
Community-Based Hip Screening for Up to Four-Month-Old Infants and Health Guidance for Their Caregivers in Japan: A Nation-Wide Survey


Abstract
:1. Introduction
2. Materials and Methods
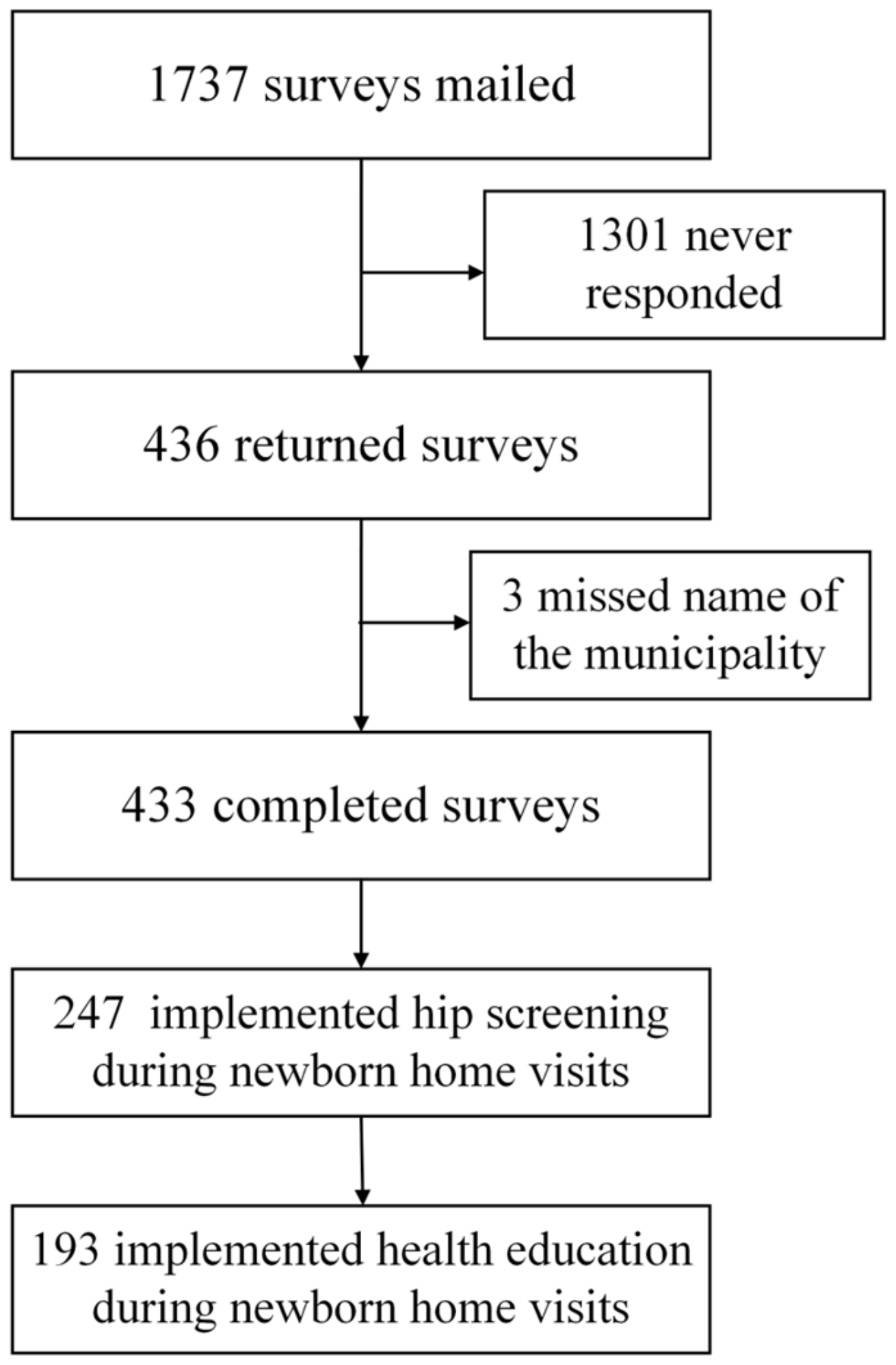
2.1. Participants and Procedure
2.2. Measurements
2.3. Data Linkage and Coding
2.4. Analysis
3. Results
3.1. Current Status of Municipalities’ Hip Screening
3.2. Observed Risk Factors, Health Guidance, and Staff Training for Newborn Visits
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Public Involvement Statement
Guidelines and Standards Statement
Data Availability Statement
Conflicts of Interest
References
- Shorter, D.; Hong, T.; Osborn, D.A. Cochrane Review: Screening programmes for developmental dysplasia of the hip in newborn infants. Evid. Based Child Health 2013, 8, 11–54. [Google Scholar] [CrossRef]
- Agostiniani, R.; Atti, G.; Bonforte, S.; Casini, C.; Cirillo, M.; De Pellegrin, M.; Di Bello, D.; Esposito, F.; Galla, A.; Marrè Brunenghi, G.; et al. Recommendations for early diagnosis of developmental dysplasia of the hip (DDH): Working group intersociety consensus document. Ital. J. Pediatr. 2020, 46, 150. [Google Scholar] [CrossRef] [PubMed]
- Lucchesi, G.; Sacco, R.; Zhou, W.; Li, Y.; Li, L.; Canavese, F. DDH in the walking age: Review of patients with long-term follow-up. Indian. J. Orthop. 2021, 55, 1503–1514. [Google Scholar] [CrossRef] [PubMed]
- Gambling, T.S.; Long, A. Psycho-social impact of developmental dysplasia of the hip and of differential access to early diagnosis and treatment: A narrative study of young adults. SAGE Open Med. 2019, 7, 2050312119836010. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, W.; van der Steen, M.C.; van Veen, M.R.; van Douveren, F.; Witlox, M.A.; Tolk, J.J. Parental experiences of children with developmental dysplasia of the hip: A qualitative study. BMJ Open 2022, 12, e062585. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Canadian Task Force on Preventive Health Care. Preventive health care, 2001 update: Screening and management of developmental dysplasia of the hip in newborns. CMAJ 2001, 164, 1669–1677. [Google Scholar]
- Ulziibat, M.; Munkhuu, B.; Bataa, A.-E.; Schmid, R.; Baumann, T.; Essig, S. Traditional Mongolian swaddling and developmental dysplasia of the hip: A randomized controlled trial. BMC Pediatr. 2021, 21, 450. [Google Scholar] [CrossRef]
- van Sleuwen, B.E.; Engelberts, A.C.; Boere-Boonekamp, M.M.; Kuis, W.; Schulpen, T.W.; L’Hoir, M.P. Swaddling: A systematic review. Pediatrics 2007, 120, e1097–e1106. [Google Scholar] [CrossRef]
- Den, H.; Ito, J.; Kokaze, A. Epidemiology of developmental dysplasia of the hip: Analysis of Japanese national database. J. Epidemiol. 2023, 33, 186–192. [Google Scholar] [CrossRef]
- Lee, W.C.; Kao, H.K.; Wang, S.M.; Yang, W.E.; Chang, C.H.; Kuo, K.N. Cold weather as a risk factor for late diagnosis and surgery for developmental dysplasia of the hip. J. Bone Jt. Surg. Am. 2022, 104, 115–122. [Google Scholar] [CrossRef]
- Harper, P.; Joseph, B.M.; Clarke, N.M.P.; Herrera-Soto, J.; Sankar, W.N.; Schaeffer, E.K.; Mulpuri, K.; Aarvold, A.; International Hip Dysplasia Institute (IHDI). Even experts can be fooled: Reliability of clinical examination for diagnosing hip dislocations in newborns. J. Pediatr. Orthop. 2020, 40, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Graf, R. The diagnosis of congenital hip-joint dislocation by the ultrasonic combound treatment. Arch Orthop Trauma Surg (1978) 1980, 97, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Harcke, H.T.; Clarke, N.M.; Lee, M.S.; Borns, P.F.; MacEwen, G.D. Examination of the infant hip with real-time ultrasonography. J. Ultrasound Med. 1984, 3, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.H.; Harcke, H.T.; MacEwen, G.D. The infant hip: Real-time US assessment of acetabular development. Radiology 1985, 157, 673–677. [Google Scholar] [CrossRef] [PubMed]
- O’Beirne, J.G.; Chlapoutakis, K.; Alshryda, S.; Aydingoz, U.; Baumann, T.; Casini, C.; de Pellegrin, M.; Domos, G.; Dubs, B.; Hemmadi, S.; et al. International interdisciplinary consensus meeting on the evaluation of developmental dysplasia of the hip. Ultraschall Med. 2019, 40, 454–464. [Google Scholar] [CrossRef] [PubMed]
- National Center for Child Health and Development. Nyuyoji Kenkou Shinsa Shintai Shinsatsu Manyuaru [Physical Examination Manual for Infant Health Screening]. Available online: https://www.ncchd.go.jp/center/activity/kokoro_jigyo/manual.pdf (accessed on 19 June 2023).
- Oka, A.; Asagai, Y. The Fiscal Year 2015, Japan Agency for Medical Research and Development Research Fund, Comprehensive Research Program for Overcoming Childhood Diseases: A Guide to Preventing and Early Detection of Developmental Dysplasia of the Hip-For the Healthy Development of Infants. Available online: http://www.jpoa.org/wp-content/uploads/2013/07/170121.pdf (accessed on 19 June 2023).
- Yamamuro, T.; Ishida, K. Recent advances in the prevention, early diagnosis, and treatment of congenital dislocation of the hip in Japan. Clin. Orthop. Relat. Res. 1984, 184, 34–40. [Google Scholar] [CrossRef]
- Ishida, K. Prevention of the development of the typical dislocation of the hip. Clin. Orthop. Relat. Res. 1977, 126, 167–169. [Google Scholar] [CrossRef]
- Nelson, A.M. Risks and benefits of swaddling healthy infants: An integrative review. MCN Am. J. Matern. Child. Nurs. 2017, 42, 216–225. [Google Scholar] [CrossRef]
- Vaidya, S.; Aroojis, A.; Mehta, R. Developmental dysplasia of hip and post-natal positioning: Role of swaddling and baby-wearing. Indian. J. Orthop. 2021, 55, 1410–1416. [Google Scholar] [CrossRef]
- World Health Organization. Responding to Child Maltreatment: A Clinical Handbook for Health Professionals. Available online: https://www.who.int/publications/i/item/9789240048737 (accessed on 19 June 2023).
- Yoshioka-Maeda, K.; Fujii, H. Mothers susceptible to child maltreatment and requiring public health nurses’ continuous support. Public. Health Nurs. 2022, 39, 48–61. [Google Scholar] [CrossRef]
- The Japan Ministry of Health, Labour and Welfare. Seiiku iryou tou no teikyou ni kansuru sesaku no sougou teki na suishin ni kansuru kihon teki na houshin ni tsuite [Basic Policy on Comprehensive Promotion of Policies for Provision of Child Health and Development and Medical Care]. Available online: https://www.mhlw.go.jp/content/000735844.pdf (accessed on 19 June 2023).
- Maternal and Child Health Act. Available online: https://elaws.e-gov.go.jp/document?lawid=340AC0000000141 (accessed on 19 June 2023).
- Child Welfare Act. Available online: https://elaws.e-gov.go.jp/document?lawid=322AC0000000164 (accessed on 19 June 2023).
- The Japan Ministry of Health, Labour and Welfare. The Guidelines for All Infant and Their Family Home Visiting Project. Available online: https://www.mhlw.go.jp/bunya/kodomo/kosodate12/03.html (accessed on 19 June 2023).
- Hattori, T.; Inaba, Y.; Ichinohe, S.; Kitano, T.; Kobayashi, D.; Saisu, T.; Ozaki, T. The epidemiology of developmental dysplasia of the hip in Japan: Findings from a nationwide multi-center survey. J. Orthop. Sci. 2017, 22, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Mert Doğan, G.; Aslantürk, O. Does the COVID-19 pandemic cause late diagnosis and delay in treatment in developmental dysplasia of hip patients? Int. J. Clin. Pract. 2021, 75, e14572. [Google Scholar] [CrossRef] [PubMed]
- The Japan Ministry of Health, Labour and Welfare. Correspondence of Novel Coronavirus to Implementation of Maternal and Child Health Projects. Available online: https://www.mhlw.go.jp/content/000621060.pdf (accessed on 19 June 2023).
- The Japan Ministry of Health, Labour and Welfare. Survey on the Implementation of All Infant Family Home Visiting Project. Available online: https://www.mhlw.go.jp/content/11900000/000987743.pdf (accessed on 19 June 2023).
- Kuitunen, I.; Uimonen, M.M.; Haapanen, M.; Sund, R.; Helenius, I.; Ponkilainen, V.T. Incidence of neonatal developmental dysplasia of the hip and late detection rates based on screening strategy: A systematic review and meta-analysis. JAMA Netw. Open 2022, 5, e2227638. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Enhancing the role of community health nursing for universal health coverage. In Human Resources for Health Observer Series; WHO: Geneva, Switzerland, 2017; Volume 18. Available online: https://apps.who.int/iris/handle/10665/255047 (accessed on 19 June 2023).
- Yamada, T.; Ehara, J.; Funakoshi, H.; Endo, K.; Kitano, Y. Effectiveness of point of care ultrasound (POCUS) simulation course and skills retention for Japanese nurse practitioners. BMC Nurs. 2023, 22, 21. [Google Scholar] [CrossRef]
- Fraleigh, C.D.M.; Duff, E. Point-of-care ultrasound: An emerging clinical tool to enhance physical assessment. Nurse Pract. 2022, 47, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Var, C.; Oberhelman, R.A.; Shu, T.; Leang, S.; Duggal, R.; Le, J.; Bazzano, A.N. A linked community and health facility intervention to improve newborn health in Cambodia: The NICCI Stepped-Wedge Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public. Health 2020, 17, 1559. [Google Scholar] [CrossRef]
- Fujiwara, T.; Isumi, A.; Sampei, M.; Yamada, F.; Miyazaki, Y. Effectiveness of using an educational video simulating the anatomical mechanism of shaking and smothering in a home-visit program to prevent self-reported infant abuse: A population-based quasi-experimental study in Japan. Child. Abuse Negl. 2020, 101, 104359. [Google Scholar] [CrossRef]
- World Health Organization. Improving Early Childhood Development: WHO Guideline. Available online: https://iris.who.int/bitstream/handle/10665/331306/9789240002098-eng.pdf?sequence=1 (accessed on 25 September 2023).
- Li, J.; Aroojis, A.; Mulpuri, K.; Shea, K.G.; Schaeffer, E.K. Development of a DDH care pathway for India: A study methodology to guide similar efforts in other countries and for other conditions. Indian. J. Orthop. 2021, 55, 1549–1558. [Google Scholar] [CrossRef]
- Vuong, B.; Zhou, J.; Park, M.; Patey, R.; Segovia, N.; Imrie, M.; Pun, S.Y. Knowledge and practices related to hip-healthy swaddling for newborns among maternity nurses. J. Obstet. Gynecol. Neonatal Nurs. 2022, 51, 566–576. [Google Scholar] [CrossRef]


{kind=link}
| Municipality, n | (%) | (95% CI) | Births, n | (%) | |||
|---|---|---|---|---|---|---|---|
| Hip screening | |||||||
| Within 4 months | Absent | 11 | (2.5) | (1.1–4.0) | 8624 | (2.9) | |
| Present | 422 | (97.5) | (96.0–98.9) | 291,872 | (97.1) | ||
| Within 2 months | Absent | 171 | (39.5) | (34.9–44.1) | 138,434 | (46.1) | |
| Present | 262 | (60.5) | (55.9–65.1) | 162,062 | (53.9) | ||
| At newborn visits | Absent | 186 | (43.0) | (38.3–47.6) | 141,519 | (47.1) | |
| Present | 247 | (57.0) | (52.4–61.7) | 158,977 | (52.9) | ||
| Using ultrasound * | Absent | 397 | (91.7) | (89.1–94.3) | 256,658 | (85.4) | |
| Present | 10 | (2.3) | (0.9–3.7) | 6371 | (2.1) | ||
| Total | 433 | (100.0) | 300,496 | (100.0) | |||
| Hip Screening | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Within Four Months | Within Two Months | At Newborn Visit | |||||||||||||||||
| Absent | Present | Absent | Present | Absent | Present | ||||||||||||||
| n | (%) | n | (%) | AOR | p | n | (%) | n | (%) | AOR | p | n | (%) | n | (%) | AOR | p | ||
| Regional climate | |||||||||||||||||||
| Warm | 4 | (1.4) | 291 | (98.6) | 105 | (35.6) | 190 | (64.4) | 112 | (38.0) | 183 | (62.0) | |||||||
| Cold | 7 | (5.1) | 131 | (94.9) | 0.17 | 0.007 | 66 | (47.8) | 72 | (52.2) | 0.51 | 0.003 | 74 | (53.6) | 64 | (46.4) | 0.33 | <0.001 | |
| Population | |||||||||||||||||||
| <10,000 | 1 | (1.1) | 94 | (98.9) | 36 | (37.9) | 59 | (62.1) | 39 | (41.1) | 56 | (58.9) | |||||||
| <200,000 | 8 | (2.7) | 283 | (97.3) | 0.19 | 0.130 | 108 | (37.1) | 183 | (62.9) | 0.78 | 0.359 | 120 | (41.2) | 171 | (58.8) | 0.75 | 0.296 | |
| ≥200,000 | 2 | (4.3) | 45 | (95.7) | 0.10 | 0.067 | 27 | (57.4) | 20 | (42.6) | 0.32 | 0.003 | 27 | (57.4) | 20 | (42.6) | 0.40 | 0.020 | |
| Newborn visitor | |||||||||||||||||||
| Nurses only | 132 | (38.6) | 210 | (61.4) | |||||||||||||||
| Non-nurses only | 17 | (77.3) | 5 | (22.7) | 0.14 | 0.000 | |||||||||||||
| Mixed | 37 | (53.6) | 32 | (46.4) | 0.42 | 0.002 | |||||||||||||
| Total | 11 | (2.5) | 422 | (97.5) | 171 | (39.5) | 262 | (60.5) | 186 | (43.0) | 247 | (57.0) | |||||||
| Observation of the Recommended Five Risk Factors | Health Guidance for Caregivers | Training for All Visitors | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Not Complete | Complete | Absent | Present | Absent | Present | ||||||||||||||
| n | (%) | n | (%) | AOR | p | n | (%) | n | (%) | AOR | p | n | (%) | n | (%) | AOR | p | ||
| Regional climate | |||||||||||||||||||
| Warm | 136 | (74.3) | 47 | (25.7) | 44 | (24.0) | 139 | (76.0) | 138 | (75.4) | 45 | (24.6) | |||||||
| Cold | 39 | (60.9) | 25 | (39.1) | 1.80 | 0.099 | 10 | (15.6) | 54 | (84.4) | 2.20 | 0.070 | 47 | (73.4) | 17 | (26.6) | 1.60 | 0.212 | |
| Population | |||||||||||||||||||
| <10,000 | 34 | (60.7) | 22 | (39.3) | 14 | (25.0) | 42 | (75.0) | 46 | (82.1) | 10 | (17.9) | |||||||
| <200,000 | 131 | (76.6) | 40 | (23.4) | 0.59 | 0.144 | 36 | (21.1) | 135 | (78.9) | 1.74 | 0.173 | 127 | (74.3) | 44 | (25.7) | 1.94 | 0.126 | |
| ≥200,000 | 10 | (50.0) | 10 | (50.0) | 2.11 | 0.193 | 4 | (20.0) | 16 | (80.0) | 2.12 | 0.271 | 12 | (60.0) | 8 | (40.0) | 3.77 | 0.034 | |
| Newborn visitor | |||||||||||||||||||
| Nurses only | 151 | (71.9) | 59 | (28.1) | 46 | (21.9) | 164 | (78.1) | 159 | (75.7) | 51 | (24.3) | |||||||
| Non-nurses only | 2 | (40.0) | 3 | (60.0) | 4.87 | 0.095 | 0 | (0.0) | 5 | (100.0) | 465,877,307.66 | 0.999 | 4 | (80.0) | 1 | (20.0) | 0.85 | 0.883 | |
| Mixed | 22 | (68.8) | 10 | (31.3) | 1.24 | 0.626 | 8 | (25.0) | 24 | (75.0) | 0.88 | 0.773 | 22 | (68.8) | 10 | (31.3) | 1.33 | 0.505 | |
| Total | 175 | (70.9) | 72 | (29.1) | 54 | (21.9) | 193 | (78.1) | 185 | (74.9) | 62 | (25.1) | |||||||
| Observation of the Recommended Five Risk Factors | Health Guidance for Caregivers | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Not Complete | Complete | Absent | Present | ||||||||||
| n | (%) | n | (%) | AOR | p | n | (%) | n | (%) | AOR | p | ||
| Training for all visitors | |||||||||||||
| Absent | 145 | (78.4) | 40 | (21.6) | 47 | (25.4) | 138 | (74.6) | |||||
| Present | 30 | (48.4) | 32 | (51.6) | 4.19 | <0.001 | 7 | (11.3) | 55 | (88.7) | 2.60 | 0.031 | |
| Observed Risk Factors (n = 247) | Not Observe | Observed | ||
| n | (%) | n | (%) | |
| Limited hip abduction * | 17 | (6.9) | 230 | (93.1) |
| Asymmetry of the groin skin folds * | 37 | (15.0) | 210 | (85.0) |
| Female sex * | 119 | (48.2) | 128 | (51.8) |
| Family history of DDH * | 144 | (58.3) | 103 | (41.7) |
| Breech presentation * | 137 | (55.5) | 110 | (44.5) |
| Barlow and Ortolani tests | 128 | (51.8) | 119 | (48.2) |
| Birth season | 190 | (76.9) | 57 | (23.1) |
| Asymmetrical head turning | 125 | (50.6) | 122 | (49.4) |
| Health guidance (n = 193) | Absent | Present | ||
| n | (%) | n | (%) | |
| Wearing diapers | 41 | (21.2) | 152 | (78.8) |
| Babywearing | 12 | (6.2) | 181 | (93.8) |
| Baby carrier | 91 | (47.2) | 102 | (52.8) |
| Baby clothes | 79 | (40.9) | 114 | (59.1) |
| Bedding | 100 | (51.8) | 93 | (48.2) |
| Swaddling | 111 | (57.5) | 82 | (42.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshioka-Maeda, K.; Matsumoto, H.; Inagaki-Asano, A.; Honda, C. Community-Based Hip Screening for Up to Four-Month-Old Infants and Health Guidance for Their Caregivers in Japan: A Nation-Wide Survey. Nurs. Rep. 2023, 13, 1442-1451. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13040121
Yoshioka-Maeda K, Matsumoto H, Inagaki-Asano A, Honda C. Community-Based Hip Screening for Up to Four-Month-Old Infants and Health Guidance for Their Caregivers in Japan: A Nation-Wide Survey. Nursing Reports. 2023; 13(4):1442-1451. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13040121
Chicago/Turabian StyleYoshioka-Maeda, Kyoko, Hiroshige Matsumoto, Asa Inagaki-Asano, and Chikako Honda. 2023. "Community-Based Hip Screening for Up to Four-Month-Old Infants and Health Guidance for Their Caregivers in Japan: A Nation-Wide Survey" Nursing Reports 13, no. 4: 1442-1451. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep13040121