

Sustained Inhibition of VEGF and TNF-α Achieves Multi-Ocular Protection and Prevents Formation of Blood Vessels after Severe Ocular Trauma
 , , and
, , and 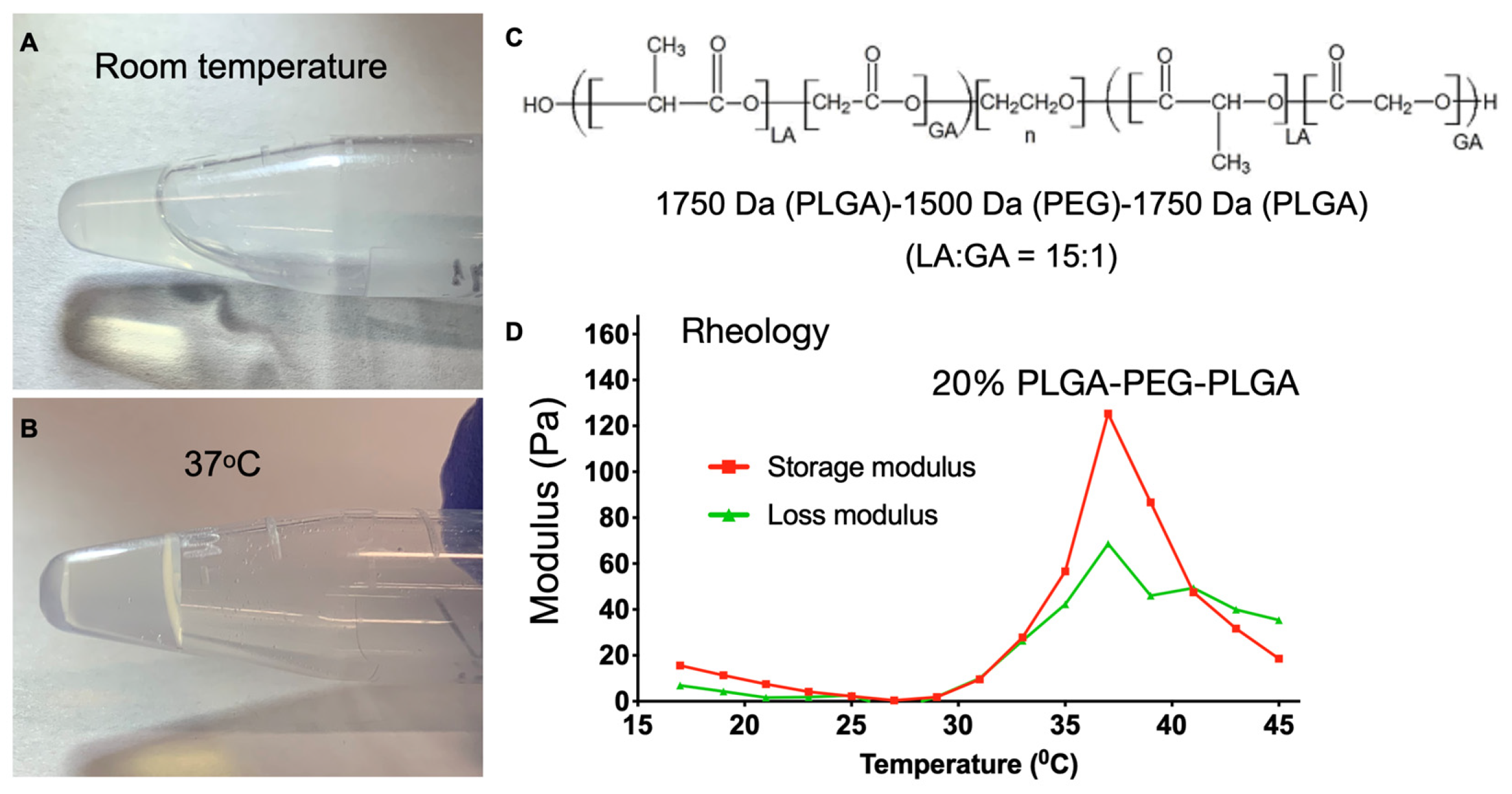{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Thermosensitive Polymer Solution Preparation
2.2. Rheology Test
2.3. Corneal Neovascularization Model
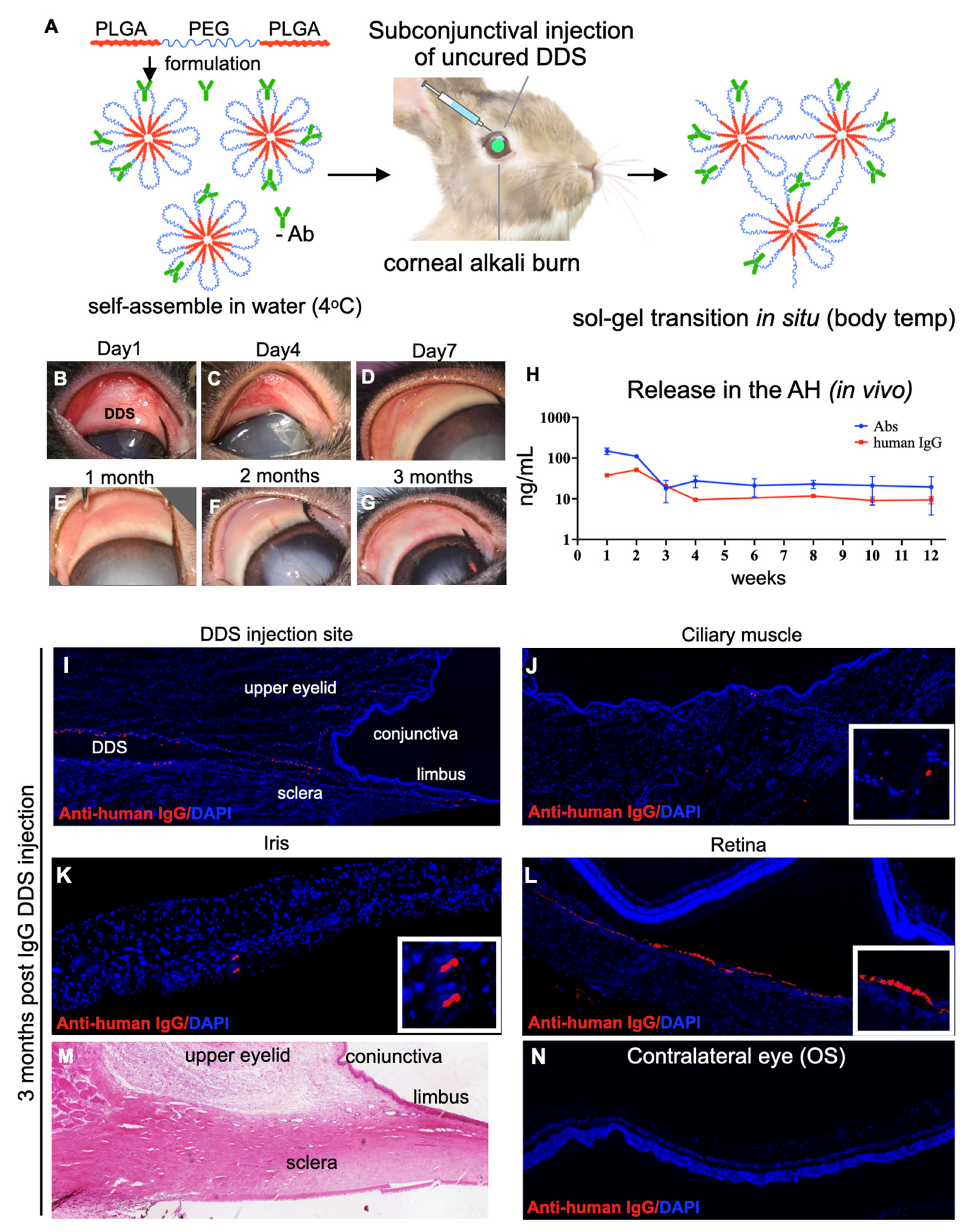
2.4. Subconjunctival DDS Placement
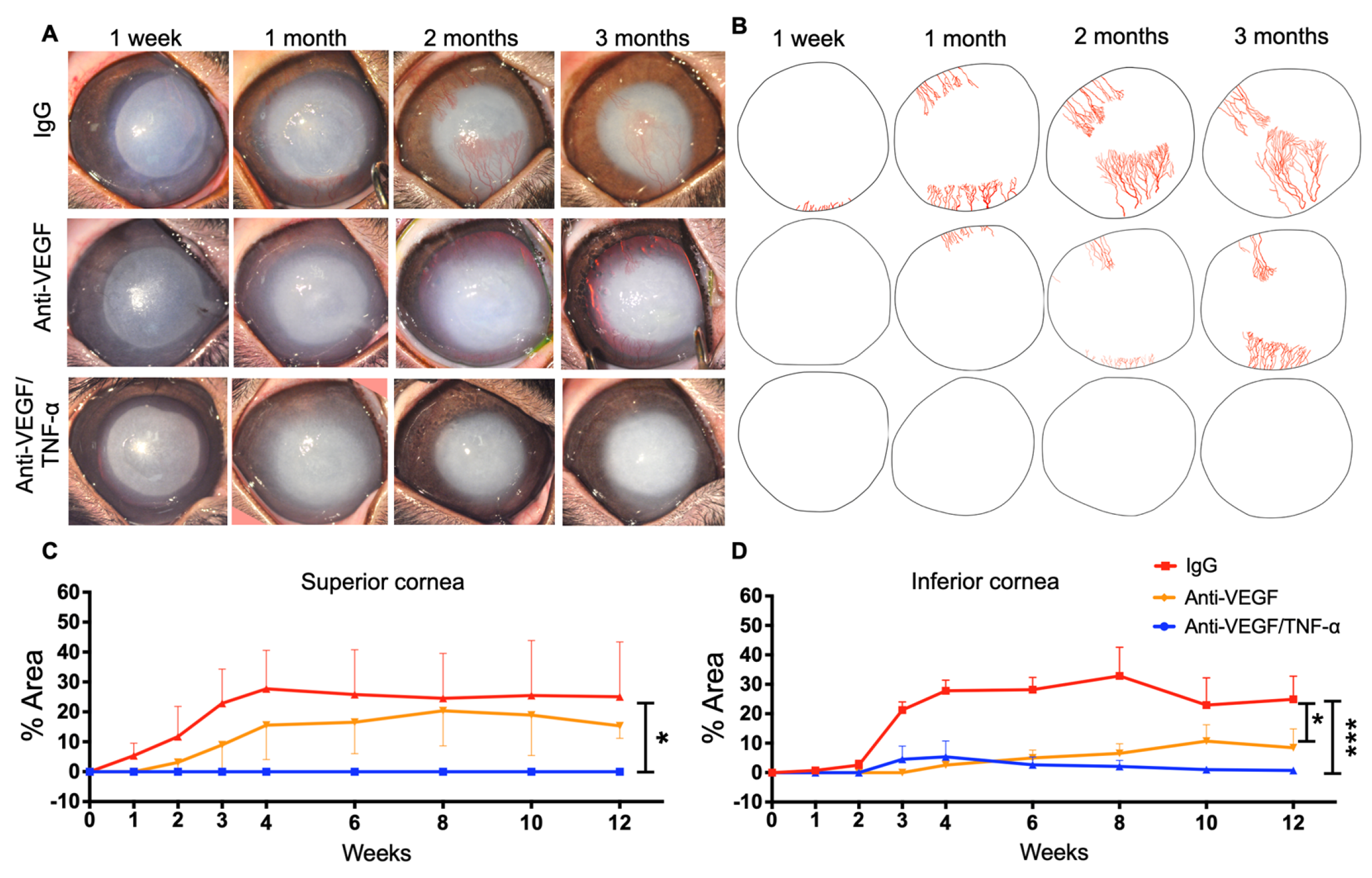
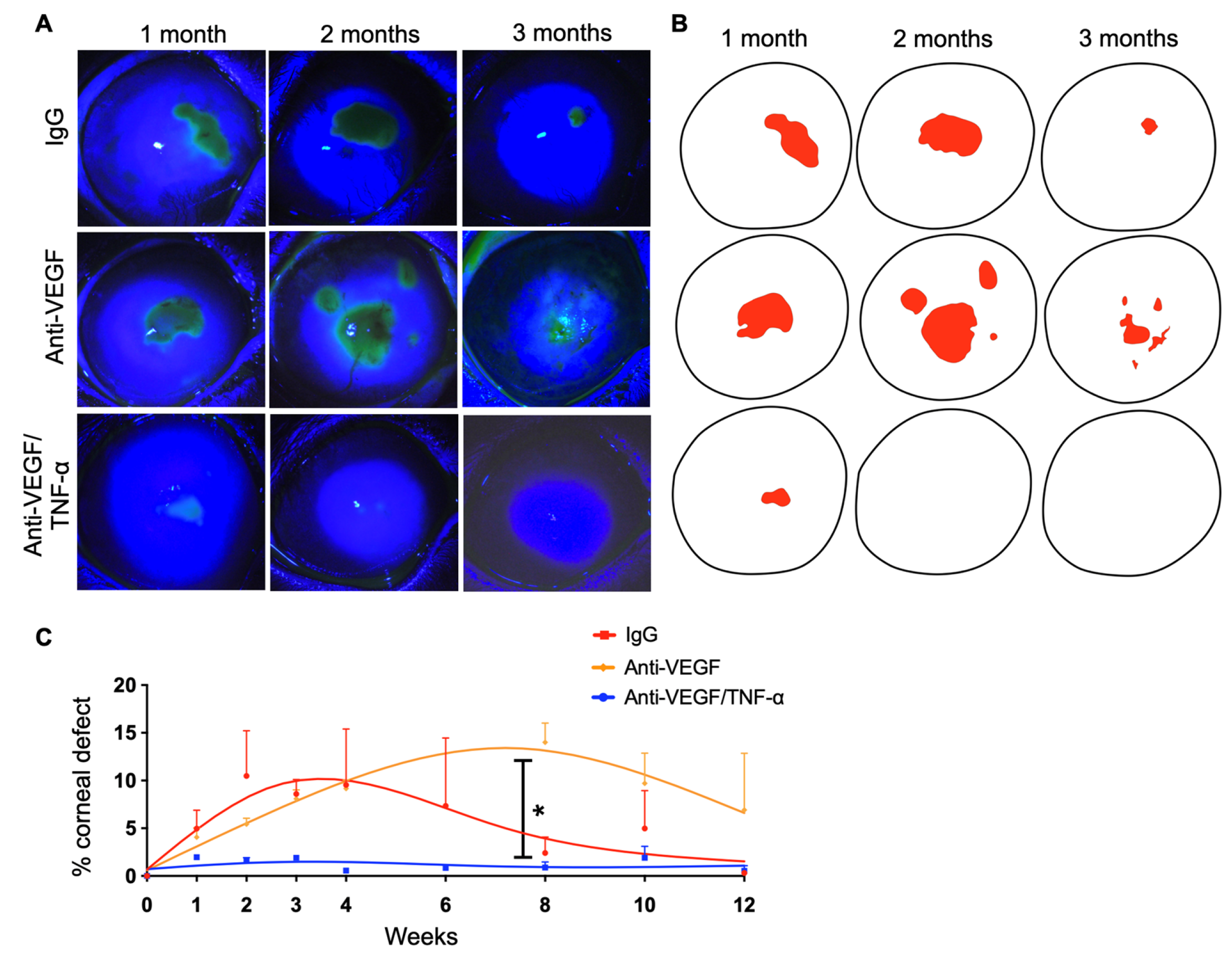
2.5. Evaluation of Corneal NV and Epithelial Defects
2.6. Aqueous Humor Collection and ELISA Assay
2.7. Histological and Immunohistochemical Evaluation of the Cornea
2.8. Statistical Analysis
3. Results
3.1. DDS Sol–Gel Transition and Drug Release Assessment In Vitro Using Fluorescein-Conjugated Dextran
3.2. Long-Term Sustained Release of Antibodies into the Eye after Single Subconjunctival Injection of the DDS
3.3. Anti-TNF-α/Anti-VEGF DDS Treatment Completely Suppresses Corneal Angiogenesis after Injury
3.4. Anti-TNF-α/Anti-VEGF DDS Treatment Improves Corneal Epithelial Healing after Injury
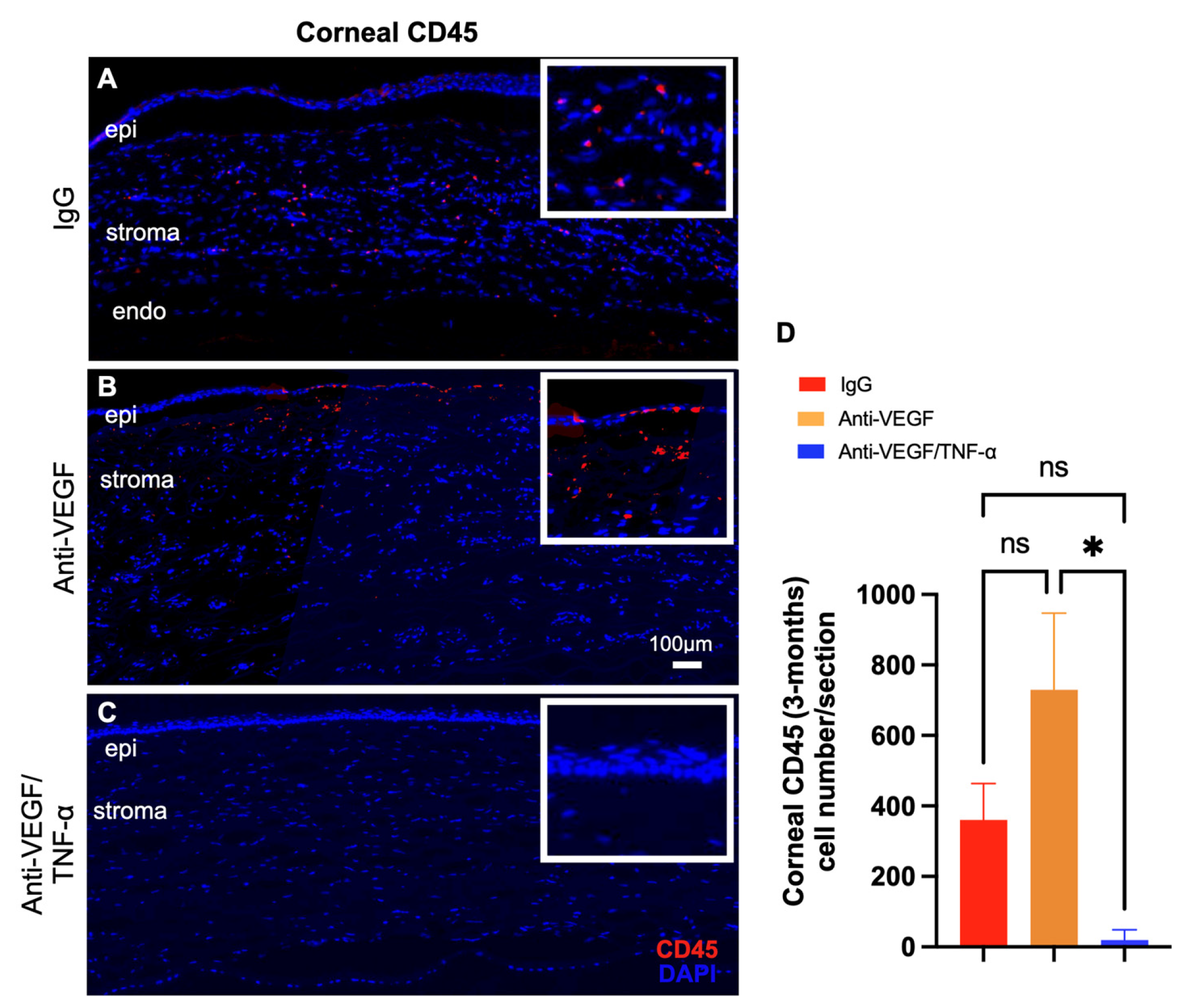
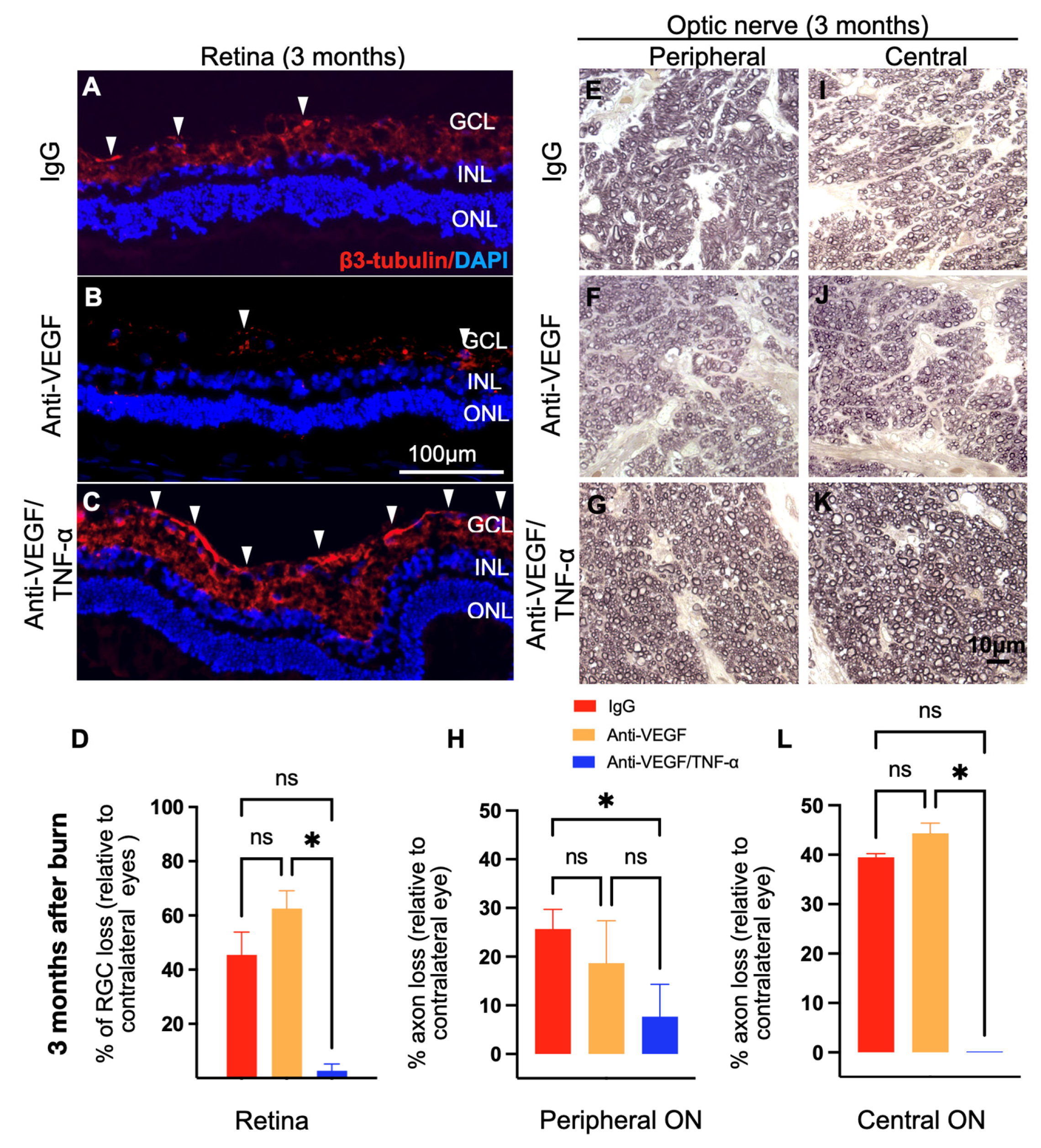
3.5. Anti-TNF-α/Anti-VEGF DDS Treatment Prevents Retinal and Optic Nerve Damage after Injury
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bachmann, B.O.; Bock, F.; Wiegand, S.J.; Maruyama, K.; Dana, M.R.; Kruse, F.E.; Luetjen-Drecoll, E.; Cursiefen, C. Promotion of graft survival by vascular endothelial growth factor a neutralization after high-risk corneal transplantation. Arch. Ophthalmol. 2008, 126, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Vlasov, A.; Ryan, D.S.; Ludlow, S.; Coggin, A.; Weichel, E.D.; Stutzman, R.D.; Bower, K.S.; Colyer, M.H. Corneal and Corneoscleral Injury in Combat Ocular Trauma from Operations Iraqi Free-dom and Enduring Freedom. Mil. Med. 2017, 182, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardillo, J.A.; Stout, J.T.; LaBree, L.; Azen, S.P.; Omphroy, L.; Cui, J.Z.; Kimura, H.; Hinton, D.R.; Ryan, S.J. Post-traumatic proliferative vitreoretinopathy. The epidemiologic profile, onset, risk factors, and visual outcome. Ophthalmology 1997, 104, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Cade, F.; Grosskreutz, C.L.; Tauber, A.; Dohlman, C.H. Glaucoma in eyes with severe chemical burn, before and after keratoprosthesis. Cornea 2011, 30, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Dohlman, C.H.; Cade, F.; Regatieri, C.V.; Zhou, C.; Lei, F.; Crnej, A.; Harissi-Dagher, M.; Robert, M.-C.; Papaliodis, G.N.; Chen, D.; et al. Chemical Burns of the Eye: The Role of Retinal Injury and New Therapeutic Possibilities. Cornea 2018, 37, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Crnej, A.; Paschalis, E.I.; Salvador-Culla, B.; Tauber, A.; Drnovsek-Olup, B.; Shen, L.Q.; Dohlman, C.H. Glaucoma progression and role of glaucoma surgery in patients with Boston keratoprosthesis. Cornea 2014, 33, 349–354. [Google Scholar] [CrossRef]
- Cade, F.; Paschalis, E.I.; Regatieri, C.V.; Vavvas, D.G.; Dana, R.; Dohlman, C.H. Alkali burn to the eye: Protection using TNF-alpha inhibition. Cornea 2014, 33, 382–389. [Google Scholar] [CrossRef]
- Paschalis, E.I.; Lei, F.; Zhou, C.; Kapoulea, V.; Dana, R.; Chodosh, J.; Vavvas, D.G.; Dohlman, C.H. Permanent neuroglial remodeling of the retina following infiltration of CSF1R inhibition-resistant peripheral monocytes. Proc. Natl. Acad. Sci. USA 2018, 115, E11359–E11368. [Google Scholar] [CrossRef] [Green Version]
- Bock, F.; König, Y.; Dietrich, T.; Zimmermann, P.; Baier, M.; Cursiefen, C. Inhibition of angiogenesis in the anterior chamber of the eye. Ophthalmologe 2007, 104, 336–344. [Google Scholar] [CrossRef]
- Manzano, R.P.; Peyman, G.A.; Khan, P.; Carvounis, P.E.; Kivilcim, M.; Ren, M.; Lake, J.C.; Chevez-Barrios, P. Inhibition of experimental corneal neovascularisation by bevacizumab (Avastin). Br. J. Ophthalmol. 2007, 91, 804–807. [Google Scholar] [CrossRef] [Green Version]
- Habot-Wilner, Z.; Barequet, I.S.; Ivanir, Y.; Moisseiev, J.; Rosner, M. The inhibitory effect of different concentrations of topical bevacizumab on corneal neovascularization. Acta Ophthalmol. 2010, 88, 862–867. [Google Scholar] [CrossRef]
- Bock, F.; Konig, Y.; Kruse, F.; Baier, M.; Cursiefen, C. Bevacizumab (Avastin) eye drops inhibit corneal neovascularization. Graefes Arch. Clin. Exp. Ophthalmol. 2008, 246, 281–284. [Google Scholar] [CrossRef]
- Kim, S.W.; Ha, B.J.; Kim, E.K.; Tchah, H.; Kim, T.I. The effect of topical bevacizumab on corneal neovascularization. Ophthalmology 2008, 115, e33–e38. [Google Scholar] [CrossRef]
- Dastjerdi, M.H.; Al-Arfaj, K.M.; Nallasamy, N.; Hamrah, P.; Jurkunas, U.V.; Pineda, R., 2nd; Pavan-Langston, D.; Dana, R. Topical bevacizumab in the treatment of corneal neovascularization: Results of a prospective, open-label, noncomparative study. Arch. Ophthalmol. 2009, 127, 381–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschalis, E.I.; Lei, F.; Zhou, C.; Kapoulea, V.; Thanos, A.; Dana, R.; Vavvas, D.G.; Chodosh, J.; Dohlman, C.H. The Role of Microglia and Peripheral Monocytes in Retinal Damage after Corneal Chemical Injury. Am. J. Pathol. 2018, 188, 1580–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arevalo, J.F.; Serrano, M.A.; Wu, L. Combined inhibition of tumor necrosis factor (TNF) and vascular endothelial growth factor (VEGF) for the treatment of macular edema of various etiologies: A short-term pilot study. Eye 2013, 27, 569–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, L.G.A.d.; Isaac, D.L.C.; Tannure, W.T.; Gabriel, L.A.R.; Reis, R.G.d.; Rassi, A.R.; Freitas, C.A.d.; Ávila, M.P.d. Intravitreal bevacizumab combined with infliximab in the treatment of choroidal neovascularization secondary to age-related macular degeneration: Case report series. Arq. Bras. Oftalmol. 2013, 76, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Robert, M.C.; Kapoulea, V.; Lei, F.; Stagner, A.M.; Jakobiec, F.A.; Dohlman, C.H.; Paschalis, E.I. Sustained Subconjunctival Delivery of Infliximab Protects the Cornea and Retina Following Alkali Burn to the Eye. Investig. Ophthalmol. Vis. Sci. 2017, 58, 96–105. [Google Scholar] [CrossRef] [Green Version]
- Nomoto, H.; Shiraga, F.; Kuno, N.; Kimura, E.; Fujii, S.; Shinomiya, K.; Nugent, A.K.; Hirooka, K.; Baba, T. Pharmacokinetics of bevacizumab after topical, subconjunctival, and intravitreal administration in rabbits. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4807–4813. [Google Scholar] [CrossRef]
- Stevenson, W.; Cheng, S.F.; Dastjerdi, M.H.; Ferrari, G.; Dana, R. Corneal neovascularization and the utility of topical VEGF inhibition: Ranibizumab (Lucentis) vs bevacizumab (Avastin). Ocul. Surf. 2012, 10, 67–83. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.H.; Garg, N.K.; Lunde, E.; Han, K.Y.; Jain, S.; Azar, D.T. Corneal neovascularization: An anti-VEGF therapy review. Surv. Ophthalmol. 2012, 57, 415–429. [Google Scholar] [CrossRef] [Green Version]
- Ranta, V.P.; Mannermaa, E.; Lummepuro, K.; Subrizi, A.; Laukkanen, A.; Antopolsky, M.; Murtomaki, L.; Hornof, M.; Urtti, A. Barrier analysis of periocular drug delivery to the posterior segment. J. Control Release 2010, 148, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, E.M.; Rimpela, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic aspects of retinal drug delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.; Pan, W.; Su, T.; Zhang, M.; Dong, W.; Qi, X. Recent advances in natural polymer-based drug delivery systems. React. Funct. Polym. 2020, 148, 104501. [Google Scholar] [CrossRef]
- Garner, J. Users Guide for Thermogelling PolyVivo PLGA-PEG-PLGA (AK12/AK19/AK24). Available online: https://akinainc.com/pdf/40307-PolyVivo-thermogel-usersguide.pdf (accessed on 28 August 2021).
- Paschalis, E.I.; Zhou, C.; Lei, F.; Scott, N.; Kapoulea, V.; Robert, M.-C.; Vavvas, D.; Dana, R.; Chodosh, J.; Dohlman, C.H. Mechanisms of Retinal Damage after Ocular Alkali Burns. Am. J. Pathol. 2017, 187, 1327–1342. [Google Scholar] [CrossRef] [Green Version]
- Paschalis, E.I.; Lei, F.; Zhou, C.; Chen, X.N.; Kapoulea, V.; Hui, P.-C.; Dana, R.; Chodosh, J.; Vavvas, D.G.; Dohlman, C.H. Microglia Regulate Neuroglia Remodeling in Various Ocular and Retinal Injuries. J. Immunol. 2019, 202, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Lei, F.; Zhou, C.; Chodosh, J.; Wang, L.; Huang, Y.; Dohlman, C.H.; Paschalis, E.I. Glaucoma after ocular surgery or trauma: The role of infiltrating monocytes and their response to cytokine inhibitors. Am. J. Pathol. 2020, 190, 2056–2066. [Google Scholar] [CrossRef]
- Zhou, C.; Singh, A.; Qian, G.; Wolkow, N.; Dohlman, C.H.; Vavvas, D.G.; Chodosh, J.; Paschalis, E.I. Microporous Drug Delivery System for Sustained Anti-VEGF Delivery to the Eye. Transl. Vis. Sci. Technol. 2020, 9, 5. [Google Scholar] [CrossRef]
- Englander, M.; Chen, T.C.; Paschalis, E.I.; Miller, J.W.; Kim, I.K. Intravitreal injections at the Massachusetts Eye and Ear Infirmary: Analysis of treatment indications and postinjection endophthalmitis rates. Br. J. Ophthalmol. 2013, 97, 460–465. [Google Scholar] [CrossRef]
- Robert, M.-C.; Frenette, M.; Zhou, C.; Yan, Y.; Chodosh, J.; Jakobiec, F.A.; Stagner, A.M.; Vavvas, D.; Dohlman, C.H.; Paschalis, E.I. A Drug Delivery System for Administration of Anti-TNF-α Antibody. Transl. Vis. Sci. Technol. 2016, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Dohlman, C.H.; Zhou, C.; Lei, F.; Cade, F.; Regatieri, C.V.; Crnej, A.; Dohlman, J.G.; Shen, L.Q.; Paschalis, E.I. Glaucoma After Corneal Trauma or Surgery—A Rapid, Inflammatory, IOP-Independent Pathway. Cornea 2019, 38, 1589. [Google Scholar] [CrossRef]
- Xie, B.; Jin, L.; Luo, Z.; Yu, J.; Shi, S.; Zhang, Z.; Shen, M.; Chen, H.; Li, X.; Song, Z. An injectable thermosensitive polymeric hydrogel for sustained release of Avastin® to treat posterior segment disease. Int. J. Pharm. 2015, 490, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Y.; Bock, F.; Horn, F.; Kruse, F.; Straub, K.; Cursiefen, C. Short- and long-term safety profile and efficacy of topical bevacizumab (Avastin) eye drops against corneal neovascularization. Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-T.; Hu, F.-R.; Kuo, K.-T.; Chen, Y.-M.; Chu, H.-S.; Lin, Y.-H.; Chen, W.-L. The Different Effects of Early and Late Bevacizumab (Avastin) Injection on Inhibiting Corneal Neovascularization and Conjunctivalization in Rabbit Limbal Insufficiency. Investig. Ophthalmol. Vis. Sci. 2010, 51, 6277–6285. [Google Scholar] [CrossRef] [PubMed]
- Canete, J.D.; Pablos, J.L.; Sanmarti, R.; Mallofre, C.; Marsal, S.; Maymo, J.; Gratacos, J.; Mezquita, J.; Mezquita, C.; Cid, M.C. Antiangiogenic effects of anti-tumor necrosis factor alpha therapy with infliximab in psoriatic arthritis. Arthritis Rheum. 2004, 50, 1636–1641. [Google Scholar] [CrossRef]
- Appel, H.; Janssen, L.; Listing, J.; Heydrich, R.; Rudwaleit, M.; Sieper, J. Serum levels of biomarkers of bone and cartilage destruction and new bone formation in different cohorts of patients with axial spondyloarthritis with and without tumor necrosis factor-alpha blocker treatment. Arthritis Res. Ther. 2008, 10, R125. [Google Scholar] [CrossRef] [Green Version]
- Klimiuk, P.A.; Sierakowski, S.; Domyslawska, I.; Chwiecko, J. Effect of etanercept on serum levels of soluble cell adhesion molecules (sICAM-1, sVCAM-1, and sE-selectin) and vascular endothelial growth factor in patients with rheumatoid arthritis. Scand. J. Rheumatol. 2009, 38, 439–444. [Google Scholar] [CrossRef]
- Murdaca, G.; Spanò, F.; Miglino, M.; Puppo, F. Effects of TNF-α inhibitors upon the mechanisms of action of VEGF. Immunotherapy 2013, 5, 113–115. [Google Scholar] [CrossRef]
- Ferrari, G.; Bignami, F.; Rama, P. Tumor Necrosis Factor-α Inhibitors as a Treatment of Corneal Hemangiogenesis and Lymphangiogenesis. Eye Contact Lens Sci. Clin. Pract. 2014, 41, 72–76. [Google Scholar] [CrossRef]
- Wang, H.; Han, X.; Wittchen, E.S.; Hartnett, M.E. TNF-α mediates choroidal neovascularization by upregulating VEGF expression in RPE through ROS-dependent β-catenin activation. Mol. Vis. 2016, 22, 116–128. [Google Scholar]
- Paschalis, E.I.; Robert, M.-C.; Dohlman, C.H. Treatment of Chemical Burn to the Eye: A Changing Picture; Springer: Cham, Switzerland, 2018; pp. 1–24. [Google Scholar]
- Dohlman, C.H.; Robert, M.-C.; Paschalis, E.I. Treatment of Chemical Burn to the Eye: A Changing Picture. In Foundations of Corneal Disease: Past, Present and Future; Colby, K., Dana, R., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 109–119. [Google Scholar]
- Rezaeian Shiadeh, S.N.; Hadizadeh, F.; Khodaverdi, E.; Gorji Valokola, M.; Rakhshani, S.; Kamali, H.; Nokhodchi, A. Injectable In-Situ Forming Depot Based on PLGA and PLGA-PEG-PLGA for Sustained-Release of Risperidone: In Vitro Evaluation and Pharmacokinetics in Rabbits. Pharmaceutics 2023, 13, 1229. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, C.; Lei, F.; Sharma, J.; Hui, P.-C.; Wolkow, N.; Dohlman, C.H.; Vavvas, D.G.; Chodosh, J.; Paschalis, E.I. Sustained Inhibition of VEGF and TNF-α Achieves Multi-Ocular Protection and Prevents Formation of Blood Vessels after Severe Ocular Trauma. Pharmaceutics 2023, 15, 2059. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics15082059
Zhou C, Lei F, Sharma J, Hui P-C, Wolkow N, Dohlman CH, Vavvas DG, Chodosh J, Paschalis EI. Sustained Inhibition of VEGF and TNF-α Achieves Multi-Ocular Protection and Prevents Formation of Blood Vessels after Severe Ocular Trauma. Pharmaceutics. 2023; 15(8):2059. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics15082059
Chicago/Turabian StyleZhou, Chengxin, Fengyang Lei, Jyoti Sharma, Pui-Chuen Hui, Natalie Wolkow, Claes H. Dohlman, Demetrios G. Vavvas, James Chodosh, and Eleftherios I. Paschalis. 2023. "Sustained Inhibition of VEGF and TNF-α Achieves Multi-Ocular Protection and Prevents Formation of Blood Vessels after Severe Ocular Trauma" Pharmaceutics 15, no. 8: 2059. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics15082059