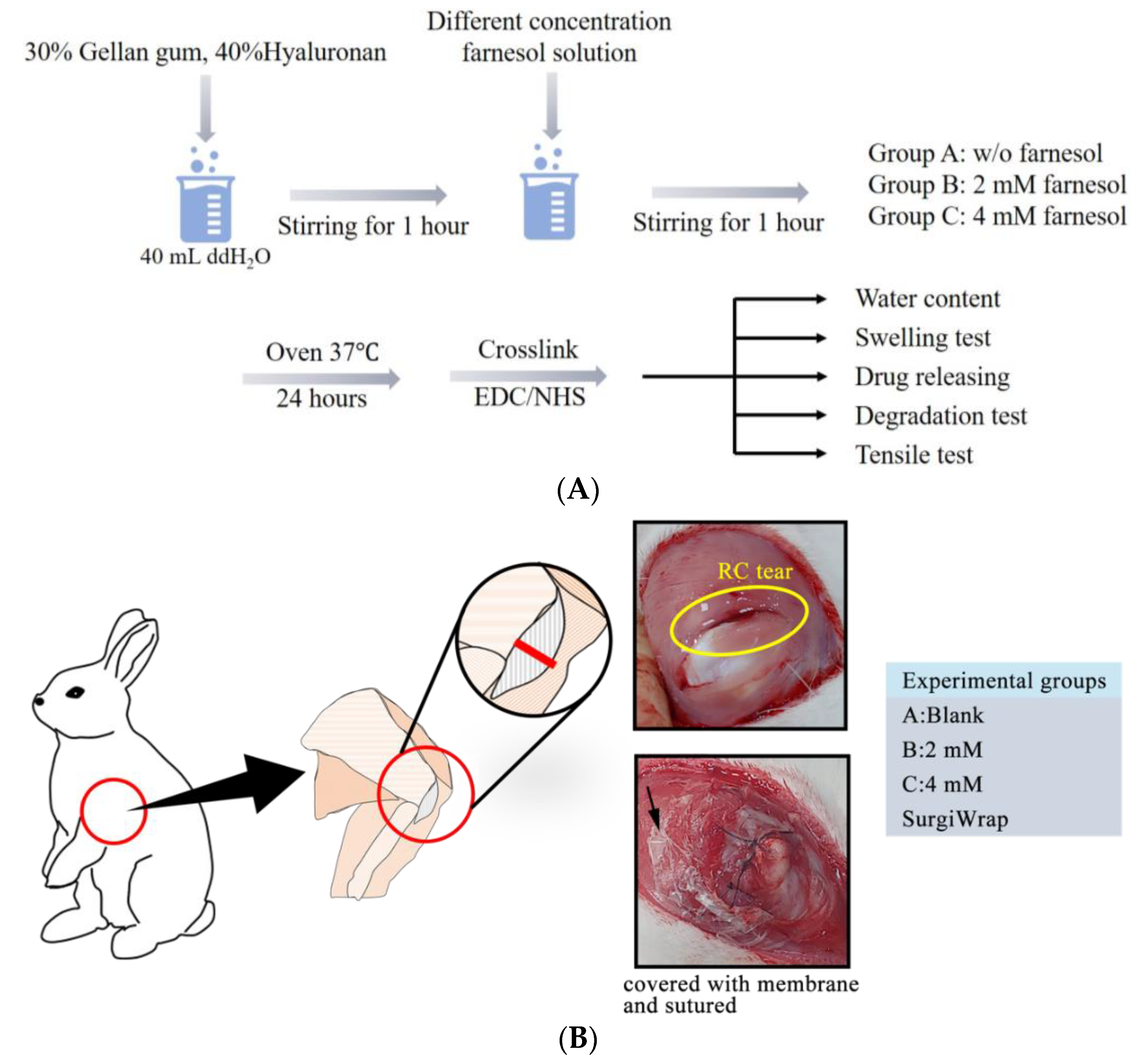
2.1. Fabrication of GHF Hydrogel Membranes
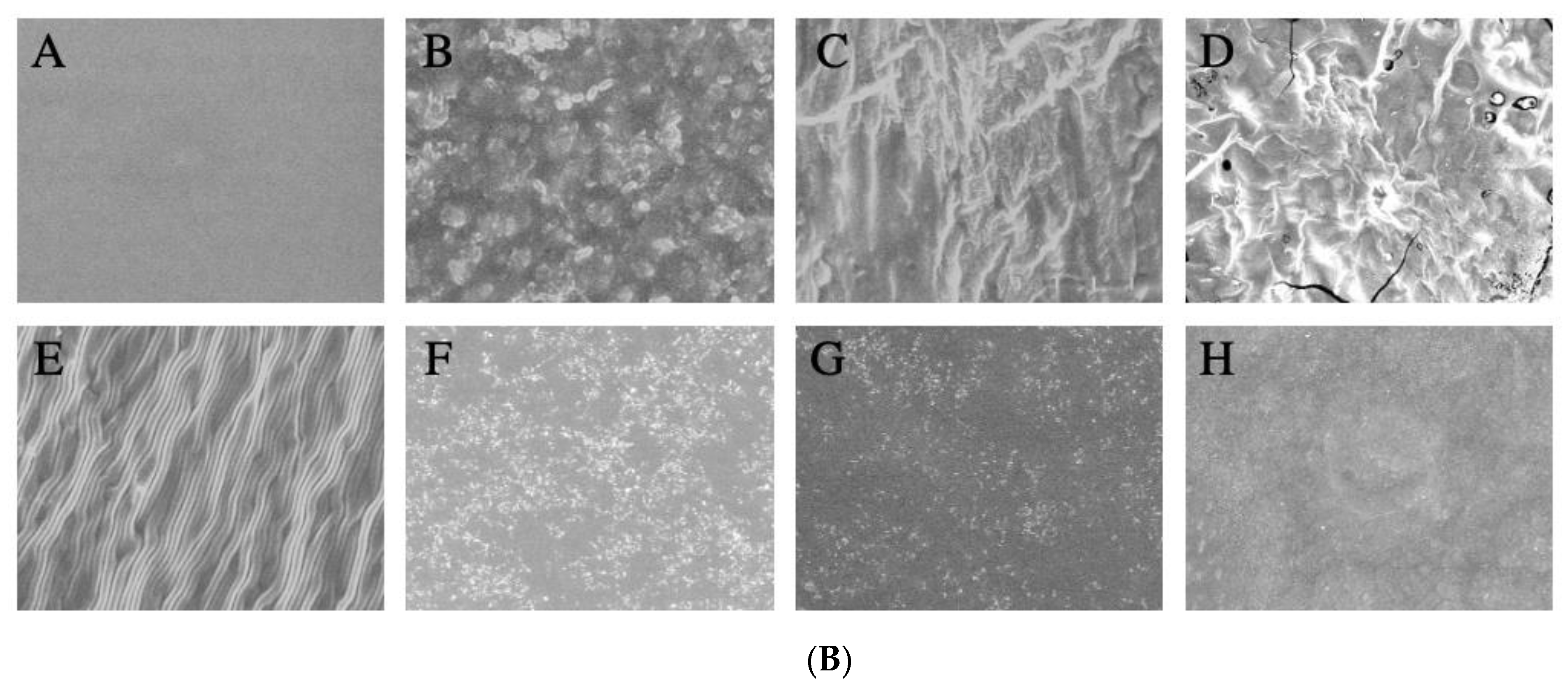
2.2. Characterization of GHF Membranes
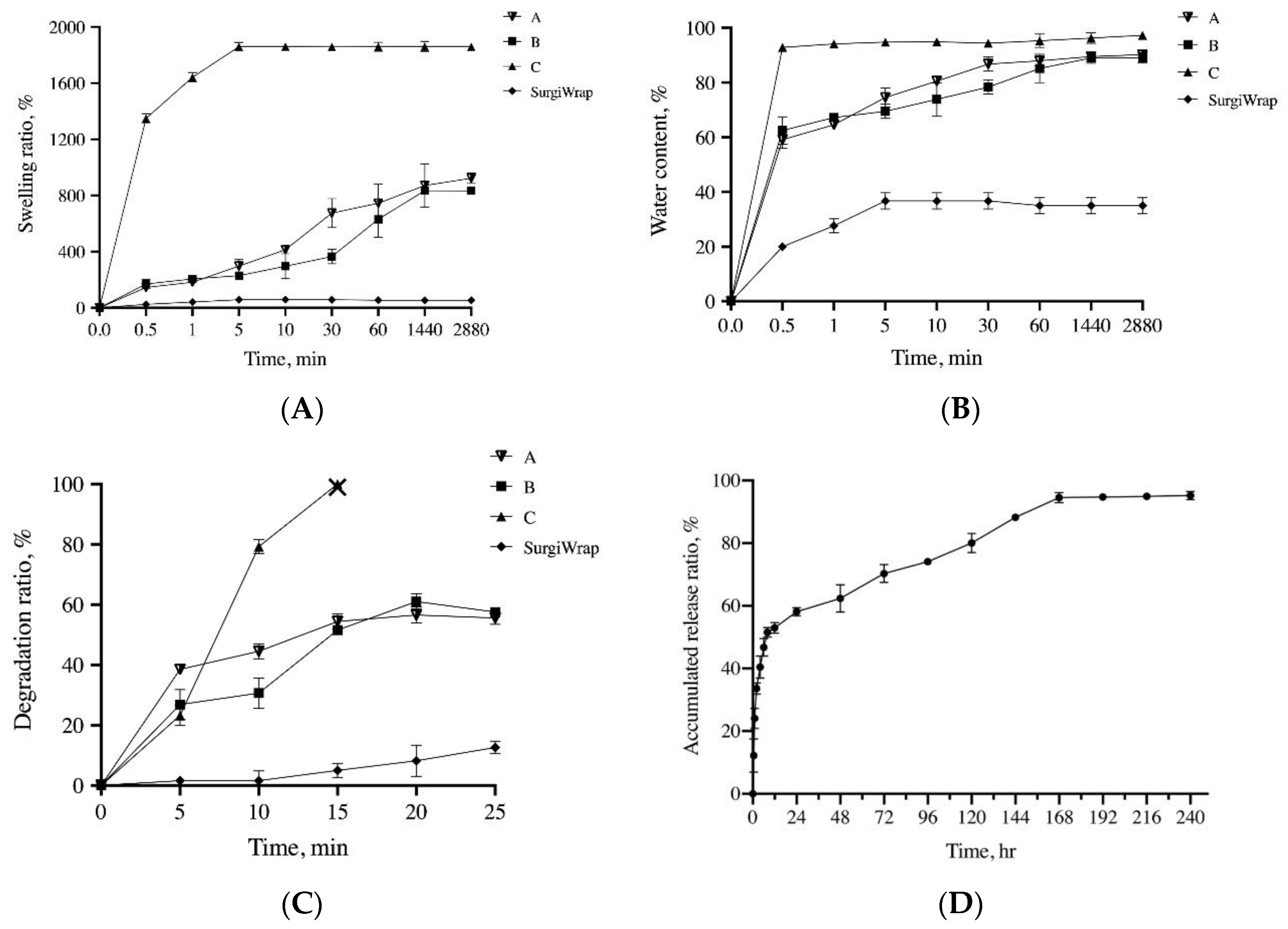
2.2.1. Water Content and Swelling Ratio Measurement
2.2.2. Mechanical Property Measurement
2.2.3. In Vitro Degradation Test
2.2.4. In Vitro Release Test
2.3. In Vitro Cell Viability
2.4. Quantification of Collagen Production
2.5. Anti-Inflammatory Test with H2O2-Induced Cells
2.6. In Vivo Experiments for the Assessment of RC Tear Repair
2.6.1. Animals and Experimental Design
2.6.2. Histopathological Analysis
2.6.3. Picrosirius Red Stain with Polarization Microscopy
2.6.4. Histological Assessments
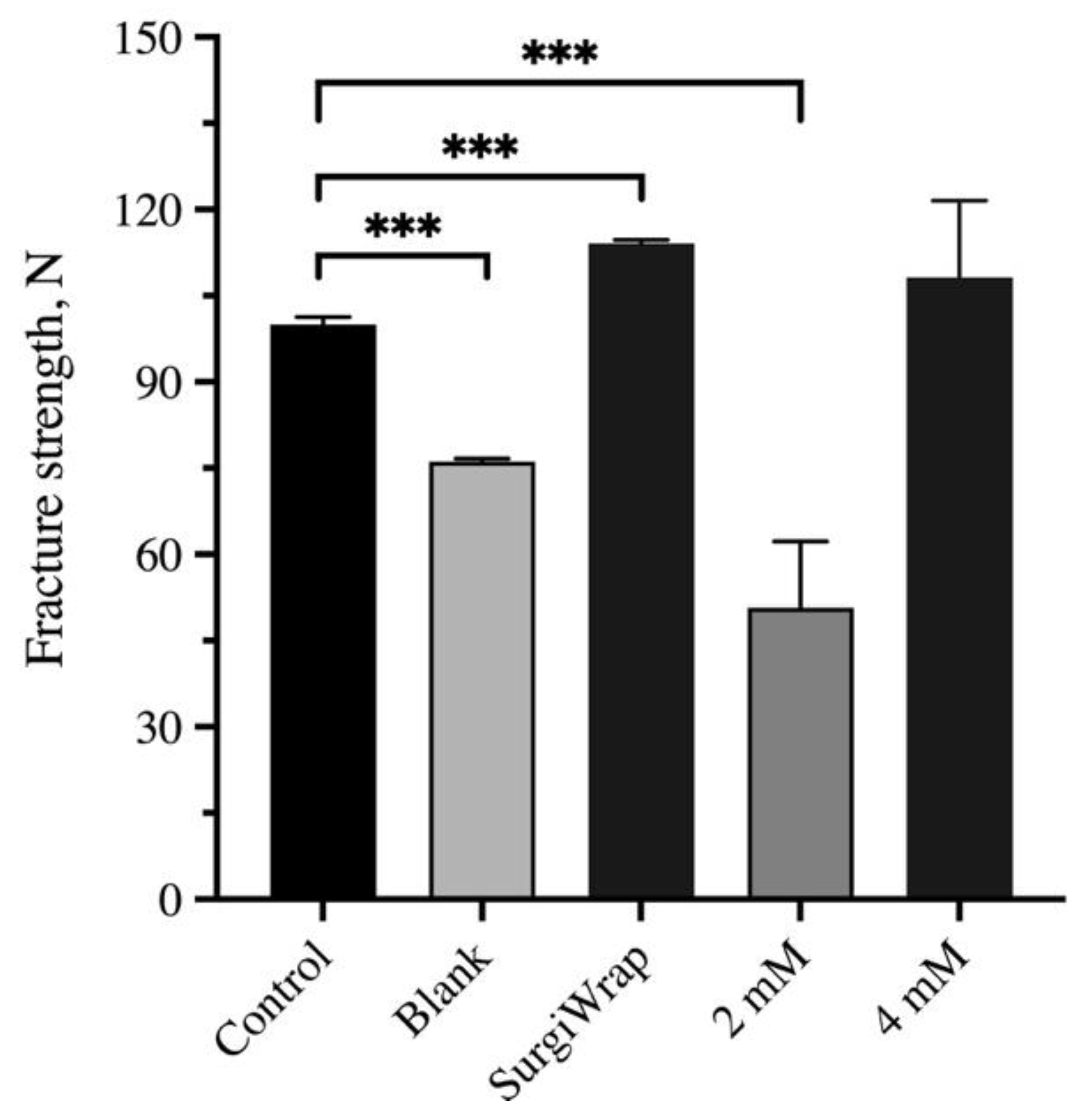
2.7. Mechanical Test of RC
2.8. Statistical Analysis
3. Results
3.1. Basic Properties of the GHF Membranes
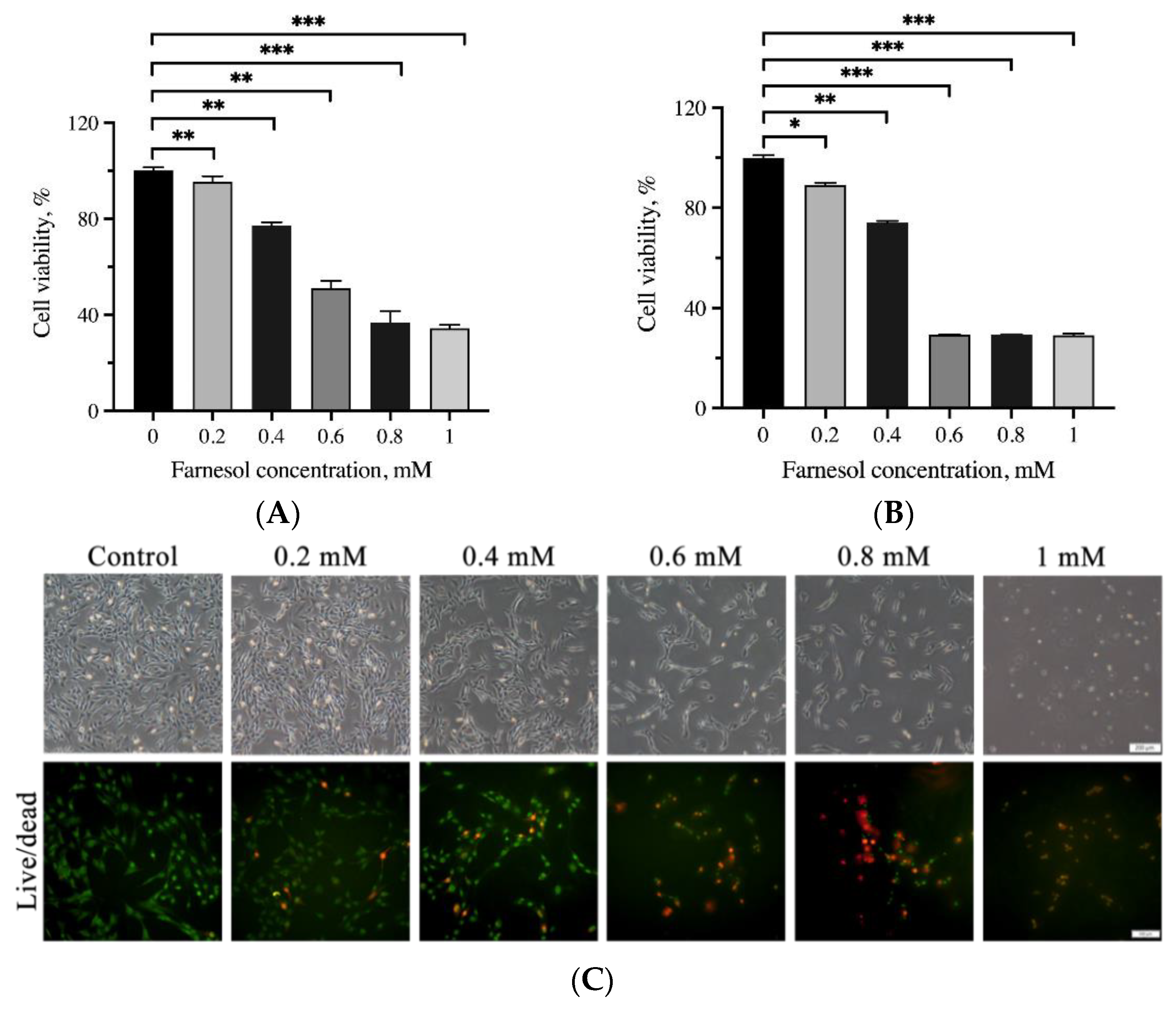
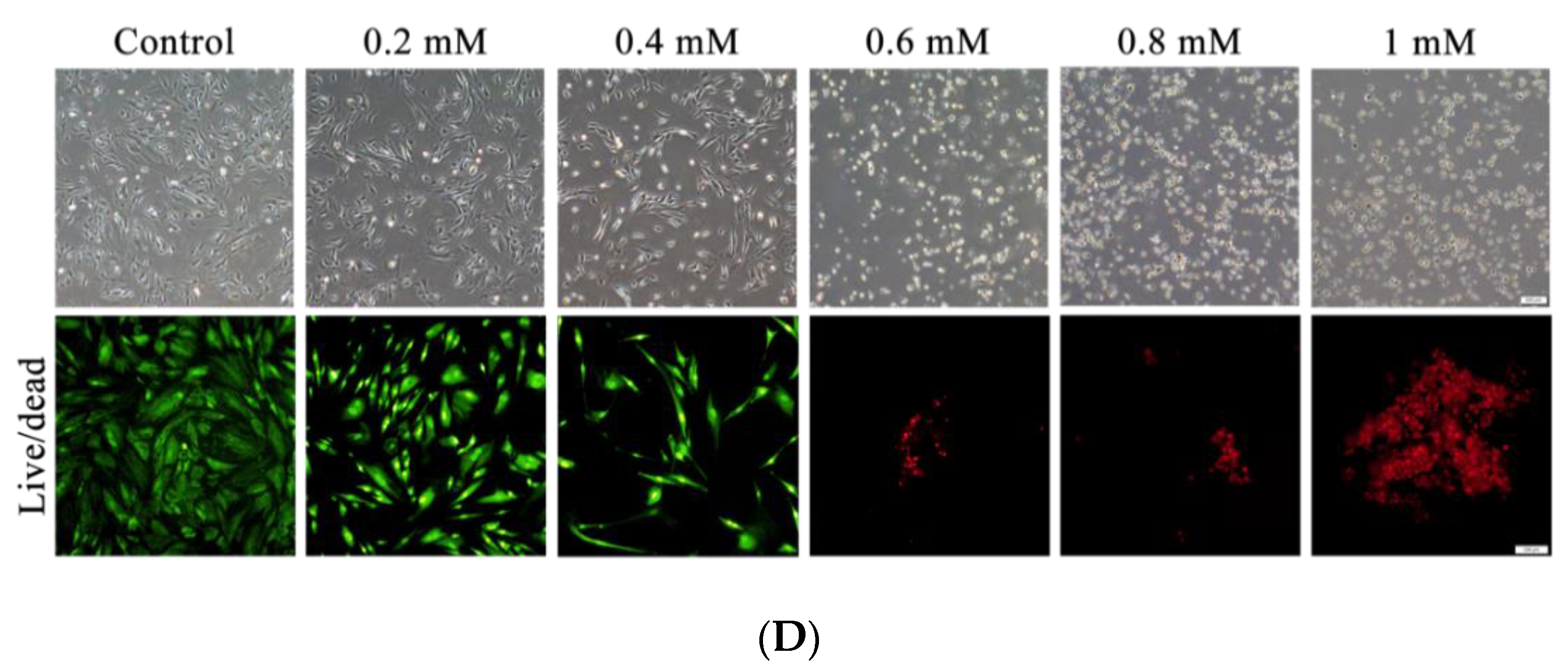
3.2. Assessment of Cell Viability through the MTT Assay and Live/Dead Cell Staining
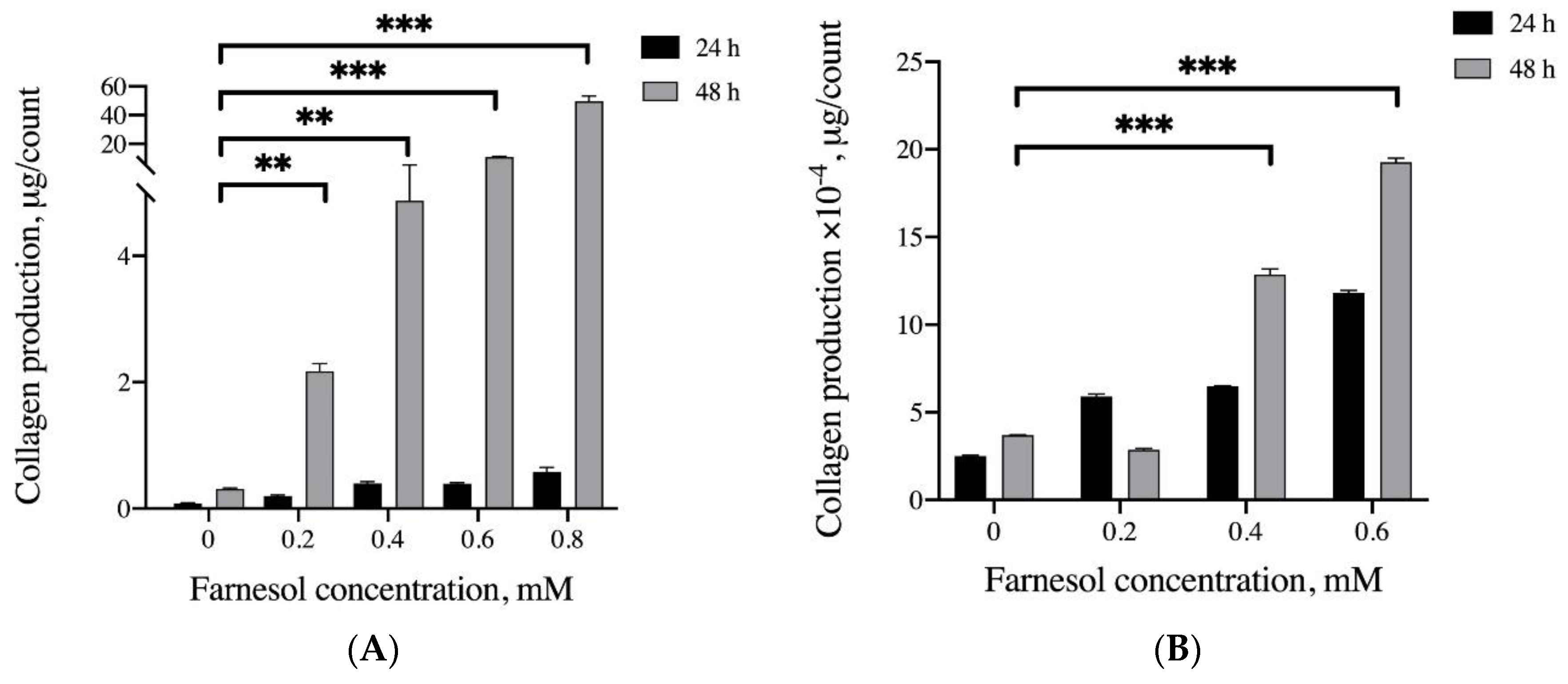
3.3. Effects of Farnesol on Collagen Production In Vitro
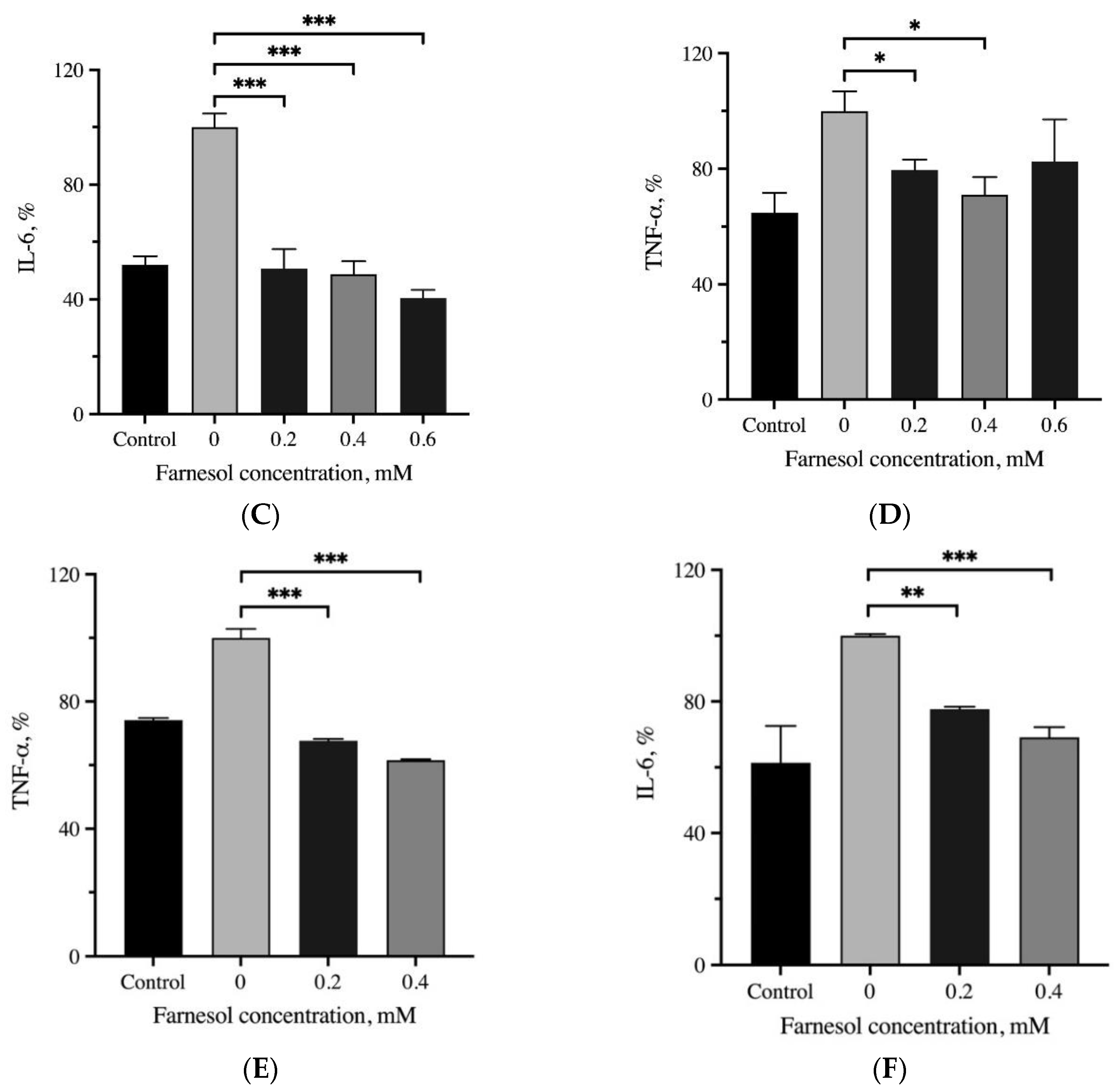
3.4. Anti-Inflammatory Effects of Farnesol
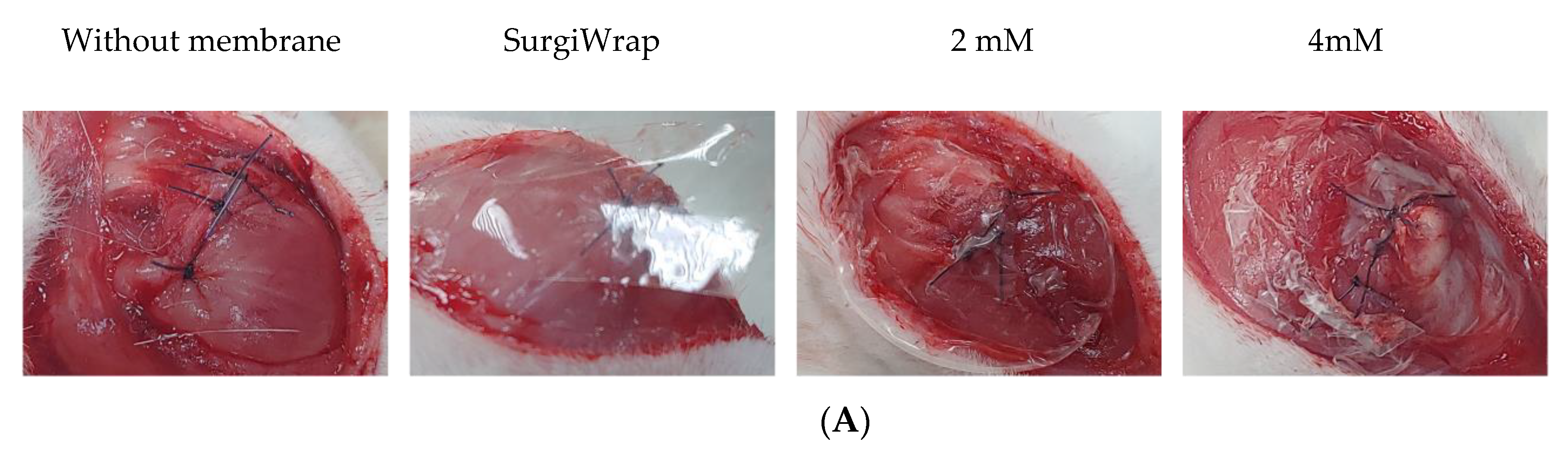
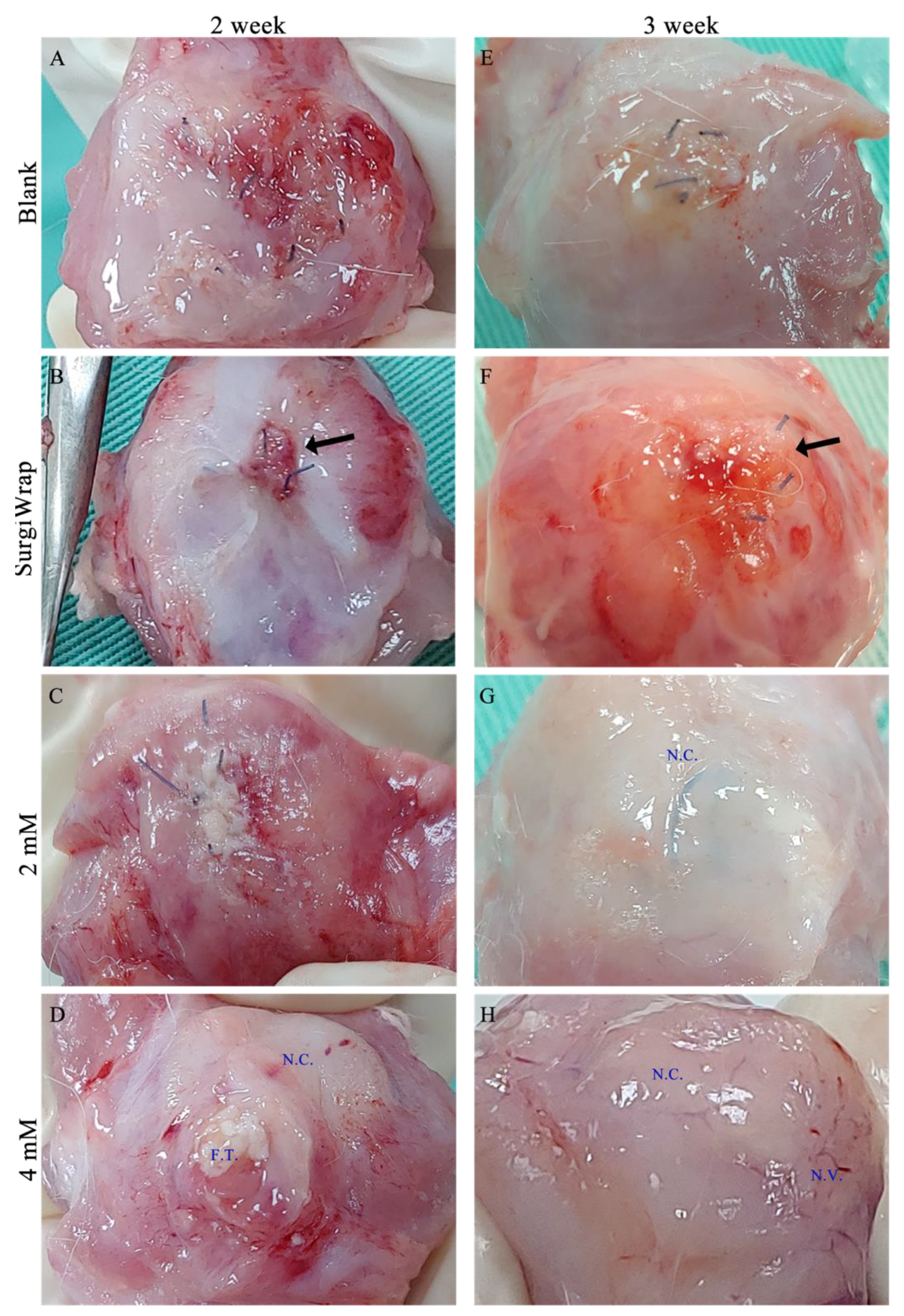
3.5. Gross Inspection of RC Tear Healing
3.6. In Vivo Histological Assessments
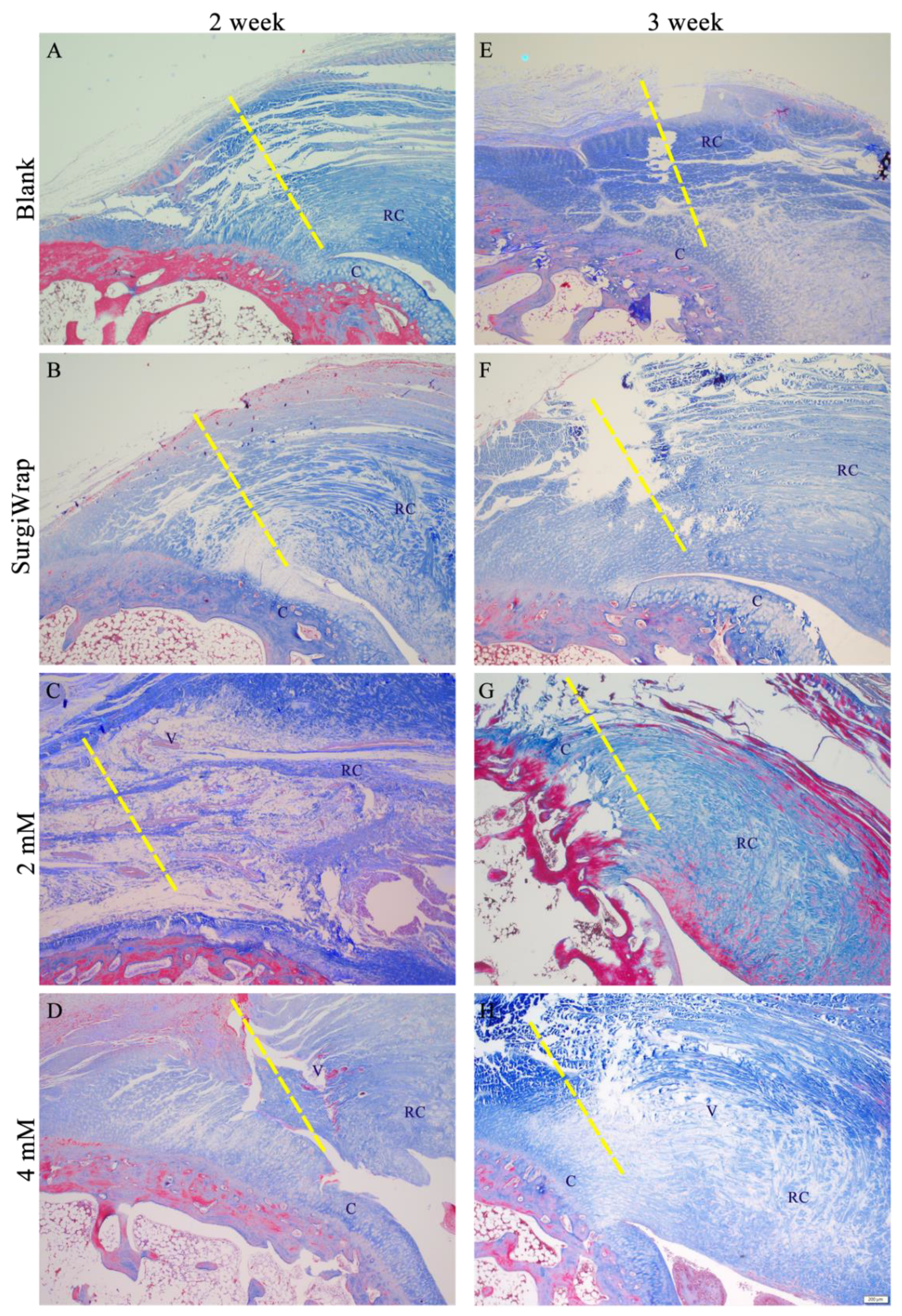
3.7. Picrosirius Red Staining for Collagen Assessment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sambandam, S.N.; Khanna, V.; Gul, A.; Mounasamy, V. Rotator cuff tears: An evidence based approach. World J. Orthop. 2015, 6, 902–918. [Google Scholar] [CrossRef]
- Pandey, V.; Willems, W.J. Rotator cuff tear: A detailed update. Asia-Pacific J. Sports Med. Arthrosc. Rehabil. Technol. 2015, 2, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zumstein, M.A.; Schaer, M.; Schober, M.; Berger, S.; Boileau, P. Biologically based strategies to augment rotator cuff tears. Int. J. Shoulder Surg. 2012, 6, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonemitsu, R.; Tokunaga, T.; Shukunami, C.; Ideo, K.; Arimura, H.; Karasugi, T.; Nakamura, E.; Ide, J.; Hiraki, Y.; Mizuta, H. Fibroblast Growth Factor 2 Enhances Tendon-to-Bone Healing in a Rat Rotator Cuff Repair of Chronic Tears. Am. J. Sports Med. 2019, 47, 1701–1712. [Google Scholar] [CrossRef]
- Kang, S.; Yoon, J.S.; Lee, J.Y.; Kim, H.J.; Park, K.; Kim, S.E. Long-term local PDGF delivery using porous microspheres modified with heparin for tendon healing of rotator cuff tendinitis in a rabbit model. Carbohydr. Polym. 2019, 209, 372–381. [Google Scholar] [CrossRef]
- Pakyari, M.; Farrokhi, A.; Maharlooei, M.K.; Ghahary, A. Critical Role of Transforming Growth Factor Beta in Different Phases of Wound Healing. Adv. Wound Care 2013, 2, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Yamakawa, S.; Hayashida, K. Advances in surgical applications of growth factors for wound healing. Burn. Trauma 2019, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Thomopoulos, S.; Genin, G.M.; Galatz, L.M. The development and morphogenesis of the tendon-to-bone insertion-what development can teach us about healing. J. Musculoskelet. Neuronal Interact. 2010, 10, 35–45. [Google Scholar]
- Khan, R.; Sultana, S. Farnesol attenuates 1,2-dimethylhydrazine induced oxidative stress, inflammation and apoptotic responses in the colon of Wistar rats. Chem. Interact. 2011, 192, 193–200. [Google Scholar] [CrossRef]
- Ku, C.-M.; Lin, J.-Y. Farnesol, a Sesquiterpene Alcohol in Herbal Plants, Exerts Anti-Inflammatory and Antiallergic Effects on Ovalbumin-Sensitized and -Challenged Asthmatic Mice. Evidence-Based Complement. Altern. Med. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.X.; Huang, H.H.; Chang, H.R.; Kuo, S.M. Evaluation of the UVB-screening capacity and restorative effects exerted by farnesol gel on UVB-caused sunburn. Environ. Toxicol. 2018, 33, 488–507. [Google Scholar] [CrossRef]
- Wu, Y.C.; Wu, G.X.; Huang, H.H.; Kuo, S.M. Liposome-encapsulated farnesol accelerated tissue repair in third-degree burns on a rat model. Burns 2019, 45, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, I.; Survase, S.; Saudagar, P.; Singhal, R. Gellan Gum: Fermentative Production, Downstream Processing and Applications. Food Technol. Biotechnol. 2007, 45, 341–354. [Google Scholar]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Veter-Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, S.; Hascall, V.C.; Markwald, R.R.; Ghatak, S. Interactions between Hyaluronan and Its Receptors (CD44, RHAMM) Regulate the Activities of Inflammation and Cancer. Front. Immunol. 2015, 6, 201. [Google Scholar] [CrossRef] [Green Version]
- Osti, L.; Berardocco, M.; di Giacomo, V.; Di Bernardo, G.; Oliva, F.; Berardi, A.C. Hyaluronic acid increases tendon derived cell viability and collagen type I expression in vitro: Comparative study of four different Hyaluronic acid preparations by molecular weight. BMC Musculoskelet. Disord. 2015, 16, 284. [Google Scholar] [CrossRef] [Green Version]
- Kuo, S.M.; Chang, S.J.; Wang, H.-Y.; Tang, S.C.; Yang, S.-W. Evaluation of the ability of xanthan gum/gellan gum/hyaluronan hydrogel membranes to prevent the adhesion of postrepaired tendons. Carbohydr. Polym. 2014, 114, 230–237. [Google Scholar] [CrossRef]
- Lattouf, R.; Younes, R.; Lutomski, D.; Naaman, N.; Godeau, G.; Senni, K.; Changotade, S. Picrosirius red staining: A useful tool to appraise collagen networks in normal and pathological tissues. J. Histochem. Cytochem. 2014, 62, 751–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, B.K.; Febbraio, M.A. Muscle as an Endocrine Organ: Focus on Muscle-Derived Interleukin-6. Physiol. Rev. 2008, 88, 1379–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiu, L.-Y.; Huang, H.H.; Chen, C.Y.; Cheng, H.-Y.; Chen, C.I.; Kuo, S.M. Reparative and toxicity-reducing effects of liposome-encapsulated saikosaponin in mice with liver fibrosis. Biosci. Rep. 2020, 40. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Liu, X.; Yin, J.; Wu, H.; Cai, X.; Wang, N.; Qian, Y.; Wang, F. IL-6 receptor blockade ameliorates diabetic nephropathy via inhibiting inflammasome in mice. Metabol. Clin. Exp. 2018, 83, 18–24. [Google Scholar] [CrossRef]
- Podbregar, M.; Lainscak, M.; Prelovsek, O.; Mars, T. Cytokine Response of Cultured Skeletal Muscle Cells Stimulated with Proinflammatory Factors Depends on Differentiation Stage. Sci. World J. 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Zhou, Y.-Q.; Liu, Z.-H.; Chen, S.-P.; Li, M.; Shahveranov, A.; Ye, D.-W.; Tian, Y.-K. Interleukin-6: An emerging regulator of pathological pain. J. Neuroinflammation 2016, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Muñoz-Cánoves, P.; Scheele, C.; Pedersen, B.K.; Serrano, A.L. Interleukin-6 myokine signaling in skeletal muscle: A double-edged sword? FEBS J. 2013, 280, 4131–4148. [Google Scholar] [CrossRef] [PubMed]
- Borges, V.M.; Vandivier, R.W.; McPhillips, K.A.; Kench, J.A.; Morimoto, K.; Groshong, S.D.; Richens, T.R.; Graham, B.B.; Muldrow, A.M.; Van Heule, L.; et al. TNFα inhibits apoptotic cell clearance in the lung, exacerbating acute inflammation. Am. J. Physiol. Cell. Mol. Physiol. 2009, 297, L586–L595. [Google Scholar] [CrossRef] [PubMed]
- Prelovsek, O.; Mars, T.; Jevsek, M.; Podbregar, M.; Grubic, Z. High dexamethasone concentration prevents stimulatory effects of TNF-α and LPS on IL-6 secretion from the precursors of human muscle regeneration. Am. J. Physiol. Integr. Comp. Physiol. 2006, 291, R1651–R1656. [Google Scholar] [CrossRef]
- Hardin, B.J.; Campbell, K.S.; Smith, J.; Arbogast, S.; Smith, J.; Moylan, J.S.; Reid, M.B. TNF-α acts via TNFR1 and muscle-derived oxidants to depress myofibrillar force in murine skeletal muscle. J. Appl. Physiol. 2008, 104, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.G.; Pierre, B.A.S. Cytokines in exertion-induced skeletal muscle injury. Mol. Cell. Biochem. 1998, 179, 159–168. [Google Scholar] [CrossRef]
- Aderka, D.; Le, J.; Vilcek, J. IL-6 inhibits lipopolysaccharide-induced tumor necrosis factor production in cultured human monocytes, U937 cells, and in mice. J. Immunol. 1989, 143, 3517. [Google Scholar]
- Kohanawa, M. A Regulatory Effect of the Balance between TNF-α and IL-6 in the Granulomatous and Inflammatory Response to Rhodococcus aurantiacus Infection in Mice. J. Immunol. 2006, 177, 642. [Google Scholar] [CrossRef] [Green Version]
- Peake, J.M.; Della Gatta, P.; Suzuki, K.; Nieman, D. Cytokine expression and secretion by skeletal muscle cells: Regulatory mechanisms and exercise effects. Exerc. Immunol. Rev. 2015, 21, 8–25. [Google Scholar] [PubMed]
- Horikawa, S.; Ishii, Y.; Hamashima, T.; Yamamoto, S.; Mori, H.; Fujimori, T.; Shen, J.; Inoue, R.; Nishizono, H.; Itoh, H.; et al. PDGFRα plays a crucial role in connective tissue remodeling. Sci. Rep. 2015, 5, 17948. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.J.; Watts, A.E.; Schnabel, L.V. Cell- and gene-based approaches to tendon regeneration. J. Shoulder Elb. Surg. 2012, 21, 278–294. [Google Scholar] [CrossRef] [PubMed]
- Williams, I.F.; Mccullagh, K.G.; Silver, I.A. The Distribution of Types I and III Collagen and Fibronectin in the Healing Equine Tendon. Connect. Tissue Res. 1984, 12, 211–227. [Google Scholar] [CrossRef]
- Sajjad, W.; Khan, T.; Ul-Islam, M.; Khan, R.; Hussain, Z.; Khalid, A.; Wahid, F. Development of modified montmorillonite-bacterial cellulose nanocomposites as a novel substitute for burn skin and tissue regeneration. Carbohydr. Polym. 2019, 206, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.S.; Callaci, J.J.; Juknelis, D.; Marra, G.; Tonino, P.; Freedman, K.B.; Wezeman, F.H. The effect of corticosteroid on collagen expression in injured rotator cuff tendon. J. Bone Joint Surg. Am. 2006, 88, 1331–1338. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Collagen Fiber Density | Collagen Fiber Orientation | Tendon–Bone Interface Interdigitation | Vascularity | Collagen I/III Ratio |
|---|---|---|---|---|---|
| 1 | None | None | <25% | None | None |
| 2 | Low | Disorganized | 25–50% | Minimal | Minimal |
| 3 | Median | Moderately aligned | 50–75% | Moderate | Moderate |
| 4 | High | Highly aligned | >75% | Abundant | Abundant |
| Group | Water Content, % | Swelling Ratio, % | Young’s Modulus, MPa | Max. Elongation, mm |
|---|---|---|---|---|
| 0 mM | 90.2 ± 0.4 | 923.3 ± 37.6 | 29.6 ± 4.8 * | 1.7 ± 0.4 |
| 2 mM | 89.0 ± 1.8 | 833.3 ± 16.0 | 50.7 ± 7.2 ** | 1.1 ± 0.03 *** |
| 4 mM | 94.8 ± 0.9 | 1860.8 ± 307.7 | 61.1 ± 7.9 ** | 1.0 ± 0.1 *** |
| SurgiWrap | 36.8 ± 3.0 | 58.3 ± 7.2 | 40.7 ± 0.3 | 1.3 ± 1.5 |
| Time | Blank | SurgiWrap | 2 mM | 4 mM |
|---|---|---|---|---|
| 2 week | 6.67 ± 0.58 | 6.33 ± 2.51 | 8.33 ± 1.53 * | 10.67 ± 1.15 **,# |
| 3 week | 11.67 ± 2.51 | 11.33 ± 1.51 | 14.33 ± 2.31 ** | 18.67 ± 0.58 ***,## |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-H.; Lee, S.-I.; Lin, F.-H.; Wu, G.-X.; Wu, C.-S.; Kuo, S.-M. Enhancement of Rotator Cuff Healing with Farnesol-Impregnated Gellan Gum/Hyaluronic Acid Hydrogel Membranes in a Rabbit Model. Pharmaceutics 2021, 13, 944. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13070944
Lin Y-H, Lee S-I, Lin F-H, Wu G-X, Wu C-S, Kuo S-M. Enhancement of Rotator Cuff Healing with Farnesol-Impregnated Gellan Gum/Hyaluronic Acid Hydrogel Membranes in a Rabbit Model. Pharmaceutics. 2021; 13(7):944. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13070944
Chicago/Turabian StyleLin, Yen-Hung, Sheng-I Lee, Feng-Huei Lin, Guan-Xuan Wu, Chun-Shien Wu, and Shyh-Ming Kuo. 2021. "Enhancement of Rotator Cuff Healing with Farnesol-Impregnated Gellan Gum/Hyaluronic Acid Hydrogel Membranes in a Rabbit Model" Pharmaceutics 13, no. 7: 944. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13070944