
Hemophagocytic Lymphohistiocytosis (HLH) in Patients with Tick-Borne Illness: A Scoping Review of 98 Cases
 , , , , , and
, , , , , and
Abstract
:1. Introduction
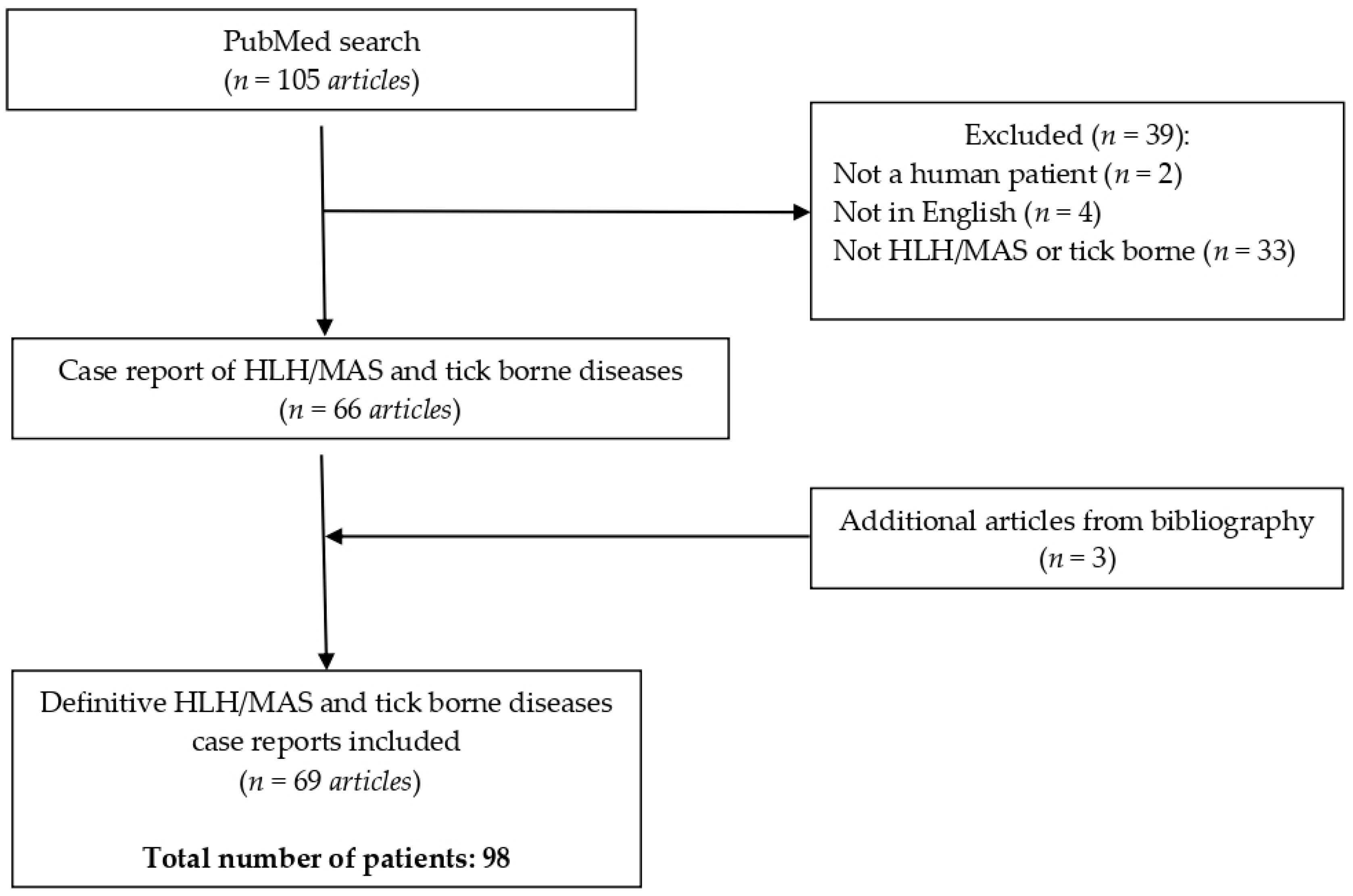
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Clinical Presentation
3.3. Treatment and Outcome
4. Discussion
4.1. Epidemiology
4.2. Tick-Borne Pathogens Associated with Secondary HLH
4.3. Clinical Presentation
4.4. Diagnosis
4.5. Treatment
4.6. Outcome
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponnatt, T.S.; Lilley, C.M.; Mirza, K.M. Hemophagocytic Lymphohistiocytosis. Arch. Pathol. Lab. Med. 2022, 146, 507–519. [Google Scholar] [CrossRef]
- Henter, J.I.; Horne, A.C.; Aricó, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef]
- Henter, J.-I.; Aricò, M.; Maarten Egeler, R.; Favara, B.E.; Filipovich, A.H.; Gadner, H.; Imashuku, S.; Janka-Schaub, G.; Komp, D.; Ladisch, S.; et al. HLH-94: A Treatment Protocol for Hemophagocytic Lymphohistiocytosis. Med. Pediatr. Oncol. 1997, 28, 342–347. [Google Scholar] [CrossRef]
- Rosée, P.L.; Horne, A.C.; Hines, M.; Greenwood, T.V.B.; Machowicz, R.; Berliner, N.; Birndt, S.; Gil-Herrera, J.; Girschikofsky, M.; Jordan, M.B.; et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood 2019, 133, 2465–2477. [Google Scholar] [CrossRef]
- Schram, A.M.; Campigotto, F.; Mullally, A.; Fogerty, A.; Massarotti, E.; Neuberg, D.; Berliner, N. Marked hyperferritinemia does not predict for HLH in the adult population. Blood 2015, 125, 1548–1552. [Google Scholar] [CrossRef] [PubMed]
- Zoref-Lorenz, A.; Murakami, J.; Hofstetter, L.; Iyer, S.; Alotaibi, A.S.; Mohamed, S.F.; Miller, P.G.; Guber, E.; Weinstein, S.; Yacobovich, J.; et al. An improved index for diagnosis and mortality prediction in malignancy-associated hemophagocytic lymphohistiocytosis. Blood 2022, 139, 1098–1110. [Google Scholar] [CrossRef] [PubMed]
- Griffin, G.; Shenoi, S.; Hughes, G.C. Hemophagocytic lymphohistiocytosis: An update on pathogenesis, diagnosis, and therapy. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101515. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Nicoli, E.R.; Serra-Vinardell, J.; Morimoto, M.; Toro, C.; Malicdan, M.C.V.; Introne, W.J. Chediak-Higashi syndrome: A review of the past, present, and future. Drug Discov. Today Dis. Model. 2020, 31, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Parvaneh, N. Chediak Higashi Syndrome with Hemophagocytic Lymphohistiocytosis. Fetal Pediatr. Pathol. 2023, 42, 259–262. [Google Scholar] [CrossRef]
- Alessandra, T.; Gianluca, M.; Alessandra, E.; Elena, S.; Luisa, C.M.; Tiziana, G. Griscelli syndrome type 2: A well defined diagnosis with an intriguing diagnostic way. Neuroimmunol. Rep. 2022, 2, 100091. [Google Scholar] [CrossRef]
- Minocha, P.; Choudhary, R.; Agrawal, A.; Sitaraman, S. Griscelli syndrome subtype 2 with hemophagocytic lympho-histiocytosis: A case report and review of literature. Intractable Rare Dis. Res. 2017, 6, 76. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.J.; Tattersall, R.S.; Ramanan, A.V. Macrophage activation syndrome in adults: Recent advances in pathophysiology, diagnosis and treatment. Rheumatology 2019, 58, 5–17. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zerón, P.; López-Guillermo, A.; Khamashta, M.A.; Bosch, X. Adult haemophagocytic syndrome. Lancet 2014, 383, 1503–1516. [Google Scholar] [CrossRef]
- Abdelhay, A.; Mahmoud, A.; Mostafa, M.; Jain, T.; Elseidy, S.; Fahmawi, S.; Alkasem, M.; Ammari, O. Delay in treatment of adult hemophagocytic lymphohistiocytosis is associated with worse in-hospital outcomes. Ann. Hematol. 2023, 102, 2989–2996. [Google Scholar] [CrossRef] [PubMed]
- Hosahalli Vasanna, S.; Lim, P.P.C.; Khan, T.S.; Dalal, J. Secondary hemophagocytic lymphohistiocytosis associated with Rocky Mountain spotted fever in a toddler: A case report. EJHaem 2022, 3, 463–466. [Google Scholar] [CrossRef]
- Gopal, G.K.; Anugrah, C.; Boorugu, H. Scrub typhus associated macrophage activation syndrome. Trop. Doct. 2010, 40, 249–250. [Google Scholar] [CrossRef]
- Patel, T.P.; Beck, P.; Chairman, D.; Regunath, H. Ehrlichiosis Presenting as Hemophagocytic Lymphohistiocytosis in an Immunocompetent Adult. IDCases 2020, 20, e00813. [Google Scholar] [CrossRef] [PubMed]
- Leal-López, V.F.; Arias-León, J.J.; Faccini-Martínez, Á.A.; Lugo-Caballero, C.; Quiñones-Vega, C.; Erosa-Gonzalez, J.M.; Dzul-Rosado, K.R. Fatal murine typhus with hemophagocytic lymphohistiocytosis in a child. Rev. Inst. Med. Trop. Sao Paulo 2020, 62, e99. [Google Scholar] [CrossRef]
- Goodman, A.; Bilal, M.; Amarnath, S.; Gentile, T.; Shepherd, Z. The unusual case of babesiosis causing disseminated intravascular coagulation with hemophagocytic lymphohistiocytosis. Clin. Case Rep. 2021, 9, e04744. [Google Scholar] [CrossRef]
- Jacquot, R.; Gerfaud-Valentin, M.; Lega, J.C.; Becker, A.; Jamilloux, Y.; Seve, P. Murine typhus complicated by sHLH mimicking adult-onset Still’s disease. Rev. Med. Interne 2022, 43, 617–621. [Google Scholar] [CrossRef]
- Al Amri, R.; Rea, B. Anaplasmosis with associated haemophagocytic lymphohistiocytosis. Br. J. Haematol. 2021, 194, 657. [Google Scholar] [CrossRef]
- Carlson, A.L.; Pastula, D.M.; Lambert, A.J.; Staples, J.E.; Muehlenbachs, A.; Turabelidze, G.; Eby, C.S.; Keller, J.; Hess, B.; Buller, R.S.; et al. Heartland virus and hemophagocytic lymphohistiocytosis in immunocompromised patient, Missouri, USA. Emerg. Infect. Dis. 2018, 24, 893–897. [Google Scholar] [CrossRef]
- Otrock, Z.K.; Gonzalez, M.D.; Eby, C.S. Ehrlichia-Induced Hemophagocytic Lymphohistiocytosis: A Case Series and Review of Literature. Blood Cells Mol. Dis. 2015, 55, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Tsiodras, S.; Spanakis, N.; Spanakos, G.; Pervanidou, D.; Georgakopoulou, T.; Campos, E.; Petra, T.; Kanellopoulos, P.; Georgiadis, G.; Antalis, E.; et al. Fatal human anaplasmosis associated with macrophage activation syndrome in Greece and the Public Health response. J. Infect. Public Health 2017, 10, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Lin, Y.H.; Shi, Z.Y. A case report of scrub typhus-associated hemophagocytic syndrome and a review of literature. Jpn. J. Infect. Dis. 2014, 67, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Cabler, S.S.; Hogan, P.G.; Fritz, S.A.; Bednarski, J.J.; Hunstad, D.A. Incidence and treatment of hemophagocytic lymphohistiocytosis in hospitalized children with Ehrlichia infection. Pediatr. Blood Cancer 2020, 67, e28436. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Almas, T.; Abdelghffar, M.; Jain, S.; Geetha, H.S.; Shah, V.; Nagarajan, V.R.; Alshareef, N.; Gunasaegaram, V.; Ravintharan, K.; et al. A rare case of delayed anaplasma phagocytophilum-induced pancytopenia: A diagnostic conundrum. Ann. Med. Surg. 2022, 75, 103366. [Google Scholar] [CrossRef] [PubMed]
- Rogers, E.; Moffet, E.W.; Huang, S.; Ouni, A.; Patel, D.; Kay, D.; Ataya, A. A 58-Year-Old Man With Acute Encephalopathy, Fever, and Multi-Organ Dysfunction. Chest 2020, 158, e187–e190. [Google Scholar] [CrossRef]
- Gynthersen, R.M.M.; Stensvold, C.R.; Nielsen, S.L.; Møller, H.J.; Nielsen, H.V.; Lebech, A.M.; Christensen, J.R.; Mens, H.; El Fassi, D. Neoehrlichia mikurensis—An emerging opportunistic tick-borne infection in immunosuppressed patients. J. Intern. Med. 2023, 293, 782–790. [Google Scholar] [CrossRef]
- Sağlam, B.; Albayrak, M.; Acar, A.; Yıldız, A.; Maral, S.; Tığlıoğlu, M.; Battal, İ.; Şahin, E.N.; Kuş, A. Q fever as a rare cause of hemophagocytic lymphohistiocytosis: Case report. Transfus. Apher. Sci. 2020, 59, 102747. [Google Scholar] [CrossRef]
- Loussaief, C.; Toumi, A.; Ben Brahim, H.; Aouam, A.; Kairallah, M.; Chakroun, M. Syndrome d’activation macrophagique: Complication rare de typhus murin. Pathol. Biol. 2014, 62, 55–56. [Google Scholar] [CrossRef]
- Gupta, P.; Hurley, R.W.; Helseth, P.H.; Goodman, J.L.; Hammerschmidt, D.E. Pancytopenia due to hemophagocytic syndrome as the presenting manifestation of babesiosis. Am. J. Hematol. 1995, 50, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Ahlers, C.G.; Matthews, H.; Perez, R.; Naggie, S. Secondary hemophagocytic lymphohistiocytosis due to Heartland virus. BMJ Case Rep. 2022, 15, e253082. [Google Scholar] [CrossRef] [PubMed]
- Go, S.A.; Phuoc, V.H.; Eichenberg, S.E.; Temesgen, Z.; Beckman, T.J. Babesia microti infection and hemophagocytic lymphohistiocytosis in an immunocompetent patient. Int. J. Infect. Dis. 2017, 65, 72–74. [Google Scholar] [CrossRef]
- Cheng, A.; Williams, F.; Fortenberry, J.; Preissig, C.; Salinas, S.; Kamat, P. Use of extracorporeal support in hemophagocytic lymphohistiocytosis secondary to ehrlichiosis. Pediatrics 2016, 138, e20154176. [Google Scholar] [CrossRef] [PubMed]
- Paine, A.; Miya, T.; Webb, B.J. Coxiella burnetii infection with severe hyperferritinemia in an asplenic patient. Open Forum Infect. Dis. 2015, 2, ofv125. [Google Scholar] [CrossRef]
- Hsairi, M.; Ben Ameur, S.; Alibi, S.; Belfitouri, Y.; Maaloul, I.; Znazen, A.; Chabchoub, I.; Hammami, A.; Hachicha, M. Syndrome d’activation macrophagique compliquant une fièvre boutonneuse méditerranéenne: Une observation pédiatrique. Arch. Pediatr. 2016, 23, 1076–1079. [Google Scholar] [CrossRef]
- Camacci, M.L.; Panganiban, R.P.; Pattison, Z.; Haghayeghi, K.; Daly, A.; Ojevwe, C.; Munyon, R.J. Severe Human Granulocytic Anaplasmosis With Significantly Elevated Ferritin Levels in an Immunocompetent Host in Pennsylvania: A Case Report. J. Investig. Med. High Impact Case Rep. 2018, 6, 2324709618758350. [Google Scholar] [CrossRef]
- Cascio, A.; Giordano, S.; Dones, P.; Venezia, S.; Iaria, C.; Ziino, O. Haemophagocytic syndrome and rickettsial diseases. J. Med. Microbiol. 2011, 60, 537–542. [Google Scholar] [CrossRef]
- Otsuki, S.; Iwamoto, S.; Azuma, E.; Nashida, Y.; Akachi, S.; Taniguchi, K.; Higashigawa, M.; Komada, Y. Hemophagocytic lymphohistiocytosis due to rickettsia japonica in a 3-month-old infant. J. Pediatr. Hematol. Oncol. 2015, 37, 627–628. [Google Scholar] [CrossRef]
- Premaratna, R.; Williams, H.S.A.; Chandrasena, T.G.A.N.; Rajapakse, R.P.V.J.; Kularatna, S.A.M.; de Silva, H.J. Unusual pancytopenia secondary to haemophagocytosis syndrome in rickettsioses. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 961–963. [Google Scholar] [CrossRef]
- Sharma, S.; Adhikari, A.; Ghimire, N.; Mainali, G.; Yadav, S.K.; Pudasaini, P.; Neupane, S. Hemophagocytic Lymphohistiocytosis secondary to Rickettsial infection: A case report. Clin. Case Rep. 2022, 10, e6730. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Kannan, S.; Meeks, M.; Sanchez, S.; Girone, K.W.; Broyhill, J.C.; Martines, R.B.; Bernick, J.; Flammia, L.; Murphy, J.; et al. Fatal Case of Heartland Virus Disease Acquired in the Mid-Atlantic Region, United States. Emerg. Infect. Dis. 2023, 29, 992–996. [Google Scholar] [CrossRef]
- Atiq, M.U.; Raza, A.; Ashfaq, A.; Cheema, K.; Khan, Y. Two Infectious Agents Causing Hemophagocytic Lymphohistiocytosis. Cureus 2021, 13, 17947. [Google Scholar] [CrossRef]
- Kumar, N.; Goyal, J.; Goel, A.; Shakoory, B.; Chatham, W. Macrophage activation syndrome secondary to human monocytic ehrlichiosis. Indian J. Hematol. Blood Transfus. 2014, 30, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Hanson, D.; Walter, A.W.; Powell, J. Ehrlichia-induced hemophagocytic lymphohistiocytosis in two children. Pediatr. Blood Cancer 2011, 56, 661–663. [Google Scholar] [CrossRef] [PubMed]
- Hufnagel, M.; Niemeyer, C.; Zimmerhackl, L.B.; Tüchelmann, T.; Sauter, S.; Brandis, M. Hemophagocytosis: A complication of acute Q fever in a child. Clin. Infect. Dis. 1995, 21, 1029–1031. [Google Scholar] [CrossRef]
- Dahm, C.N.; Yang, B.Q.; Clark, D.E.; Armstrong, W.C.; Stevenson, L.W. Human Monocytic Ehrlichiosis Associated With Myocarditis and Hemophagocytic Lymphohistiocytosis. JACC Case Rep. 2020, 2, 420–425. [Google Scholar] [CrossRef]
- Saha, A.; Browning, C.; Dandamudi, R.; Barton, K.; Graepel, K.; Cullity, M.; Abusalah, W.; Christine, D.; Rossi, C.; Drexler, N.; et al. Donor-derived Ehrlichiosis: 2 Clusters Following Solid Organ Transplantation. Clin. Infect. Dis. 2022, 74, 918–923. [Google Scholar] [CrossRef]
- Guccione, C.; Colomba, C.; Rubino, R.; Bonura, C.; Anastasia, A.; Agrenzano, S.; Caputo, V.; Giammanco, G.M.; Cascio, A. A severe case of Israeli spotted fever with pleural effusion in Italy. Infection 2022, 50, 269–272. [Google Scholar] [CrossRef]
- Akel, T.; Mobarakai, N. Hematologic manifestations of babesiosis. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 6. [Google Scholar] [CrossRef]
- Ladha, D.; Khalife, R.; Hummel, B.; Purssell, A. Human granulocytic anaplasmosis complicated by hemophagocytic syndrome and coinfection. Can. Med. Assoc. J. 2022, 194, E1685–E1688. [Google Scholar] [CrossRef]
- Agudelo Higuita, N.I.; Yuen, C. Hemophagocytic Lymphohistiocytosis Secondary to Ehrlichia Chaffeensis in Adults: A Case Series From Oklahoma. Am. J. Med. Sci. 2021, 361, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Scribner, J.; Wu, B.; Lamyaithong, A.; Arcega, V.; Villanueva, D.-D. Anaplasmosis-Induced Hemophagocytic Lymphohistiocytosis: A Case Report and Review of the Literature. Open Forum Infect. Dis. 2023, 10, ofad213. [Google Scholar] [CrossRef] [PubMed]
- Padhi, S.; Varghese, R.G.B.; Ramdas, A.; Phansalkar, M.D.; Sarangi, R.L. Hemophagocytic lymphohistiocytosis: Critical reappraisal of a potentially under-recognized condition. Front. Med. China 2013, 7, 492–498. [Google Scholar] [CrossRef]
- Naqash, A.R.; Yogarajah, M.; Vallangeon, B.D.; Hafiz, M.; Patel, D.; Kolychev, E.; Lebron, D.A.; Liles, D. Hemophagocytic lymphohistiocytosis (HLH) secondary to Ehrlichia chaffeensis with bone marrow involvement. Ann. Hematol. 2017, 96, 1755–1758. [Google Scholar] [CrossRef]
- Kwon, H.J.; Yoo, I.H.; Lee, J.W.; Chung, N.G.; Cho, B.; Kim, H.K.; Kang, J.H. Life-threatening scrub typhus with hemophagocytosis and acute respiratory distress syndrome in an infant. J. Trop. Pediatr. 2013, 59, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Jayakrishnan, M.P.; Veny, J.; Feroze, M. Rickettsial infection with hemophagocytosis. Trop. Doct. 2011, 41, 111–112. [Google Scholar] [CrossRef]
- Mitma, A.A.; Burgess, M.J.; van Rhee, F. Ehrlichia-induced hemophagocytic lymphohistiocytosis after autologous stem cell transplant. Transpl. Infect. Dis. 2021, 23, e13621. [Google Scholar] [CrossRef]
- Rocco, J.M.; Mallarino-Haeger, C.; McCurry, D.; Shah, N. Severe anaplasmosis represents a treatable cause of secondary hemophagocytic lymphohistiocytosis: Two cases and review of literature. Ticks Tick. Borne Dis. 2020, 11, 101468. [Google Scholar] [CrossRef]
- Voisin, O.; Monpierre, L.; Le Lorc’h, E.; Pilmis, B.; Le Monnier, A.; Mourad, J.J.; Senghor, Y.; Mizrahi, A. A typical babesiosis in an immunocompetent patient. Ann. Biol. Clin. 2021, 79, 456–459. [Google Scholar] [CrossRef]
- Yi, J.; Kim, K.H.; Ko, M.K.; Lee, E.Y.; Choi, S.J.; Oh, M.D. Human granulocytic anaplasmosis as a cause of febrile illness in Korea since at least 2006. Am. J. Trop. Med. Hyg. 2017, 96, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.; Kochar, R.; Kemp, S.; Rotaru, D.; Shah, S.V. Ehrlichiosis presenting with toxic shock-like syndrome and secondary hemophagocytic lymphohistiocytosis. J. Ark. Med. Soc. 2013, 109, 280–282. [Google Scholar]
- Kaplan, R.M.; Swat, S.A.; Singer, B.D. Human monocytic ehrlichiosis complicated by hemophagocytic lymphohistiocytosis and multi-organ dysfunction syndrome. Diagn. Microbiol. Infect. Dis. 2016, 86, 327–328. [Google Scholar] [CrossRef]
- Chen, T.C.; Chang, K.; Lu, P.L.; Liu, Y.C.; Chen, Y.H.; Hsieh, H.C.; Yang, W.C.; Lin, W.R.; Tsai, J.J.; Lin, S.F. Acute Q fever with hemophagocytic syndrome: Case report and literature review. Scand. J. Infect. Dis. 2006, 38, 1119–1122. [Google Scholar] [CrossRef]
- Bläckberg, J.; Lazarevic, V.L.; Hunfeld, K.P.; Persson, K.E.M. Low-virulent Babesia venatorum infection masquerading as hemophagocytic syndrome. Ann. Hematol. 2018, 97, 731–733. [Google Scholar] [CrossRef] [PubMed]
- Andrade, M.M.; Gorgulho, A.; Magalhães, R.T.; Valadas, R.; Pereira, L.M.; Freire, S.; Cruz, D. Haemophagocytic Lymphohistiocytosis as a Complication of Israeli Spotted Fever. Eur. J. Case Rep. Intern. Med. 2022, 9, 003073. [Google Scholar] [CrossRef] [PubMed]
- Valsalan, R.; Kosaraju, K.; Sohanlal, T.; Prem Kumar, P.S. Hemophagocytosis in scrub typhus. J. Postgrad. Med. 2010, 56, 301–302. [Google Scholar] [CrossRef]
- Karra, N.; Dolinski, R.; Akria, L.; Yampoulski, Y.; Awad, J. A Case of Hemophagocytic Lymphohistiocytosis Associated With Mediterranean Spotted Fever in a Healthy 29-Year-Old Female. Open Forum Infect. Dis. 2020, 7, ofaa355. [Google Scholar] [CrossRef] [PubMed]
- Burns, S.; Saylors, R.; Mian, A. Hemophagocytic lymphohistiocytosis secondary to ehrlichia chaffeensis infection: A case report. J. Pediatr. Hematol. Oncol. 2010, 32, e142–e143. [Google Scholar] [CrossRef]
- Nakano, A.; Ogawa, H.; Nakanishi, Y.; Fujita, H.; Mahara, F.; Shiogama, K.; Tsutsumi, Y.; Takeichi, T. Hemophagocytic lymphohistiocytosis in a fatal case of severe fever with thrombocytopenia syndrome. Intern. Med. 2017, 56, 1597–1602. [Google Scholar] [CrossRef]
- Dermawan, J.K.; Mukherjee, S. Hemophagocytic lymphohistiocytosis secondary to babesiosis. Blood 2020, 135, 779. [Google Scholar] [CrossRef]
- de Jesus, M.; Lopez, A.; Yabut, J.; Vu, S.; Manne, M.; Ibrahim, L.; Mutneja, R. Anaplasmosis-induced hemophagocytic lymphohistiocytosis. Bayl. Univ. Med. Cent. Proc. 2022, 35, 379–381. [Google Scholar] [CrossRef]
- Hammoud, K.; Fulmer, R.; Hamner, M.; El Atrouni, W. Ehrlichiosis-Associated Hemophagocytic Lymphohistiocytosis: A Case Series and Review of the Literature. Case Rep. Hematol. 2023, 2023, 5521274. [Google Scholar] [CrossRef]
- Statler, V.A.; Marshall, G.S. Hemophagocytic lymphohistiocytosis induced by monocytic ehrlichiosis. J. Pediatr. 2015, 166, 499–499.e1. [Google Scholar] [CrossRef]
- Harris, P.; Dixit, R.; Norton, R. Coxiella burnetii causing haemophagocytic syndrome: A rare complication of an unusual pathogen. Infection 2011, 39, 579–582. [Google Scholar] [CrossRef]
- Kennedy-Snodgrass, C.; Obayomi, M.; Muddasani, R.; Slonim, L.B.; Braunstein, M. Hemophagocytic lymphohistiocytosis secondary to Babesia in an immunocompetent adult. Am. J. Hematol. 2019, 94, 379–383. [Google Scholar] [CrossRef]
- Bolling, T.; Ritter, A.S.; Gupte, A.A. An Unusual Case of Ehrlichiosis Manifesting With Hyponatremia, Acute Encephalopathy, and Hemophagocytic Lymphohistiocytosis. Cureus 2022, 14, e26943. [Google Scholar] [CrossRef] [PubMed]
- Vijayan, V.; Thambundit, A.; Sukumaran, S. Hemophagocytic lymphohistiocytosis secondary to ehrlichiosis in a child. Clin. Pediatr. 2015, 54, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.M.; Brown, M.S.; Rabbat, M.; Slim, J. Hemophagocytic lymphohistiocytosis associated with anaplasmosis. J. Glob. Infect. Dis. 2017, 9, 76–78. [Google Scholar] [CrossRef]
- Singh, N.S.; Pagano, A.L.; Hays, A.J.; Kats, A.; Dahl, S.M.; Warady, B.A.; Beins, N.T.; Yin, D.E. Ehrlichia-induced hemophagocytic lymphohistiocytosis in a pediatric kidney transplant recipient. Pediatr. Transplant. 2022, 26, e14134. [Google Scholar] [CrossRef]
- Chandramohan, D.; Awobajo, M.; Fisher, O.; Dayton, C.L.; Anstead, G.M. Flea-Borne Typhus Causing Hemophagocytic Lymphohistiocytosis: An Autopsy Case. Infect. Dis. Rep. 2023, 15, 132–141. [Google Scholar] [CrossRef]
- Zahra, A.; Marcos, L.A. Hemagophagocytic lymphohistiocytosis associated with recurrent Babesiosis with Lyme disease co-infection in an immunocompromised host on anti-CD20 monoclonal antibody therapy: A case report. IDCases 2022, 29, e01570. [Google Scholar] [CrossRef]
- Ishii, E.; Ohga, S.; Imashuku, S.; Yasukawa, M.; Tsuda, H.; Miura, I.; Yamamoto, K.; Horiuchi, H.; Takada, K.; Ohshima, K.; et al. Nationwide survey of hemophagocytic lymphohistiocytosis in Japan. Int. J. Hematol. 2007, 86, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Niece, J.A.; Rogers, Z.R.; Ahmad, N.; Langevin, A.M.; McClain, K.L. Hemophagocytic lymphohistiocytosis in Texas: Observations on ethnicity and race. Pediatr. Blood Cancer 2010, 54, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Crayne, C.B.; Albeituni, S.; Nichols, K.E.; Cron, R.Q. The Immunology of Macrophage Activation Syndrome. Front. Immunol. 2019, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Cui, T.; Wang, J.; Wang, Z. The Outcome of Induction Therapy for EBV-Related Hemophagocytic Lymphohistiocytosis: A Model for Risk Stratification. Front. Immunol. 2022, 13, 876415. [Google Scholar] [CrossRef] [PubMed]
- Imashuku, S.; Morimoto, A.; Ishii, E. Virus-triggered secondary hemophagocytic lymphohistiocytosis. Acta Paediatr. 2021, 110, 2729–2736. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Jevtic, D.; Veselinovic, M.; Nordstrom, C.W.; Jovanovic, M.; Mogulla, V.; Veselinovic, E.M.; Hudson, A.; Simeunovic, G.; Petcu, E.; et al. Human Granulocytic Anaplasmosis-A Systematic Review of Published Cases. Microorganisms 2022, 10, 1433. [Google Scholar] [CrossRef]
- George, M.R. Hemophagocytic lymphohistiocytosis: Review of etiologies and management. J. Blood Med. 2014, 5, 69. [Google Scholar] [CrossRef]
- Krause, P.J.; Gewurz, B.E.; Hill, D.; Marty, F.M.; Vannier, E.; Foppa, I.M.; Furman, R.R.; Neuhaus, E.; Skowron, G.; Gupta, S.; et al. Persistent and relapsing babesiosis in immunocompromised patients. Clin. Infect. Dis. 2008, 46, 370–376. [Google Scholar] [CrossRef]
- Ismail, N.; Bloch, K.C.; McBride, J.W. Human Ehrlichiosis and Anaplasmosis. Clin. Lab. Med. 2010, 30, 261. [Google Scholar] [CrossRef]
- McMullan, L.K.; Folk, S.M.; Kelly, A.J.; MacNeil, A.; Goldsmith, C.S.; Metcalfe, M.G.; Batten, B.C.; Albariño, C.G.; Zaki, S.R.; Rollin, P.E.; et al. A new phlebovirus associated with severe febrile illness in Missouri. N. Engl. J. Med. 2012, 367, 834–841. [Google Scholar] [CrossRef]
- Pastula, D.M.; Turabelidze, G.; Yates, K.F.; Jones, T.F.; Lambert, A.J.; Panella, A.J.; Kosoy, O.I.; Velez, J.O.; Fisher, M.; Staples, E.; et al. Heartland Virus Disease—United States, 2012–2013. Morb. Mortal. Wkly. Rep. 2014, 63, 270. [Google Scholar]
- Zhang, Z.; Wang, J.; Ji, B.; von Bahr Greenwood, T.; Zhang, Y.; Wang, Y.; Kong, D.; Li, A.; Jiang, Y.; Guo, Y.; et al. Clinical presentation of hemophagocytic lymphohistiocytosis in adults is less typical than in children. Clinics 2016, 71, 205–209. [Google Scholar] [CrossRef]
- Dumic, I.; Madrid, C.; Rueda Prada, L.; Nordstrom, C.W.; Taweesedt, P.T.; Ramanan, P. Splenic Complications of Babesia microti Infection in Humans: A Systematic Review. Can. J. Infect. Dis. Med. Microbiol. 2020, 2020, 6934149. [Google Scholar] [CrossRef]
- Song, Y.; Pei, R.J.; Wang, Y.N.; Zhang, J.; Wang, Z. Central Nervous System Involvement in Hemophagocytic Lymphohistiocytosis in Adults: A Retrospective Analysis of 96 Patients in a Single Center. Chin. Med. J. 2018, 131, 776–783. [Google Scholar] [CrossRef]
- Sekeyová, Z.; Danchenko, M.; Filipčík, P.; Fournier, P.E. Rickettsial infections of the central nervous system. PLoS Negl. Trop. Dis. 2019, 13, e0007469. [Google Scholar] [CrossRef]
- Cosiquien, R.J.S.; Stojiljkovic, N.; Nordstrom, C.W.; Amadi, E.; Lutwick, L.; Dumic, I. Anaplasma phagocytophilum Encephalitis: A Case Report and Literature Review of Neurologic Manifestations of Anaplasmosis. Infect. Dis. Rep. 2023, 15, 354. [Google Scholar] [CrossRef] [PubMed]
- Venigalla, T.; Adekayode, C.; Doreswamy, S.; Al-Sudani, H.; Sekhar, S. Atypical Presentation of Babesiosis With Neurological Manifestations as Well as Hematological Manifestations. Cureus 2022, 14, e26811. [Google Scholar] [CrossRef] [PubMed]
- Kahloun, R.; Gargouri, S.; Abroug, N.; Sellami, D.; Ben Yahia, S.; Feki, J.; Khairallah, M. Visual loss associated with rickettsial disease. Ocul. Immunol. Inflamm. 2014, 22, 373–378. [Google Scholar] [CrossRef]
- Boulahri, T.; Taous, A.; Berri, M.A.; Traibi, I.; Elbenaye, J.; Rouimi, A. Rickettsiosis associated with cerebral infarction: A new case study. Pan Afr. Med. J. 2017, 26, 80. [Google Scholar]
- Kularatne, S.A.M.; Fernando, R.; Selvaratnam, S.; Narampanawa, C.; Weerakoon, K.; Wickramasinghe, S.; Pathirage, M.; Weerasinghe, V.; Bandara, A.; Rajapakse, J. Intra-aural tick bite causing unilateral facial nerve palsy in 29 cases over 16 years in Kandy, Sri Lanka: Is rickettsial aetiology possible? BMC Infect. Dis. 2018, 18, 418. [Google Scholar] [CrossRef]
- Aulagnon, F.; Lapidus, N.; Canet, E.; Galicier, L.; Boutboul, D.; Peraldi, M.N.; Reuter, D.; Bernard, R.; Schlemmer, B.; Azoulay, E.; et al. Acute kidney injury in adults with hemophagocytic lymphohistiocytosis. Am. J. Kidney Dis. 2015, 65, 851–859. [Google Scholar] [CrossRef]
- Kuriakose, K.; Pettit, A.C.; Schmitz, J.; Moncayo, A.; Bloch, K.C. Assessment of Risk Factors and Outcomes of Severe Ehrlichiosis Infection. JAMA Netw. Open 2020, 3, e2025577. [Google Scholar] [CrossRef] [PubMed]
- Bratton, R.L.; Corey, G.R. Tick-Borne Disease. Am. Fam. Physician 2005, 71, 2323–2330. [Google Scholar]
- Pinto, C.J.; Maldar, S.B.; Subramaniam, S.; Fathima, N.; Nayyar, R.; Patel, R.J. Clustered Incidence of Leukocytoclastic Vasculitis and Purpura Fulminans: A Case Series of a Rare Dermatological Manifestation of Rickettsial Disease. Cureus 2022, 14, e27187. [Google Scholar] [CrossRef]
- Pace, E.J.; O’Reilly, M. Tickborne Diseases: Diagnosis and Management. Am. Fam. Physician 2020, 101, 530–540. [Google Scholar]
- Kim, Y.R.; Kim, D.Y. Current status of the diagnosis and treatment of hemophagocytic lymphohistiocytosis in adults. Blood Res. 2021, 56, 17. [Google Scholar] [CrossRef]
- Cetica, V.; Sieni, E.; Pende, D.; Danesino, C.; De Fusco, C.; Locatelli, F.; Micalizzi, C.; Putti, M.C.; Biondi, A.; Fagioli, F.; et al. Genetic predisposition to hemophagocytic lymphohistiocytosis: Report on 500 patients from the Italian registry. J. Allergy Clin. Immunol. 2016, 137, 188–196.e4. [Google Scholar] [CrossRef]
- Jordan, M.B.; Allen, C.E.; Weitzman, S.; Filipovich, A.H.; McClain, K.L. How I treat hemophagocytic lymphohistiocytosis. Blood 2011, 118, 4041–4052. [Google Scholar] [CrossRef]
- Rocco, J.M.; Laidlaw, E.; Galindo, F.; Anderson, M.; Rupert, A.; Higgins, J.; Sortino, O.; Ortega-Villa, A.M.; Sheikh, V.; Roby, G.; et al. Severe Mycobacterial Immune Reconstitution Inflammatory Syndrome (IRIS) in Advanced Human Immunodeficiency Virus (HIV) Has Features of Hemophagocytic Lymphohistiocytosis and Requires Prolonged Immune Suppression. Clin. Infect. Dis. 2023, 76, e561–e570. [Google Scholar] [CrossRef]
- Bergsten, E.; Horne, A.C.; Aricó, M.; Astigarraga, I.; Egeler, R.M.; Filipovich, A.H.; Ishii, E.; Janka, G.; Ladisch, S.; Lehmberg, K.; et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: Long-term results of the cooperative HLH-2004 study. Blood 2017, 130, 2728–2738. [Google Scholar] [CrossRef]
- Zimmer, A.J.; Simonsen, K.A. Babesiosis; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Ehl, S. Etoposide for HLH: The limits of efficacy. Blood 2017, 130, 2692–2693. [Google Scholar] [CrossRef]
- Schram, A.M.; Berliner, N. How I treat hemophagocytic lymphohistiocytosis in the adult patient. Blood 2015, 125, 2908–2914. [Google Scholar] [CrossRef]
- Konkol, S.; Rai, M. Lymphohistiocytosis; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Yoon, J.H.; Park, S.S.; Jeon, Y.W.; Lee, S.E.; Cho, B.S.; Eom, K.S.; Kim, Y.J.; Kim, H.J.; Lee, S.; Min, C.K.; et al. Treatment outcomes and prognostic factors in adult patients with secondary hemophagocytic lymphohistiocytosis not associated with malignancy. Haematologica 2019, 104, 269–276. [Google Scholar] [CrossRef]
- Wang, H.; Xiong, L.; Tang, W.; Zhou, Y.; Li, F. A systematic review of malignancy-associated hemophagocytic lymphohistiocytosis that needs more attentions. Oncotarget 2017, 8, 59977. [Google Scholar] [CrossRef]
- Setiadi, A.; Zoref-Lorenz, A.; Lee, C.Y.; Jordan, M.B.; Chen, L.Y.C. Malignancy-associated haemophagocytic lymphohistiocytosis. Lancet Haematol. 2022, 9, e217–e227. [Google Scholar] [CrossRef]


{kind=link}
| Pathogen | Number of Patients (%) |
|---|---|
| Ehrlichia spp. | 45 (45.9%) |
| Rickettsia spp. | 14 (14.3%) |
| Anaplasma spp. | 12 (12.2%) |
| Babesia spp. | 10 (10.2%) |
| Orientia spp. | 8 (8.2%) |
| Coxiella spp. | 5 (5.1%) |
| Heartland virus | 3 (3.1%) |
| Bunyavirus spp. | 1 (1%) |
| Complications | Number of Patients (%) |
|---|---|
| Acute kidney injury | 35 (35.7%) |
| Shock with multiple organ dysfunction | 22 (22.5%) |
| Encephalopathy/seizure | 20 (20.4%) |
| Respiratory failure | 16 (16.3%) |
| Myocarditis/Pericarditis/Cardiac arrest | 7 (7.1%) |
| Antibiotics (n = 94, 95.9%) | Immunosuppressants (n = 55, 56.1%) * | ||||
|---|---|---|---|---|---|
| Appropriate empiric (n = 61, 62.2%) | Not appropriate empiric/unknown (n = 33, 33.7%) | Steroids (n = 50, 51%) | IVIG (n = 10, 10.2%) | Anakinra (n = 5, 5.1%) | Cyclosporine (n = 3, 3.1%) |
| Publication | Age | Sex | Comorbidities | Pathogen | Immunosuppression | Antibiotics |
|---|---|---|---|---|---|---|
| Dahm CN, et al., 2020 [48] | 68 | M | NA | Ehrlichia spp. | Corticosteroids | Vancomycin and cefepime (admission). Doxycycline (5th hospital day) |
| Saha A, et al., 2022 [49] | 70 | M | ESRD, kidney transplant | Ehrlichia spp. | Corticosteroids and etoposide | Doxycycline and caspofungin (7th day after the initial symptoms) |
| Sharma S, et al., 2022 [42] | 34 | M | NA | Rickettsia typhi | Corticosteroids and etoposide | Doxycycline and Ciprofloxacin (1st hospital day) |
| Mitma AA, et al., 2021 [59] | 72 | M | Multiple myeloma | Ehrlichia spp. | Corticosteroids and tocilizumab | Vancomycin and cefepime (admission). Doxycycline was added afterwards. |
| Carlson AL, et al., 2018 [22] | * | M | DM, COPD, HTN, ischemic CMP, hypothyroidism, RA (prednisone, methotrexate, and adalimumab) | Heartland virus | Corticosteroids and etoposide | Vancomycin, meropenem, ampicillin, acyclovir, and doxycycline |
| Leal-López VF, et al., 2020 [18] | 2 | M | NA | Rickettsia typhi | Corticosteroids | Amoxicillin (symptoms onset). Doxycycline (third week) |
| Cabler SS, et al., 2020 [26] | 7 | F | NA | Ehrlichia spp. | Corticosteroids and etoposide | Doxycycline |
| Yi J, et al., 2017 [62] | 32 | M | NA | Anaplasma phagocytophilum | Corticosteroids, etoposide, and IVIg | / |
| Yi J, et al., 2017 [62] | 53 | M | NA | Anaplasma phagocytophilum | Corticosteroids, etoposide, and IVIg | / |
| Nakano A, et al., 2017 [71] | 86 | F | HTN | Bunyavirus | Corticosteroids | Not specified which, but prescribed on diagnosis |
| Saha A, et al., 2022 [49] | 66 | M | ESRD on HD, DM, kidney transplant | Ehrlichia spp. | Corticosteroids, tocilizumab, and IVIg | / |
| Lin YH, et al., 2014 [25] | 34 | F | Drug abuse, HCV infection | Orientia tsutsugamushi | Corticosteroids | Ceftriaxone and minocycline (1st hospital day). |
| Dahm CN, et al., 2020 [48] | 60 | F | NA | Ehrlichia spp. | / | Piperacillin-tazobactam and levofloxacin (1st hospital day). Doxycyclin (3rd hospital day) |
| Chandramohan D, et al., 2023 [82] | 71 | F | DM, HTN, dyslipidemia | Rickettsia typhi | / | Ceftriaxone |
| Liu S, et al., 2023 [43] | 60 | M | Asplenia, HTN, coronary arthery disease | Heartland virus | / | Doxycycline |
| Tsiodras S, et al., 2017 [24] | 57 | M | Anaplasma phagocytophilum | Meropenem and doxycycline (3rd hospital day) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jevtic, D.; da Silva, M.D.; Haylock, A.B.; Nordstrom, C.W.; Oluic, S.; Pantic, N.; Nikolajevic, M.; Nikolajevic, N.; Kotseva, M.; Dumic, I. Hemophagocytic Lymphohistiocytosis (HLH) in Patients with Tick-Borne Illness: A Scoping Review of 98 Cases. Infect. Dis. Rep. 2024, 16, 154-169. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020012
Jevtic D, da Silva MD, Haylock AB, Nordstrom CW, Oluic S, Pantic N, Nikolajevic M, Nikolajevic N, Kotseva M, Dumic I. Hemophagocytic Lymphohistiocytosis (HLH) in Patients with Tick-Borne Illness: A Scoping Review of 98 Cases. Infectious Disease Reports. 2024; 16(2):154-169. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020012
Chicago/Turabian StyleJevtic, Dorde, Marilia Dagnon da Silva, Alberto Busmail Haylock, Charles W. Nordstrom, Stevan Oluic, Nikola Pantic, Milan Nikolajevic, Nikola Nikolajevic, Magdalena Kotseva, and Igor Dumic. 2024. "Hemophagocytic Lymphohistiocytosis (HLH) in Patients with Tick-Borne Illness: A Scoping Review of 98 Cases" Infectious Disease Reports 16, no. 2: 154-169. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16020012