
Relation between Plasma Trough Concentration of Pazopanib and Progression-Free Survival in Metastatic Soft Tissue Sarcoma Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
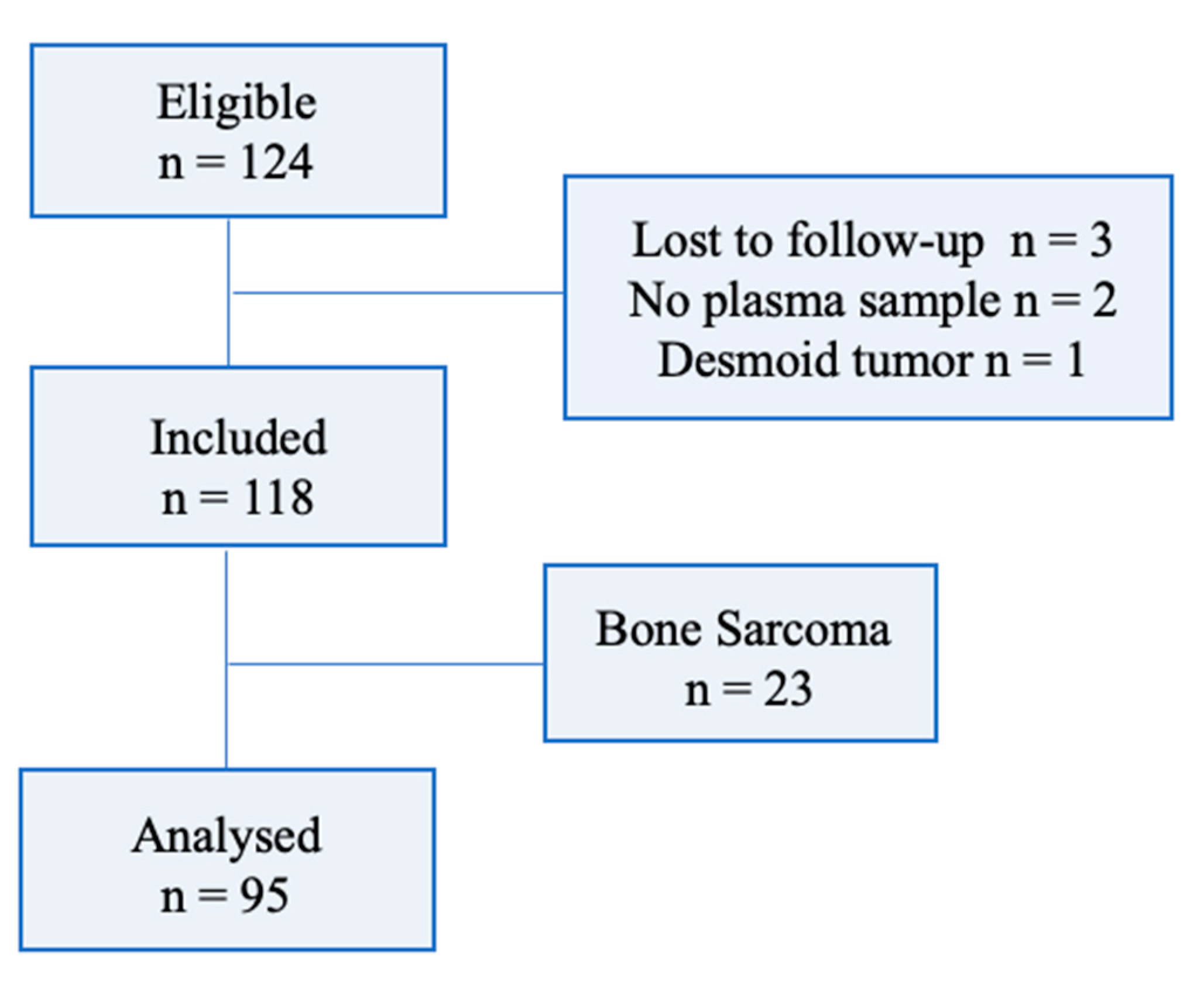
2.1. Study Design and Patients
2.2. Procedures
2.3. Pharmacokinetic Assessments
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
3.1. Patients and Treatment
3.2. Plasma Concentration of Pazopanib
3.3. Efficacy of PAZ
3.4. Overall Survival
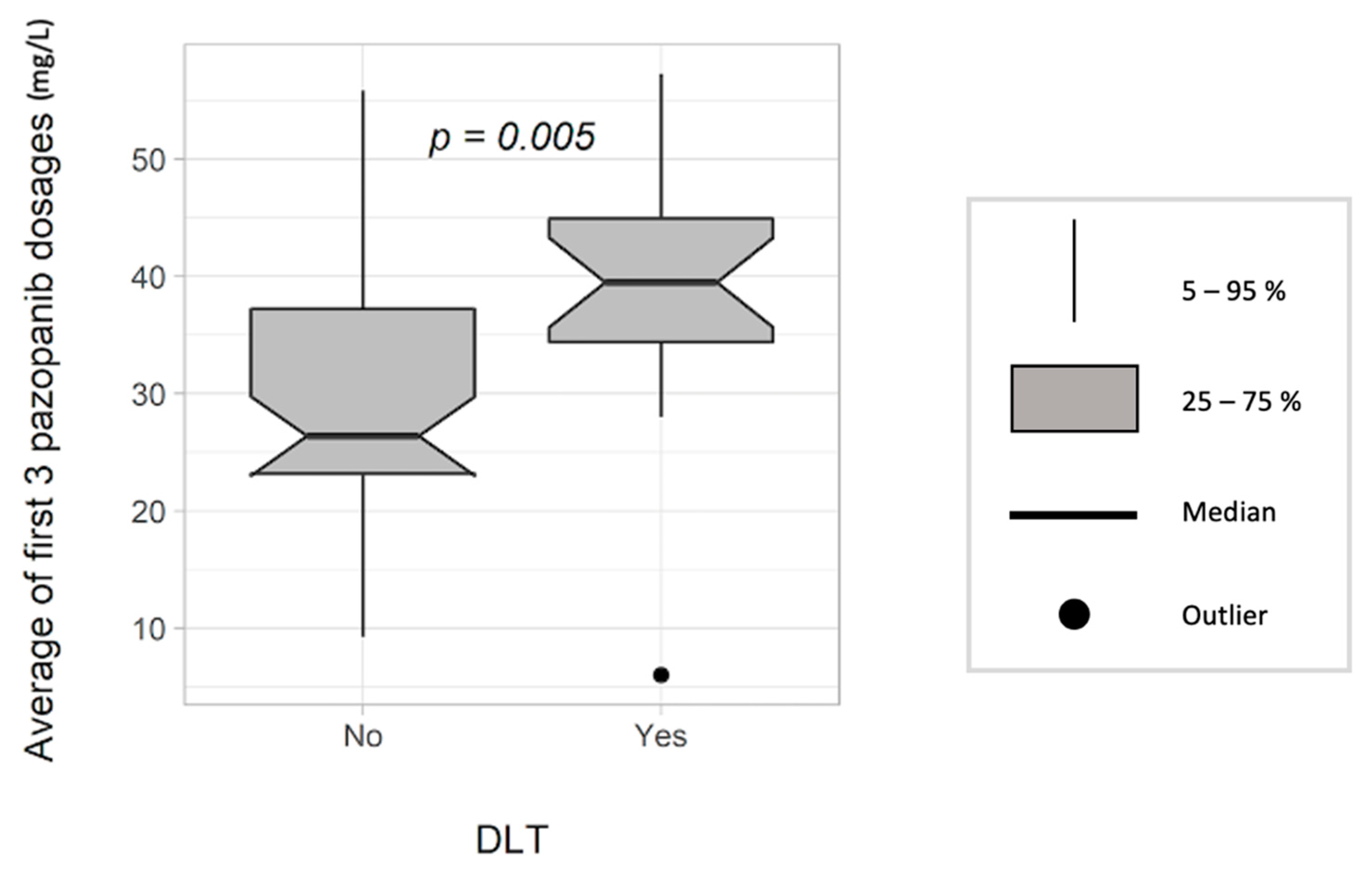
3.5. Relationship between Exposure and Dose-Limiting Toxicity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gatta, G.; Capocaccia, R.; Botta, L.; Mallone, S.; De Angelis, R.; Ardanaz, E.; Comber, H.; Dimitrova, N.; Leinonen, M.K.; Siesling, S.; et al. Burden and centralised treatment in Europe of rare tumours: Results of RARECAREnet—A population-based study. Lancet Oncol. 2017, 18, 1022–1039. [Google Scholar] [CrossRef] [Green Version]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.; Schöffski, P.; Blay, J.; De Tos, A.; Marreaud, S.; Litiere, S.; Van Der Graaf, W. Results of a Randomised Phase III Trial (EORTC 62012) of Single Agent Doxorubicin Versus Doxorubicin Plus Ifosfamide as First Line Chemotherapy for Patients with Advanced or Metastatic Soft Tissue Sarcoma: A Survival Study by the Eortc Soft Tissue and Bone Sarcoma Group. Ann. Oncol. 2012, 23, ixe28. [Google Scholar] [CrossRef]
- Schutz, F.A.; Choueiri, T.K.; Sternberg, C.N. Pazopanib: Clinical development of a potent anti-angiogenic drug. Crit. Rev. Oncol. 2011, 77, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Hamberg, P.; Verweij, J.; Sleijfer, S. (Pre-)Clinical Pharmacology and Activity of Pazopanib, a Novel Multikinase Angiogenesis Inhibitor. Oncologist 2010, 15, 539–547. [Google Scholar] [CrossRef] [Green Version]
- Sternberg, C.N.; Davis, I.D.; Mardiak, J.; Szczylik, C.; Lee, E.; Wagstaff, J.; Barrios, C.H.; Salman, P.; Gladkov, O.A.; Kavina, A.; et al. Pazopanib in Locally Advanced or Metastatic Renal Cell Carcinoma: Results of a Randomized Phase III Trial. J. Clin. Oncol. 2010, 28, 1061–1068. [Google Scholar] [CrossRef]
- van der Graaf, W.T.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Suttle, A.B.; Ball, H.A.; Molimard, M.; Hutson, T.E.; Carpenter, C.; Rajagopalan, D.; Lin, Y.; Swann, S.; Amado, R.; Pandite, L. Relationships between pazopanib exposure and clinical safety and efficacy in patients with advanced renal cell carcinoma. Brain J. Cancer 2014, 111, 1909–1916. [Google Scholar] [CrossRef] [Green Version]
- Verheijen, R.B.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Clinical Pharmacokinetics and Pharmacodynamics of Pazopanib: Towards Optimized Dosing. Clin. Pharmacokinet. 2017, 56, 987–997. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Van Erp, N.; Bins, S.; Mathijssen, R.H.J.; Schellens, J.H.M.; Beijnen, J.H.; Steeghs, N.; Huitema, A.D.R. Development of a Pharmacokinetic Model to Describe the Complex Pharmacokinetics of Pazopanib in Cancer Patients. Clin. Pharmacokinet. 2016, 56, 293–303. [Google Scholar] [CrossRef]
- Ozbey, A.C.; Combarel, D.; Poinsignon, V.; Lovera, C.; Saada, E.; Mir, O.; Paci, A. Population Pharmacokinetic Analysis of Pazopanib in Patients and Determination of Target AUC. Pharmaceuticals 2021, 14, 927. [Google Scholar] [CrossRef]
- Demetri, G.D.; Wang, Y.; Wehrle, E.; Racine, A.; Nikolova, Z.; Blanke, C.D.; Joensuu, H.; von Mehren, M. Imatinib Plasma Levels Are Correlated With Clinical Benefit in Patients With Unresectable/Metastatic Gastrointestinal Stromal Tumors. J. Clin. Oncol. 2009, 27, 3141–3147. [Google Scholar] [CrossRef] [PubMed]
- HoukCarlo, B.E.; Bello, C.L.; Poland, B.; Rosen, L.S.; Demetri, G.D.; Motzer, R.J. Relationship between exposure to sunitinib and efficacy and tolerability endpoints in patients with cancer: Results of a pharmacokinetic/pharmacodynamic meta-analysis. Cancer Chemother. Pharmacol. 2009, 66, 357–371. [Google Scholar] [CrossRef]
- Cabel, L.; Blanchet, B.; Thomas-Schoemann, A.; Huillard, O.; Bellesoeur, A.; Cessot, A.; Giroux, J.; Boudou-Rouquette, P.; Coriat, R.; Vidal, M.; et al. Drug monitoring of sunitinib in patients with advanced solid tumors: A monocentric observational French study. Fundam. Clin. Pharmacol. 2017, 32, 98–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verheijen, R.B.; Swart, L.E.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Exposure-survival analyses of pazopanib in renal cell carcinoma and soft tissue sarcoma patients: Opportunities for dose optimization. Cancer Chemother. Pharmacol. 2017, 80, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellesoeur, A.; Boudou-Rouquette, P.; Thomas-Schoemann, A.; Joly, C.; Tlemsani, C.; Vidal, M.; Goldwasser, F.; Blanchet, B. Individualized Pazopanib Dosing-Letter. Clin. Cancer Res. Off. J. Am Assoc. Cancer Res. 2017, 23, 6377. [Google Scholar] [CrossRef] [Green Version]
- Justice, C.N.; Derbala, M.H.; Baich, T.M.; Kempton, A.N.; Guo, A.S.; Ho, T.; Smith, S.A. The Impact of Pazopanib on the Cardiovascular System. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 387–398. [Google Scholar] [CrossRef]
- Anonymous. Votrient [Internet]. European Medicines Agency. 2018. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/votrient (accessed on 26 June 2021).
- U.S. Department of Health and Human Service. Common Terminology Criteria for Adverse Events (CTCAE); U.S. Department of Health and Human Service: Washington, DC, USA, 2017; p. 155.
- Verheijen, R.B.; Bins, S.; Mathijssen, R.H.; Lolkema, M.P.; van Doorn, L.; Schellens, J.H.; Beijnen, J.H.; Langenberg, M.H.; Huitema, A.D.; Steeghs, N. Individualized Pazopanib Dosing: A Prospective Feasibility Study in Cancer Patients. Clin. Cancer Res. 2016, 22, 5738–5746. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, H.I.; Dowlati, A.; Saini, S.; Savage, S.; Suttle, A.B.; Gibson, D.M.; Hodge, J.P.; Merkle, E.M.; Pandite, L. Phase I Trial of Pazopanib in Patients with Advanced Cancer. Clin. Cancer Res. 2009, 15, 4220–4227. [Google Scholar] [CrossRef] [Green Version]
- de Wit, D.; van Erp, N.P.; den Hartigh, J.; Wolterbeek, R.; den Hollander-van Deursen, M.; Labots, M.; Guchelaar, H.J.; Verheul, H.M.; Gelderblom, H. Therapeutic drug monitoring to individualise the dosing of pazopanib: A pharmacokinetic feasibility study. Ther. Drug Monit. 2015, 37, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Hamberg, P.; Boers-Sonderen, M.J.; Van Der Graaf, W.T.A.; De Bruijn, P.; Suttle, A.B.; Eskens, F.A.L.M.; Verweij, J.; Van Herpen, C.M.L.; Sleijfer, S. Pazopanib exposure decreases as a result of an ifosfamide-dependent drug–drug interaction: Results of a phase I study. Br. J. Cancer 2013, 110, 888–893. [Google Scholar] [CrossRef] [Green Version]
- Hamberg, P.; Mathijssen, R.H.J.; De Bruijn, P.; Leonowens, C.; Van Der Biessen, D.; Eskens, F.A.L.M.; Sleijfer, S.; Verweij, J.; De Jonge, M.J.A. Impact of pazopanib on docetaxel exposure: Results of a phase I combination study with two different docetaxel schedules. Cancer Chemother. Pharmacol. 2014, 75, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bible, K.C.; Suman, V.J.; Molina, J.R.; Smallridge, R.C.; Maples, W.J.; Menefee, M.E.; Rubin, J.; Sideras, K.; Morris, J.C., III; McIver, B.; et al. Efficacy of pazopanib in progressive, radioiodine-refractory, metastatic differentiated thyroid cancers: Results of a phase 2 consortium study. Lancet Oncol. 2010, 11, 962–972. [Google Scholar] [CrossRef] [Green Version]
- Bender, J.L.G.; Lee, A.; Reid, J.M.; Baruchel, S.; Roberts, T.; Voss, S.D.; Wu, B.; Ahern, C.H.; Ingle, A.M.; Harris, P.; et al. Phase I Pharmacokinetic and Pharmacodynamic Study of Pazopanib in Children With Soft Tissue Sarcoma and Other Refractory Solid Tumors: A Children’s Oncology Group Phase I Consortium Report. J. Clin. Oncol. 2013, 31, 3034–3043. [Google Scholar] [CrossRef] [Green Version]
- Tran, H.T.; Liu, Y.; Zurita, A.J.; Lin, Y.; Baker-Neblett, K.; Martin, A.-M.; Figlin, R.A.; Hutson, T.E.; Sternberg, C.N.; Amado, R.G.; et al. Prognostic or predictive plasma cytokines and angiogenic factors for patients treated with pazopanib for metastatic renal-cell cancer: A retrospective analysis of phase 2 and phase 3 trials. Lancet Oncol. 2012, 13, 827–837. [Google Scholar] [CrossRef]
- Van Der Graaf, W.T.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Nguyen, B.B.; Casali, P.G.; Schoffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. PALETTE: Final overall survival (OS) data and predictive factors for OS of EORTC 62072/GSK VEG110727, a randomized double-blind phase III trial of pazopanib versus placebo in advanced soft tissue sarcoma (STS) patients. J. Clin. Oncol. 2012, 30, 10009. [Google Scholar] [CrossRef]
- Lin, Y.; Ball, H.A.; Suttle, B.; Mehmud, F.; Amado, R.G.; Hutson, T.E.; Pandite, L.N. Relationship between plasma pazopanib concentration and incidence of adverse events in renal cell carcinoma. J. Clin. Oncol. 2011, 29, 345. [Google Scholar] [CrossRef]
- Noda, S.; Yoshida, T.; Hira, D.; Murai, R.; Tomita, K.; Tsuru, T.; Kageyama, S.; Kawauchi, A.; Ikeda, Y.; Morita, S.-Y.; et al. Exploratory Investigation of Target Pazopanib Concentration Range for Patients With Renal Cell Carcinoma. Clin. Genitourin. Cancer 2019, 17, e306–e313. [Google Scholar] [CrossRef]
- Nakamura, M.; Yamada, T.; Ishiyama, S.; Enomoto, M.; Yokomizo, H.; Kosugi, C.; Sonoda, H.; Ishimaru, K.; Ishibashi, K.; Kuramochi, H.; et al. Regorafenib dose escalation therapy for patients with refractory metastatic colorectal cancer (RECC Study). J. Clin. Oncol. 2020, 38, 116. [Google Scholar] [CrossRef]
- Yang, J.-H.; Sequist, L.; Zhou, C.; Schuler, M.; Geater, S.; Mok, T.; Hu, C.-P.; Yamamoto, N.; Feng, J.; O’Byrne, K.; et al. Effect of dose adjustment on the safety and efficacy of afatinib for EGFR mutation-positive lung adenocarcinoma: Post hoc analyses of the randomized LUX-Lung 3 and 6 trials. Ann. Oncol. 2016, 27, 2103–2110. [Google Scholar] [CrossRef]
- Groenland, S.L.; Van Eerden, R.A.; Verheijen, R.B.; Huitema, A.; Mathijssen, R.H.; Steeghs, N. Boosting pazopanib exposure by splitting intake moments: A prospective pharmacokinetic study in cancer patients. J. Clin. Oncol. 2019, 37, 3119. [Google Scholar] [CrossRef]
- Mueller-Schoell, A.; Groenland, S.L.; Scherf-Clavel, O.; van Dyk, M.; Huisinga, W.; Michelet, R.; Jaehdem, U.; Steeghs, N.; Huitema, A.D.R.; Kloft, C. Therapeutic drug monitoring of oral targeted antineoplastic drugs. Eur. J. Clin. Pharmacol. 2021, 77, 441–464. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhang, X.; Sun, G.; Liu, Z.; Zhang, H.; Yang, Y.; Ni, Y.; Dai, J.; Zhu, S.; Chen, J.; et al. Efficacy and Safety of Individualized Schedule of Sunitinib by Drug Monitoring in Patients with Metastatic Renal Cell Carcinoma. Cancer Manag. Res. 2021, 13, 6833–6845. [Google Scholar] [CrossRef] [PubMed]
- Boudou-Rouquette, P.; Ropert, S.; Mir, O.; Coriat, R.; Billemont, B.; Tod, M.; Cabanes, L.; Franck, N.; Blanchet, B.; Goldwasser, F. Variability of Sorafenib Toxicity and Exposure over Time: A Pharmacokinetic/Pharmacodynamic Analysis. Oncologist 2012, 17, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Arrondeau, J.; Mir, O.; Boudou-Rouquette, P.; Coriat, R.; Ropert, S.; Dumas, G.; Rodrigues, M.J.; Rousseau, B.; Blanchet, B.; Goldwasser, F. Sorafenib exposure decreases over time in patients with hepatocellular carcinoma. Investig. New Drugs 2011, 30, 2046–2049. [Google Scholar] [CrossRef] [PubMed]
- Mir, O.; Touati, N.; Lia, M.; Litière, S.; Le Cesne, A.; Sleijfer, S.; Blay, J.Y.; Leahy, M.; Young, R.; Mathijssen, R.H.J.; et al. Impact of Concomitant Administration of Gastric Acid-Suppressive Agents and Pazopanib on Outcomes in Soft-Tissue Sarcoma Patients Treated within the EORTC 62043/62072 Trials. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 1479–1485. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Sex, n (%) Male | 49 (52%) |
| Median age, years (range) | 53.5 (19–83) |
| Age, n (%) ≥70 years | 12 (13%) |
| Performance status, n (%) 0–1 ≥2 | 71 (75%) 24 (25%) |
| Body Mass Index, n (%) <25 ≥25 | 50 (53%) 45 (47%) |
| Subtypes, n (%) Leiomyosarcoma Synovial sarcoma Malignant solitary fibrous tumor Epithelioid and clear cell sarcoma Myxofibrosarcoma Undifferentiated pleomorphic and fusiform cell sarcoma Other * | 28 (30%) 14 (15%) 12 (13%) 8 (9%) 7 (8%) 6 (6%) 13 (13%) |
| Site of primitive tumor, n (%) Lower member Upper member Trunk (thorax, abdomen, head and neck) Uterus | 43 (45%) 11 (11%) 30 (32%) 11 (11%) |
| Histological grade, n (%) 1–2 3 Not concerned ** | 30 (31.5%) 35 (37%) 30 (31.5%) |
| Pazopanib metastatic line, n (%) First Second ≥Third | 20 (21%) 39 (41%) 36 (38%) |
| Initial daily dose of pazopanib, n (%) 200 mg 400 mg 600 mg 800 mg | 2 (2%) 15 (16%) 24 (25%) 54 (57%) |
| Initial dose-weight, mg/kg (standard deviation) | 9.68 (3.1) |
| Albumin, n (%) <35 ≥35 | 14 (15%) 81 (85%) |
| SGOT-SGPT, n (%) ≤ULN (≤40) >ULN (>40) | 78 (82%) 17 (18%) |
| C Reactive Protein, n (%) <10 ≥10 | 56 (61%) 36 (39%) |
| Neutrophils/Lymphocytes Ratio (NLR) <3.5 ≥3.5 | 55 (58%) 40 (42%) |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR [95 CI] | p-Value | OR [95 CI] | p-Value | |
| Initial daily dose | ||||
| <800 vs. 800 mg | 1.95 [0.85–4.5] | 0.12 | 2.15 [0.71–6.57] | 0.18 |
| PAZ Cmin at D15 | ||||
| <27 vs. ≥27 mg/L | 3.09 [1.31–7.28] | 0.01 | 4.21 [1.47–12.12] | 0.008 |
| Histological subtype | ||||
| Leiomyosarcoma vs. other | 1.22 (0.48–3.07) | 0.68 | 1.99 (0.62–6.40) | 0.25 |
| Synovial sarcoma vs. other | 0.54 (0.15–1.99) | 0.35 | 0.67 (0.14–3.26) | 0.62 |
| Tumor grade * | ||||
| Grade 3 vs. 1–2 | 2.91 (1.03–8.20) | 0.04 | ||
| Metastatic sites | ||||
| Bone metastasis | 2.85 (1.15–7.06) | 0.02 | 2.63 (0.87–7.95) | 0.09 |
| Lymph node metastasis | 2.78 (1.16–6.70) | 0.02 | 4.55 (1.43–14.46) | 0.01 |
| ECOG PS | ||||
| ≥2 vs. 0–1 | 3.10 (1.16–8.32) | 0.02 | 1.89 (0.55–6.55) | 0.31 |
| Previous treatments | ||||
| ≥2 vs. 0–1 previous lines | 0.93 (0.40–2.18) | 0.87 | ||
| Dosage per kilogram of body weight | ||||
| /1 mg/kg increase | 0.88 (0.77–1.02) | 0.09 | ||
| BMI | ||||
| >25 vs. ≤25 kg/m2 | 2.63 (1.13–6.13) | 0.03 | 3.05 (1.02–9.15) | 0.046 |
| Albumin | ||||
| ≥ 5 vs. <5 g/L | 0.77 (0.25–2.41) | 0.66 | ||
| NLR | ||||
| ≥3.5 vs. <3.5 | 0.40 (0.17–0.95) | 0.04 | 0.31 (0.10–0.93) | 0.04 |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95 CI) | p-Value | HR (95 CI) | p-Value | |
| Age | ||||
| ≥70 vs. < 70 yrs | 1.01 (0.99–1.02) | 0.58 | ||
| Sex | ||||
| Female vs. Male | 1.02 (0.62–1.68) | 0.94 | ||
| Initial daily dose | ||||
| <800 vs. 800 mg | 1.38 (0.83–2.30) | 0.22 | 1.01 (0.58–1.77) | 0.97 |
| PAZ Cmin at D15 | ||||
| <27 vs. ≥27 mg/L | 1.57 (0.95–2.61) | 0.08 | 1.62 (0.97–2.72) | 0.07 |
| Histological subtype | ||||
| Leiomyosarcoma vs. other | 1.08 (0.62–1.87) | 0.8 | 1.19 (0.67–2.13) | 0.55 |
| Synovial sarcoma vs. other | 0.71 (0.30–1.70) | 0.45 | 0.86 (0.35–2.09) | 0.74 |
| Tumor grade * | ||||
| Grade 3 vs. 1–2 | 1.72 (0.94–3.18) | 0.08 | ||
| Metastatic sites | ||||
| Bone metastasis | 1.78 (1.07–2.97) | 0.03 | 1.42 (0.82–2.47) | 0.22 |
| Lymph node metastasis | 0.98 (0.57–1.67) | 0.93 | ||
| ECOG PS | ||||
| ≥2 vs. 0–1 | 2.54 (1.49–4.33) | 0.0006 | 2.31 (1.26–4.23) | 0.007 |
| Previous treatments | ||||
| ≥2 vs. 0–1 previous lines | 1.44 (0.86–2.41) | 0.17 | ||
| BMI | ||||
| >25 vs. ≤25 kg/m2 | 1.41 (0.85–2.33) | 0.19 | ||
| Dosage per kilogram of body weight | ||||
| /1 mg/kg increase | 0.96 (0.88–1.04) | 0.33 | ||
| Albumin | ||||
| ≥35 vs. <35 g/L | 1.07 (0.53–2.18) | 0.85 | ||
| NLR | ||||
| ≥3.5 vs. <3.5 | 1.00 (0.60–1.67) | 0.99 |
| Variable | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (95 CI) | p-Value | OR (95 CI) | p-Value | |
| Sex | ||||
| Female vs. Male | 1.22 (0.54–2.75) | 0.64 | ||
| Age | ||||
| ≥70 vs. <70 years | 1.65 (0.51–5.34) | 0.41 | ||
| Initial daily dose | ||||
| <800 vs. 800 mg | 0.62 (0.27–1.42) | 0.26 | ||
| First 3 PAZ Cmin | ||||
| /1 mg/L increase | 1.07 (1.02–1.13) | 0.007 | 1.07 (1.01–1.13) | 0.01 |
| ECOG PS | ||||
| ≥2 vs. 0–1 | 2.88 (1.11–7.51) | 0.03 | 3.53 (0.62–20.25) | 0.16 |
| BMI | ||||
| >25 vs. ≤25 kg/m2 | 2.66 (1.5–6.13) | 0.02 | 1.63 (0.45–5.98) | 0.46 |
| Albumin | ||||
| ≥35 vs. <35 g/L | 1.44 (0.444.68) | 0.54 | ||
| NLR | ||||
| ≥3.5 vs. <3.5 | 1.14 (0.5–2.59) | 0.76 | ||
| SGOT or SGPT | ||||
| >40 vs. ≤40 | 1.39 (0.47–4.09) | 0.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minot-This, M.-S.; Boudou-Rouquette, P.; Jouinot, A.; de Percin, S.; Balakirouchenane, D.; Khoudour, N.; Tlemsani, C.; Chauvin, J.; Thomas-Schoemann, A.; Goldwasser, F.; et al. Relation between Plasma Trough Concentration of Pazopanib and Progression-Free Survival in Metastatic Soft Tissue Sarcoma Patients. Pharmaceutics 2022, 14, 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061224
Minot-This M-S, Boudou-Rouquette P, Jouinot A, de Percin S, Balakirouchenane D, Khoudour N, Tlemsani C, Chauvin J, Thomas-Schoemann A, Goldwasser F, et al. Relation between Plasma Trough Concentration of Pazopanib and Progression-Free Survival in Metastatic Soft Tissue Sarcoma Patients. Pharmaceutics. 2022; 14(6):1224. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061224
Chicago/Turabian StyleMinot-This, Marie-Sophie, Pascaline Boudou-Rouquette, Anne Jouinot, Sixtine de Percin, David Balakirouchenane, Nihel Khoudour, Camille Tlemsani, Jonathan Chauvin, Audrey Thomas-Schoemann, François Goldwasser, and et al. 2022. "Relation between Plasma Trough Concentration of Pazopanib and Progression-Free Survival in Metastatic Soft Tissue Sarcoma Patients" Pharmaceutics 14, no. 6: 1224. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics14061224