
Early Female Transgender Identity after Prenatal Exposure to Diethylstilbestrol: Report from a French National Diethylstilbestrol (DES) Cohort

 ,
,
Abstract
:1. Introduction
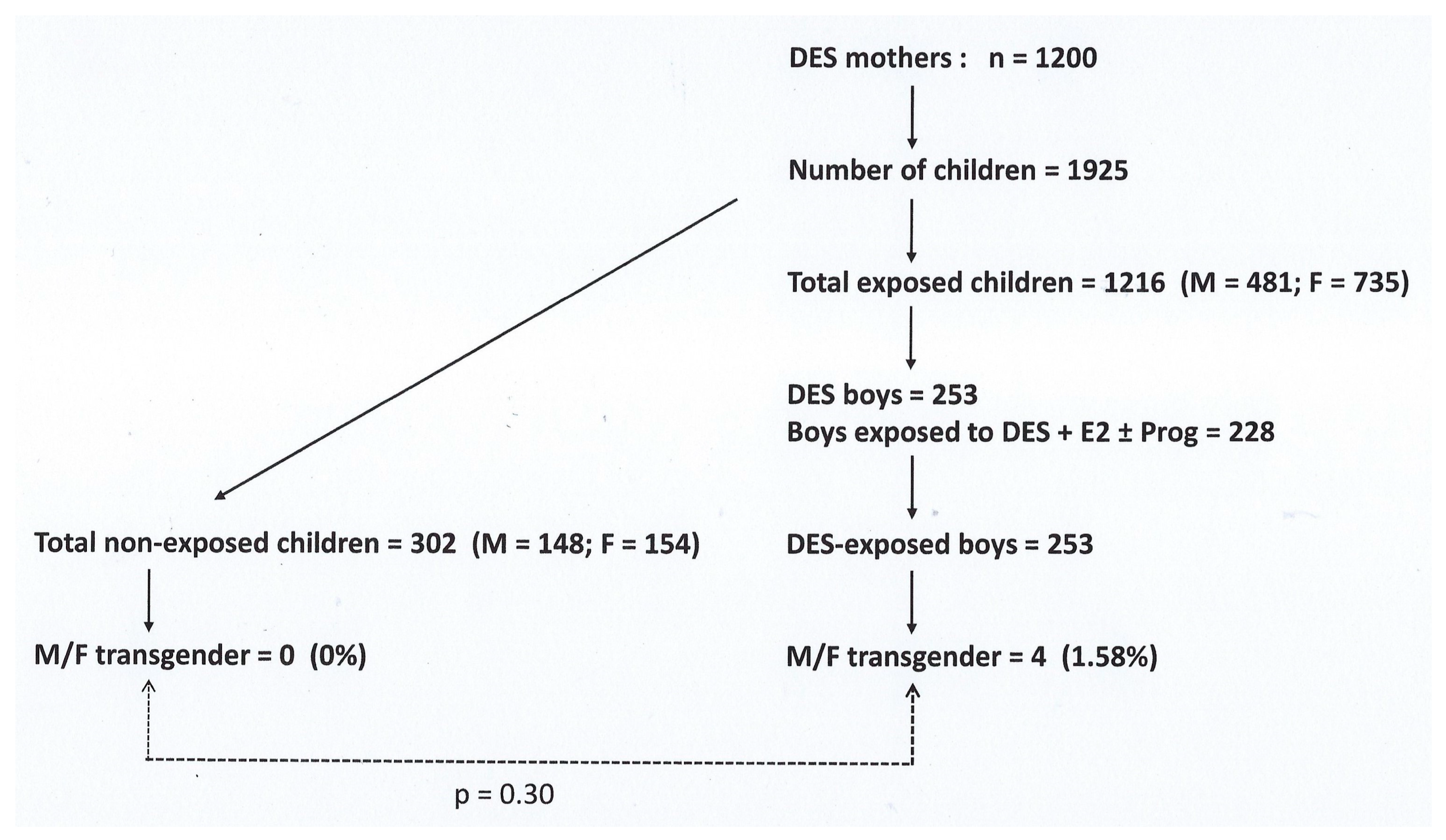
2. Patients and Methods
2.1. Patient 1 (M.) (Table 1, First Column)
2.2. Patient 2 (S.) (Table 1, Second Column)
2.3. Patient 3 (Chr.) (Table 1, Third Column)
2.4. Patient 4 (J.) (Table 1, Fourth Column)
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nguyen, H.B.; Loughead, J.; Lipner, E.; Hantsoo, L.; Kornfield, S.L.; Epperson, C.N. What has sex got to do with it? The role of hormones in the transgender brain. Neuropsychopharmacology 2019, 44, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Collin, L.; Reisner, S.L.; Tangpricha, V.; Goodman, M. Prevalence of Transgender Depends on the “Case” Definition: A Systematic Review. J. Sex. Med. 2016, 13, 613–626. [Google Scholar] [CrossRef]
- Bowman, S.J.; Hakeem, A.; Demant, D.; McAloon, J.; Wootton, B.M. Assessing Gender Dysphoria: Development and Validation of the Gender Preoccupation and Stability Questionnaire—2nd Edition (GPSQ-2). J. Homosex. 2022, 1–25. [Google Scholar] [CrossRef]
- T’Sjoen, G.; Arcelus, J.; Gooren, L.; Klink, D.T.; Tangpricha, V. Endocrinology of Transgender Medicine. Endocr. Rev. 2019, 40, 97–117. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Adams, N.; Corneil, T.; Kreukels, B.; Motmans, J.; Coleman, E. Size and Distribution of Transgender and Gender Nonconforming Populations: A Narrative Review. Endocrinol. Metab. Clin. N. Am. 2019, 48, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, D.E.; Gardner, M. Differences/Disorders of Sex Development: Medical Conditions at the Intersection of Sex and Gender. Annu. Rev. Clin. Psychol. 2022, 18, 201–231. [Google Scholar] [CrossRef]
- Arcelus, J.; Bouman, W.P.; Van Den Noortgate, W.; Claes, L.; Witcomb, G.; Fernandez-Aranda, F. Systematic review and meta-analysis of prevalence studies in transsexualism. Eur. Psychiatry 2015, 30, 807–815. [Google Scholar] [CrossRef]
- Hassler, T.; Glazier, J.J.; Olson, K.R. Consistency of gender identity and preferences across time: An exploration among cisgender and transgender children. Dev. Psychol. 2022, 58, 2184–2196. [Google Scholar] [CrossRef]
- Zucker, K.J. Epidemiology of gender dysphoria and transgender identity. Sex. Health 2017, 14, 404–411. [Google Scholar] [CrossRef]
- Zhang, Q.; Goodman, M.; Adams, N.; Corneil, T.; Hashemi, L.; Kreukels, B.; Motmans, J.; Snyder, R.; Coleman, E. Epidemiological considerations in transgender health: A systematic review with focus on higher quality data. Int. J. Transgend. Health 2020, 21, 125–137. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Sevelius, J.M. Transgender Population Size in the United States: A Meta-Regression of Population-Based Probability Samples. Am. J. Public Health 2017, 107, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Spizzirri, G.; Eufrasio, R.; Lima, M.C.P.; de Carvalho Nunes, H.R.; Kreukels, B.P.C.; Steensma, T.D.; Abdo, C.H.N. Proportion of people identified as transgender and non-binary gender in Brazil. Sci. Rep. 2021, 11, 2240. [Google Scholar] [CrossRef]
- Korpaisarn, S.; Safer, J.D. Etiology of Gender Identity. Endocrinol. Metab. Clin. N. Am. 2019, 48, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Hines, M. Neuroscience and Sex/Gender: Looking Back and Forward. J. Neurosci. 2020, 40, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Kiesow, H.; Dunbar, R.I.M.; Kable, J.W.; Kalenscher, T.; Vogeley, K.; Schilbach, L.; Marquand, A.F.; Wiecki, T.V.; Bzdok, D. 10,000 social brains: Sex differentiation in human brain anatomy. Sci. Adv. 2020, 6, eaaz1170. [Google Scholar] [CrossRef]
- Ristori, J.; Cocchetti, C.; Romani, A.; Mazzoli, F.; Vignozzi, L.; Maggi, M.; Fisher, A.D. Brain sex differences related to gender identity development: Genes or Hormones? Int. J. Mol. Sci. 2020, 21, 2123. [Google Scholar] [CrossRef]
- McCarthy, M.M. Origins of Sex Differentiation of Brain and Behavior. In Developmental Neuroendocrinology; Wray, S., Blackshaw, S., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 393–412. [Google Scholar]
- Swaab, D.F.; Wolff, S.E.C.; Bao, A.M. Sexual differentiation of the human hypothalamus: Relationship to gender identity and sexual orientation. Handb. Clin. Neurol. 2021, 181, 427–443. [Google Scholar]
- Corona, G.; Rastrelli, G.; Vignozzi, L.; Maggi, M. Androgens and male sexual function. Best Pract. Res. Clin. Endocrinol. Metab. 2022, 36, 101615. [Google Scholar] [CrossRef]
- Newbold, R.R. Lessons learned from perinatal exposure to diethylstilbestrol. Toxicol. Appl. Pharmacol. 2004, 199, 142–150. [Google Scholar] [CrossRef]
- Tournaire, M.; Epelboin, S.; Devouche, E. Histoire du diéthylstilbestrol. Therapie 2014, 69, 101–114. [Google Scholar] [CrossRef]
- Titus, L.; Hatch, E.E.; Drake, K.M.; Parker, S.E.; Hyer, M.; Palmer, J.R.; Strohsnitter, W.C.; Adam, E.; Herbst, A.L.; Huo, D.; et al. Reproductive and hormone-related outcomes in women whose mothers were exposed in utero to diethylstilbestrol (DES): A report from the US National Cancer Institute DES Third Generation Study. Reprod. Toxicol. 2019, 84, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Klip, H.; Verloop, J.; van Gool, J.D.; Koster, M.E.; Burger, C.W.; van Leeuwen, F.E.; Group, O.P. Hypospadias in sons of women exposed to diethylstilbestrol in utero: A cohort study. Lancet 2002, 359, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.R.; Herbst, A.L.; Noller, K.L.; Boggs, D.A.; Troisi, R.; Titus-Ernstoff, L.; Hatch, E.E.; Wise, L.A.; Strohsnitter, W.C.; Hoover, R.N. Urogenital abnormalities in men exposed to diethylstilbestrol in utero: A cohort study. Environ. Health 2009, 8, 37. [Google Scholar] [CrossRef]
- Kalfa, N.; Paris, F.; Soyer-Gobillard, M.O.; Daures, J.P.; Sultan, C. Prevalence of hypospadias in grandsons of women exposed to diethylstilbestrol during pregnancy: A multigenerational national cohort study. Fertil. Steril. 2011, 95, 2574–2577. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, H.E.; Adamsson, A. Cryptorchidism and endocrine disrupting chemicals. Mol. Cell. Endocrinol. 2012, 355, 208–220. [Google Scholar] [CrossRef]
- Soyer-Gobillard, M.O.; Paris, F.; Gaspari, L.; Courtet, P.; Sultan, C. Association between fetal DES-exposure and psychiatric disorders in adolescence/adulthood: Evidence from a French cohort of 1002 prenatally exposed children. Gynecol. Endocrinol. 2016, 32, 25–29. [Google Scholar] [CrossRef]
- Rivollier, F.; Chaumette, B.; Bendjemaa, N.; Chayet, M.; Millet, B.; Jaafari, N.; Barhdadi, A.; Lemieux Perreault, L.P.; Provost, S.; Dubé, M.P.; et al. Methylomic changes in individuals with psychosis, prenatally exposed to endocrine disrupting compounds: Lessons from diethylstilbestrol. PLoS ONE 2017, 12, e0174783. [Google Scholar] [CrossRef]
- Kioumourtzoglou, M.-A.; Coull, B.A.; O’Reilly, E.J.; Ascherio, A.; Weisskopf, M.G. Association of exposure to diethylstilbestrol during pregnancy with multigenerational neurodevelopmental deficits. JAMA Pediatr. 2018, 172, 670–677. [Google Scholar] [CrossRef]
- Deng, Q.; Hu, L.; Ding, Y.-Q.; Lang, B. Editorial: The commonality in converged pathways and mechanisms underpinning neurodevelopmental and psychiatric disorders. Front. Mol. Neurosci. 2023, 16, 1349631. [Google Scholar] [CrossRef]
- Tournaire, M.; Devouche, E.; Epelboin, S.; Cabau, A. Diethylstilbestrol exposure: Evaluation of the doses received in France. Eur. J. Epidemiol. 2012, 27, 315–318. [Google Scholar] [CrossRef]
- James, H.A.; Chang, A.Y.; Imhof, R.L.; Sahoo, A.; Montenegro, M.M.; Imhof, N.R.; Gonzalez, C.A.; Lteif, A.N.; Nippoldt, T.B.; Davidge-Pitts, C.J. A community-based study of demographics, medical and psychiatric conditions, and gender dysphoria/incongruence treatment in transgender/gender diverse individuals. Biol. Sex. Differ. 2020, 11, 55. [Google Scholar] [CrossRef]
- Wiepjes, C.M.; Nota, N.M.; de Blok, C.J.M.; Klaver, M.; de Vries, A.L.C.; Wensing-Kruger, S.A.; de Jongh, R.T.; Bouman, M.B.; Steensma, T.D.; Cohen-Kettenis, P.; et al. The Amsterdam Cohort of Gender Dysphoria Study (1972–2015): Trends in Prevalence, Treatment, and Regrets. J. Sex. Med. 2018, 15, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Loch Batista, R.; Inacio, M.; Prado Arnhold, I.J.; Gomes, N.L.; Diniz Faria, J.A.; Rodrigues de Moraes, D.; Frade Costa, E.M.; Domenice, S.; Bilharinho Mendonca, B. Psychosexual Aspects, Effects of Prenatal Androgen Exposure, and Gender Change in 46 XY Disorders of Sex Development. J. Clin. Endocrinol. Metab. 2019, 104, 1160–1170. [Google Scholar] [CrossRef]
- Stynes, H.; Lane, C.; Pearson, B.; Wright, T.; Ranieri, V.; Masic, U.; Kennedy, E. Gender identity development in children and young people: A systematic review of longitudinal studies. Clin. Child Psychol. Psychiatry 2021, 26, 706–719. [Google Scholar] [CrossRef] [PubMed]
- Soyer-Gobillard, M.O.; Gaspari, L.; Sultan, C. Evidence for a link between in utero exposure to synthetic estrogens and progestins and mental disorders. In Mental Disorders; Woolfolk, R., Allen, L., Eds.; IntechOpen Press: London, UK, 2019; pp. 1–20. [Google Scholar]
- Saleem, F.; Rizvi, S.W. Transgender Associations and Possible Etiology: A Literature Review. Cureus 2017, 9, e1984. [Google Scholar] [CrossRef] [PubMed]
- Foreman, M.; Hare, L.; York, K.; Balakrishnan, K.; Sanchez, F.J.; Harte, F.; Erasmus, J.; Vilain, E.; Harley, V.R. Genetic Link Between Gender Dysphoria and Sex Hormone Signaling. J. Clin. Endocrinol. Metab. 2019, 104, 390–396. [Google Scholar] [CrossRef]
- Ramirez, K.; Fernández, R.; Collet, S.; Kiyar, M.; Delgado-Zayas, E.; Gómez-Gil, E.; Van Den Eynde, T.; T’Sjoen, G.; Guillamon, A.; Mueller, S.C.; et al. Epigenetics Is Implicated in the Basis of Gender Incongruence: An Epigenome-Wide Association Analysis. Front. Neurosci. 2021, 15, 701017. [Google Scholar] [CrossRef]
- Folkierska-Zukowska, M.; Rahman, Q.; Marchewka, A.; Wypych, M.; Drozdziel, D.; Sokolowski, A.; Dragan, W.L. Male sexual orientation, gender nonconformity, and neural activity during mental rotations: An fMRI study. Sci. Rep. 2020, 10, 18709. [Google Scholar] [CrossRef]
- Votinov, M.; Goerlich, K.S.; Puiu, A.A.; Smith, E.; Nickl-Jockschat, T.; Derntl, B.; Habel, U. Brain structure changes associated with sexual orientation. Sci. Rep. 2021, 11, 5078. [Google Scholar] [CrossRef]
- Panzica, G.C.; Mura, E.; Miceli, D.; Martini, M.A.; Gotti, S.; Viglietti-Panzica, C. Effects of xenoestrogens on the differentiation of behaviorally relevant neural circuits in higher vertebrates. Ann. N. Y. Acad. Sci. 2009, 1163, 271–278. [Google Scholar] [CrossRef]
- Hernandez Scudder, M.E.; Young, R.L.; Thompson, L.M.; Kore, P.; Crews, D.; Hofmann, H.A.; Gore, A.C. EDCs Reorganize Brain-Behavior Phenotypic Relationships in Rats. J. Endocr. Soc. 2021, 5, bvab021. [Google Scholar] [CrossRef] [PubMed]
- Diamond, M. Transsexuality among Twins: Identity Concordance, Transition, Rearing, and Orientation. Int. J. Transgenderism 2013, 14, 24–38. [Google Scholar] [CrossRef]
- Sultan, C.; Gaspari, L.; Kalfa, N.; Paris, F. Chapter 16—Androgen insensitivity syndrome. In Genetic Steroid Disorders, 2nd ed.; New, M.I., Ed.; Academic Press: San Diego, CA, USA, 2023; pp. 327–341. [Google Scholar]
- Maimoun, L.; Philibert, P.; Cammas, B.; Audran, F.; Bouchard, P.; Fenichel, P.; Cartigny, M.; Pienkowski, C.; Polak, M.; Skordis, N.; et al. Phenotypical, biological, and molecular heterogeneity of 5α-reductase deficiency: An extensive international experience of 55 patients. J. Clin. Endocrinol. Metab. 2011, 96, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Sultan, C.; Lumbroso, S.; Paris, F.; Jeandel, C.; Terouanne, B.; Belon, C.; Audran, F.; Poujol, N.; Georget, V.; Gobinet, J.; et al. Disorders of androgen action. Semin. Reprod. Med. 2002, 20, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Kreukels, B.P.C.; Kohler, B.; Nordenstrom, A.; Roehle, R.; Thyen, U.; Bouvattier, C.; de Vries, A.L.C.; Cohen-Kettenis, P.T.; dsd-LIFE Group. Gender Dysphoria and Gender Change in Disorders of Sex Development/Intersex Conditions: Results From the dsd-LIFE Study. J. Sex. Med. 2018, 15, 777–785. [Google Scholar] [CrossRef]
- Zamora-Leon, P. Are the Effects of DES Over? A Tragic Lesson from the Past. Int. J. Environ. Res. Public Health 2021, 18, 10309. [Google Scholar] [CrossRef]
- Titus-Ernstoff, L.; Perez, K.; Hatch, E.E.; Troisi, R.; Palmer, J.R.; Hartge, P.; Hyer, M.; Kaufman, R.; Adam, E.; Strohsnitter, W.; et al. Psychosexual characteristics of men and women exposed prenatally to diethylstilbestrol. Epidemiology 2003, 14, 155–160. [Google Scholar] [CrossRef]
- Troisi, R.; Palmer, J.R.; Hatch, E.E.; Strohsnitter, W.C.; Huo, D.; Hyer, M.; Fredriksen-Goldsen, K.I.; Hoover, R.; Titus, L. Gender Identity and Sexual Orientation Identity in Women and Men Prenatally Exposed to Diethylstilbestrol. Arch. Sex. Behav. 2020, 49, 447–454. [Google Scholar] [CrossRef]
- Sohoni, P.; Sumpter, J.P. Several environmental oestrogens are also anti-androgens. J. Endocrinol. 1998, 158, 327–339. [Google Scholar] [CrossRef]
- La Merrill, M.A.; Vandenberg, L.N.; Smith, M.T.; Goodson, W.; Browne, P.; Patisaul, H.B.; Guyton, K.Z.; Kortenkamp, A.; Cogliano, V.J.; Woodruff, T.J.; et al. Consensus on the key characteristics of endocrine-disrupting chemicals as a basis for hazard identification. Nat. Rev. Endocrinol. 2020, 16, 45–57. [Google Scholar] [CrossRef]
- McKinnell, C.; Atanassova, N.; Williams, K.; Fisher, J.S.; Walker, M.; Turner, K.J.; Saunders, T.K.; Sharpe, R.M. Suppression of androgen action and the induction of gross abnormalities of the reproductive tract in male rats treated neonatally with diethylstilbestrol. J. Androl. 2001, 22, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Luders, E.; Sanchez, F.J.; Gaser, C.; Toga, A.W.; Narr, K.L.; Hamilton, L.S.; Vilain, E. Regional gray matter variation in male-to-female transsexualism. Neuroimage 2009, 46, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.C.; Guillamon, A.; Zubiaurre-Elorza, L.; Junque, C.; Gomez-Gil, E.; Uribe, C.; Khorashad, B.S.; Khazai, B.; Talaei, A.; Habel, U.; et al. The Neuroanatomy of Transgender Identity: Mega-Analytic Findings from the ENIGMA Transgender Persons Working Group. J. Sex. Med. 2021, 18, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Joel, D. Beyond the binary: Rethinking sex and the brain. Neurosci. Biobehav. Rev. 2021, 122, 165–175. [Google Scholar] [CrossRef]
- Zhou, J.N.; Hofman, M.A.; Gooren, L.J.; Swaab, D.F. A sex difference in the human brain and its relation to transsexuality. Nature 1995, 378, 68–70. [Google Scholar] [CrossRef]
- Garcia-Falgueras, A.; Swaab, D.F. A sex difference in the hypothalamic uncinate nucleus: Relationship to gender identity. Brain 2008, 131, 3132–3146. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Data | Patient | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| (A) During childhood | ||||
| Strong desire to be female | X | X | X | X |
| Strong preference for wearing female clothes | X | X | X | X |
| Strong preference for cross-gender role in make-believe play or fantasy play | X | X | X | X |
| Strong preference for toys, games or activities stereotypically used or engaged in by the female gender | X | 0 | 0 | 0 |
| Strong preference for playmates of female gender | 0 | X | X | X |
| Strong rejection of toys, games and activities typical of the male gender | 0 | 0 | 0 | 0 |
| Strong dislike of one’s sexual anatomy | X | X | X | X |
| Strong desire for the physical sex characteristics that match one’s experienced gender | X | 0 | 0 | X |
| (B) During puberty/adolescence | ||||
| Experiencing the wrong puberty for transgender youth | 0 | X | X | X |
| Self-mutilation (external genitalia) | X | 0 | 0 | 0 |
| Vulnerability | X | X | X | X |
| Mood disorders | X | X | X | X |
| Depression/anxiety | 0 | 0 | 0 | X |
| Maladaptive coping | X | X | X | X |
| Suicidality | 0 | 0 | 0 | 0 |
| Psychiatric hospitalization | 0 | 0 | 0 | 0 |
| Institutional discrimination | X | X | 0 | X |
| Economic marginalization | X | X | 0 | X |
| Social isolation | X | X | 0 | X |
| Risk of drug abuse | 0 | 0 | 0 | 0 |
| Violence | 0 | 0 | 0 | X |
| Homelessness | 0 | 0 | 0 | 0 |
| (C) In adulthood | ||||
| Gender-affirming surgery | X | X | X | 0 |
| Gender-Affirming Hormone Therapy | X | X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspari, L.; Soyer-Gobillard, M.-O.; Kerlin, S.; Paris, F.; Sultan, C. Early Female Transgender Identity after Prenatal Exposure to Diethylstilbestrol: Report from a French National Diethylstilbestrol (DES) Cohort. J. Xenobiot. 2024, 14, 166-175. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010010
Gaspari L, Soyer-Gobillard M-O, Kerlin S, Paris F, Sultan C. Early Female Transgender Identity after Prenatal Exposure to Diethylstilbestrol: Report from a French National Diethylstilbestrol (DES) Cohort. Journal of Xenobiotics. 2024; 14(1):166-175. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010010
Chicago/Turabian StyleGaspari, Laura, Marie-Odile Soyer-Gobillard, Scott Kerlin, Françoise Paris, and Charles Sultan. 2024. "Early Female Transgender Identity after Prenatal Exposure to Diethylstilbestrol: Report from a French National Diethylstilbestrol (DES) Cohort" Journal of Xenobiotics 14, no. 1: 166-175. https://0-doi-org.brum.beds.ac.uk/10.3390/jox14010010