
Amylase Levels Are Useful for Diagnosing Omphalomesenteric Cysts: A Case Report

 , ,
, ,
Abstract
:1. Introduction
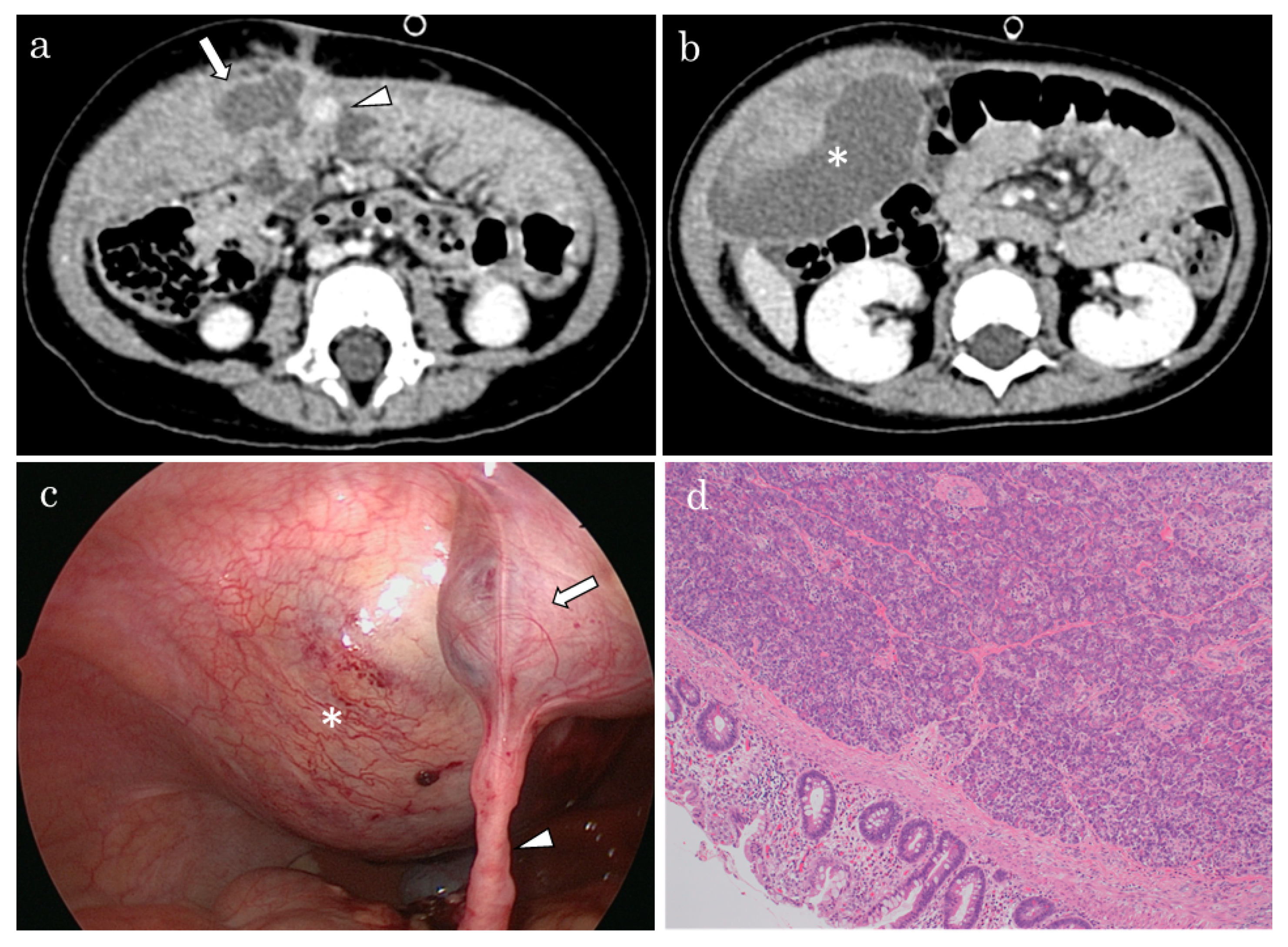
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gray, S.W.; Skandalakis, J.; Achauer, B.M. Embryology for surgeons. Plast. Reconstr. Surg. 1980, 65, 156–186. [Google Scholar] [CrossRef]
- Vane, D.W.; West, K.W.; Grosfeld, J.L. Vitelline duct anomalies: Experience with 217 childhood cases. Arch. Surg. 1987, 122, 542–547. [Google Scholar] [CrossRef] [PubMed]
- De Castro Barbosa, J.J.; Dockerty, M.B.; Waugh, J.M. Pancreatic heterotopia: Review of the literature and report of 41 authenticated surgical cases of which 25 were clinically significant. Surg. Gynecol. Obstet. 1946, 82, 527–542. [Google Scholar] [PubMed]
- Yamaguchi, M.; Takeuchi, S.; Awazu, S. Meckel’s diverticulum. Investigation of 600 patients in Japanese literature. Am. J. Surg. 1978, 136, 247–249. [Google Scholar] [CrossRef]
- Chiang, L.S. Vitelline duct remnant appearing as a hemorrhagic umbilical mass. JAMA 1982, 247, 2812–2813. [Google Scholar] [CrossRef] [PubMed]
- Tillig, B.; Gerein, V.; Coerdt, W.; Vahdad, R.; Engert, J. Supraumbilical pseudocystic tumour due to ectopic pancreatic tissue located in a rest of the omphaloenteric duct. Eur. J. Pediatr. Surg. 2004, 14, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Abdelgabar, A.; Wojciechowski, M.; Van de Vijver1, E.; Ruppert, M.; Hubens, G.; Balliu, L.; Creytens, D.; Vaneerdeweg1, W. Ectopic pancreatic tissue at the umbilicus in childhood: A case report and review of the literature. Acta Chir. Belg. 2013, 113, 452–454. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Kim, H.; Jung, K.W.; Chung, J.H. Heterotopic pancreas in omphalomesenteric duct remnant results in persistent umbilical discharge. Korean J. Pathol. 2014, 48, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Nakib, G.; Saviour, M.J. Bruises around the umbilicus in an infant. Pediatr. Rep. 2016, 8, 6555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Sim, C.K.; Mantoo, S. Heterotopic pancreas in the omphalomesenteric duct remnant in a 9-month-old girl: A case report and literature review. Diagn. Pathol. 2017, 12, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| No. | Age/Sex | Umbilical Abnormality | Stomach Tissue | Intestinal Tissue | Reference |
|---|---|---|---|---|---|
| 1 | 1 year/M | Swelling after trauma | No | Yes | [5] |
| 2 | 2 years/M | Umbilical tumor | No | No | [6] |
| 3 | 2 years/M | Abrasion, oozing | Yes | Yes | [7] |
| 4 | 3 months/F | Umbilical discharge | No | Yes | [8] |
| 5 | 16 months/M | Umbilical discharge, erythema | No | No | [9] |
| 6 | 9 months/F | Erythema | No | Yes | [10] |
| 7 | 15 months/F | None | Yes | Yes | Present case |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshizawa, H.; Terui, K.; Nakata, M.; Mitsunaga, T.; Komatsu, S.; Saito, T.; Hishiki, T. Amylase Levels Are Useful for Diagnosing Omphalomesenteric Cysts: A Case Report. Pediatr. Rep. 2022, 14, 127-130. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14010018
Yoshizawa H, Terui K, Nakata M, Mitsunaga T, Komatsu S, Saito T, Hishiki T. Amylase Levels Are Useful for Diagnosing Omphalomesenteric Cysts: A Case Report. Pediatric Reports. 2022; 14(1):127-130. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14010018
Chicago/Turabian StyleYoshizawa, Hiroko, Keita Terui, Mitsuyuki Nakata, Tetsuya Mitsunaga, Shugo Komatsu, Takeshi Saito, and Tomoro Hishiki. 2022. "Amylase Levels Are Useful for Diagnosing Omphalomesenteric Cysts: A Case Report" Pediatric Reports 14, no. 1: 127-130. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14010018