Diagnosis and Treatment of Acute Pancreatitis Due to Hypertriglyceridemia in Italy: A Survey among Physicians of the Italian Association for the Study of the Pancreas: A Brief Report


Abstract
:1. Introduction
2. Methods
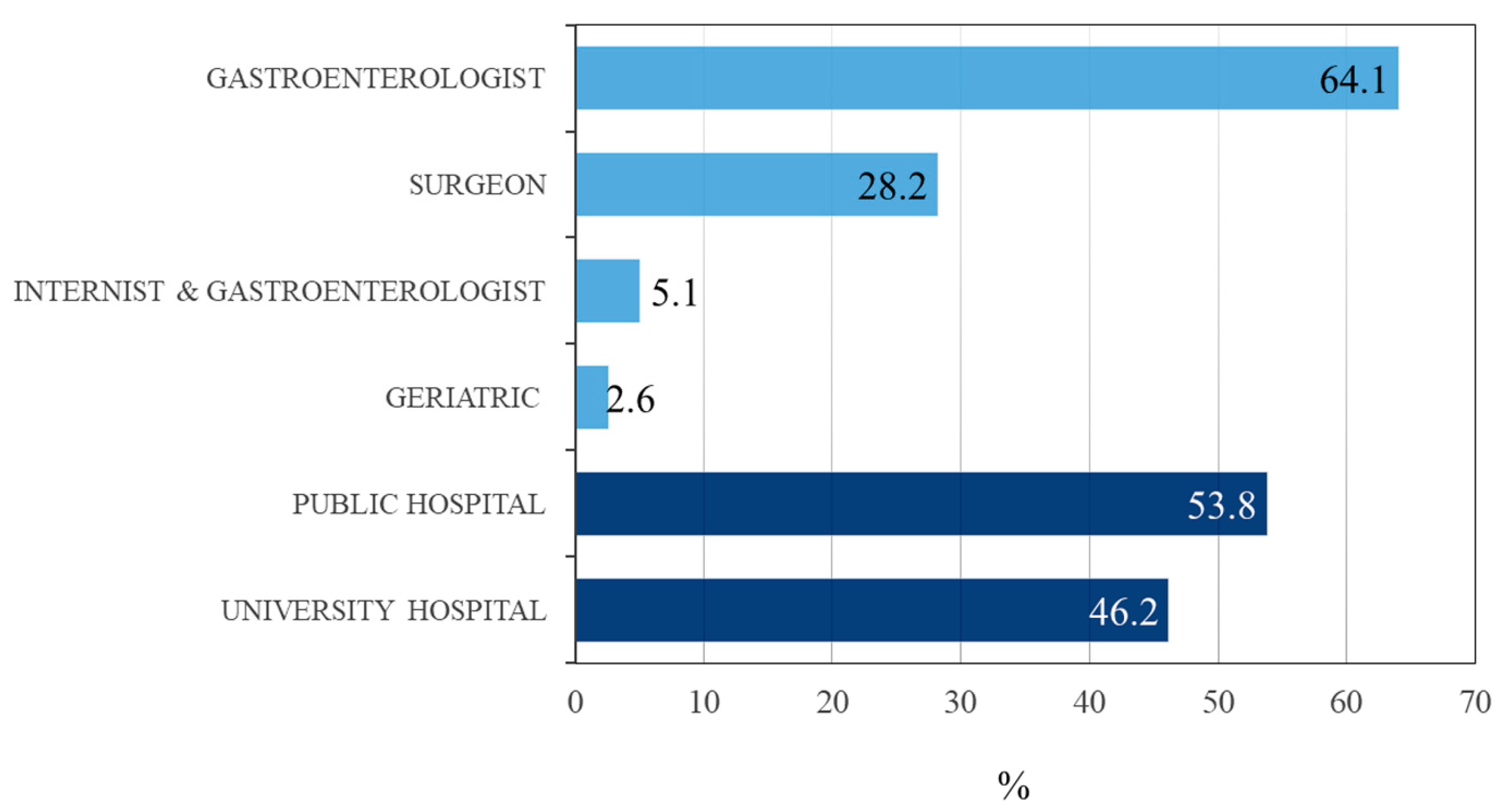
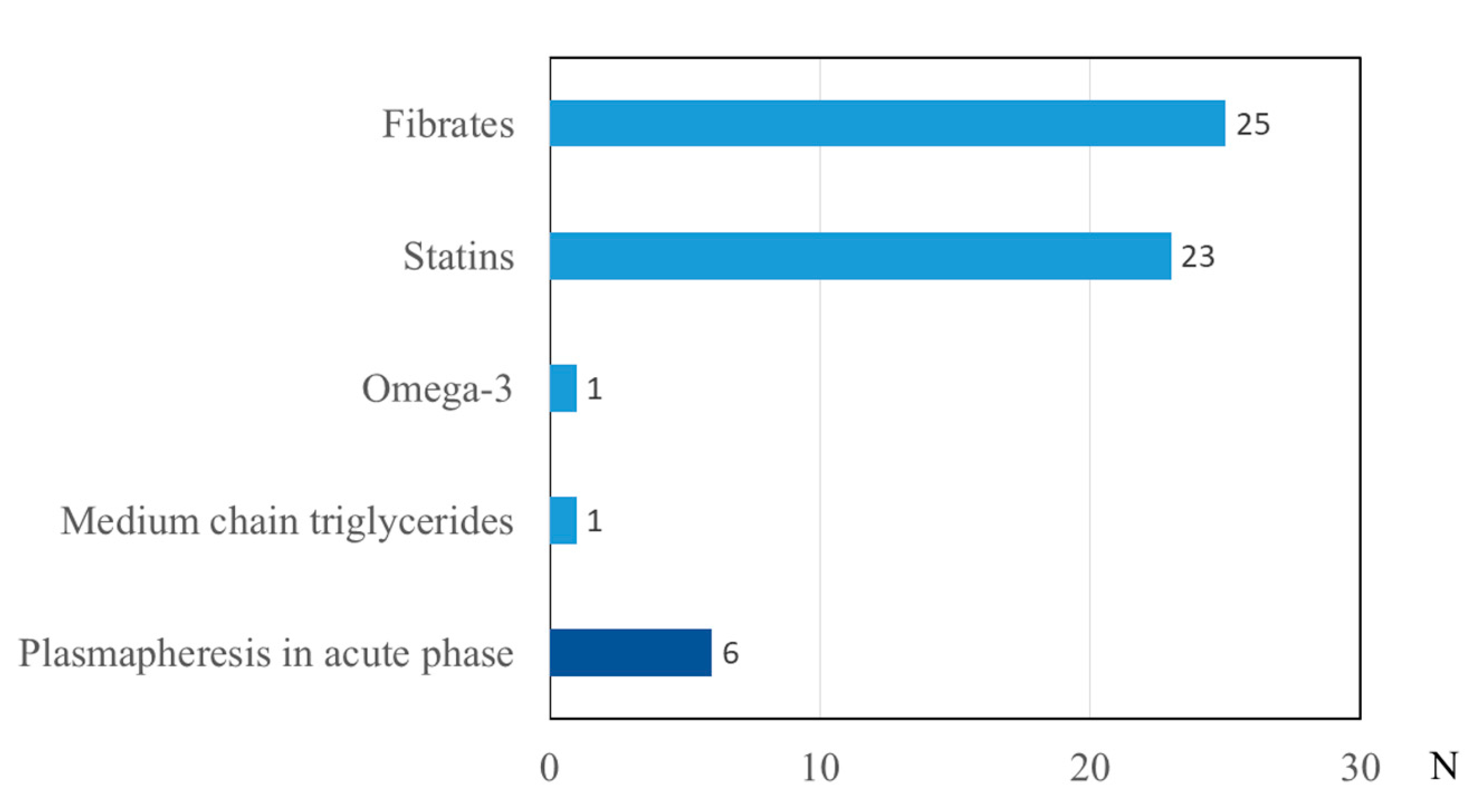
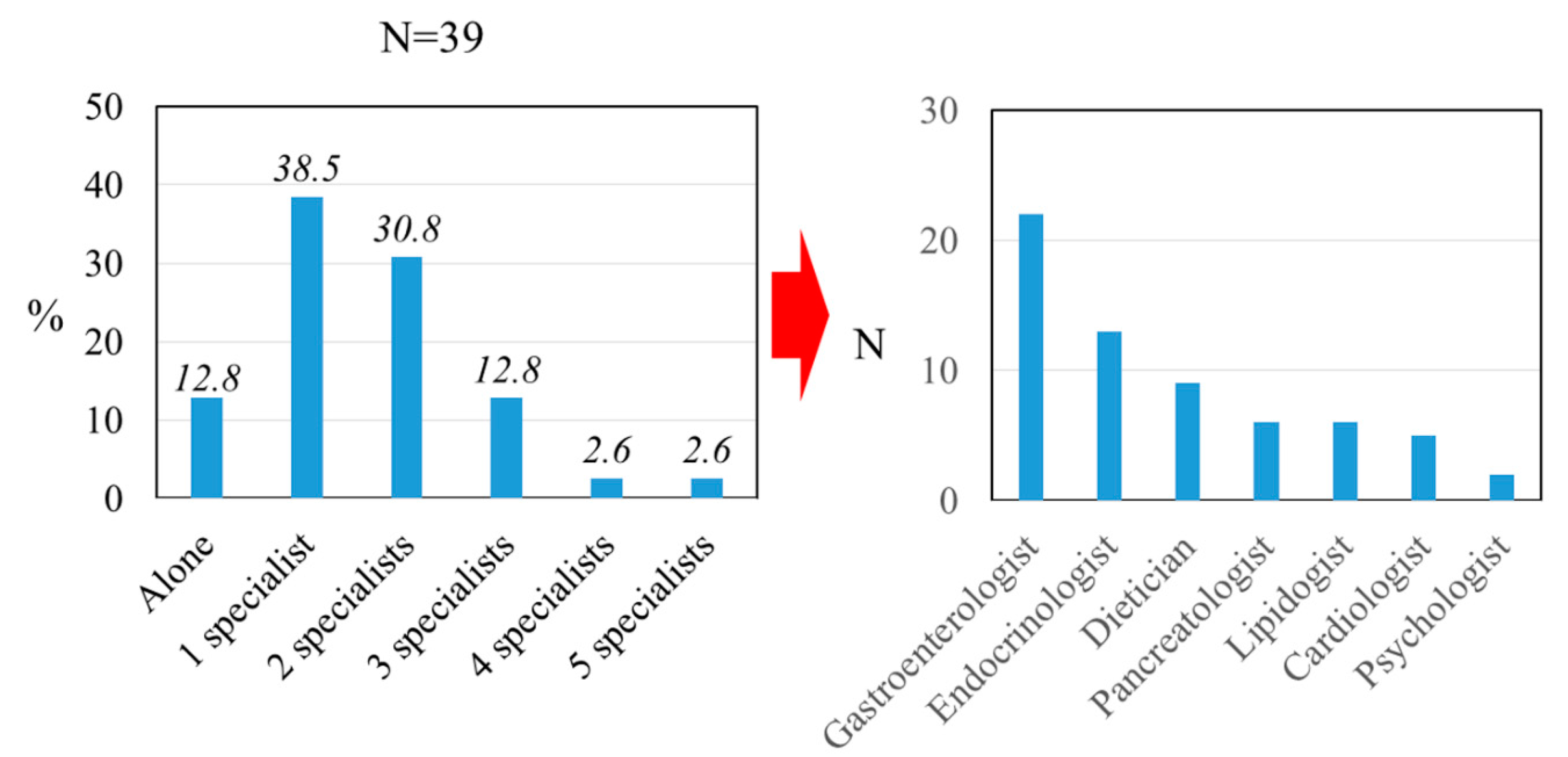
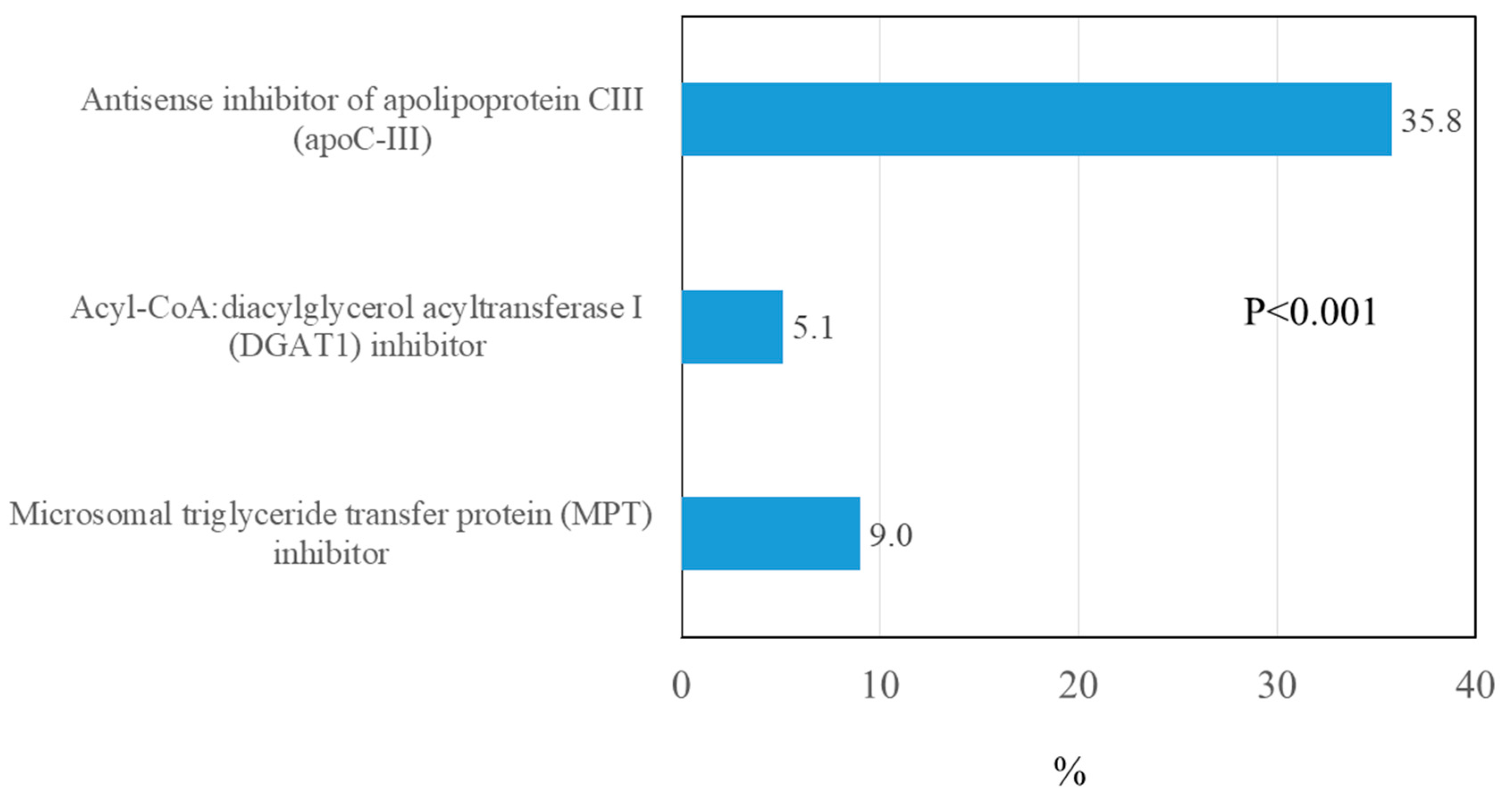
3. Results
4. Discussion
Funding
Acknowledgments
Conflicts of Interest
References
- Pezzilli, R.; Uomo, G.; Zerbi, A.; Gabbrielli, A.; Frulloni, L.; De Rai, P.; Delle Fave, G.; Di Carlo, V. Diagnosis and treatment of acute pancreatitis: The position statement of the Italian Association for the study of the pancreas. Dig. Liver Dis. 2008, 40, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kang, H.; Kim, E.J.; Cho, J.H. Clinical features and outcomes of hypertriglyceridemia-induced acute pancreatitis: Propensity score matching analysis from a prospective acute pancreatitis registry. Pancreatology 2020, 20, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Pothoulakis, I.; Paragomi, P.; Archibugi, L.; Tuft, M.; Talukdar, R.; Kochhar, R.; Goenka, M.K.; Gulla, A.; Singh, V.K.; Gonzalez, J.A.; et al. Clinical features of hypertriglyceridemia-induced acute pancreatitis in an international, multicenter, prospective cohort (APPRENTICE consortium). Pancreatology 2020, 20, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Gullo, L.; Migliori, M.; Pezzilli, R.; Oláh, A.; Farkas, G.; Levy, P.; Arvanitakis, C.; Lankisch, P.; Beger, H. An update on recurrent acute pancreatitis: Data from five European countries. Am. J. Gastroenterol. 2002, 97, 1959–1962. [Google Scholar] [CrossRef]
- Yadav, D.; Lowenfels, A.B. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013, 144, 1252–1261. [Google Scholar] [CrossRef] [Green Version]
- Scherer, J.; Singh, V.; Pitchumoni, C.; Yadav, D. Issues in hypertriglyceridemic pancreatitis-an update. J. Clin. Gastroenterol. 2014, 48, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Yadav, D.; Pitchumoni, C. Issues in hyperlipidemic pancreatitis. J. Clin. Gastroenterol. 2003, 36, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Berglund, L.; Brunzell, J.D.; Goldberg, A.C.; Goldberg, I.J.; Sacks, F.; Murad, M.H.; Stalenhoef, A.F. Evaluation and treatment of hypertriglyceridemia: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2012, 97, 2969–2989. [Google Scholar] [CrossRef] [Green Version]
- Párniczky, A.; Kui, B.; Szentesi, A.; Balázs, A.; Szűcs, Á.; Mosztbacher, D.; Czimmer, J.; Sarlós, P.; Bajor, J.; Gódi, S.; et al. Prospective, multicentre, nationwide clinical data from 600 cases of acute pancreatitis. PLoS ONE 2016, 11, e0165309. [Google Scholar]
- Zhu, Y.; Pan, X.; Zeng, H.; He, W.; Xia, L.; Liu, P.; Zhu, Y.; Chen, Y.; Lv, N. A study on the etiology, severity, and mortality of 3260 patients with acute pancreatitis according to the revised Atlanta classification in Jiangxi, China over an 8-year period. Pancreas 2017, 46, 504–509. [Google Scholar] [CrossRef]
- Mosztbacher, D.; Hanák, L.; Farkas, N.; Szentesi, A.; Mikó, A.; Bajor, J.; Sarlós, P.; Czimmer, J.; Vincze, Á.; Hegyi, P.J.; et al. Hypertriglyceridemia-induced acute pancreatitis: A prospective, multicenter, international cohort analysis of 716 acute pancreatitis cases. Pancreatology 2020, 20, 608–616. [Google Scholar] [CrossRef]
- Khatua, B.; El-Kurdi, B.; Singh, V.P. Obesity and pancreatitis. Curr. Opin. Gastroenterol. 2017, 33, 374–382. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhou, Z.; Li, H.; Li, J.; Li, A.; Ma, B.; Zhang, T.; Liao, Q.; Ye, Y.; Zhang, Z.; et al. A multicenter study on etiology of acute pancreatitis in Beijing during 5 years. Pancreas 2015, 44, 409–414. [Google Scholar] [CrossRef]
- Zhang, R.; Deng, L.; Jin, T.; Zhu, P.; Shi, N.; Jiang, K.; Li, L.; Yang, X.; Guo, J.; Yang, X.; et al. Hypertriglyceridaemia-associated acute pancreatitis: Diagnosis and impact on severity. HPB 2019, 21, 1240–1249. [Google Scholar] [CrossRef] [Green Version]
- Kiss, L.; Fűr, G.; Mátrai, P.; Hegyi, P.; Ivány, E.; Cazacu, I.M.; Szabó, I.; Habon, T.; Alizadeh, H.; Gyöngyi, Z.; et al. The effect of serum triglyceride concentration on the outcome of acute pancreatitis: Systematic review and meta-analysis. Sci. Rep. 2018, 8, 14096. [Google Scholar] [CrossRef] [PubMed]
- Czakó, L.; Szabolcs, A.; Vajda, A.; Csáti, S.; Venglovecz, V.; Rakonczay, Z., Jr.; Hegyi, P.; Tiszlavicz, L.; Csont, T.; Pósa, A.; et al. Hyperlipidemia induced by a cholesterol-rich diet aggravates necrotizing pancreatitis in rats. Eur. J. Pharmacol. 2007, 572, 74–81. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, G.; Qiu, Z.; He, X.; Liu, C. Elevated serum triglycerides in the prognostic assessment of acute pancreatitis. J. Clin. Gastroenterol. 2017, 51, 586–593. [Google Scholar] [CrossRef]
- Yang, N.; Li, B.; Pan, Y.; Tu, J.; Liu, G.; Lu, G.; Li, W. Hypertriglyceridaemia delays pancreatic regeneration after acute pancreatitis in mice and patients. Gut 2019, 68, 378–380. [Google Scholar] [CrossRef] [Green Version]
- IAP, W.G.; Guidelines, A.A.P. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar]
- Isaji, S.; Takada, T.; Mayumi, T.; Yoshida, M.; Wada, K.; Yokoe, M.; Itoi, T.; Gabata, T. Revised Japanese guidelines for the management of acute pancreatitis 2015: Revised concepts and updated points. J. Hepato-Biliary-Pancreat. Sci. 2015, 22, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Witztum, J.L.; Gaudet, D.; Freedman, S.D.; Alexander, V.J.; Digenio, A.; Williams, K.R.; Yang, Q.; Hughes, S.G.; Geary, R.S.; Arca, M.; et al. Volanesorsen and triglyceride levels in familial chylomicronemia syndrome. N. Engl. J. Med. 2019, 381, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Thandra, K.C.; Gaduputi, V. Hypertriglyceridemia-induced pancreatitis: Updated review of current treatment and preventive strategies. Clin. J. Gastroenterol. 2018, 11, 441–448. [Google Scholar] [CrossRef]
- Matta, B.; Gougol, A.; Gao, X.; Reddy, N.; Talukdar, R.; Kochhar, R.; Goenka, M.K.; Gulla, A.; Gonzalez, J.A.; Singh, V.K.; et al. Worldwide Variations in Demographics, Management, and Outcomes of Acute Pancreatitis. Clin. Gastroenterol. Hepatol. 2020, 18, 1567–1575. [Google Scholar] [CrossRef]
- Stevens, C.; Linder, B.; Soo, C. What do gastroenterologists know about hereditary angioedema? Results of a 2012 Digestive Disease Week (DDW) Survey. Am. J. Gastroenterol. 2012, 107, S127. [Google Scholar] [CrossRef]
- Pezzilli, R.; Uomo, G.; Gabbrielli, A.; Zerbi, A.; Frulloni, L.; De Rai, P.; Castoldi, L.; Cavallini, G.; Di Carlo, V.; ProInf-AISP Study Group. A prospective multicentre survey on the treatment of acute pancreatitis in Italy. Dig. Liver Dis. 2007, 39, 838–846. [Google Scholar] [CrossRef]
- Falko, J.M. Familial chylomicronemia syndrome: A clinical guide for endocrinologists. Endocr. Pract. 2018, 24, 756–763. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Content | Number of Questions |
|---|---|---|
| First section | Epidemiological characteristics of the participants | 5 |
| Second section | How the participants made the diagnosis of the disease | 4 |
| Third section | How the participants treat the hypertriglyceridemia after an attack of acute pancreatitis | 2 with multiple choice |
| Fourth section | If the participants know of the new drugs developed for the treatment of hypertriglyceridemia | 1 with multiple choice |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pezzilli, R. Diagnosis and Treatment of Acute Pancreatitis Due to Hypertriglyceridemia in Italy: A Survey among Physicians of the Italian Association for the Study of the Pancreas: A Brief Report. Gastroenterol. Insights 2020, 11, 20-26. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11020005
Pezzilli R. Diagnosis and Treatment of Acute Pancreatitis Due to Hypertriglyceridemia in Italy: A Survey among Physicians of the Italian Association for the Study of the Pancreas: A Brief Report. Gastroenterology Insights. 2020; 11(2):20-26. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11020005
Chicago/Turabian StylePezzilli, Raffaele. 2020. "Diagnosis and Treatment of Acute Pancreatitis Due to Hypertriglyceridemia in Italy: A Survey among Physicians of the Italian Association for the Study of the Pancreas: A Brief Report" Gastroenterology Insights 11, no. 2: 20-26. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent11020005