
Knowledge and Attitudes Regarding Medication Errors among Nurses: A Cross-Sectional Study in Major Jeddah Hospitals


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Study Instrument and Measurement of the Variables
2.4. Ethical Approval
2.5. Administration of the Questionnaire
2.6. Data Analysis
3. Results
3.1. Descriptive Analysis and Nurses’ Demographic Profile
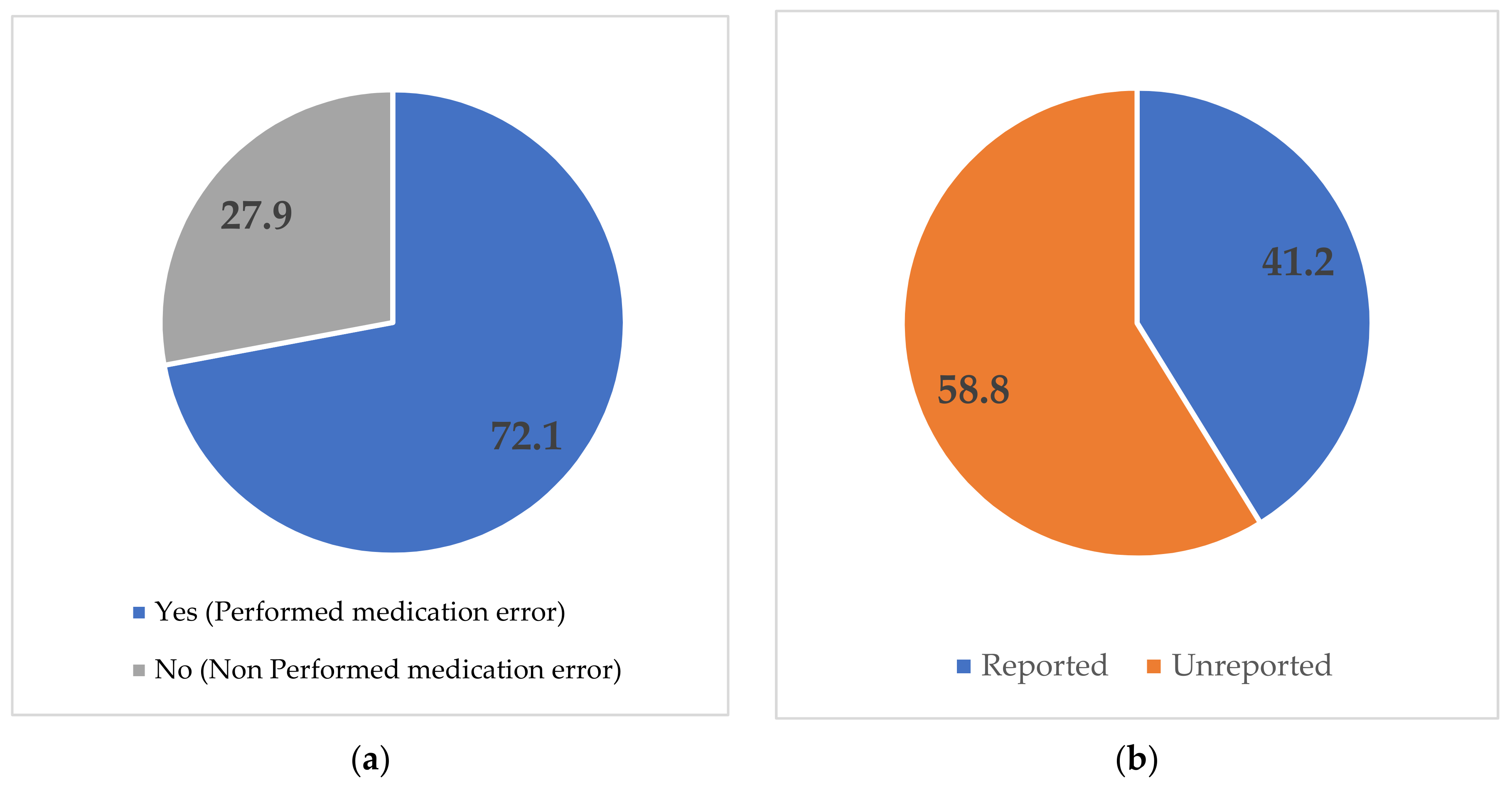
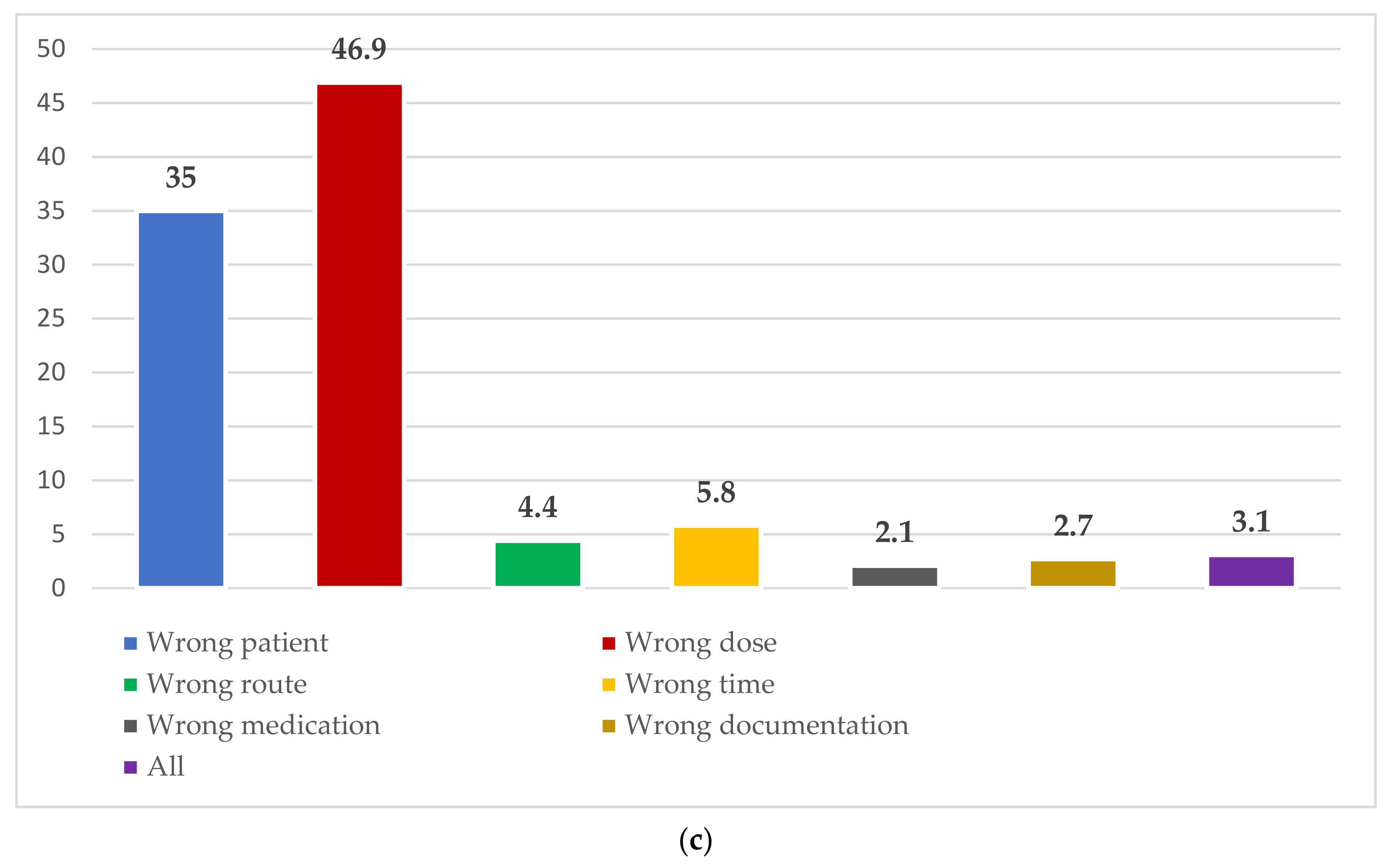
3.2. Prevalence of Medication Error
3.3. Nurses’ Knowledge of Medication Error
3.4. Nurses’ Attitudes toward Medication Error
3.5. Overall Knowledge of and Attitude towards Medication Error
3.6. Factors Associated with Medication Error
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cloete, L. Reducing medication errors in nursing practice. Nurs. Stand. 2015, 14, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Zarea, K.; Mohammadi, A.; Beiranvand, S.; Hassani, F.; Baraz, S. Iranian nurses’ medication errors: A survey of the types, the causes, and the related factors. Int. J. Afr. Nurs. Sci. 2018, 8, 112–116. [Google Scholar] [CrossRef]
- Cheragi, M.A.; Manoocheri, H.; Mohammadnejad, E.; Ehsani, S.R. Types and causes of medication errors from nurse’s viewpoint. Iran. J. Nurs. Midwifery Res. 2013, 18, 228–231. [Google Scholar] [PubMed]
- Tariq, R.A.; Vashisht, R.; Sinha, A.; Scherbak, Y. Medication Dispensing Errors and Prevention. 2018. Available online: https://europepmc.org/article/NBK/nbk519065#__NBK519065_dtls__ (accessed on 5 May 2022).
- Gebre, M.; Addisu, N.; Getahun, A.; Workye, J.; Gamachu, B.; Fekadu, G.; Tekle, T.; Wakuma, B.; Fetensa, G.; Mosisa, B.; et al. Medication errors among hospitalized adults in medical wards of nekemte specialized hospital, west ethiopia: A prospective observational study. Drug. Healthc. Patient Saf. 2021, 13, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Perven, N.; Razia, M.S.; Nesa, M.; Park, J.S. Knowledge regarding medication error among nurses at tertiary hospital. Int. Acad. J Adv. Pract. Nurs. 2020, 1, 9–15. [Google Scholar] [CrossRef]
- Alsulami, S.L.; Sardidi, H.O.; Almuzaini, R.S.; Alsaif, M.A.; Almuzaini, H.S.; Moukaddem, A.K.; Kharal, M.S. Knowledge, attitude and practice on medication error reporting among health practitioners in a tertiary care setting in Saudi Arabia. Saudi Med. J. 2019, 40, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Tella, S.A.; Logan, P.; Khakurel, J.; Vizcaya-Moreno, F. Nurses’ adherence to patient safety principles: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2028. [Google Scholar] [CrossRef] [Green Version]
- Ogunleye, O.O.; Oreagba, I.A.; Falade, C.; Isah, A.; Enwere, O.; Olayemi, S.; Ogundele, S.O.; Obiako, R.; Odesanya, R.; Bassi, P.; et al. Medication errors among health professionals in Nigeria: A national survey. Int. J. Risk Saf. Med. 2016, 28, 77–91. [Google Scholar] [CrossRef]
- Hammoudi, B.M.; Ismaile, S.; Abu Yahya, O. Factors associated with medication administration errors and why nurses fail to report them. Scand. J. Caring Sci. 2018, 32, 1038–1046. [Google Scholar] [CrossRef]
- Márquez-Hernández, V.V.; Fuentes- Colmenero, A.L.; Cañadas-Nuñez, F.; Di Muzio, M.; Giannetta, N.; Gutiérrez-Puertas, L. Factors related to medication errors in the preparation and administration of intravenous medication in the hospital environment. PLoS ONE 2019, 14, e0220001. [Google Scholar]
- Almalki, Z.S.; Alqahtani, N.; Salway, N.T.; Alharbi, M.M.; Alqahtani, A.; Alotaibi, N.; Alotaibi, T.M.; Alshammari, T. Evaluation of medication error rates in Saudi Arabia: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e24956. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, F.M.; Alanazi, E.J.; Alanazi, A.M.; Alturifi, A.K.; Alshammari, T.M. Medication error concept and reporting practices in saudi arabia: A multiregional study among healthcare professionals. Risk Manag. Healthc. Policy 2021, 14, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Al-Harkan, A.; Al-Harkan, N.; Al-Najjar, A.; Al-Hunti, A.; Al-Rashidi, A.; Al-Themery, A. Investigation of medication errors in a tertiary care hospitals in the Qassim region, Saudi Arabia. Open Access Maced. J. Med. Sci. 2020, 8, 209–212. [Google Scholar] [CrossRef]
- Alyami, M.H.; Naser, A.Y.; Alswar, H.S.; Alyami, H.S.; Alyami, A.H.; Al Sulayyim, H.J. Medication errors in Najran, Saudi Arabia: Reporting, responsibility, and characteristics: A cross-sectional study. Saudi Pharm. J. 2022, 30, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observa-tional studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Yung, H.P.; Yu, S.; Chu, C.; Hou, I.C.; Tang, F.I. Nurses’ attitudes and perceived barriers to the reporting of medication administration errors. J. Nurs. Manag. 2016, 24, 580–588. [Google Scholar] [CrossRef]
- Jose, J.; Rao, P.G. Pattern of adverse drug reactions notified by spontaneous reporting in an Indian tertiary care teaching hospital. Pharmacol Res. 2006, 54, 226–233. [Google Scholar] [CrossRef]
- Abdel-Latif, M.M. Knowledge of healthcare professionals about medication errors in hospitals. J. Basic Clin. Pharm. 2016, 7, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Altebainawi, A.; Aljofan, M.; Alrashidi, M.N.; Alshammari, T.M. Completeness of medication prescriptions: Prescription errors study in Hail region, Saudi Arabia (PeSHR). Int. J. Adv. Appl. Sci. 2019, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Mrayyan, M.T.; Shishani, K.; Al-faouri, I. Rate, causes and reporting of medication errors in Jordan: Nurses’ perspectives. J. Nurs. Manag. 2007, 15, 659–670. [Google Scholar] [CrossRef]
- Vazin, A.; Delfani, S. Medication errors in an internal intensive care unit of a large teaching hospital: A direct observation study. Acta. Med. Iran. 2012, 50, 425–432. [Google Scholar] [PubMed]
- Carandang, R.; Resuello, D.; Hocson, G.; Respicio, K.; Reynoso, C. Knowledge, attitude and practices on medication error reporting among health practitioners from Hospitals in Manila. Sch. Acad. J. Pharm. 2015, 4, 293–300. [Google Scholar]
- Teoh, B.; Alrasheedy, A.; Hassali, M.; Tew, M.; Samsudin, M. Perceptions of doctors and pharmacists towards medication error reporting and prevention in Kedah, Malaysia: A Rasch model analysis. Adv. Pharmacoepidemiol. Drug. Saf. 2015, 4, 1052–2167. [Google Scholar]
- Alsafi, E.; Baharoon, S.; Ahmed, A.; Al Jahdali, H.H.; Al Zahrani, S.; Al Sayyari, A. Physicians’ knowledge and practice towards medical error reporting: A cross-sectional hospital-based study in Saudi Arabia. E. Mediterr. Health J. 2015, 21, 655–664. [Google Scholar] [CrossRef]
- Samundeeswari, A.; Muthamilselvi, G. Nurses knowledge on prevention of medication error. J. Med. Sci. Clin. Res. 2018, 6, 274–296. [Google Scholar] [CrossRef]
- Al-saleh, K.S.; Ramadan, M.Z. Studying medical errors among hospital-staff at Saudi health providers. J. Mater. Sci. Eng. 2012, 2, 41–52. [Google Scholar]
- Lesar, T.S.; Briceland, L.; Stein, D.S. Factors related to errors in medica- tion prescribing. JAMA. 1997, 277, 312–317. [Google Scholar] [CrossRef]
- Shawahna, R.; Rahman, N.U.; Ahmad, M.; Debray, M.; Yliperttula, M.; Declèves, X. Impact of prescriber’s handwriting style and nurse’s duty duration on the prevalence of transcription errors in public hospitals. J. Clin. Nurs. 2013, 22, 550–558. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Frequency | Percentage (%) |
|---|---|---|
| Age, mean (SD) | 34.04 (3.98) | |
| <30 years old | 42 | 10.3 |
| 30–40 years old | 346 | 84.8 |
| >40 years old | 20 | 4.9 |
| Gender | ||
| Male | 127 | 31.1 |
| Female | 281 | 68.9 |
| Nationality | ||
| Saudi | 199 | 48.8 |
| Non-Saudi | 209 | 51.2 |
| Marital status | ||
| Single | 110 | 27.0 |
| Married | 243 | 59.6 |
| Divorced | 48 | 11.8 |
| Widower/Widow | 7 | 1.7 |
| Education level | ||
| College Diploma or Below | 45 | 11.0 |
| Bachelor Degree | 279 | 68.4 |
| Master Degree | 81 | 19.9 |
| Doctoral Degree | 3 | 0.7 |
| Monthly income (Saudi Riyal), mean (SD) | 8722.18 (3470.74) | |
| <10,000 | 261 | 64.0 |
| 10,000–15,000 | 127 | 31.1 |
| >15,000 | 20 | 4.9 |
| First language | ||
| Arabic | 233 | 57.1 |
| English | 18 | 4.4 |
| Other * | 157 | 38.5 |
| Religion | ||
| Muslim | 308 | 75.5 |
| Non-Muslim | 100 | 24.5 |
| Hospital | ||
| King Fahad Hospital | 180 | 44.1 |
| King Abdulaziz hospital | 86 | 21.1 |
| East Jeddah hospital | 71 | 17.4 |
| King Abdullah Medical Complex | 71 | 17.4 |
| Role/Profession | ||
| General Nurse | 103 | 25.2 |
| Assistant Nurse | 1 | 0.2 |
| Critical Care Nurse | 44 | 11 |
| Specialist Nurse | 259 | 63.5 |
| Department/Unit | ||
| Emergency room | 140 | 34.3 |
| Surgical Ward | 34 | 8.3 |
| Medical Ward | 53 | 13.0 |
| Intensive care unit | 130 | 31.9 |
| Others | 51 | 12.5 |
| Experience in years, mean (SD) | 9.44 (4.68) | |
| Less than 5 Years | 33 | 8.1 |
| 5–10 Years | 252 | 61.8 |
| More than 10 Years | 123 | 30.1 |
| Work weekly hours, mean (SD) | 51.83 (6.97) | |
| 40 h | 6 | 1.5 |
| >40 h | 402 | 98.5 |
| Attend training course on MER | ||
| Yes | 255 | 62.5 |
| No | 153 | 37.5 |
| No. | Items | Frequency | Percentage (%) | ||
|---|---|---|---|---|---|
| 1. | Which one of the following do you consider to be the MOST important when administering medication? | ||||
| (a). Right Patient | 402 | 98.5 | |||
| (b). Right dose | 3 | 0.7 | |||
| (c). Right route | 0 | 0 | |||
| (d). Right time | 1 | 0.2 | |||
| (e). Right medication | 2 | 0.5 | |||
| 2. | Which one of the following do you consider to be the LEAST important when administering medication? | ||||
| (a). Right Patient | 1 | 0.2 | |||
| (b). Right dose | 9 | 2.2 | |||
| (c). Right route | 65 | 15.9 | |||
| (d). Right time | 328 | 80.4 | |||
| (e). Right medication | 5 | 1.2 | |||
| 3. | The most common preventable adverse events were related to: | ||||
| (a). Culture of Safety | 60 | 14.7 | |||
| (b). Medications | 126 | 30.9 | |||
| (c). Administrative oversight | 133 | 32.6 | |||
| (d). Poor communication | 89 | 21.8 | |||
| 4. | Most medication administration errors go unreported because: | ||||
| (a). The nurse is unaware an error has occurred. | 151 | 37.0 | |||
| (b). They did not harm the patient. | 28 | 6.9 | |||
| (c). Adverse event reporting systems are not designed to capture these data. | 216 | 52.9 | |||
| (d). The nurse is embarrassed and avoids reporting. | 13 | 3.2 | |||
| 5. | The use of direct observation for medication administration accuracy assessment is: | ||||
| (a). Not as reliable as adverse event reporting systems. | 16 | 3.9 | |||
| (b). More reliable than adverse event reporting systems, when combined with medical record review. | 310 | 76.0 | |||
| (c). Strictly a research method. | 65 | 15.9 | |||
| (d). None of the above. | 17 | 4.2 | |||
| 6. | The medication administration accuracy assessment includes: | ||||
| (a). Systematic observation of six selected fundamental practices performed by the nurse during preparation, administration, and documentation of medications. | 40 | 9.8 | |||
| (b). Review of the medical record to extract relevant medication orders. | 30 | 7.4 | |||
| (c). Comparison of medications administered and medications ordered to determine medication administration accuracy. | 123 | 30.1 | |||
| (d). All the above. | 215 | 52.7 | |||
| 7. | Which of the following is not one of the six safe practices observed in the medication administration accuracy assessment? | ||||
| (a). The nurse compared the medication with the medication administration record. | 34 | 8.3 | |||
| (b). The nurse ensured the medication was labeled throughout the process from preparation to administration. | 50 | 12.3 | |||
| (c). The nurse asked the patient to verify the purpose of the medication. | 301 | 73.8 | |||
| (d). The nurse charted/documented medication administration immediately after completion. | 23 | 5.6 | |||
| No. | Items | True n (%) | False n (%) | I don’t know n (%) | |
| 8. | Based on your experience as a nurse, what do you consider to be the contributing factors to medication errors? | ||||
| a. Interruptions during medication rounds | 364 (89.2) | 36 (8.8) | 8 (2.0) | ||
| b. Lack of familiarity with medications | 363 (89.0) | 43 (10.5) | 2 (0.5) | ||
| c. Lack of supervision for inexperienced staff | 357 (87.5) | 49 (12.0) | 2 (0.5) | ||
| d. Inadequate initial nurse training | 364 (89.2) | 42 (10.3) | 2 (0.5) | ||
| e. Poor quality control and management | 357 (87.5) | 45 (11.0) | 6 (1.5) | ||
| f. High workload | 362 (88.7) | 39 (9.6) | 7 (1.7) | ||
| g. Lack of medication skills competence by nurses | 352 (86.3) | 43 (10.5) | 13 (3.2) | ||
| h. High patient-to-nurse ratio onwards/units | 359 (88.0) | 35 (8.6) | 14 (3.4) | ||
| i. High levels of patient need | 362 (88.7) | 37 (9.1) | 9 (2.2) | ||
| j. ‘8 rights’ not followed (“five rights”: the right patient, the right drug, the right dose, the right route, the right time, the right documentation, the right reason, and the right response). | 356 (87.3) | 45 (11.0) | 7 (1.7) | ||
| k. Unclear verbal instructions between doctors and nurses | 350 (85.8) | 49 (12.0) | 9 (2.2) | ||
| l. Poor handwriting by the doctor | 346 (84.8) | 47 (11.5) | 15 (3.7) | ||
| m. Drugs that look alike or have similar sounding names | 348 (85.3) | 52 (12.7) | 8 (2.0) | ||
| 9. | Based on your experience as a nurse, which of the following sentence is correct? | ||||
| a. Forgetting to administer medication on time is an example of unethical behavior. | 128 (31.4) | 268 (65.7) | 12 (2.9) | ||
| b. The FIRST thing you should do if you make a medication error is to watch the individual closely. | 124 (30.4) | 282 (69.1) | 2 (0.5) | ||
| c. Medication errors must be documented only in a medication error report form. | 136 (33.3) | 264 (64.7) | 8 (2.0) | ||
| d. ALL medication may be crushed. | 101 (24.8) | 299 (73.3) | 8 (2.0) | ||
| e. You should sign off on the medication that you administer before successfully administering the medication. | 178 (43.6) | 228 (55.9) | 2 (0.5) | ||
| f. You should refuse to give the medications that your colleague prepared. | 234 (57.4) | 165 (40.4) | 9 (2.2) | ||
| g. You should erase or “white out” the error if you accidentally mark the Medication Administration Record (MAR) for medication for the wrong time of the day. | 141 (34.6) | 256 (62.7) | 11 (2.7) | ||
| h. You should complete a medication error form before the end of the shift if you discover I did not make the error after informing the charge nurse. | 135 (33.1) | 261 (64.0) | 12 (2.9) | ||
| No. | Statement | Scale | ||||
|---|---|---|---|---|---|---|
| Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree | ||
| 1 | 2 | 3 | 4 | 5 | ||
| 1. | I would rather not report a medication error than being blamed when I report it | 107 (26.2) | 78 (19.1) | 5 (1.2) | 78 (19.1) | 140 (34.3) |
| 2. | I would rather not report a medication error than risk being labeled a troublemaker | 107 (26.2) | 71 (17.4) | 6 (1.5) | 100 (24.5) | 124 (30.4) |
| 3. | I would rather not report a medication error for fear of my manager’s reaction | 130 (31.9) | 58 (14.2) | 7 (1.7) | 99 (24.3) | 114 (27.9) |
| 4. | I would rather not report a medication error than look incompetent in front of my coworkers | 131 (32.1) | 57 (14.0) | 7 (1.7) | 102 (25.0) | 111 (27.2) |
| 5. | I fear punitive action or retribution | 125 (30.6) | 69 (16.9) | 7 (1.7) | 96 (23.5) | 111 (27.2) |
| 6. | I fear judicial issues | 133 (32.6) | 57 (14.0) | 5 (1.2) | 103 (25.2) | 110 (27.0) |
| 7. | I fear malpractice suits | 123 (30.1) | 52 (12.7) | 6 (1.5) | 111 (27.2) | 116 (28.4) |
| 8. | I fear media exposure in public | 115 (28.2) | 43 (10.5) | 5 (1.2) | 121 (29.7) | 124 (30.4) |
| 9. | I believe reporting medication errors makes patients or their families develop negative attitudes toward my profession | 72 (17.6) | 37 (9.1) | 9 (2.2) | 115 (28.2) | 175 (42.9) |
| 10. | I believe reporting a medication error could cost me my professional registration | 106 (26.0) | 45 (11.0) | 6 (1.5) | 128 (31.4) | 123 (30.1) |
| 11. | I believe reporting a medication error could cost me my honor and dignity | 132 (32.4) | 47 (11.5) | 4 (1.0) | 107 (26.2) | 118 (28.9) |
| 12. | I believe reporting a medication error could cost me my job | 96 (23.5) | 47 (11.5) | 11 (2.7) | 113 (27.7) | 141 (34.6) |
| 13. | I believe some nurses do not report errors because they fear punishment | 53 (13.0) | 27 (6.6) | 8 (2.0) | 118 (28.9) | 202 (49.5) |
| 14. | I believe some nurses do not report errors because of different cultural views about what constitutes an error | 41 (10.0) | 23 (5.6) | 6 (1.5) | 109 (26.7) | 229 (56.1) |
| 15. | I believe sanctions against nurses should be proportionate to the consequences of the error and whether the nurse has self-reported | 46 (11.3) | 35 (8.6) | 7 (1.7) | 114 (27.9) | 206 (50.5) |
| 16. | I believe in some circumstances it is better to ignore a medication error | 102 (25.0) | 37 (9.1) | 5 (1.2) | 107 (26.2) | 157 (38.5) |
| 17. | I believe most of medication errors are inevitable and non-avoidable | 67 (16.4) | 37 (9.1) | 7 (1.7) | 101 (24.8) | 196 (48.0) |
| 18. | I believe educational interventions and training courses can reduce medication errors and consciously approach with adverse drug events. | 17 (4.2) | 17 (4.2) | 6 (1.5) | 116 (28.4) | 252 (61.8) |
| 19. | I believe more studies and the use of modern methods for drugs information are essential for increasing scientific and practical skills | 17 (4.2) | 14 (3.4) | 5 (1.2) | 126 (30.9) | 246 (60.3) |
| 20. | I believe the use of bar-coding technology on medication labels can reduce medication errors | 13 (3.2) | 13 (3.2) | 5 (1.2) | 102 (25.0) | 275 (67.4) |
| 21. | I believe the use of dispensing technology can reduce medication errors | 15 (3.7) | 12 (2.9) | 4 (1.0) | 106 (26.0) | 271 (66.4) |
| 22. | I believe it is important to report medication errors even whether or not harm to the patient may occur | 22 (5.4) | 20 (4.9) | 5 (1.2) | 88 (21.6) | 273 (66.9) |
| 23. | I believe that patients and families have a right to be told about medication errors and whether or not harm to the patient may occur | 34 (8.3) | 17 (4.2) | 7 (1.7) | 53 (13.0) | 297 (72.8) |
| Variables | Frequency | Percentage (%) |
|---|---|---|
| Total Knowledge | ||
| Median (IQR) | 22 (6) | |
| Min-Max | 8–28 | |
| Poor | 184 | 45.1 |
| Good | 224 | 54.9 |
| Total Attitude | ||
| Median (IQR) | 69 (34) | |
| Min-Max | 51–115 | |
| Negative | 204 | 50 |
| Positive | 204 | 50 |
| Variables | Medication Error | χ2 | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| n (%) | n (%) | |||
| Age | ||||
| <25 years old | 37 (88.1%) | 5 (11.9%) | 15.575 | <0.001 * |
| 25–35 years old | 249 (72.0%) | 97 (28.0%) | ||
| >35 years old | 8 (40.0%) | 12 (60.0%) | ||
| Gender | ||||
| Male | 91 (71.7%) | 36 (28.3%) | 0.015 | 0.903 |
| Female | 203 (72.2%) | 78 (27.8%) | ||
| Nationality | ||||
| Saudi | 147 (73.9%) | 52 (26.1%) | 0.632 | 0.427 |
| Non-Saudi | 147 (70.3%) | 62 (29.7%) | ||
| Marital status | ||||
| Single | 81 (73.6%) | 29 (26.4%) | 2.913 | 0.668 |
| Married | 169 (69.5%) | 74 (30.5%) | ||
| Divorced | 39 (81.3%) | 9 (18.8%) | ||
| Widower/Widow | 5 (71.4%) | 2 (28.6%) | ||
| Education level | ||||
| College Diploma or Below | 36 (80.0%) | 9 (20.0%) | 9.910 | 0.030 * |
| Bachelor Degree | 203 (72.8%) | 76 (27.2%) | ||
| Master Degree | 55 (67.9%) | 26 (32.1%) | ||
| Doctoral Degree | 0 (0.0%) | 3 (100.0%) | ||
| Monthly income | ||||
| <10,000 | 187 (71.6%) | 74 (28.4%) | 12.422 | 0.313 |
| 10,000–15,000 | 99 (78.0%) | 28 (22.0%) | ||
| >15,000 | 8 (40.0%) | 12 (60.0%) | ||
| First language | ||||
| Arabic | 167 (71.7%) | 66 (28.3%) | 2.693 | 0.887 |
| English | 16 (88.9%) | 2 (11.1%) | ||
| Other | 111 (70.7%) | 46 (29.3%) | ||
| Religion | ||||
| Muslim | 224 (72.7%) | 84 (27.3%) | 0.279 | 0.609 |
| Non-Muslim | 70 (70.0%) | 30 (30.0%) | ||
| Hospital | ||||
| King Fahad Hospital | 173 (96.1%) | 7 (3.9%) | 188.13 | <0.001 * |
| King Abdulaziz hospital | 76 (88.4%) | 10 (11.6%) | ||
| East Jeddah hospital | 31 (43.7%) | 40 (56.3%) | ||
| King Abdullah Medical Complex | 14 (19.7%) | 57 (80.3%) | ||
| Role/Profession | ||||
| General Nurse | 94 (91.3%) | 9 (8.7%) | 27.421 | <0.001 *,a |
| Critical Care Nurse | 1 (100.0%) | 0 (0.0%) | ||
| Specialist Nurse | 26 (59.1%) | 18 (40.9%) | ||
| Others | 172 (66.4%) | 87 (33.6%) | ||
| Department/Unit | ||||
| Emergency room (ER) | 116 (82.9%) | 24 (17.1%) | 21.991 | <0.001 * |
| Surgical Ward | 24 (70.6%) | 10 (29.4%) | ||
| Medical Ward | 33 (62.3%) | 20 (37.7%) | ||
| Intensive care unit (ICU) | 95 (73.1%) | 35 (26.9%) | ||
| Others | 26 (51.0%) | 25 (49.0%) | ||
| Experience in year | ||||
| Less than 5 Years | 27 (81.8%) | 6 (18.2%) | 20.261 | <0.001 * |
| 5–10 Years | 197 (78.2%) | 55 (21.8%) | ||
| More than 10 Years | 70 (56.9%) | 53 (43.1%) | ||
| Work weekly hours | ||||
| 40 h | 4 (66.7%) | 2 (33.3%) | 0.088 | 0.673 a |
| >40 h | 290 (72.1%) | 112 (27.9%) | ||
| Attend training course on MER | ||||
| Yes | 155 (60.8%) | 100 (39.2%) | 42.931 | <0.001 * |
| No | 139 (90.8%) | 14 (9.2%) | ||
| Knowledge | ||||
| Good | 134 (59.8%) | 90 (40.2%) | 36.943 | <0.001 * |
| Poor | 160 (87.0%) | 24 (13.0%) | ||
| Attitude | ||||
| Positive | 101 (49.5%) | 103 (50.5%) | 103.035 | <0.001 * |
| Negative | 193 (94.6%) | 11 (5.4%) | ||
| B a | S.E b | Wald | df c | p-Value | OR d | 95% CI for OR e | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Age group | ||||||||
| <25 years old | −5.080 | 1.427 | 12.674 | 1 | <0.0001 * | 0.006 | 0.000 | 0.102 |
| 25–35 years old | −3.030 | 0.972 | 9.708 | 1 | 0.002 * | 0.048 | 0.007 | 0.325 |
| [>35 years old] | 1 | |||||||
| Gender | ||||||||
| [Male] | 1 | |||||||
| female | −0.368 | 0.523 | 0.496 | 1 | 0.481 | 0.692 | 0.248 | 1.928 |
| Nationality | ||||||||
| Saudi | 1.251 | 0.842 | 2.205 | 1 | 0.138 | 3.493 | 0.670 | 18.205 |
| [Non-Saudi] | 1 | |||||||
| Monthly income | ||||||||
| <10,000 | 0.850 | 1.187 | 0.513 | 1 | 0.474 | 2.340 | 0.229 | 23.952 |
| 10,000–15,000 | 0.049 | 1.062 | 0.002 | 1 | 0.964 | 1.050 | 0.131 | 8.415 |
| [>15,000] | 1 | |||||||
| Hospital | ||||||||
| King Fahad Hospital | −4.390 | 0.715 | 37.745 | 1 | 0.0001 * | 0.012 | 0.003 | 0.050 |
| King Abdulaziz hospital | −4.187 | 0.710 | 34.755 | 1 | 0.0001 * | 0.015 | 0.004 | 0.061 |
| East Jeddah hospital | −1.050 | 0.545 | 3.709 | 1 | 0.054 | 0.350 | 0.120 | 1.019 |
| [King Abdullah Medical Complex] | 1 | |||||||
| Role/Profession | ||||||||
| General Nurse | −1.098 | 0.706 | 2.419 | 1 | 0.120 | 0.333 | 0.084 | 1.331 |
| Critical Care Nurse | −1.025 | 401.97 | 0.000 | 1 | 1.000 | 0.001 | 0.001 | 1.200 |
| Specialist Nurse | −0.528 | 0.0635 | 0.0690 | 1 | 0.406 | 0.590 | 0.170 | 2.049 |
| [Others] | 1 | |||||||
| Department/Unit | ||||||||
| Emergency room | 0.603 | 0.634 | 0.903 | 1 | 0.342 | 1.827 | 0.527 | 6.337 |
| Surgical Ward | 1.414 | 0.883 | 2.561 | 1 | 0.110 | 4.110 | 0.728 | 23.211 |
| Medical Ward | 0.290 | 0.774 | 0.140 | 1 | 0.708 | 1.336 | 0.293 | 6.093 |
| Intensive care unit | 1.139 | 0.592 | 3.695 | 1 | 0.055 | 3.123 | 0.978 | 9.975 |
| [Others] | 1 | |||||||
| Experience in year | ||||||||
| Less than 5 Years | 0.971 | 1.251 | 0.603 | 1 | 0.438 | 2.641 | 0.228 | 30.643 |
| 5–10 Years | −0.455 | 0.482 | 0.891 | 1 | 0.345 | 0.634 | 0.246 | 1.633 |
| [More than 10 Years] | 1 | |||||||
| Attend training course on MER | ||||||||
| [Yes] | 1 | |||||||
| No | −1.985 | 0.475 | 17.463 | 1 | 0.0001 * | 7.29 | 2.86 | 18.51 |
| Knowledge | ||||||||
| [Good] | 1 | |||||||
| Poor | −1.516 | 0.491 | 9.550 | 1 | 0.002 * | 4.54 | 1.74 | 11.90 |
| Attitude | ||||||||
| [Positive] | 1 | |||||||
| Negative | −2.651 | 0.563 | 22.195 | 1 | 0.0001 * | 14.08 | 4.69 | 43.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alandajani, A.; Khalid, B.; Ng, Y.G.; Banakhar, M. Knowledge and Attitudes Regarding Medication Errors among Nurses: A Cross-Sectional Study in Major Jeddah Hospitals. Nurs. Rep. 2022, 12, 1023-1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12040098
Alandajani A, Khalid B, Ng YG, Banakhar M. Knowledge and Attitudes Regarding Medication Errors among Nurses: A Cross-Sectional Study in Major Jeddah Hospitals. Nursing Reports. 2022; 12(4):1023-1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12040098
Chicago/Turabian StyleAlandajani, Alham, Bahariah Khalid, Yee Guan Ng, and Maram Banakhar. 2022. "Knowledge and Attitudes Regarding Medication Errors among Nurses: A Cross-Sectional Study in Major Jeddah Hospitals" Nursing Reports 12, no. 4: 1023-1039. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep12040098