
The Impact of Transformational Leadership in the Nursing Work Environment and Patients’ Outcomes: A Systematic Review

 , and
, and
Abstract
:1. Introduction
1.1. Rational
1.2. Objective and Research Question
2. Methodology
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection of Studies Process
2.4. Data Collection Process
2.5. Synthesis Methods
3. Results
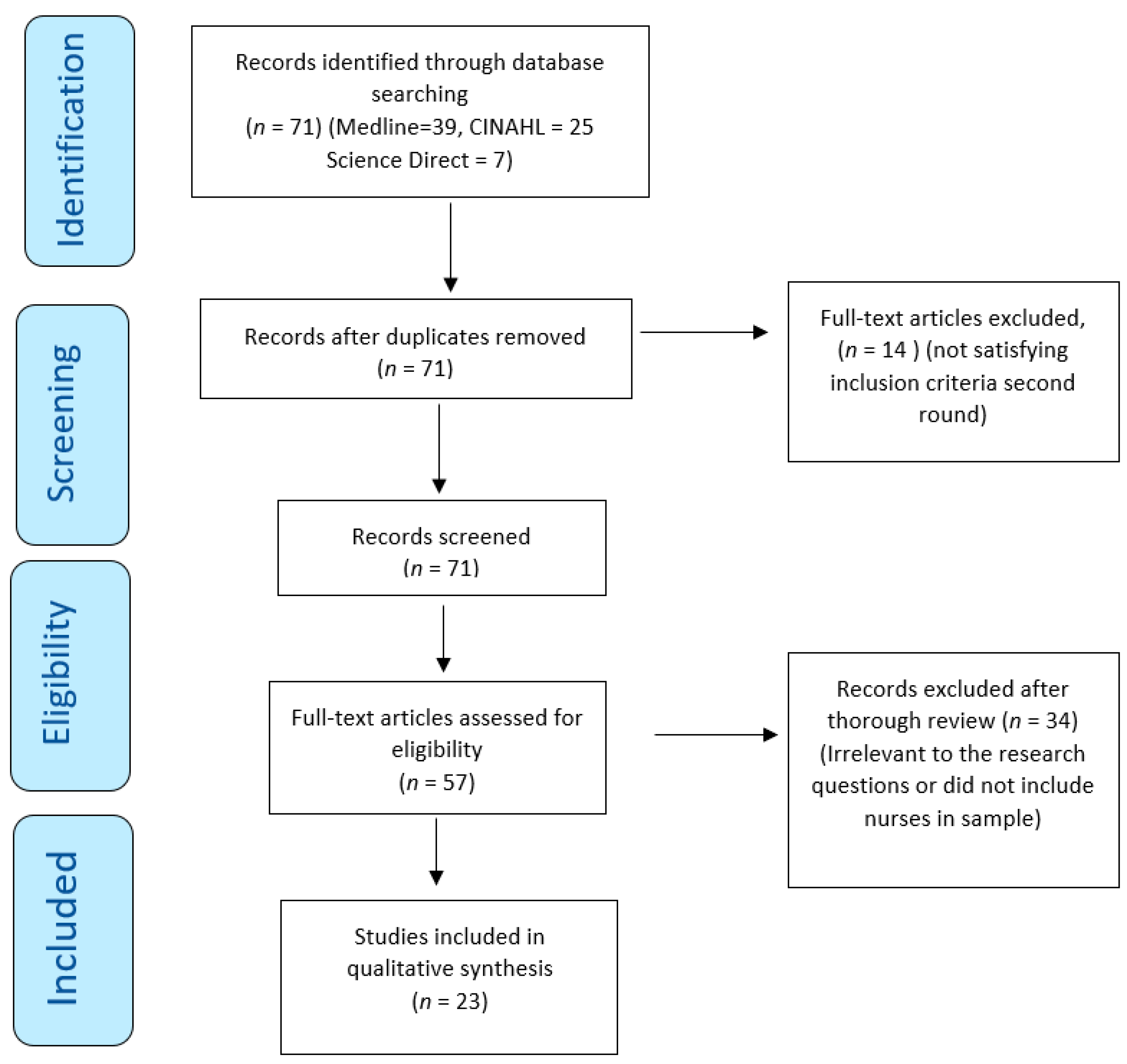
3.1. Studies Selection
3.2. Studies Characteristics
3.3. Study Assessment
3.4. Results of Synthesis
- Job Satisfaction and Organizational Commitment;
- Reduce Nurse Retention;
- Nurses’ Empowerment and Autonomy;
- Nurses’ Compliance with Safety Measures.
- Patient Safety Culture;
- Reporting Adverse Events.
3.4.1. Job Satisfaction and Organizational Commitment
3.4.2. Reducing Intention to Leave the Job/Organization
3.4.3. Nurses’ Empowerment and Autonomy
3.4.4. Nurses’ Compliance with Safety Measures
3.4.5. Increase Patient Safety Culture
3.4.6. Reporting Adverse Events
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
Appendix A

{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported (Page Number) |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 3 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 3 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 4 |
| Information sources | 6 | Specify all databases, registers, websites, organizations, reference lists, and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 4 |
| Search strategy | 7 | Present the full search strategies for all databases, registers, and websites, including any filters and limits used. | 4 |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and, if applicable, details of automation tools used in the process. | 5 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and, if applicable, details of automation tools used in the process. | 5 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and, if not, the methods used to decide which results to collect. | N/A |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | N/A | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and, if applicable, details of automation tools used in the process. | 7 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | N/A |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | 20 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling missing summary statistics or data conversions. | N/A | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | N/A | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | N/A | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | N/A | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | N/A | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | N/A |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | N/A |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | 6 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | 6 | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | 7 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | N/A |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | N/A |
| Results of syntheses | 20a | For each synthesis, briefly summarize the characteristics and risk of bias among contributing studies. | N/A |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | N/A | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | 20–25 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | 20–25 | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | N/A |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | 20–25 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 25–26 |
| 23b | Discuss any limitations of the evidence included in the review. | 25–26 | |
| 23c | Discuss any limitations of the review processes used. | 25–26 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | 25–26 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | N/A |
| 24b | Indicate where the review protocol can be accessed or state that a protocol was not prepared. | N/A | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | N/A | |
| Support | 25 | Describe sources of financial or non-financial support for the review and the role of the funders or sponsors in the review. | 27 |
| Competing interests | 26 | Declare any competing interests of review authors. | 27 |
| Availability of data, code, and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | 31 |
References
- Panagioti, M.; Khan, K.; Keers, R.N.; Abuzour, A.S.; Phipps, D.; Kontopantelis, E.; Bower, P.; Campbell, S.; Haneef, R.; Avery, A.J.; et al. Prevalence, severity, and nature of preventable patient harm across medical care settings: Systematic review and meta-analysis. BMJ 2019, 366, l4185. [Google Scholar] [CrossRef] [PubMed]
- Ree, E.; Wiig, S. Employees’ perceptions of patient safety culture in Norwegian nursing homes and home care services. BMC Health Serv. Res. 2019, 19, 607. [Google Scholar] [CrossRef] [PubMed]
- Cummings, G.G.; MacGregor, T.; Davey, M.; Lee, H.; Wong, C.A.; Lo, E.; Muise, M.; Stafford, E. Leadership styles and outcome patterns for the nursing workforce and work environment: A systematic review. Int. J. Nurs. Stud. 2010, 47, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Alves, P.C.; Oliveira, A.D.F.; Paro, H. Quality of life and burnout among faculty members: How much does the field of knowledge matter? PLoS ONE 2019, 14, e0214217. [Google Scholar] [CrossRef]
- Maben, J.; Conolly, A.; Abrams, R.; Rowland, E.; Harris, R.; Kelly, D.; Kent, B.; Couper, K. “You can’t walk through water without getting wet” UK nurses’ distress and psychological health needs during the COVID-19 pandemic: A longitudinal in-terview study. Int. J. Nurs. Stud. 2022, 131, 104242. [Google Scholar] [CrossRef]
- Kim, M.-N.; Yoo, Y.-S.; Cho, O.-H.; Hwang, K.-H. Emotional Labor and Burnout of Public Health Nurses during the COVID-19 Pandemic: Mediating Effects of Perceived Health Status and Perceived Organizational Support. Int. J. Environ. Res. Public Health 2022, 19, 549. [Google Scholar] [CrossRef]
- Fahmy, A.M.; Saber, E.H.; Gabra, S.F. Relation between Compassion Fatigue, Pandemic Emotional Impact, and Time Management among Nurses at Isolation Hospitals during COVID-19. Minia Sci. Nurs. J. 2022, 012, 57–68. [Google Scholar] [CrossRef]
- Shivairová, O.; Bártlová, S.; Hellerová, V.; Chloubová, I. Nurseʼs mental health during COVID-19 pandemic. Cent. Eur. J. Nurs. Midwifery 2023, 14, 795–804. [Google Scholar] [CrossRef]
- Asif, M.; Jameel, A.; Hussain, A.; Hwang, J.; Sahito, N. Linking Transformational Leadership with Nurse-Assessed Adverse Patient Outcomes and the Quality of Care: Assessing the Role of Job Satisfaction and Structural Empowerment. Int. J. Environ. Res. Public Health 2019, 16, 2381. [Google Scholar] [CrossRef]
- Labrague, L.J. Influence of nurse managers’ toxic leadership behaviours on nurse-reported adverse events and quality of care. J. Nurs. Manag. 2020, 29, 855–863. [Google Scholar] [CrossRef]
- Farokhzadian, J.; Nayeri, N.D.; Borhani, F. The long way ahead to achieve an effective patient safety culture: Challenges perceived by nurses. BMC Health Serv. Res. 2018, 18, 654. [Google Scholar] [CrossRef] [PubMed]
- Pronovost, P.J.; Cleeman, J.I.; Wright, D.; Srinivasan, A. Fifteen years after To Err is Human: A success story to learn from: Table 1. BMJ Qual. Saf. 2015, 25, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, J.; Cope, V.; Baum, G. Postgraduate nurses’ insights into the nursing leadership role. Do they intuitively link the role to patient safety? J. Nurs. Educ. Pract. 2015, 5, 72–77. [Google Scholar] [CrossRef]
- Murray, M.; Sundin, D.; Cope, V. The nexus of nursing leadership and a culture of safer patient care. J. Clin. Nurs. 2017, 27, 1287–1293. [Google Scholar] [CrossRef]
- Suratno, K. The relationship between transformational leadership and quality of nursing work life in hospital. Int. J. Caring Sci. 2018, 11, 1416–1422. [Google Scholar]
- Gottlieb, L.N.; Gottlieb, B.; Bitzas, V. Creating Empowering Conditions for Nurses with Workplace Autonomy and Agency: How Healthcare Leaders Could Be Guided by Strengths-Based Nursing and Healthcare Leadership (SBNH-L). J. Healthc. Leadersh. 2021, 13, 169–181. [Google Scholar] [CrossRef]
- Wong, C.A.; Cummings, G.G.; Ducharme, L. The relationship between nursing leadership and patient outcomes: A systematic review update. J. Nurs. Manag. 2013, 21, 709–724. [Google Scholar] [CrossRef]
- Weberg, D.R.; Davidson, S. Leadership for Evidence-Based Innovation in Nursing and Health Professions, 2nd ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2022. [Google Scholar]
- Schein, H.; Schein, P.A. Organizational Culture and Leadership, 5th ed.; Wiley: Hoboken, NJ, USA, 2016. [Google Scholar]
- Bass, B.M.; Riggio, R.E. Transformational Leadership; Psychology Press: London, UK, 2006. [Google Scholar] [CrossRef]
- Bass, B.M. Theory of transformational leadership redux. Leadersh. Q. 1996, 6, 463–478. [Google Scholar] [CrossRef]
- Bass, B.M.; Avolio, B.J.; Jung, D.I.; Berson, Y. Predicting unit performance by assessing transformational and transactional leadership. J. Appl. Psychol. 2003, 88, 207–218. [Google Scholar] [CrossRef]
- Lu, Q.; Liu, Y.; Huang, X. Follower Dependence, Independence, or Interdependence: A Multi-Foci Framework to Unpack the Mystery of Transformational Leadership Effects. Int. J. Environ. Res. Public Health 2020, 17, 4534. [Google Scholar] [CrossRef]
- Hutchinson, M.; Jackson, D. Transformational leadership in nursing: Towards a more critical interpretation. Nurs. Inq. 2012, 20, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Mikkonen, K.; Kääriäinen, M. Content Analysis in Systematic Reviews. In The Application of Content Analysis in Nursing Science Research; Kyngäs, H., Mikkonen, K., Kääriäinen, M., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Zhang, Y.; Wildemuth, B.M. Qualitative analysis of content. In Applications of Social Research Methods to Questions in Information and Library Science; Wildemuth, B., Ed.; Libraries Unlimited: Westport, CT, USA, 2009; pp. 308–319. [Google Scholar]
- Dekkers, O.M.; Vandenbroucke, J.P.; Cevallos, M.; Renehan, A.G.; Altman, D.G.; Egger, M. COSMOS-E: Guidance on conducting systematic reviews and meta-analyses of observational studies of etiology. PLoS Med. 2019, 16, e1002742. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-Y.; MacLennan, S.; Hunt, N.; Cox, T. The influences of nursing transformational leadership style on the quality of nurses’ working lives in Taiwan: A cross-sectional quantitative study. BMC Nurs. 2015, 14, 33. [Google Scholar] [CrossRef]
- Choi, S.L.; Goh, C.F.; Adam, M.B.H.; Tan, O.K. Transformational leadership, empowerment, and job satisfaction: The mediating role of employee empowerment. Hum. Resour. Health 2016, 14, 73. [Google Scholar] [CrossRef]
- Wu, X.; Hayter, M.; Lee, A.J.; Yuan, Y.; Li, S.; Bi, Y.; Zhang, L.; Cao, C.; Gong, W.; Zhang, Y. Positive spiritual climate supports transformational leadership as means to reduce nursing burnout and intent to leave. J. Nurs. Manag. 2020, 28, 804–813. [Google Scholar] [CrossRef]
- Boamah, S.A.; Laschinger, H.K.S.; Wong, C.; Clarke, S. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs. Outlook 2018, 66, 180–189. [Google Scholar] [CrossRef]
- Xie, Y.; Gu, D.; Liang, C.; Zhao, S.; Ma, Y. How transformational leadership and clan culture influence nursing staff’s willingness to stay. J. Nurs. Manag. 2020, 28, 1515–1524. [Google Scholar] [CrossRef]
- Wagner, A.; on behalf of the WorkSafeMed Consortium; Rieger, M.A.; Manser, T.; Sturm, H.; Hardt, J.; Martus, P.; Lessing, C.; Hammer, A. Healthcare professionals’ perspectives on working conditions, leadership, and safety climate: A cross-sectional study. BMC Health Serv. Res. 2019, 19, 53. [Google Scholar] [CrossRef]
- Brewer, C.S.; Kovner, C.T.; Djukic, M.; Fatehi, F.; Greene, W.; Chacko, T.P.; Yang, Y. Impact of transformational leadership on nurse work outcomes. J. Adv. Nurs. 2016, 72, 2879–2893. [Google Scholar] [CrossRef]
- Asiri, S.A.; Rohrer, W.W.; Al-Surimi, K.; Da’ar, O.O.; Ahmed, A. The association of leadership styles and empowerment with nurses’ organizational commitment in an acute health care setting: A cross-sectional study. BMC Nurs. 2016, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Boamah, S.A. The impact of transformational leadership on nurse faculty satisfaction and burnout during the COVID-19 pandemic: A moderated mediated analysis. J. Adv. Nurs. 2022, 78, 2815–2826. [Google Scholar] [CrossRef] [PubMed]
- El-Demerdash, A.M.S.; Elhosany, W.A.; Hefny, M.A.M. Professional Forces of Magnetism and Patient Safety Culture at Suez Canal University Hospitals. Int. J. Nurs. Didact. 2018, 8, 10–18. [Google Scholar] [CrossRef]
- Weng, R.-H.; Huang, C.-Y.; Chen, L.-M.; Chang, L.-Y. Exploring the impact of transformational leadership on nurse innovation behaviour: A cross-sectional study. J. Nurs. Manag. 2013, 23, 427–439. [Google Scholar] [CrossRef]
- Khan, B.P.; Griffin, M.T.Q.; Fitzpatrick, J.J. Staff Nurses’ Perceptions of Their Nurse Managers’ Transformational Leadership Behaviors and Their Own Structural Empowerment. JONA J. Nurs. Adm. 2018, 48, 609–614. [Google Scholar] [CrossRef]
- Lievens, I.; Vlerick, P. Transformational leadership and safety performance among nurses: The mediating role of knowledge-related job characteristics. J. Adv. Nurs. 2013, 70, 651–661. [Google Scholar] [CrossRef]
- Seljemo, C.; Viksveen, P.; Ree, E. The role of transformational leadership, job demands and job resources for patient safety culture in Norwegian nursing homes: A cross-sectional study. BMC Health Serv. Res. 2020, 20, 799. [Google Scholar] [CrossRef]
- Kvist, T.; Mäntynen, R.; Turunen, H.; Partanen, P.; Miettinen, M.; Wolf, G.A.; Vehviläinen-Julkunen, K. How magnetic are Finnish hospitals measured by transformational leadership and empirical quality outcomes? J. Nurs. Manag. 2012, 21, 152–164. [Google Scholar] [CrossRef]
- Yilmaz, A.; Duygulu, S. The Relationship Between Charge Nurses and Clinical Nurses’ Perceptions of Patient Safety Culture and Leadership Practices. Dokuz Eylül Üniversitesi Hemşirelik Fakültesi Elektron. Derg. 2021, 14, 29–37. [Google Scholar] [CrossRef]
- Anselmann, V.; Mulder, R.H. Transformational leadership, knowledge sharing and reflection, and work teams’ performance: A structural equation modelling analysis. J. Nurs. Manag. 2020, 28, 1627–1634. [Google Scholar] [CrossRef]
- Lappalainen, M.; Härkänen, M.; Kvist, T. The relationship between nurse manager’s transformational leadership style and medication safety. Scand. J. Caring Sci. 2019, 34, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, S.F.; Mohammadi, T.K.; Adib, M.; Lili, E.K.; Soodmand, M. Barriers to nurses reporting errors and adverse events. Br. J. Nurs. 2019, 28, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Alfadhalah, T.; Elamir, H. Patient safety and leadership style in the government general hospitals in Kuwait: A multi-method study. Leadersh. Health Serv. 2021, 35, 190–209. [Google Scholar] [CrossRef]
- Tekingündüz, S.; Yıldız, E.; İnci, R. Relationships Between Nurses’ Perceptions of Patient Safety Culture and Job Stress, Trust, Identification, and Leadership. Leadership 2021, 8, 344–354. [Google Scholar] [CrossRef]
- Liukka, M.; Hupli, M.; Turunen, H. How transformational leadership appears in action with adverse events? A study for Finnish nurse manager. J. Nurs. Manag. 2017, 26, 639–646. [Google Scholar] [CrossRef]
- Merrill, K.C. Leadership Style and Patient Safety. JONA J. Nurs. Adm. 2015, 45, 319–324. [Google Scholar] [CrossRef]
- Burns, K.E.A.; Pattani, R.; Lorens, E.; Straus, S.E.; Hawker, G.A. The impact of organizational culture on professional fulfillment and burnout in an academic department of medicine. PLoS ONE 2021, 16, e0252778. [Google Scholar] [CrossRef]
- Murray, M.; Cope, V. Leadership: Patient safety depends on it! Collegian 2021, 28, 604–609. [Google Scholar] [CrossRef]
- O’connor, S.; Carlson, E. Safety Culture and Senior Leadership Behavior. JONA J. Nurs. Adm. 2016, 46, 215–220. [Google Scholar] [CrossRef]

| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Peer Reviewed | The sample does not include nurses |
| Primary sources | Secondary sources |
| Include nurses in the study sample | Not written in the English Language |
| Written in English | Published earlier than 2012 |
| Published between 2012 and 2022 (to capture a broad range of research on our topic within the last decade) |
| Population | Interest | Context | ||
|---|---|---|---|---|
| (TL (“Registered Nurse” OR “RN” OR “Nurs * p *” OR “Nursing staff” OR “Clinical nurse” OR “Nurse specialist” OR “Nurse clinician” OR “Nursing care provider” OR “Nursing team member”) OR AB (“Registered Nurse” OR “RN” OR “Nurs * p *” OR “Nursing staff” OR “Clinical nurse” OR “Nurse specialist” OR “Nurse clinician” OR “Nursing care provider” OR “Nursing team member”) OR DE “Nursing”) | AND | (TL (“Transformational leadership” OR “TFL” OR “Transformational leader*” OR “Transformational manager*”) OR AB (“Transformational leadership” OR “TFL” OR “Transformational leader *” OR “Transformational manager *”) OR DE “Transformational leadership”) | AND | (TL (“Work Environment” OR “Working Conditions” OR “Workplace” OR “Job Satisfaction” OR “Patient Outcome” OR “Health Outcome” OR “Treatment Outcome”) OR AB (“Work Environment” OR “Working Conditions” OR “Workplace” OR “Job Satisfaction” OR “Patient Outcome” OR “Health Outcome” OR “Treatment Outcome”) OR MM (“Working Environments” OR “Outcome Assessment, Health Care”)) |
| Authors and Year | Tool | Methodology | Sample | Main Results |
|---|---|---|---|---|
| TFL—Multifactor Leadership Questionnaire (MLQ) Job satisfaction—Global Job Satisfaction Scale (GJSS) Conditions Of Work-Effectiveness II (CWEQ-II) Nurse-assessed adverse patient outcomes | Cross-sectional | 378 nurses | Significant indirect relationship between TFL and adverse patient outcomes. The level of staff empowerment strongly influences the job satisfaction of nurses. Nurses perceived TFL behaviors of managers to be moderate. |
| TFL (7-item scale) Structural empowerment (12-item scale) Job satisfaction (3-item scale) Adverse patient outcomes (5-item scale) | Cross-sectional | 386 nurses | TFL behavior was found to have a positive effect on patient outcomes, decreasing the likelihood of unfavorable outcomes and improving the overall quality of care. The mediator between TFL and these desired patient outcomes was structural empowerment and job satisfaction. Nurses perceived TFL behaviors of managers to be high. |
| TFL—Transformational Leadership Scale (TLS) Medication error—Medication Safety Scale (MSS) | Cross-sectional | 161 nurses | Nurses did not perceive managers to fully adapt TFL behaviors. Support for professional development was strongly perceived. Giving feedback and rewarding was the weakest area of TFL. TFL related the strongest to medication safety through the management of the nursing process. |
| TFL—The Global Transformational Leadership Scale (GTL) Job demands and resources—Short Inventory to Monitor Psychological Hazards (SIMPH)/Job Demands–Resources model Patient safety culture—Nursing Home Survey On Patient Safety Culture (NHSOPSC) | Cross-sectional | 156 nurses | The speed of work and the amount of emotional strain on employees had a negative effect on patient safety culture. The impact of TFL on patient safety culture and overall perception of patient safety was the most significant factor. |
| TFL—The Global Transformational Leadership Scale (GTL) Job demands and resources—Short Inventory to Monitor Psychological Hazards (SIMPH)/Job Demands–Resources model Patient safety culture—Nursing Home Survey On Patient Safety Culture (NHSOPSC) | Cross-sectional | 139 nurses | TFL was responsible for 35.7% of variance in patient safety culture TFL and job resources positively related to work engagement Skill utilization was the strongest single predictor of work engagement compared to TFL. |
| TFL—Multifactor Leadership Questionnaire (MLQ) Knowledge-related job characteristics—Work Design Questionnaire (WDQ) Safety performance and compliance | Cross-sectional | 152 nurses | The more transformational the leader was perceived, the more nursing staff participated and complied with patient safety. Indirect link between TFL and safety performance via knowledge-related job characteristics. TFL can influence perceptions of knowledge-related job characteristics of followers through intellectual stimulation. |
| TFL—MLQ Psychological empowerment Employee commitment | Cross-sectional | 332 acute care nurses | Highest perceived leadership style was TFL, with inspirational motivation and idealized attributes being high. Transactional leadership and laissez-faire leadership had a more positive and significant effect on commitment than TFL. Having a TFL style of management can increase employee devotion through granting authority, as well as involving staff in the decision-making process. |
| TFL—Global Transformational Leadership Scale (GTFLS) Organizational trust—organizational trust scale Organizational identification—Organizational identification Job stress—Job Stress Scale (JSS) 7 items | Cross-sectional | 150 nurses | Non-punctuative reporting medical errors: 52.7% no adverse events reported in 12 months, 31.3% reported 1–2 adverse events and 10% reported 3–5 adverse events. Positive relationship between organizational identification, organizational trust, and TFL. |
| TFL—MLQ-5X Structural empowerment—C WEQ11 | Cross-sectional | 181 clinical nurses | Statistically significant correlation between staff nurses’ perception of managers’ TFL behaviors and their structural empowerment as frontline staff. A negative correlation was found between structural empowerment and staff nurses’ perception of NMs’ laissez-faire leadership. |
| TFL—adopted from earlier studies 19 items Patient safety climate | Cross-sectional | 439 nurses | Manager support was highly associated with nurse innovation behaviors. TFL had a significantly positive effect on nurse innovation behavior. TFL was strongly related to both innovation climate and patient safety climate. |
| Patient safety culture—AHRQ (2004) TFL—Forces of Magnetism questionnaire | Cross-sectional | 324 nursing staff | TFL was found to have a high magnetic force. Strong positive correlation between TFL and patient safety culture. Management support for patient safety was reported as highly important. |
| Patient safety culture—HSPSCPatient satisfaction—RHCS | Descriptive correlational | 2566 patients 5778 nursing staff and leaders | Highest score of managers TFL behavior: support for professional development. Feedback and rewards were the weakest for nurse managers. Awareness of the work of nursing directors was low. Patient satisfaction outcome was the only factor exceeding target level. |
| TFL—MLQ Job satisfaction Empowerment | Cross-sectional | 200 clinical nurses | TFL showed a significant indirect positive effect on job satisfaction. TFL was directly related to fostering structural empowerment, which in turn affected job satisfaction positively. |
| Organizational commitment Job satisfaction TFL | Cross-sectional | 1037 newly licensed registered nurses | TFL did not have direct impact on intent to stay. Organizational commitment, job satisfaction, RN-MD collaboration, and mentor support had a positive effect on the intent to stay. TFL had non-significant direct probability of increasing organizational commitment. TFL was not found to be a significant predictor of job satisfaction. |
| Spiritual Climate Scale Emotional Exhaustion ScaleIntent to leave—Turnover Intention Scale | Cross-sectional | 319 nurse clinicians | Nurse staff experienced moderate levels of TFL. Nurses frequently felt emotional exhaustion, burnt out, and had thoughts of leaving profession. Strong relationship between TFL and spiritual climate, where spiritual climate had a mediating effect on TFL’s ability to reduce burnout and intention to leave. |
| TFL—research questionnaire Clan culture Organizational Culture Measurement Scale Organizational commitmentJob satisfaction | Cross-sectional | 217 geriatric nurses | TFL and clan culture together explained job satisfaction amongst nursing staff. Organizational commitment, job satisfaction, and professional identity had a significantly positive effect on willingness to stay. |
| MLQ-5X—shorter rate form Workplace culture six-item measure created for the study Job satisfaction—GJS Burnout—MBI- COVID-19—measured with six items around demand and pressure | Cross-sectional | 645 nurses | TFL had a strong, significantly positive effect on job satisfaction and workplace culture and a negative effect on burnout. TFL was found to, directly and indirectly, improve work environment. Direct, robust positive relationship between TFL and workplace culture. TFL can influence staff nurses’ satisfaction and mitigate the risk of burnout by establishing a supportive and inclusive work environment. |
| TFL—GTL Team performance Team climate Knowledge sharing | Cross-sectional | 183 geriatric nurses | TFL facilitated a safe team climate, which allowed knowledge sharing and reflection on processes and tasks. This was found to increase the team performance, including effectiveness and innovativeness. TFL enhanced learning activities of teams, which in turn affects their performance and outcomes positively. |
| Leadership Practices Inventory (LPI) Patient safety culture—HSOPSC | Cross-sectional | Nursing managers and nursing staff | Nursing manager’s perception of their own TFL was higher than staff nurses. Lowest sub-dimension was the sub-dimensions of staffing, non-punctuative response to errors, and frequency of errors reported by both parties, at lower than 50%, indicating PSC weakness. |
| Semi-structured interview | Qualitative study | 11 nurse managers | Adverse events reporting reform leaving dysfunctional operational models. Encouraging nursing staff’s openness around adverse events by establishing a blame-free culture. Blame and shame—a challenge to recognize adverse events. |
| TFL—MLQ Patient safety—PSQ | Cross-sectional | 1355 nurses and pharmacists | Non-significant effect on error reporting compared to transactional leaders who showed higher levels of good reporting practices. Even though TFL was main behavior, no preventative actions were mentioned in incident reports. |
| Multifactor Leadership Questionnaire Karasek’s Job Content Questionnaire (JCQ) Occupational Stress Indicator (OSI) Organisational Commitment Questionnaire (OCQ) General Health Questionnaire | Cross-sectional | 651 nurses | Based on the main hypotheses of the research, the results revealed a positive relationship between nursing transformational leadership and general health status. The supervisor support plays a mediating role between transformational leadership styles and job satisfaction. Supervisor support has a dramatic influence on employees’ job satisfaction compared with other factors. |
| Multifactor Leadership Questionnaire Organizational Description Questionnaire Annual quality indicators from the hospitals | Cross-sectional | 1626 health care workers | In each hospital, 66.4% to 87.1% of participants identified their hospital’s organizational culture as transformational, whereas 41 out of 48 departments were identified as having a transformational culture. The differences between leadership style and organizational culture were statistically significant for four of the hospitals. For most of the quality indicators, there was a positive but non-significant, correlation with leadership style. |
| Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 |
|---|---|---|---|---|---|---|---|---|
| Boamah, S., Spence Laschinger, H., Wong, C., and Clarke, S. (2018) | √ | √ | √ | √ | √ | √ | √ | √ |
| Asif, M., Jameel, A., Hussain, A., Hwang, J., and Sahito, N. (2019) | √ | √ | √ | √ | √ | √ | √ | √ |
| Lappalainen, M., Härkänen, M., and Kvist, T. (2020) | √ | √ | √ | √ | √ | √ | √ | |
| Seljemo, C., Viksveen, P., and Ree, E. (2020) | √ | √ | √ | √ | √ | √ | √ | √ |
| Ree, E. and Wiig, S. (2019) | √ | √ | √ | √ | √ | √ | √ | √ |
| Lievens and Vlerick, P. (2014) | √ | √ | √ | √ | √ | √ | √ | √ |
| Asiri, S., Rohrer, W., Al-Surimi, K., Da’ar, O., and Ahmed, A. (2016) | √ | √ | √ | √ | √ | √ | √ | √ |
| Y Tekingündüz, S., Yıldız, E., and İnci, R. (2021) | √ | √ | √ | √ | √ | √ | √ | √ |
| Choi, S., Goh, C., Adam, M., and Tan, O. (2016) | √ | √ | √ | √ | √ | √ | √ | √ |
| Khan, B., Quinn Griffin, M., and Fitzpatrick, J. (2018) | √ | √ | √ | √ | √ | √ | √ | √ |
| Weng, R., Huang, C., Chen, L., and Chang, L. (2015) | √ | √ | √ | √ | √ | √ | √ | √ |
| El-Demerdash, A. M. S., Elhosany, W. A., and Hefny, M. A. M (2018) | √ | √ | √ | √ | √ | √ | √ | |
| Brewer, C., Kovner, C., Djukic, M., Fatehi, F., Greene, W., Chacko, T., and Yang, Y. (2016) | √ | √ | √ | √ | √ | √ | √ | √ |
| Xie, Y. et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ |
| Boamah, S.A. (2022) | √ | √ | √ | √ | √ | √ | √ | √ |
| Anselmann, V. and Mulder, R.H. (2020) | √ | √ | √ | √ | √ | √ | √ | √ |
| Yilmaz, A. and Duygulu, S. (2020) | √ | √ | √ | √ | √ | √ | √ | |
| Wagner, A. et al. (2019) | √ | √ | √ | √ | √ | √ | √ | √ |
| ALFadhalah, T. and Elamir, H. (2021) | √ | √ | √ | √ | √ | √ | √ | |
| Liukka, M., Hupli, M., and Turunen, H. (2017) | √ | √ | √ | √ | √ | √ | √ | √ |
| Lin, PY., MacLennan, S., and Hunt, N (2015) | √ | √ | √ | √ | √ | √ | √ | √ |
| Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Liukka, M., Hupli, M., and Turunen, H. (2017) | √ | √ | √ | √ | √ | No | No | √ | √ | √ |
| Authors and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| Kvist, T., Mäntynen, R., Turunen, H., Partanen, P., Miettinen, M., Wolf, G., and Vehviläinen-Julkunen, K. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | √ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ystaas, L.M.K.; Nikitara, M.; Ghobrial, S.; Latzourakis, E.; Polychronis, G.; Constantinou, C.S. The Impact of Transformational Leadership in the Nursing Work Environment and Patients’ Outcomes: A Systematic Review. Nurs. Rep. 2023, 13, 1271-1290. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13030108
Ystaas LMK, Nikitara M, Ghobrial S, Latzourakis E, Polychronis G, Constantinou CS. The Impact of Transformational Leadership in the Nursing Work Environment and Patients’ Outcomes: A Systematic Review. Nursing Reports. 2023; 13(3):1271-1290. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13030108
Chicago/Turabian StyleYstaas, Line Miray Kazin, Monica Nikitara, Savoula Ghobrial, Evangelos Latzourakis, Giannis Polychronis, and Costas S. Constantinou. 2023. "The Impact of Transformational Leadership in the Nursing Work Environment and Patients’ Outcomes: A Systematic Review" Nursing Reports 13, no. 3: 1271-1290. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13030108