
Outcomes of the Pregnancies with Chronic Myeloid Leukemia in the Tyrosine Kinase Inhibitor Era and Literature Review

Abstract
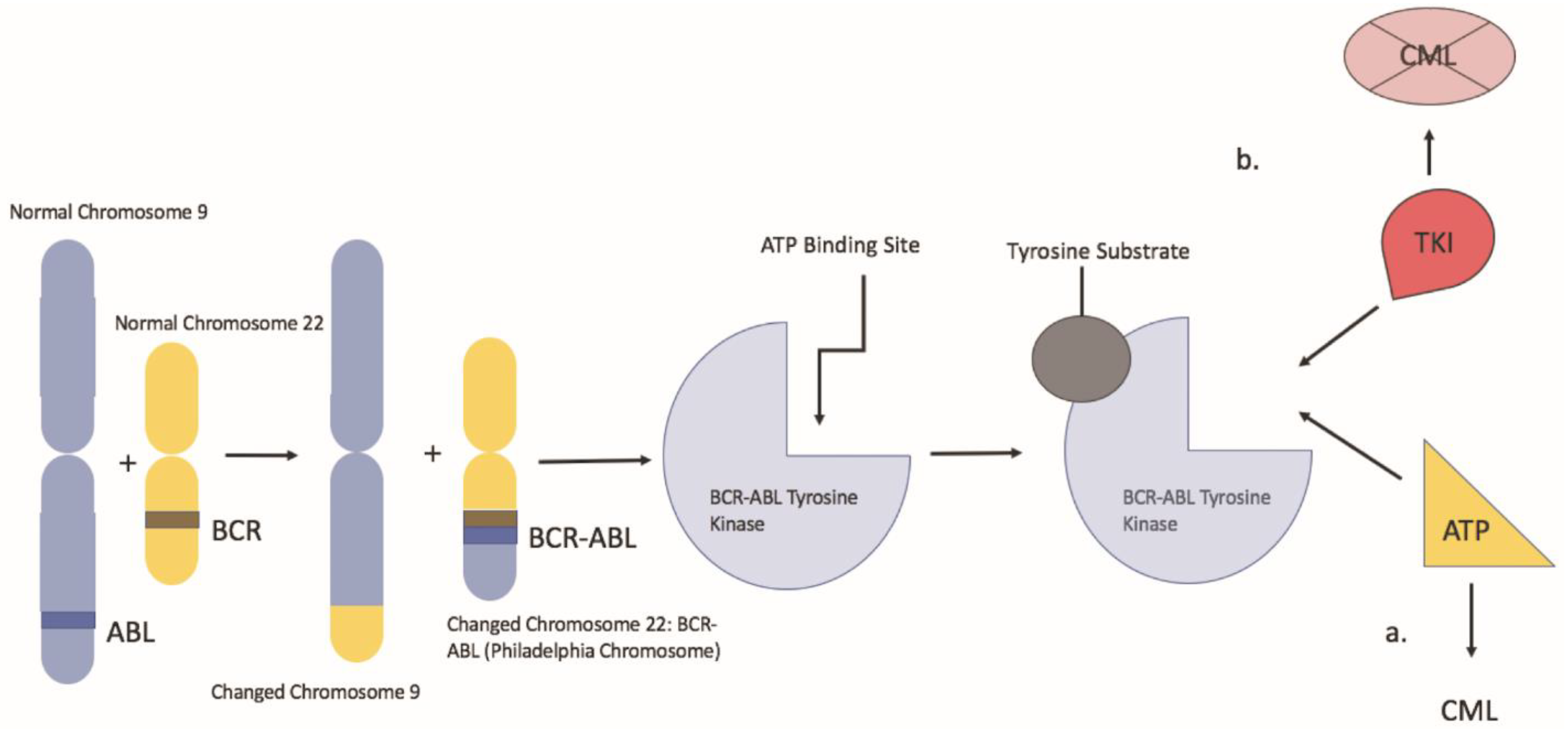
:1. Introduction
2. Case Presentations
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rowley, J.D. Letter: A new consistent chromosomal abnormality in chronic myelogenous leukaemia identified by quinacrine fluorescence and Giemsa staining. Nature 1973, 243, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Iqbal, N. Imatinib: A breakthrough of targeted therapy in cancer. Chemother. Res. Pract. 2014, 2014, 357027. [Google Scholar] [CrossRef] [PubMed]
- Hehlmann, R. Chronic Myeloid Leukemia in 2020. Hemasphere 2020, 4, e468. [Google Scholar] [CrossRef]
- Press, R.D.; Kamel-Reid, S.; Ang, D. BCR-ABL1 RT-qPCR for monitoring the molecular response to tyrosine kinase inhibitors in chronic myeloid leukemia. J. Mol. Diagn. 2013, 15, 565–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Milojkovic, D.; Apperley, J.F. How I treat leukemia during pregnancy. Blood 2014, 123, 974–984. [Google Scholar] [CrossRef] [Green Version]
- Abruzzese, E.; Mauro, M.; Apperley, J.; Chelysheva, E. Tyrosine kinase inhibitors and pregnancy in chronic myeloid leukemia: Opinion, evidence, and recommendations. Ther. Adv. Hematol. 2020, 11, 2040620720966120. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, S.; Kantarjian, H.; Ault, P.; Cortes, J.E. Successful completion of pregnancy in a patient with chronic myeloid leukemia without active intervention: A case report and review of the literature. Clin. Lymphoma Myeloma 2009, 9, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Abruzzese, E.; Chelysheva, E.; Guha, M.; Wallis, N.; Apperley, J.F. The impact of dasatinib on pregnancy outcomes. Am. J. Hematol. 2015, 90, 1111–1115. [Google Scholar] [CrossRef] [Green Version]
- Burwick, R.M.; Kuo, K.; Brewer, D.; Druker, B.J. Maternal, Fetal, and Neonatal Imatinib Levels With Treatment of Chronic Myeloid Leukemia in Pregnancy. Obstet. Gynecol. 2017, 129, 831–834. [Google Scholar] [CrossRef]
- Pye, S.M.; Cortes, J.; Ault, P.; Hatfield, A.; Kantarjian, H.; Pilot, R.; Rosti, G.; Apperley, J.F. The effects of imatinib on pregnancy outcome. Blood 2008, 111, 5505–5508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abruzzese, E.; de Fabritiis, P.; Trawinska, M.M.; Niscola, P.; Apperley, J.F.; Mauro, M.J. Back to the future: Treatment-free remission and pregnancy in chronic myeloid leukemia. Eur. J. Haematol. 2019, 102, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Barkoulas, T.; Hall, P.D. Experience with dasatinib and nilotinib use in pregnancy. J. Oncol. Pharm. Pract. 2018, 24, 121–128. [Google Scholar] [CrossRef] [PubMed]
- El Gendy, M.M.; Kandil, A.M.; Helal, M.A.; Zahou, F.M. The teratogenic effects of imatinib mesylate on rat fetuses. Toxicol. Rep. 2015, 2, 654–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, Y.; Murai, K.; Yamaguchi, K.; Miyagishima, T.; Shindo, M.; Ogawa, K.; Nagashima, T.; Sato, S.; Watanabe, R.; Yamamoto, S.; et al. Pharmacokinetics and pharmacodynamics of dasatinib in the chronic phase of newly diagnosed chronic myeloid leukemia. Eur. J. Clin. Pharmacol. 2016, 72, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Rambhatla, A.; Strug, M.R.; De Paredes, J.G.; Cordoba Munoz, M.I.; Thakur, M. Fertility considerations in targeted biologic therapy with tyrosine kinase inhibitors: A review. J. Assist. Reprod. Genet. 2021, 38, 1897–1908. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Dasgupta, S.; Kanti Ray, U.; Gharami, F.; Bose, C.K.; Mukhopadhyay, S. Pregnancy outcome in chronic myeloid leukemia patients on imatinib therapy. Ir. J. Med. Sci. 2015, 184, 183–188. [Google Scholar] [CrossRef]
- Apperley, J. Issues of imatinib and pregnancy outcome. J. Natl. Compr. Cancer Netw. 2009, 7, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Carlier, P.; Markarian, M.; Bernard, N.; Lagarce, L.; Dautriche, A.; Bene, J.; Sam-Lai, N.F.; Eftekhari, P. Erratum to: Pregnancy outcome among partners of male patients receiving imatinib, dasatinib or nilotinib in chronic myeloid leukemia: Reports collected by the French network pharmacovigilance centers. Arch. Gynecol. Obstet. 2017, 295, 1059. [Google Scholar] [CrossRef] [Green Version]
- Sheng, W.; Sun, N. Successful pregnancy and delivery in a patient with chronic myeloid leukemia: A case report and review of the literature. Springerplus 2016, 5, 2055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balsat, M.; Etienne, M.; Elhamri, M.; Hayette, S.; Salles, G.; Thomas, X. Successful pregnancies in patients with BCR-ABL-positive leukemias treated with interferon-alpha therapy during the tyrosine kinase inhibitors era. Eur. J. Haematol. 2018, 101, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Chelysheva, E.; Turkina, A.; Polushkina, E.; Shmakov, R.; Zeifman, A.; Aleshin, S.; Shokhin, I.; Guranda, D.; Oksenjuk, O.; Mordanov, S.; et al. Placental transfer of tyrosine kinase inhibitors used for chronic myeloid leukemia treatment. Leuk. Lymphoma 2018, 59, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, H.; Jaafar, H.; Rajnics, P.; Khan, M.I.; Kajtar, B. Outcome of pregnancy in chronic myeloid leukaemia patients treated with tyrosine kinase inhibitors: Short report from a single centre. Leuk. Res. 2015, 39, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Mahon, F.X. Discontinuation of TKI therapy and ’functional’ cure for CML. Best Pract. Res. Clin. Haematol. 2016, 29, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Rea, D.; Nicolini, F.E.; Tulliez, M.; Guilhot, F.; Guilhot, J.; Guerci-Bresler, A.; Gardembas, M.; Coiteux, V.; Guillerm, G.; Legros, L.; et al. Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood 2017, 129, 846–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imagawa, J.; Tanaka, H.; Okada, M.; Nakamae, H.; Hino, M.; Murai, K.; Ishida, Y.; Kumagai, T.; Sato, S.; Ohashi, K.; et al. Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicentre phase 2 trial. Lancet Haematol. 2015, 2, e528–e535. [Google Scholar] [CrossRef]
- Saussele, S.; Richter, J.; Guilhot, J.; Gruber, F.X.; Hjorth-Hansen, H.; Almeida, A.; Janssen, J.; Mayer, J.; Koskenvesa, P.; Panayiotidis, P.; et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): A prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018, 19, 747–757. [Google Scholar] [CrossRef] [Green Version]
- Palani, R.; Milojkovic, D.; Apperley, J.F. Managing pregnancy in chronic myeloid leukaemia. Ann. Hematol. 2015, 94 (Suppl. 2), S167–S176. [Google Scholar] [CrossRef] [PubMed]
- Deininger, M.W.; Shah, N.P.; Altman, J.K.; Berman, E.; Bhatia, R.; Bhatnagar, B.; DeAngelo, D.J.; Gotlib, J.; Hobbs, G.; Maness, L.; et al. Chronic Myeloid Leukemia, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1385–1415. [Google Scholar] [CrossRef]
- Dowding, C.; Gordon, M.; Guo, A.P.; Maison, D.; Osterholz, J.; Siczkowski, M.; Goldman, J. Potential mechanisms of action of interferon-alpha in CML. Leuk. Lymphoma 1993, 11 (Suppl. 1), 185–191. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; O’Brien, S.; Cortes, J.E.; Shan, J.; Giles, F.J.; Rios, M.B.; Faderl, S.H.; Wierda, W.G.; Ferrajoli, A.; Verstovsek, S.; et al. Complete cytogenetic and molecular responses to interferon-alpha-based therapy for chronic myelogenous leukemia are associated with excellent long-term prognosis. Cancer 2003, 97, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Mubarak, A.A.; Kakil, I.R.; Awidi, A.; Al-Homsi, U.; Fawzi, Z.; Kelta, M.; Al-Hassan, A. Normal outcome of pregnancy in chronic myeloid leukemia treated with interferon-alpha in 1st trimester: Report of 3 cases and review of the literature. Am. J. Hematol. 2002, 69, 115–118. [Google Scholar] [CrossRef]
- Yazdani Brojeni, P.; Matok, I.; Garcia Bournissen, F.; Koren, G. A systematic review of the fetal safety of interferon alpha. Reprod. Toxicol. 2012, 33, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Abu-Tineh, M.; Kassem, N.; Abdulla, M.A.; Ismail, O.M.; Ghasoub, R.; Aldapt, M.B.; Yassin, M.A. Outcome of Pregnancy in the Era of Pegylated Interferon Alpha 2a in Females with Essential Thrombocythemia: An Experience from Qatar. Case Rep. Oncol. 2020, 13, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, M.; Samuelsson, J.; Nilsson, L.; Knutsen, H.; Ghanima, W.; Westin, J.; Johansson, P.L.; Andreasson, B. Genetic variation in IL28B (IFNL3) and response to interferon-alpha treatment in myeloproliferative neoplasms. Eur. J. Haematol. 2018, 100, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Kreil, S.; Waghorn, K.; Ernst, T.; Chase, A.; White, H.; Hehlmann, R.; Reiter, A.; Hochhaus, A.; Cross, N.C.; German, C.M.L.S.G. A polymorphism associated with STAT3 expression and response of chronic myeloid leukemia to interferon alpha. Haematologica 2010, 95, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.J.; Alhejazi, A.; Ahmed, S.O.; Al Mohareb, F.; AlSharif, F.; AlZahrani, H.; Mohamed, S.Y.; Rasheed, W.; AlDawsari, G.; Ibrahim, K.; et al. Leukemia during pregnancy: Long term follow up of 32 cases from a single institution. Hematol. Oncol. Stem Cell Ther. 2014, 7, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes, J.; Kantarjian, H. How I treat newly diagnosed chronic phase CML. Blood 2012, 120, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Granatowicz, A.; Piatek, C.I.; Moschiano, E.; El-Hemaidi, I.; Armitage, J.D.; Akhtari, M. An Overview and Update of Chronic Myeloid Leukemia for Primary Care Physicians. Korean J. Fam. Med. 2015, 36, 197–202. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | n | Treatment during Pregnancy | Elective Abortion | Spontaneous Abortion | Fetal Abnormalities | Normal Live Birth | Unknown Outcome |
|---|---|---|---|---|---|---|---|
| Pye et al. | 180 | 1st trimester Imatinib use: 70% 1st-3rd trimester Imatinib use 26% | 19% | 10% | 7% | 35% | 31% |
| Abruzzese et al. | 265 | Exposed to Imatinib during organogenesis (>5-week gestation) | 17% | 9% | 6% | 48% | 21% |
| Cortes et al. | 78 | Dasatinib | 23% | 10% | 9% | 19% | 41% |
| Wang et al. | 25 | Imatinib: 24 patients Nilotinib: 1 patient | 44% | 175 | 0% | 39% | 0% |
| Hall et al. | 6 | 1st trimester TKI use: 4 patients 1st-3rd trimester TKI use: 1 patient | 17% | 17% | 33% | 33% | 0% |
| Study | n | Pre-Pregnancy Treatment | Therapy during Pregnancy | Outcomes |
|---|---|---|---|---|
| Balsat et al. | 12 | 7 Imatinib, 3 Nilotinib, 2 None | 9 PEG-IFN, 2 IFN | 12 live healthy births |
| Law et al.. | 6 | 6 Imatinib | 5 IFN, 1 Observation | 1 elective abortion 5 full term deliveries |
| Chelyshava et al. | 48 | Unclear | 14 Observation, 5 IFN, 1HU | 14 elective abortions 1 spontaneous abortion 7 live healthy births |
| Alizadeh et al. | 28 (16 patients) | 13 Imatinib: 2 Dasatinib 1 Nilotinib | 8 Observation, 8 IFN | 1 spontaneous abortion 2 congenital defects 23 lives healthy births |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo, D.R.; Park, D.; Mehta, A.; Kaur, S.; Nguyen, A.; Akhtari, M. Outcomes of the Pregnancies with Chronic Myeloid Leukemia in the Tyrosine Kinase Inhibitor Era and Literature Review. Hematol. Rep. 2022, 14, 45-53. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010008
Castillo DR, Park D, Mehta A, Kaur S, Nguyen A, Akhtari M. Outcomes of the Pregnancies with Chronic Myeloid Leukemia in the Tyrosine Kinase Inhibitor Era and Literature Review. Hematology Reports. 2022; 14(1):45-53. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010008
Chicago/Turabian StyleCastillo, Dan Ran, Daniel Park, Akhil Mehta, Simmer Kaur, Anthony Nguyen, and Mojtaba Akhtari. 2022. "Outcomes of the Pregnancies with Chronic Myeloid Leukemia in the Tyrosine Kinase Inhibitor Era and Literature Review" Hematology Reports 14, no. 1: 45-53. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep14010008