
Physical Health and Work Ability among Healthcare Workers. A Cross-Sectional Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Tools
2.3. Data Analysis
3. Results
3.1. Study Participants
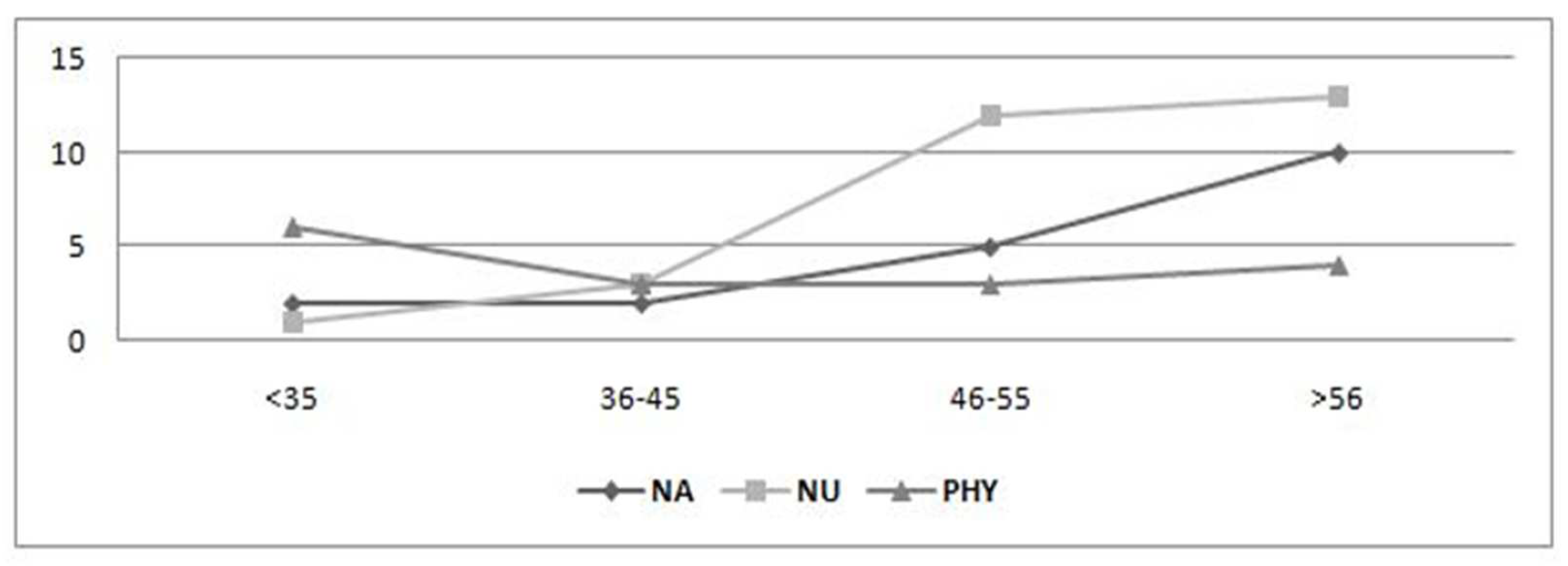
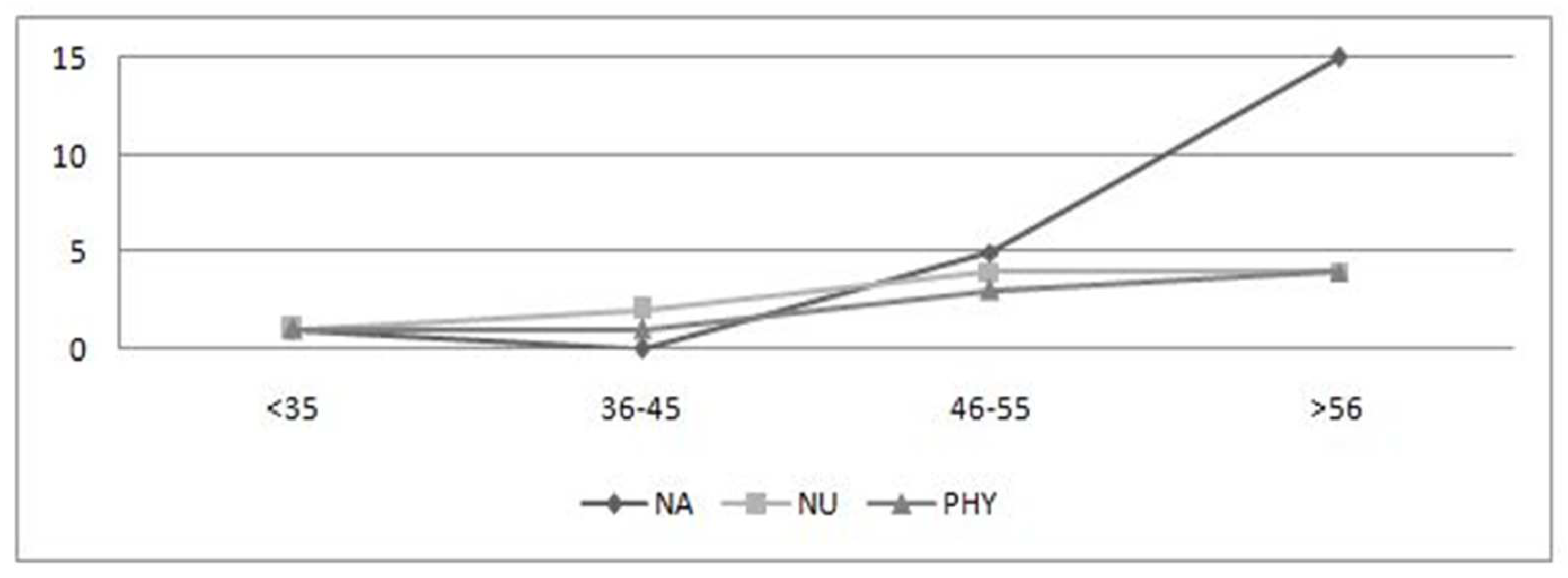
3.2. Physical Health Status and Workability
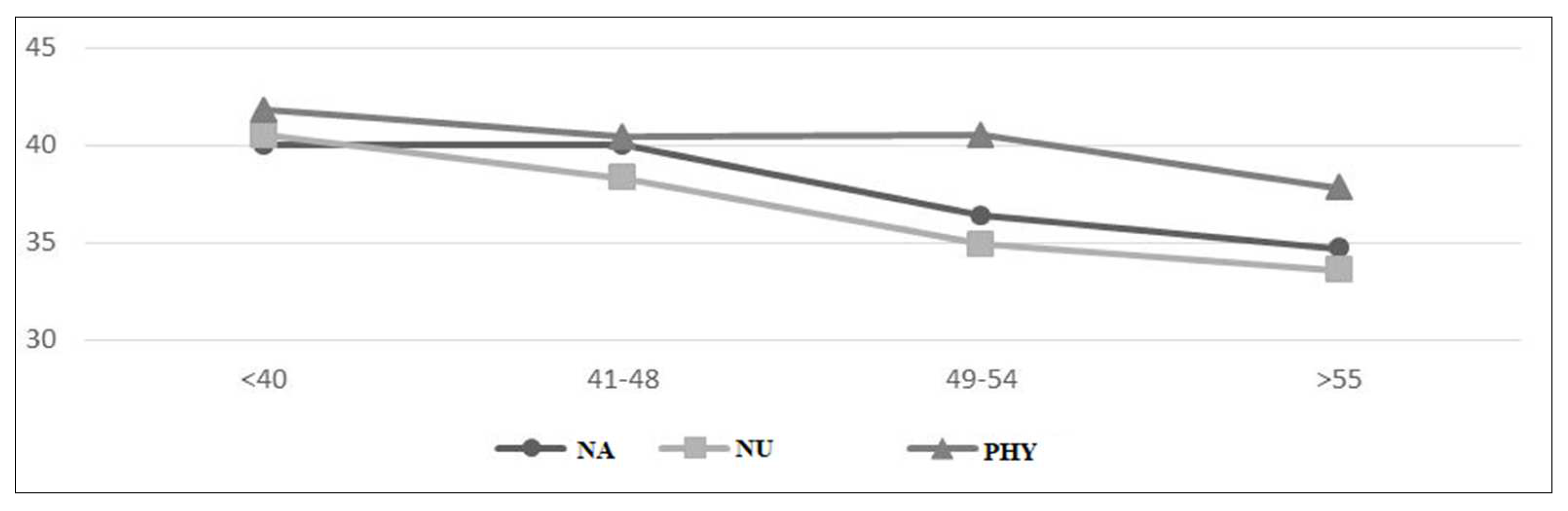
3.3. Relationship between Age and Physical Health Status
4. Discussion
5. Conclusions
Applying Research to Occupational Health Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aiyar, S.; Ebeke, C.; Shao, X. 2016. The Impact of Workforce Aging on European Productivity. Available online: https://www.imf.org/external/pubs/ft/wp/2016/wp16238.pdf (accessed on 15 February 2022).
- Eurostat. 2020. Health Workers in Thew EU by Age Group. Available online: https://ec.europa.eu/eurostat/documents/4187653/10321595/Health_workers_2019Q4-02.jpg/a4443889-9ae8-43bd-a47b-b45b44b21278?t=1586348190441 (accessed on 15 February 2022).
- Ng, T.W.H.; Feldman, D.C. How do within-person changes due to aging affect job performance? J. Vocat. Behav. 2013, 83, 500–513. [Google Scholar] [CrossRef]
- Pira, E.; Garzaro, G.; De Cillis, E.; Donato, F.; Ciocan, C.; Patrucco, M. Evolution of the concept OS&H from the second Post-war to today: From prescriptive system to assessment and management of risks in system quality-The extended model in collaboration with large Facilities. Evolution of multidisciplinary culture of safety and OS&H. GEAM 2018, 154, 6–20. [Google Scholar]
- Harman, D. Aging: Phenomena and theories. Ann. N. Y. Acad Sci. 1998, 20, 1–7. [Google Scholar] [CrossRef]
- Knoche, K.; Sochert, R.; Houston, K. Promoting Healthy Work for Workers with Chronic Illness: A Guide to Good Practice; European Network for Workplace Health Promotion (ENWHP): Edinburgh, UK, 2012; p. 34. [Google Scholar]
- Gragnano, A.; Miglioretti, M.; Frings-Dresen, M.H.W.; de Boer, A.G.E.M. Adjustment between work demands and health needs: Development of the Work–Health Balance Questionnaire. Rehabil. Psychol. 2017, 62, 374–386. [Google Scholar] [CrossRef] [PubMed]
- Börsch-Supan, A.; Bristle, J.; Brugiavini, A.; Jusot, F. Health and Socio-Economic Status over the Life Course: First Results from SHARE Waves 6 and 7; De Gruyter Oldenbourg: Berlin, Germany, 2019; p. 200. [Google Scholar]
- Camerino, D.; Conway, P.M.; Van Der Heijden, B.I.J.M.; Estryn-Behar, M.; Consonni, D.; Gould, D.; Hasselhorn, H.-M.; The NEXT-Study Group. Low-perceived work ability, ageing and intention to leave nursing: A comparison among 10 European countries. J. Adv. Nurs. 2006, 56, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Leijten, F.R.; Heuvel, S.G.V.D.; Ybema, J.F.; Van Der Beek, A.J.; Robroek, S.; Alex, B. The influence of chronic health problems on work ability and productivity at work: A longitudinal study among older employees. Scand. J. Work. Environ. Health 2014, 40, 473–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilmarinen, J. Aging workers. Occup. Environ. Med. 2001, 58, 546–552. [Google Scholar] [CrossRef] [Green Version]
- Sottimano, I.; Viotti, S.; Guidetti, G.; Converso, D. Protective factors for work ability in preschool teachers. Occup. Med. 2017, 67, 301–304. [Google Scholar] [CrossRef] [Green Version]
- Ilmarinen, J. From Work Ability Research to Implementation. Int. J. Environ. Res. Public Health 2019, 16, 2882. [Google Scholar] [CrossRef] [Green Version]
- Tuomi, K.; Huuhtanen, P.; Nykyri, E.; Ilmarinen, J. Promotion of work ability, the quality of work and retirement. Occup. Med. 2001, 51, 318–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pohjonen, T. Perceived work ability of home care workers in relation to individual and work-related factors in different age groups. Occup. Med. 2001, 51, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazloumi, A.; Rostamabadi, A.; Saraji, G.N.; Foroushani, A.R. Work Ability Index (WAI) and Its Association with Psychosocial Factors in One of the Petrochemical Industries in Iran. J. Occup. Health 2012, 54, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, T.I.J.; Elders, L.; de Zwart, B.C.H.; Burdorf, A. The effects of work-related and individual factors on the work ability index: A systematic review. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garzaro, G.; Sottimano, I.; Di Maso, M.; Bergamaschi, E.; Coggiola, M.; Converso, D.; Iavicoli, S.; Pira, E.; Viotti, S. Work Ability among Italian Bank Video Display Terminal Operators: Socio-Demographic, Lifestyle, and Occupational Correlates. Int. J. Environ. Res. Public Health 2019, 16, 1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emberland, J.S.; Knardahl, S. Contribution of psychological, social and mechanical work exposure to low work ability, a prospective study. Occup. Environ. Med. 2015, 57, 300–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viotti, S.; Guidetti, G.; Loera, B.; Martini, M.; Sottimano, I.; Converso, D. Stress, work ability, and an aging workforce: A study among women aged 50 and over. Int. J. Stress Manag. 2017, 24, 98–121. [Google Scholar] [CrossRef]
- Costa, G.; Sartori, S.; Åkerstedt, T. Influence of Flexibility and Variability of Working Hours on Health and Well-Being. Chrono. Int. 2006, 23, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Copertaro, A.; Bracci, M.; Barbaresi, M.; Santarelli, L. Role of waist circumference in the diagnosis of metabolic syndrome and assessment of cardiovascular risk in shift workers. La Med. Del Lav. 2008, 99, 444–453. [Google Scholar]
- Costa, G.; Sartori, S. Ageing, working hours and workability. Ergonomics 2007, 50, 1914–1930. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L.; Turan, B.; Scheibe, S.; Ram, N.; Ersner-Hershfield, H.; Samanez-Larkin, G.R.; Brooks, K.P.; Nesselroade, J.R. Emotional experience improves with age: Evidence based on over 10 years of experience sampling. Psychol. Aging 2011, 26, 21–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byers, A.L.; Yaffe, K.; Covinsky, K.E.; Friedman, M.B.; Bruce, M.L. High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2010, 67, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index, 2nd ed.; Finnish Institute of Occupational Health: Helsinki, Finland, 1998. [Google Scholar]
- IBM SPSS Statistics for Windows; Version 25.0; IBM Corp: Armonk, NY, USA, 2017.
- Aittomäki, A.; Lahelma, E.; Roos, E. Work conditions and socioeconomic inequalities in work ability. Scand. J. Work. Environ. Health 2003, 29, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carel, R.S.; Zusman, M.; Karakis, I. Work Ability Index in Israeli Hospital Nurses: Applicability of the Adapted Questionnaire. Exp. Aging Res. 2013, 39, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Martini, M.; Converso, D. Lo studio del burnout in sanità: Rapporto coi pazienti e relazione lavoro-famiglia come richieste e risorse. G Ital Med Lav Ergon 2012, 34, 41–50. [Google Scholar]
- Silva, T.P.D.; Araujo, W.N.; Stival, M.M.; Toledo, A.M.; Burke, T.N.; Carregaro, R.I. Musculoskeletal discomfort, work ability and fatigue in nursing professionals working in a hospital environment. Rev. Esc. Enferm. 2018, 52, e03332. [Google Scholar]
- Nigeliskii, C.; Lautert, L. Occupational stress and work capacity of nurses of a hospital group. Rev. Lat. Am. De Enferm. 2011, 19, 606–613. [Google Scholar] [CrossRef]
- Najimi, A.; Goudarzi, A.M.; Sharifirad, G. Causes of job stress in nurses: A cross-sectional study. Iran. J. Nurs. Midwifery Res. 2012, 17, 301–305. [Google Scholar]
- Turci, C.; Alvaro, R.; Fabretti, A.; Fida, R.; Giorgi, F.; Maccari, A.; Proietti Sili, A.; Stievano, A.; Tolentino Diaz, M.Y.; Trinca, D.; et al. La salute organizzativa degli infermieri in alcune strutture sanitarie di Roma e della Provincia. L’Infermiere 2013, 50, e89–e98. [Google Scholar]
- Sehlen, S.; Vordermark, D.; Schäfer, C.; Herschbach, P.; Bayerl, A.; Pigorsch, S.; Rittweger, J.; Dormin, C.; Bolling, T.; Wypior, H.J.; et al. Job stress and job satisfaction of physicians, radiographers, nurses and physicists working in radiotherapy: A multicenter analysis by the DEGRO Quality of Life Work Group. Radiat. Oncol. 2009, 4, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, T.I.; Robroek, S.J.; Plat, J.F.; Koopmanschap, M.A.; Burdorf, A. The importance of job control for workers with decreased work ability to remain productive at work. Int. Arch. Occup. Environ. Health 2011, 84, 705–712. [Google Scholar] [CrossRef] [Green Version]
- Uthaman, T.; Chua, T.L.; Ang, S.Y. Older nurses: A literature review on challenges, factors in early retirement and workforce retention. Proc. Singap. Healthc. 2015, 25, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Tillmann, T.; Vaucher, J.; Okbay, A.; Pikhart, H.; Peasey, A.; Kubinova, R.; Pajak, A.; Tamosiunas, A.; Malyutina, S.; Hartwig, F.P.; et al. Education and coronary heart disease: Mendelian randomisation study. BMJ 2017, 358, j3542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baracco, A.; Coggiola, M.; Bosio, D.; Perrelli, F.; Garzaro, G.; Turcu, V.; Pira, E. Whole body biomechanical burden of healthcare workers: Proposal for a complementary risk assessment and management tool (HOARA). Med. Lav. 2019, 110, 372–388. [Google Scholar] [PubMed]
- Costa, G.; Sartori, S.; Bertoldo, B.; Olivato, D.; Ciuffa, V.; Antonacci, G. L’Indice di Capacità di Lavoro in operatori sanitari The Work Ability Index in hospital workers. G. Ital. Di Med. Del Lav. Ed Ergon. 2005, 27, 355–358. (In Italian) [Google Scholar]
- Petrelli, A.; Sebastiani, G.; Di Napoli, A.; Macciotta, A.; Di Filippo, P.; Strippoli, E.; Mirisola, A.; d’Errico, A. Education inequalities in cardiovascular and coronary heart disease in Italy and the role of behavioral and biological risk factor. Nutr. Metab. Cardiovasc. Dis. 2021, (in press). [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Nursing Aides n (%) | Nurses n (%) | Physicians n (%) |
|---|---|---|---|
| Sex | |||
| Male | 33 (45.2) | 15(20.5) | 39(52.7) |
| Female | 40 (54.8) | 58(79.5) | 35(47.3) |
| Age | |||
| <35 | 8 (11) | 8 (11) | 38 (51.4) |
| 36–45 | 18 (24.7) | 25 (34.2) | 10 (13.5) |
| 46–55 | 22 (30.1) | 24 (32.9) | 14 (18.9) |
| >56 | 25 (34.2) | 16 (21.9) | 12 (16.2) |
| Work contract | |||
| Full Time | 64 (87.7) | 66 (94.3) | 74 (100) |
| Part Time | 7 (9.6) | 4 (5.7) | - |
| Marital status | |||
| Single | 17 (23.3) | 20 (27.4) | 36 (48.6) |
| Married/partner | 39 (54.4) | 42 (57.5) | 33 (44.6) |
| Separated/divorced | 10 (13.7) | 10 (13.7) | 4 (5.4) |
| Widow/widower | 7 (9.6) | 1 (1.4) | 1 (1.4) |
| Children | |||
| Yes | 55 (75.3) | 51 (70.8) | 31 (41.9) |
| No | 18 (24.7) | 21 (29.2) | 43 (58.1) |
| Other people to care for | |||
| Yes | 30 (41.7) | 27 (37.5) | 14 (19.7) |
| No | 42 (58.3) | 45 (62.5) | 57 (80.3) |
| Benefits according to Law 104/92 | |||
| Yes | 17 (23.3) | 10 (14.1) | 4 (5.5) |
| No | 56 (76.7) | 61 (85.9) | 69 (94.5) |
| Body Mass Index (BMI) | |||
| Underweight | - | 2 (2.8) | 3 (4.2) |
| Normal weight | 36 (52.2) | 48 (67.6) | 53 (74.6) |
| Overweight | 27 (39.1) | 14 (19.7) | 13 (18.3) |
| Obesity | 6 (8.7) | 7 (9.9) | 2 (2.8) |
| Diagnosis | Nursing Aides n (%) | Nurses n (%) | Physicians n (%) |
|---|---|---|---|
| Cardiovascular disease | 21 (28.8) | 11 (15.1) | 9 (12.2) |
| Musculoskeletal disorders | 19 (26) | 29 (39.7) | 16 (21.6) |
| Respiratory disorders | 6 (8.2) | 6 (8.2) | 3 (4.1) |
| Mental disorders | 3 (4.1) | 8 (11) | 6 (8.1) |
| Sensory neurological disorders | 6 (8.2) | 11 (15.1) | 10 (13.5) |
| Gastrointestinal disorders | 11 (15.1) | 11 (15.1) | 6 (8.1) |
| Genitourinary disorders | 8 (11) | 4 (5.5) | 3 (4.1) |
| Dermatological disorders | 17 (23.3) | 19 (26.0) | 8 (10.8) |
| Oncological disorders | 1 (1.4) | - | 1 (1.4) |
| Metabolic and/or endocrine disorders | 17 (23.3) | 7 (9.6) | 2 (2.7) |
| Nephropathies | - | 2 (2.7) | - |
| Birth defects | - | 1 (1.4) | 2 (2.7) |
| Variable | Nursing Aides M (SD) | Nurses M (SD) | Physicians M (SD) |
|---|---|---|---|
| Average WAI score | 37.1 (6.4) | 36.4 (6.1) | 40.8 (3.6) |
| Workability | n (%) | n (%) | n (%) |
| Very good (WAI 49–44) | 12 (16.4) | 9 (13.2) | 18 (25.4) |
| Good (WAI 43–37) | 28 (38.4) | 28 (41.2) | 43 (60.6) |
| Medium (WAI 36–28) | 26 (35.6) | 28 (41.2) | 10 (14.1) |
| Poor (WAI 7–27) | 7 (9.6) | 3 (4.4) | - |
| Workability according to age | M (SD) | M (SD) | M (SD) |
| <35 years | 40.0 (5.5) | 40.5 (3.2) | 47.8 (3.2) |
| 36–45 years | 40.0 (7.0) | 38.3 (6.8) | 40.4 (3.2) |
| 46–55 years | 36.4 (5.8) | 34.9 (5.3) | 40.5 (4.1) |
| >56 years | 34.7 (5.6) | 33.6 (4.9) | 37.8 (3.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garzaro, G.; Clari, M.; Ciocan, C.; Albanesi, B.; Guidetti, G.; Dimonte, V.; Sottimano, I. Physical Health and Work Ability among Healthcare Workers. A Cross-Sectional Study. Nurs. Rep. 2022, 12, 259-269. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12020026
Garzaro G, Clari M, Ciocan C, Albanesi B, Guidetti G, Dimonte V, Sottimano I. Physical Health and Work Ability among Healthcare Workers. A Cross-Sectional Study. Nursing Reports. 2022; 12(2):259-269. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12020026
Chicago/Turabian StyleGarzaro, Giacomo, Marco Clari, Catalina Ciocan, Beatrice Albanesi, Gloria Guidetti, Valerio Dimonte, and Ilaria Sottimano. 2022. "Physical Health and Work Ability among Healthcare Workers. A Cross-Sectional Study" Nursing Reports 12, no. 2: 259-269. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12020026