
Effect of Behavioral Activation for Women with Postnatal Depression: A Systematic Review and Meta-Analysis
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
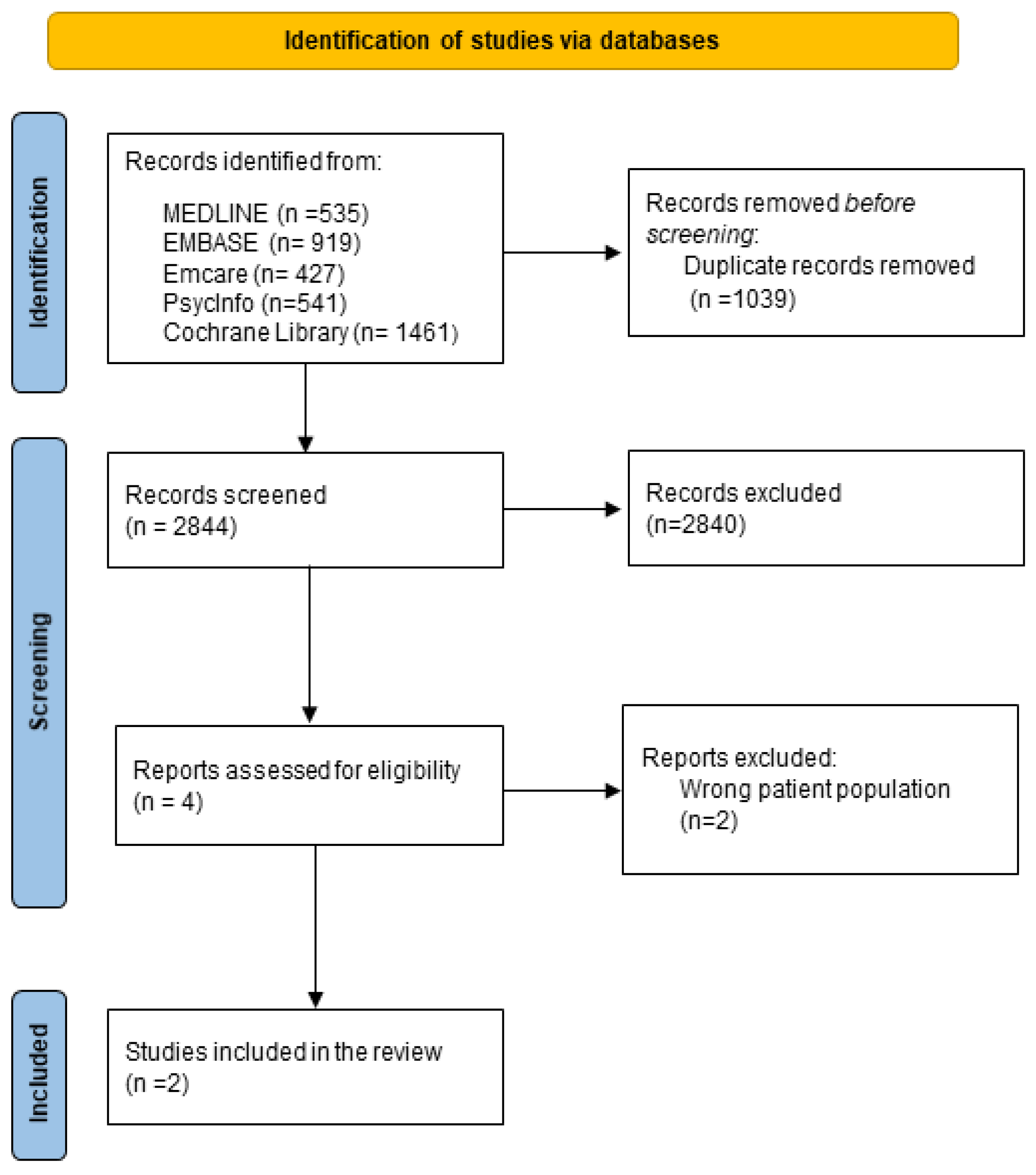
2.1. Eligibility Criteria
2.2. Search Methods
2.3. Data Collection and Extraction
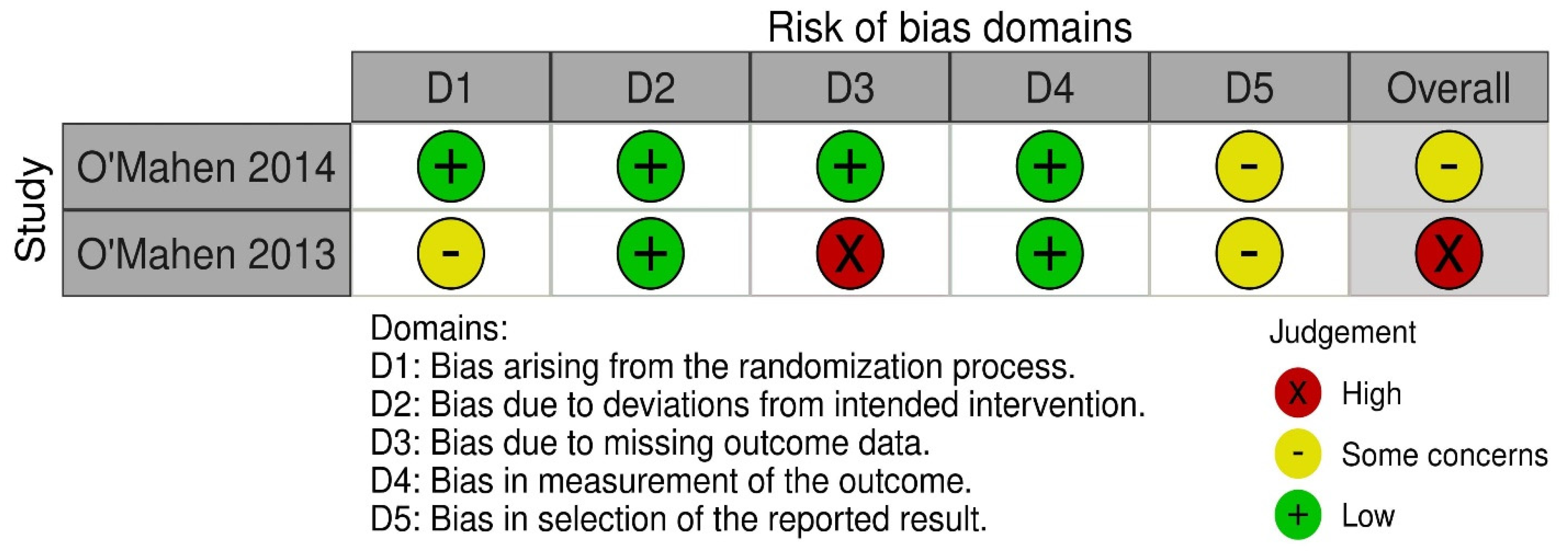
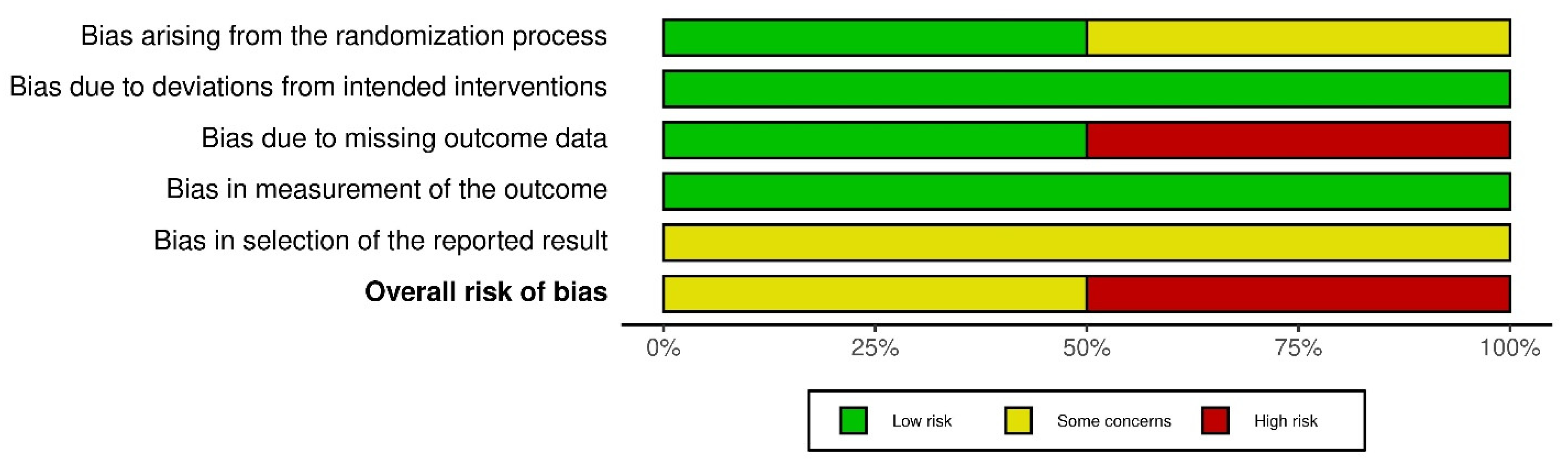
2.4. Quality Assessment and Risk of Bias
2.5. Data Synthesis and Statistical Analysis
2.6. Patient and Public Involvement
3. Results
3.1. Descriptive Characteristics of Studies, Population, Intervention, and Outcomes
3.2. Risk of Bias Assessment
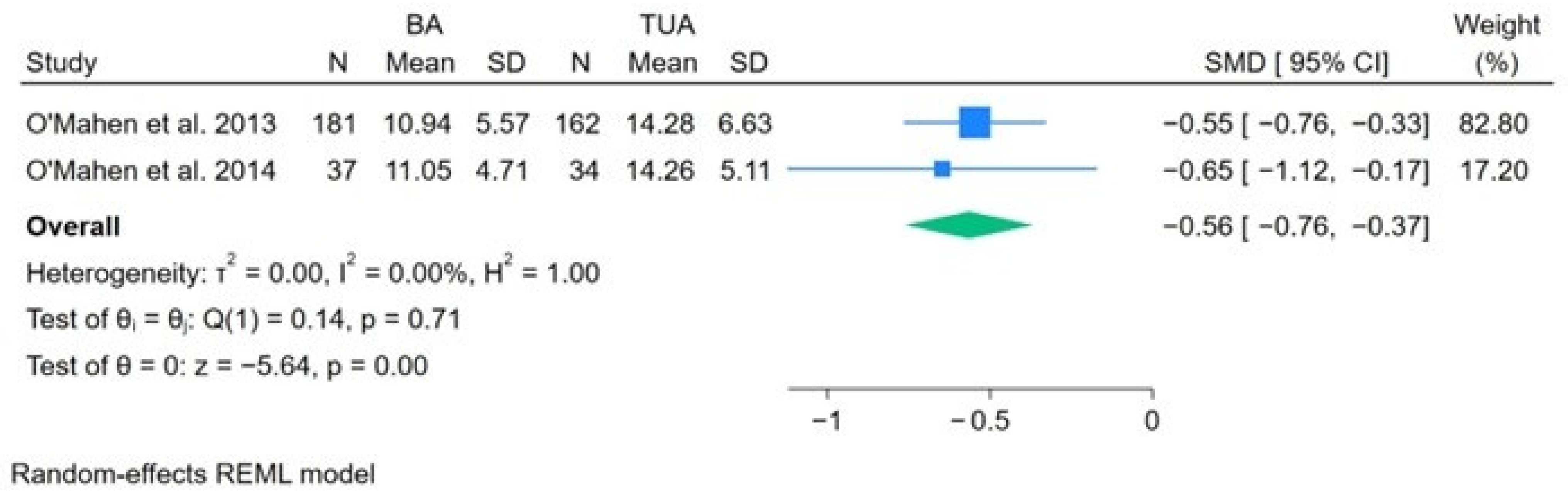
3.3. Effects of BA versus TAU on Reducing Postnatal Depression
4. Discussion
4.1. Online BA with Support May Be Beneficial to Women with PND
4.2. Scalability of BA
4.3. Effectiveness of BA
4.4. Clinical Governance
4.5. Strengths and Limitations of the Study
5. Conclusions
6. Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.; Arteche, A.; Fearon, P.; Halligan, S.; Croudace, T.; Cooper, P. The effects of maternal postnatal depression and child sex on academic performance at age 16 years: A developmental approach. J. Child Psychol. Psychiatry 2010, 51, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Pawlby, S.; Sharp, D.; Hay, D.; O’Keane, V. Postnatal depression and child outcome at 11 years: The importance of accurate diagnosis. J. Affect. Disord. 2008, 107, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.; Woolgar, M.; Cooper, P. Detection and treatment of postpartum depression. Community Pract. J. Community Pract. Health Visit. Assoc. 2004, 77, 13–17. [Google Scholar]
- Goodman, J.H. Women’s attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth 2009, 36, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Ayers, S.; Drey, N. A Thematic Analysis of Stigma and Disclosure for Perinatal Depression on an Online Forum. JMIR Ment. Health 2016, 3, e18. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, J.; Holt, C.J.; Gemmill, A.W.; Ericksen, J.; Leigh, B.; Buist, A.; Schembri, C. Treating postnatal depressive symptoms in primary care: A randomised controlled trial of GP management, with and without adjunctive counselling. BMC Psychiatry 2011, 11, 95. [Google Scholar] [CrossRef]
- Dennis, C.L.; Chung-Lee, L. Postpartum depression help-seeking barriers and maternal treatment preferences: A qualitative systematic review. Birth 2006, 33, 323–331. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance [NICE Clinical Guideline [CG192]]. 2020. Available online: https://www.nice.org.uk/guidance/cg192 (accessed on 17 June 2022).
- Huang, L.; Zhao, Y.; Qiang, C.; Fan, B. Is cognitive behavioral therapy a better choice for women with postnatal depression? A systematic review and meta-analysis. PLoS ONE 2018, 13, e0205243. [Google Scholar] [CrossRef]
- Ross, E.L.; Vijan, S.; Miller, E.M.; Valenstein, M.; Zivin, K. The Cost-Effectiveness of Cognitive Behavioral Therapy Versus Second-Generation Antidepressants for Initial Treatment of Major Depressive Disorder in the United States: A Decision Analytic Model. Ann. Intern. Med. 2019, 171, 785–795. [Google Scholar] [CrossRef]
- Ekers, D.; Webster, L.; Van Straten, A.; Cuijpers, P.; Richards, D.; Gilbody, S. Behavioural activation for depression; an update of meta-analysis of effectiveness and subgroup analysis. PLoS ONE 2014, 9, e100100. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, P. Explainer: What is Behavioural Activation for Depression? [Online] The Conversation. Available online: https://theconversation.com/explainer-what-is-behavioural-activation-for-depression-62910 (accessed on 5 July 2022).
- Dimidjian, S.; Barrera, M., Jr.; Martell, C.; Munoz, R.F.; Lewinsohn, P.M. The origins and current status of behavioral activation treatments for depression. Annu. Rev. Clin. Psychol. 2011, 7, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Martell, C.R.; Addis, M.E.; Jacobson, N.S. Depression in Context: Strategies for Guided Action; W W Norton & Co: New York, NY, USA, 2001. [Google Scholar]
- Richards, D.A.; Ekers, D.; McMillan, D.; Taylor, R.S.; Byford, S.; Warren, F.C.; Barrett, B.; Farrand, P.A.; Gilbody, S.; Kuyken, W.; et al. Cost and Outcome of Behavioural Activation versus Cognitive Behavioural Therapy for Depression (COBRA): A randomised, controlled, non-inferiority trial. Lancet 2016, 388, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D.; on behalf of the DEPRESsion Screening Data (DEPRESSD) EPDS Group. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef] [PubMed]
- Small, R.; Lumley, J.; Yelland, J.; Brown, S. The performance of the Edinburgh Postnatal Depression Scale in English speaking and non-English speaking populations in Australia. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- O’Mahen, H.A.; Woodford, J.; McGinley, J.; Warren, F.C.; Richards, D.A.; Lynch, T.R.; Taylor, R.S. Internet-based behavioral activation—Treatment for postnatal depression (Netmums): A randomized controlled trial. J. Affect. Disord. 2013, 150, 814–822. [Google Scholar] [CrossRef]
- Addis, M.E.; Martell, C.R. Overcoming Depression One Step at a Time: The New Behavioral Activation Approach to Getting Your Life Back; New Harbinger Press: New York, NY, USA, 2004. [Google Scholar]
- O’Mahen, H.; Fedock, G.; Henshaw, E.; Himle, J.A.; Forman, J.; Flynn, H.A. Modifying CBT for Perinatal Depression: What Do Women Want? Cogn. Behav. Pract. 2012, 19, 359–371. [Google Scholar] [CrossRef]
- O’Mahen, H.A.; Richards, D.A.; Woodford, J.; Wilkinson, E.; McGinley, J.; Taylor, R.S.; Warren, F.C. Netmums: A phase II randomized controlled trial of a guided Internet behavioural activation treatment for postpartum depression. Psychol. Med. 2014, 44, 1675–1689. [Google Scholar] [CrossRef] [PubMed]
- So, M.; Yamaguchi, S.; Hashimoto, S.; Sado, M.; Furukawa, T.A.; McCrone, P. Is computerised CBT really helpful for adult depression?—A meta-analytic re-evaluation of CCBT for adult depression in terms of clinical implementation and methodological validity. BMC Psychiatry 2013, 13, 113. [Google Scholar] [CrossRef] [PubMed]
- Rost, T.; Stein, J.; Lobner, M.; Kersting, A.; Luck-Sikorski, C.; Riedel-Heller, S.G. User Acceptance of Computerized Cognitive Behavioral Therapy for Depression: Systematic Review. J. Med. Internet Res. 2017, 19, e309. [Google Scholar] [CrossRef]
- Uphoff, E.; Ekers, D.; Robertson, L.; Dawson, S.; Sanger, E.; South, E.; Samaan, Z.; Richards, D.; Meader, N.; Churchill, R. Behavioural activation therapy for depression in adults. Cochrane Database Syst. Rev. 2020, 7, CD013305. [Google Scholar] [CrossRef]
- Steen, M.; Green, B. Mental health during pregnancy and parenthood. In Mental Health Across the Lifespan; Steen, M., Thomas, M., Eds.; Taylor & Francis Group: London, UK, 2015; pp. 60–87. [Google Scholar]
- Obikane, E.; Baba, T.; Shinozaki, T.; Obata, S.; Nakanishi, S.; Murata, C.; Ushio, E.; Suzuki, Y.; Shirakawa, N.; Honda, M.; et al. Internet-based behavioural activation to improve depressive symptoms and prevent child abuse in postnatal women (SmartMama): A protocol for a pragmatic randomized controlled trial. BMC Pregnancy Childbirth 2021, 21, 314. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yisma, E.; Walsh, S.; Steen, M.; Gray, R.; Dennis, S.; Gillam, M.; Parange, N.; Jones, M. Effect of Behavioral Activation for Women with Postnatal Depression: A Systematic Review and Meta-Analysis. Nurs. Rep. 2024, 14, 78-88. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep14010007
Yisma E, Walsh S, Steen M, Gray R, Dennis S, Gillam M, Parange N, Jones M. Effect of Behavioral Activation for Women with Postnatal Depression: A Systematic Review and Meta-Analysis. Nursing Reports. 2024; 14(1):78-88. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep14010007
Chicago/Turabian StyleYisma, Engida, Sandra Walsh, Mary Steen, Richard Gray, Shaun Dennis, Marianne Gillam, Nayana Parange, and Martin Jones. 2024. "Effect of Behavioral Activation for Women with Postnatal Depression: A Systematic Review and Meta-Analysis" Nursing Reports 14, no. 1: 78-88. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep14010007