Infective Endocarditis Caused by Pseudomonas stutzeri: A Case Report and Literature Review

 ,
,
Abstract
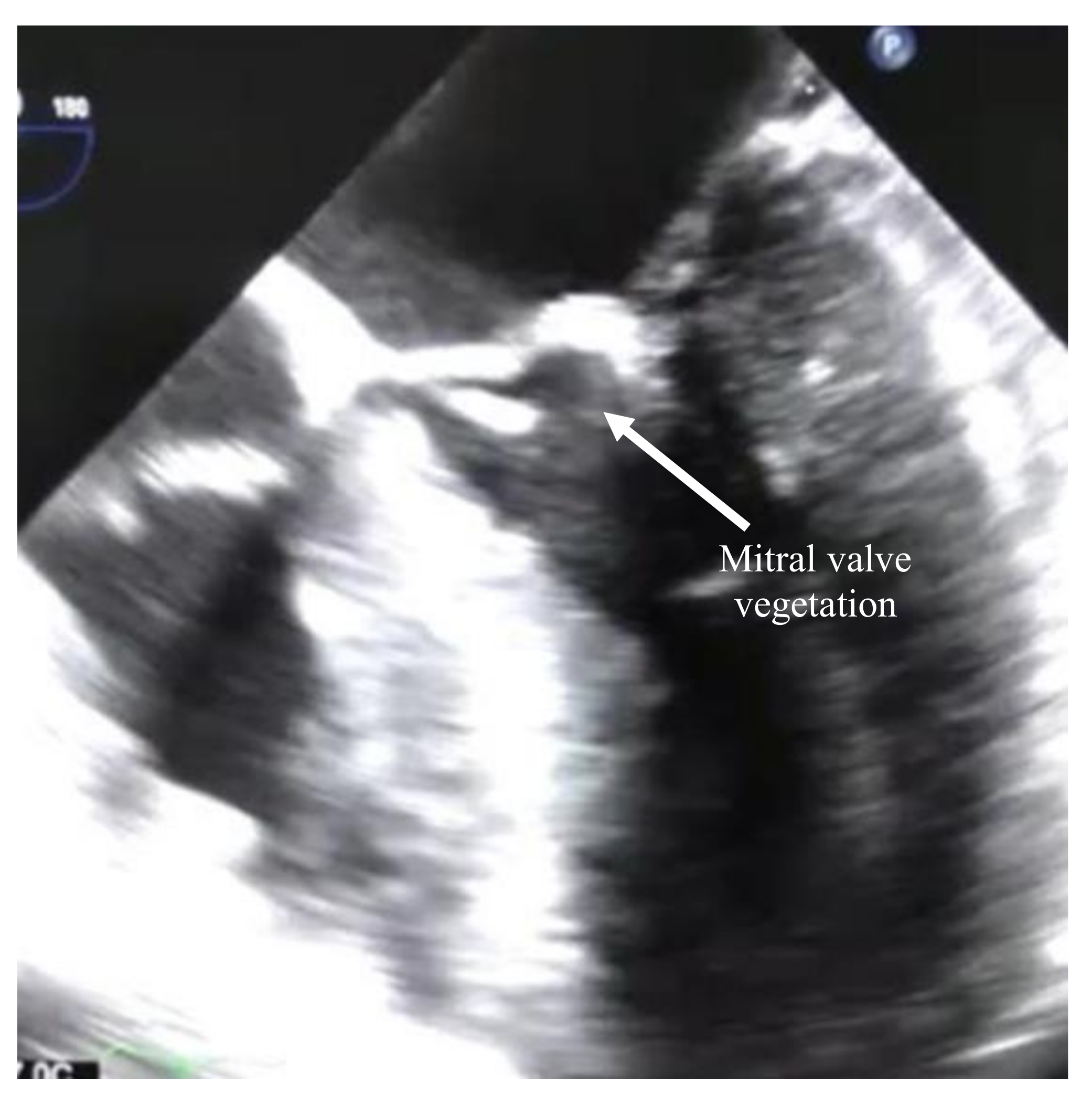
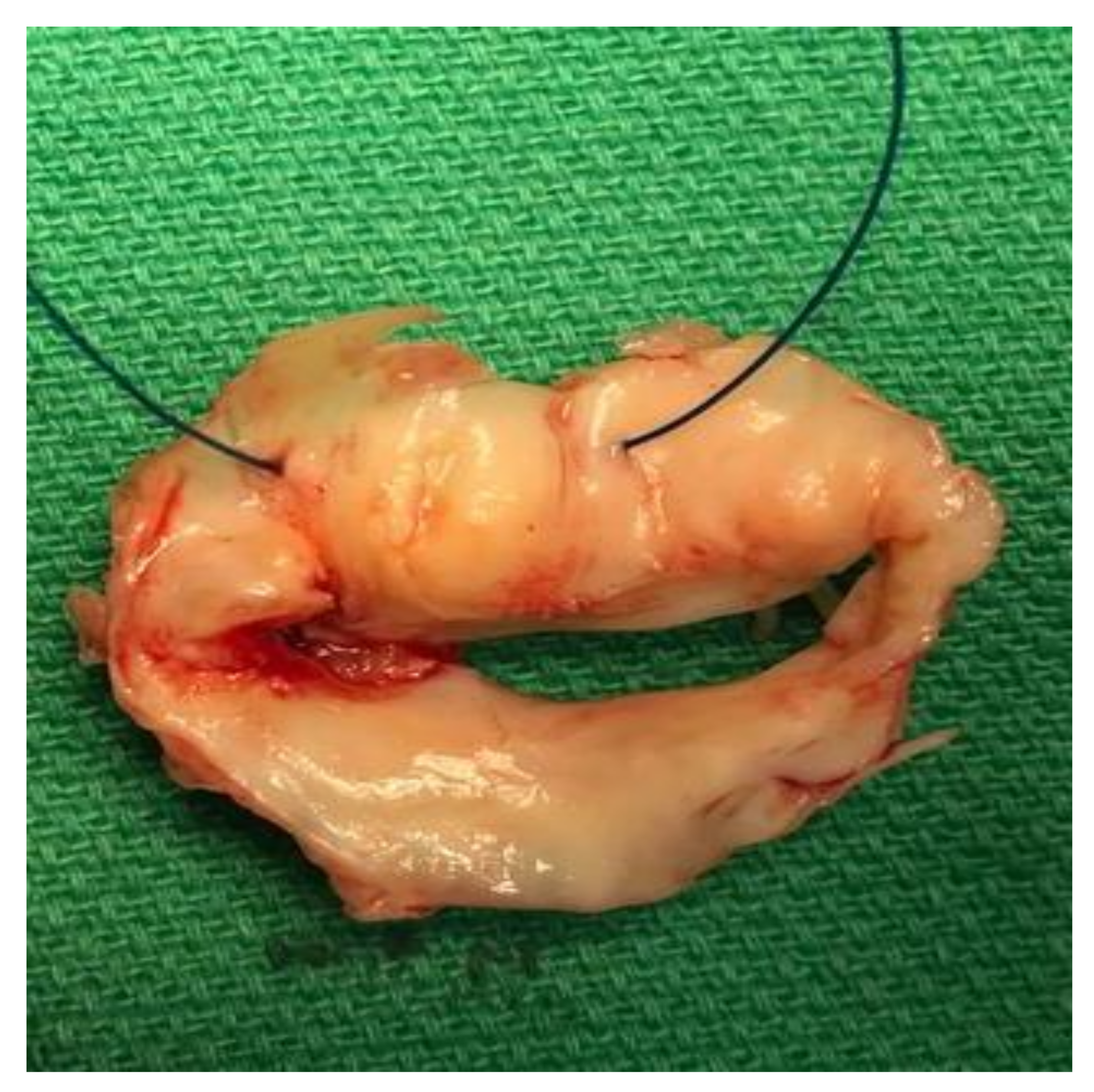
:1. Case Report
2. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lalucat, J.; Bennasar, A.; Bosch, R.; García-Valdés, E.; Palleroni, N.J. Biology of Pseudomonas stutzeri. Microbiol. Mol. Biol. Rev. 2006, 70, 510–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilardi, G.L. Infrequently Encountered Pseudomonas Species Causing Infection in Humans. Ann. Intern. Med. 1972, 77, 211. [Google Scholar] [CrossRef] [PubMed]
- Shalabi, A.; Ehrlich, T.; Schäfers, H.-J.; Becker, S.L. Infective endocarditis caused by Pseudomonas stutzeri in a patient with Marfan syndrome: Case report and brief literature review. IDCases 2017, 10, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Chen, C.-M.; Wang, J.-H.; Ho, M.-W. Pseudomonas stutzeri necrotizing pneumonia in pre-existing pulmonary tuberculosis. Intern. Med. 2014, 53, 2543–2546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosioni, J.; The Hospital Clinic Infective Endocarditis Investigators; Hernandez-Meneses, M.; Téllez, A.; Pericàs, J.; Falces, C.; Tolosana, J.M.; Vidal, B.; Almela, M.; Quintana, E.; et al. The Changing Epidemiology of Infective Endocarditis in the Twenty-First Century. Curr. Infect. Dis. Rep. 2017, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, I.; Leibovici, L.; Mor, F.; Block, C.; Wysenbeek, A.J. Pseudomonas Stutzeri Causing Late Prosthetic Valve Endocarditis. J. R. Soc. Med. 1987, 80, 457–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López, A.; Baraia-Etxaburu, J.; Ezpeleta, C.; Teira, R.; Ayarza, R.; Cisterna, R.; Santamaría, J.M. Multimicrobial endocarditis caused by Streptococcus salivarius and Pseudomonas stutzeri: Good course after early surgery. An. Med. Interna 2002, 19. [Google Scholar]
- Grimaldi, D.; Podglajen, I.; Aubert, A.; Buu-Hoï, A.; Diebold, B.; Mainardi, J.-L. Case of Indolent Endocarditis Due to Pseudomonas stutzeri with Genetic Evidence of Relapse after 4 Years. J. Clin. Microbiol. 2009, 47, 503–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halabi, Z.; Mocadie, M.; El Zein, S.; Kanj, S. Pseudomonas stutzeri prosthetic valve endocarditis: A case report and review of the literature. J. Infect. Public Heal. 2019, 12, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Raphael, C.E.; Heit, J.A.; Reeder, G.S.; Bois, M.C.; Maleszewski, J.J.; Tilbury, R.T. Coronary Embolus: An Underappreciated Cause of Acute Coronary Syndromes. JACC Cardiovasc Interv. 2018, 11, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Van Niel, C.B.; Allen, M.B. A note on Pseudomonas stutzeri. J. Bacteriol. 1952, 64, 413–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, P.; Bouza, E.; Marín, M.; Alcalá, L.; Créixems, M.R.; Valerio, M.; Pinto, A.; on behalf of the Group for the Management of Infective Endocarditis of the Gregorio Maranon Hospital. Heart Valves Should Not Be Routinely Cultured. J. Clin. Microbiol. 2008, 46, 2897–2901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, S.; Watkin, R.; Lambert, P.; Bonser, R.; Littler, W.; Elliott, T. Evaluation of PCR in the molecular diagnosis of endocarditis. J. Infect. 2004, 48, 269–275. [Google Scholar] [CrossRef]
- Alqanatish, J.T.; Alfadhel, A.; Albelali, A.; Alqahtani, D. Acute rheumatic fever diagnosis and management: Review of the global implications of the new revised diagnostic criteria with a focus on Saudi Arabia. J. Saudi Hear. Assoc. 2019, 31, 273–281. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cases | Country | Year | Valve/Type | Antibiotics and Duration | Surgery | Outcome | Time after Cardiac Surgery |
|---|---|---|---|---|---|---|---|
| Rosenberg et al. [6] | Israel | 1987 | Mitral/prosthetic | Tobramycin and mezlocillin for 28 days, then mezlocillin for 14 days | Not done | Cured | 2 years |
| Lopez et al. [7] | Spain | 2002 | Aortic valve/native | aztreonam for 6 weeks | Aortic replacement | Cured | Not applicable |
| Grimaldi et al. [8] | France | 2008 | Aortic/Prosthetic | 1st cefotaxime 1 month then ceftriaxone 1 month 2nd cefotaxime 14 days, ciprofloxacin and doxycycline for 16 months | Not done | Cured | 6 and 10 years |
| Shalabi et al. [3] | Lebanon | 2017 | Aortic and mitral/prosthetic | Ceftazidime 8 weeks | Aortic replacement | Cured | 3 year |
| Halabi et al. [9] | Lebanon | 2018 | Aortic/Prosthetic | Ceftazidime for a couple of days | Aortic and tricuspid valve replacement | Deceased | 26 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alwazzeh, M.J.; Alkuwaiti, F.A.; Alqasim, M.; Alwarthan, S.; El-ghoneimy, Y. Infective Endocarditis Caused by Pseudomonas stutzeri: A Case Report and Literature Review. Infect. Dis. Rep. 2020, 12, 105-109. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030020
Alwazzeh MJ, Alkuwaiti FA, Alqasim M, Alwarthan S, El-ghoneimy Y. Infective Endocarditis Caused by Pseudomonas stutzeri: A Case Report and Literature Review. Infectious Disease Reports. 2020; 12(3):105-109. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030020
Chicago/Turabian StyleAlwazzeh, Marwan J., Feras A. Alkuwaiti, Moammer Alqasim, Sarah Alwarthan, and Yasser El-ghoneimy. 2020. "Infective Endocarditis Caused by Pseudomonas stutzeri: A Case Report and Literature Review" Infectious Disease Reports 12, no. 3: 105-109. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030020