Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients


Abstract
:1. Introduction
2. Materials and Methods
3. Endoscopic and Histopathologic Evaluation
4. Statistical Analyses
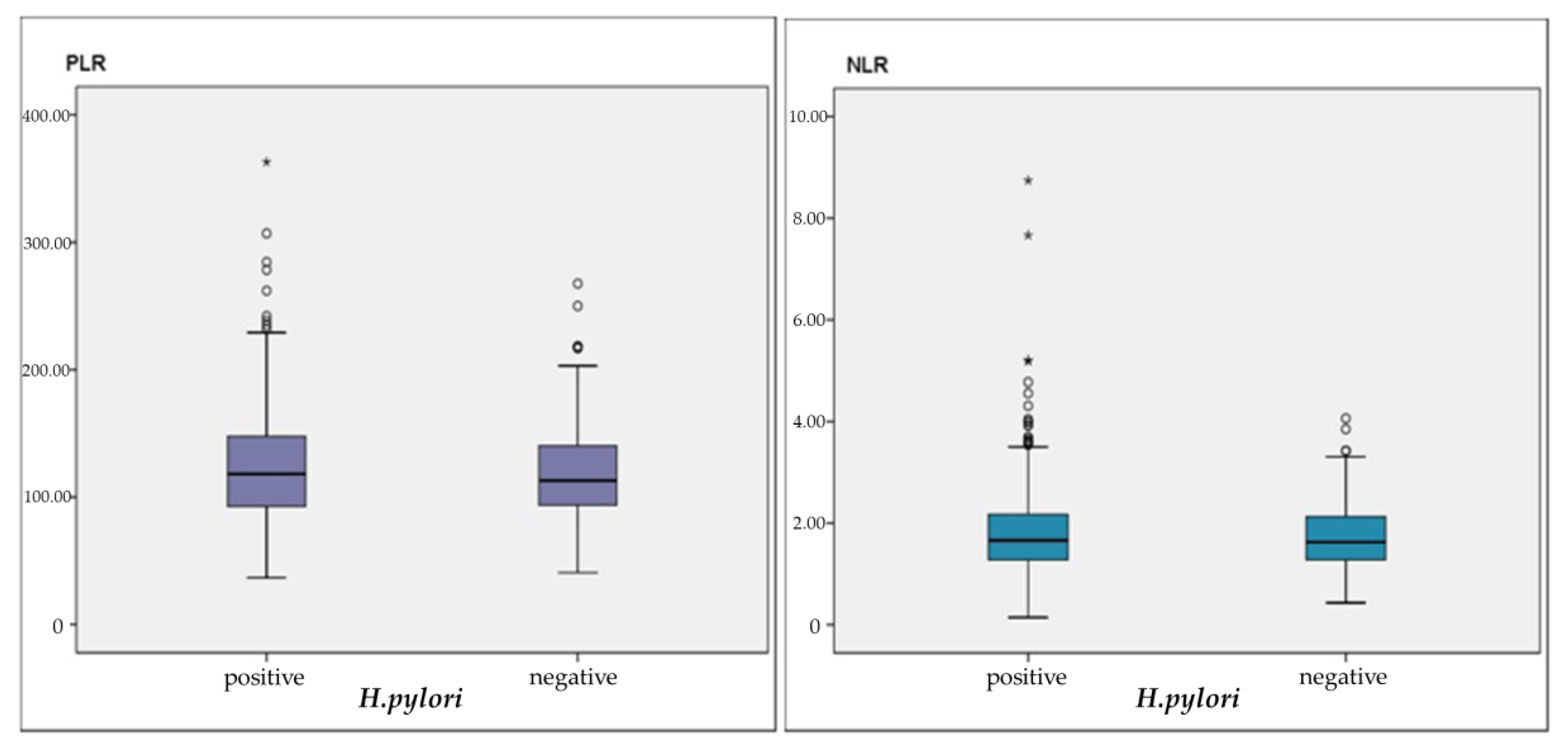
5. Results
6. Discussions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Go, M.F. Natural history and epidemiology of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2002, 16 (Suppl. 1), 3–15. [Google Scholar] [CrossRef]
- Lúquez, M.A.; Otero, R.W.; Schmulson, M. Enfoque diagnóstico y terapéutico de dispepsia y dispepsia funcional: Qué hay nuevo en el 2019? [Diagnostic and therapeutic approach to dyspepsia and functional dyspepsia:what’s new in 2019?]. Rev. Gastroenterol. Peru. 2019, 39, 141–152. [Google Scholar]
- Balta, S.; Demirkol, S.; Unlu, M.; Arslan, Z.; Celik, T. Neutrophil to lymphocyte ratio may be predict of mortality in all conditions. Br. J. Cancer 2013, 109, 3125–3126. [Google Scholar] [CrossRef] [PubMed]
- Mosso, E.; Bonetto, S.; Longobardi, G.; Abenavoli, L.; Ribaldone, D.G.; Saracco, G.M.; Pellicano, R. Management of functional dyspepsia in the year 2020. A clinical point of view. Minerva Gastroenterol. Dietol. 2020. [Google Scholar] [CrossRef]
- Kang, S.J.; Park, B.; Shin, C.M. Helicobacter pylori Eradication Therapy for Functional Dyspepsia: A Meta-Analysis by Region and H. pylori Prevalence. J. Clin. Med. 2019, 8, 1324. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Li, X. Stage-Dependent Changes in Albumin, NLR, PLR, and AFR are correlated with Shorter Survival in Patients with Gastric Cancer. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef]
- Jafarzadeh, A.; Akbarpoor, V.; Nabizadeh, M.; Nemati, M.; Rezayati, M.T. Total leukocyte counts and neutrophil-lymphocyte count ratios among Helicobacter pylori-infected patients with peptic ulcers: Independent of bacterial CagA status. Southeast Asian J. Trop. Med. Public Health 2013, 44, 82–88. [Google Scholar]
- Bilge, M.; Yeşilova, A.M.; Adas, M.; Helvaci, A. Neutrophil- and Platelet- to Lymphocyte Ratio in Patients with Euthyroid Hashimoto’s Thyroiditis. Exp. Clin. Endocrinol. Diabetes 2019, 127, 545–549. [Google Scholar] [CrossRef]
- Pacifico, L.; Osborn, J.F.; Tromba, V.; Romaggioli, S.; Bascetta, S.; Chiesa, C. Helicobacter pylori infection and extragastric disorders in children: A critical update. World J. Gastroenterol. 2014, 20, 1379–1401. [Google Scholar] [CrossRef]
- Mendoza, E.; Duque, X.; Franco, J.I.H.; Reyes-Maldonado, E.; Morán, S.; Martínez, G.; Rodríguez, A.S.; Martinez, H. Association between Active H. pylori Infection and Iron Deficiency Assessed by Serum Hepcidin Levels in School-Age Children. Nutrients 2019, 11, 2141. [Google Scholar] [CrossRef] [Green Version]
- Oporto, M.; Pavez, M.; Troncoso, C.; Cerda, A.; Hofmann, E.; Sierralta, A.; Rios, E.; Coppelli, L.; Barrientos, L. Prevalence of Infection and Antibiotic Susceptibility of Helicobacter pylori: An Evaluation in Public and Private Health Systems of Southern Chile. Pathogens 2019, 8, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mentis, A.; Lehours, P.; Megraud, F. Epidemiology and Diagnosis of Helicobacter pylori infection. Helicobacter 2015, 20 (Suppl. 1), 1–7. [Google Scholar] [CrossRef] [Green Version]
- Breckan, R.K.; Paulssen, E.J.; Asfeldt, A.M.; Kvamme, J.-M.; Straume, B.; Florholmen, J. The All-Age Prevalence ofHelicobacter pyloriInfection and Potential Transmission Routes. A Population-Based Study. Helicobacter 2016, 21, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, F.; Covino, M.; Baudron, C.R. Review: Helicobacter pylori and extragastric diseases. Helicobacter 2019, 24 (Suppl. 1), e12636. [Google Scholar] [CrossRef] [Green Version]
- Mekonnen, H.D.; Fisseha, H.; Getinet, T.; Tekle, F.; Galle, P.R. Helicobacter pylori Infection as a Risk Factor for Hepatocellular Carcinoma: A Case-Control Study in Ethiopia. Int. J. Hepatol. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.; Yang, Z.; Lu, N.-H. Helicobacter pyloriinfection and diabetes: Is it a myth or fact. World J. Gastroenterol. 2014, 20, 4607–4617. [Google Scholar] [CrossRef] [PubMed]
- Jia, E.-Z.; Zhao, F.-J.; Hao, B.; Zhu, T.; Wang, L.-S.; Chen, B.; Cao, K.-J.; Huang, J.; Ma, W.-Z.; Yang, Z.; et al. Helicobacter pylori infection is associated with decreased serum levels of high density lipoprotein, but not with the severity of coronary atherosclerosis. Lipids Health Dis. 2009, 8, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, K.; White, J.R.; Winter, J.A. Differential inflammatory response to Helicobacter pylori infection: Etiology and clinical outcomes. J. Inflamm. Res. 2015, 8, 137–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahtes, A.; Geng, S.; Lee, C.; Li, L. Cellular and molecular mechanisms involved in the resolution of innate leukocyte inflammation. J. Leukoc. Biol. 2018, 104, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Guclu, M.; Agan, A.F. Association of Severity of Helicobacter pylori Infection with Peripheral Blood Neutrophil to Lymphocyte Ratio and Mean Platelet Volume. Euroasian J. Hepato-Gastroenterol. 2017, 7, 11–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalbant, A.; Aydin, A. Association of Helicobacter pylori infection with vitamin D, hemogram parameters, and blood group. Turk. J. Acad. Gastroenterol. 2017, 16, 1–5. [Google Scholar]
- Asil, M.; Dertli, R. Neutrophil to lymphocyte ratio is increased in chronic helicobacter pylori infection and returns to normal after successful eradication. J. Turgut Ozal Med. Cent. 2016, 23, 409. [Google Scholar] [CrossRef]
- Krenn-Pilko, S.; Langsenlehner, U.; Thurner, E.-M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Br. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Gao, L.; Zhang, B.; Zhang, L.; Wang, C. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 22618. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xie, Z.; Liu, X.; Huang, X.; Lin, J.; Huang, D.; Yu, B.; Hou, J. Association of Platelet to lymphocyte ratio with non-culprit atherosclerotic plaque vulnerability in patients with acute coronary syndrome: An optical coherence tomography study. BMC Cardiovasc. Disord. 2017, 17, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farah, R.; Khamisy-Farah, R. Association of Neutrophil to Lymphocyte Ratio with Presence and Severity of Gastritis Due to Helicobacter pylori Infection. J. Clin. Lab. Anal. 2014, 28, 219–223. [Google Scholar] [CrossRef]
- Farah, R.; Hamza, H.; Khamisy-Farah, R. A link between platelet to lymphocyte ratio and Helicobacter pylori infection. J. Clin. Lab. Anal. 2018, 32, e22222. [Google Scholar] [CrossRef] [Green Version]
- Shimoyama, Y.; Umegaki, O.; Agui, T.; Kadono, N.; Minami, T. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are superior to other inflammation-based prognostic scores in predicting the mortality of patients with gastrointestinal perforation. JA Clin. Rep. 2017, 3, 49. [Google Scholar] [CrossRef]
- Umit, H.; Umit, E.G. Helicobacter pylori and mean platelet volume: A relation way before immune thrombocytopenia? Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2818–2823. [Google Scholar]
- Burns, M.; Amaya, A.; Bodi, C.; Ge, Z.; Bakthavatchalu, V.; Ennis, K.; Wang, T.C.; Georgieff, M.; Fox, J.G. Helicobacter pylori infection and low dietary iron alter behavior, induce iron deficiency anemia, and modulate hippocampal gene expression in female C57BL/6 mice. PLoS ONE 2017, 12, e0173108. [Google Scholar] [CrossRef]
- Muhsen, K.; Cohen, D. Helicobacter pylori Infection and Iron Stores: A Systematic Review and Meta-analysis. Helicobacter 2008, 13, 323–340. [Google Scholar] [CrossRef]
- Hacihanefioglu, A.; Edebali, F.; Celebi, A.; Karakaya, T.; Senturk, O.; Hulagu, S. Improvement of complete blood count in patients with iron deficiency anemia and Helicobacter pylori infection after the eradication of Helicobacter pylori. Hepatogastroenterology 2004, 51, 313–315. [Google Scholar] [PubMed]
- Fiorini, G.; Bland, J.M.; Hughes, E.; Castelli, V.; Vaira, D. A Systematic Review on Drugs Absorption Modifications after Eradication in Helicobacter pylori Positive Patients undergoing Replacement Therapy. J. Gastrointest. Liver Dis. 2015, 24, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, J.L. Iron biology in immune function, muscle metabolism and neuronal functioning. J. Nutr. 2001, 131, 568S–580S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| H. pylori | p | |||
|---|---|---|---|---|
| Negative (185) Mean ± sd, n (%) | Positive (263) Mean ± sd, n (%) | |||
| Age (years) | 51.30 ± 14.10 | 47.87 ± 13.98 | a 0.011 * | |
| Gender | Male | 55 (29.7) | 75 (28.5) | c 0.781 |
| Female | 130 (70.3) | 188 (71.5) | ||
| HGB (g/dL) | 12.66 ± 1.56 | 12.59 ± 1.67 | b 0.501 | |
| MCV (fL) | 87.57 ± 6.85 | 86.55 ± 7.57 | b 0.185 | |
| Leukocyte (µL) | 682.70 ± 1607.57 | 6944.12 ± 1973.45 | b 0.647 | |
| Neutrophil (µL) | 3781.03 ± 1273.28 | 3995.82 ± 1555.09 | b 0.278 | |
| Lymphocyte (µL) | 2278.65 ± 580.43 | 2300.87 ± 1013.54 | b 0.373 | |
| NLR (%) | 1.74 ± 0.65 | 1.92 ± 1.00 | b 0.338 | |
| PLR (%) | 118.91 ± 38.66 | 125.59 ± 47.42 | b 0.237 | |
| Platelet (µL) | 258,718.92 ± 66,735.34 | 264,551.33 ± 75,162.24 | b 0.502 | |
| Iron (µg/dL) | 67.28 ± 39.82 | 56.45 ± 33.64 | b 0.029 * | |
| TIBC (µg/dL) | 356.01 ± 60.33 | 363.94 ± 60.20 | b 0.268 | |
| Ferritin (ng/mL) | 36.04 ± 42.36 | 30.11 ± 52.80 | b 0.003 ** | |
| B12 (pg/mL) | 268.77 ± 158.22 | 278.53 ± 186.21 | b 0.859 | |
| Folic acid (ng/mL) | 8.72 ± 4.15 | 7.27 ± 2.77 | b 0.081 | |
| CRP (mg/L) | 6.04 ± 6.22 | 5.28 ± 4.48 | b 0.530 | |
| Intestinal metaplasia | 26 (14.1) | 48 (18.3) | c 0.239 | |
| Atrophy | 6 (3.2) | 18 (6.8) | c 0.096 | |
| Gastritis | 156 (84.3) | 219 (83.3) | c 0.766 | |
| Gastric ulcer | 31 (16.8) | 45 (17.1) | c 0.933 | |
| Duodenal ulcer | 14 (7.6) | 27 (10.3) | c 0.329 | |
| Esophagitis | 49 (26.5) | 77 (29.3) | c 0.518 | |
| N | NLR | PLR | |||
|---|---|---|---|---|---|
| R | p | R | p | ||
| Age (years) | 263 | 0.020 | 0.743 | 0.054 | 0.386 |
| HGB | 263 | −0.133 | 0.031 * | −0.310 | 0.001 ** |
| MCV | 263 | −0.084 | 0.173 | −0.187 | 0.002 ** |
| Leukocyte (µL) | 263 | 0.302 | 0.001 ** | −0.144 | 0.020 * |
| Neutrophil (µL) | 263 | 0.644 | 0.001 ** | 0.064 | 0.301 |
| Lymphocyte (µL) | 263 | −0.596 | 0.001 ** | −0.622 | 0.001 ** |
| Platelet (µL) | 263 | 0.032 | 0.606 | 0.502 | 0.001 ** |
| Iron (µg/dL) | 131 | −0.270 | 0.002 ** | −0.335 | 0.001 ** |
| TIBC (µg/dL) | 129 | 0.016 | 0.853 | 0.072 | 0.416 |
| Ferritin (ng/mL) | 175 | −0.162 | 0.032 * | −0.290 | 0.001 ** |
| B12 (pg/mL) | 177 | −0.035 | 0.644 | −0.013 | 0.861 |
| Folic acid (ng/mL) | 81 | −0.078 | 0.490 | 0.066 | 0.561 |
| CRP (mg/L) | 52 | 0.006 | 0.967 | −0.085 | 0.548 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyuk, B.; Saydan, D.; Mavis, O.; Erman, H. Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients. Gastroenterol. Insights 2020, 11, 2-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11010002
Boyuk B, Saydan D, Mavis O, Erman H. Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients. Gastroenterology Insights. 2020; 11(1):2-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11010002
Chicago/Turabian StyleBoyuk, Banu, Dogukan Saydan, Osman Mavis, and Hande Erman. 2020. "Evaluation of Helicobacter pylori Infection, Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Dyspeptic Patients" Gastroenterology Insights 11, no. 1: 2-9. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11010002