Effects of a Multicomponent Exercise Program, a Detraining Period and Dietary Intake Prediction of Body Composition of Frail and Pre-Frail Older Adults from the EXERNET Elder 3.0 Study

 , ,
, ,  , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
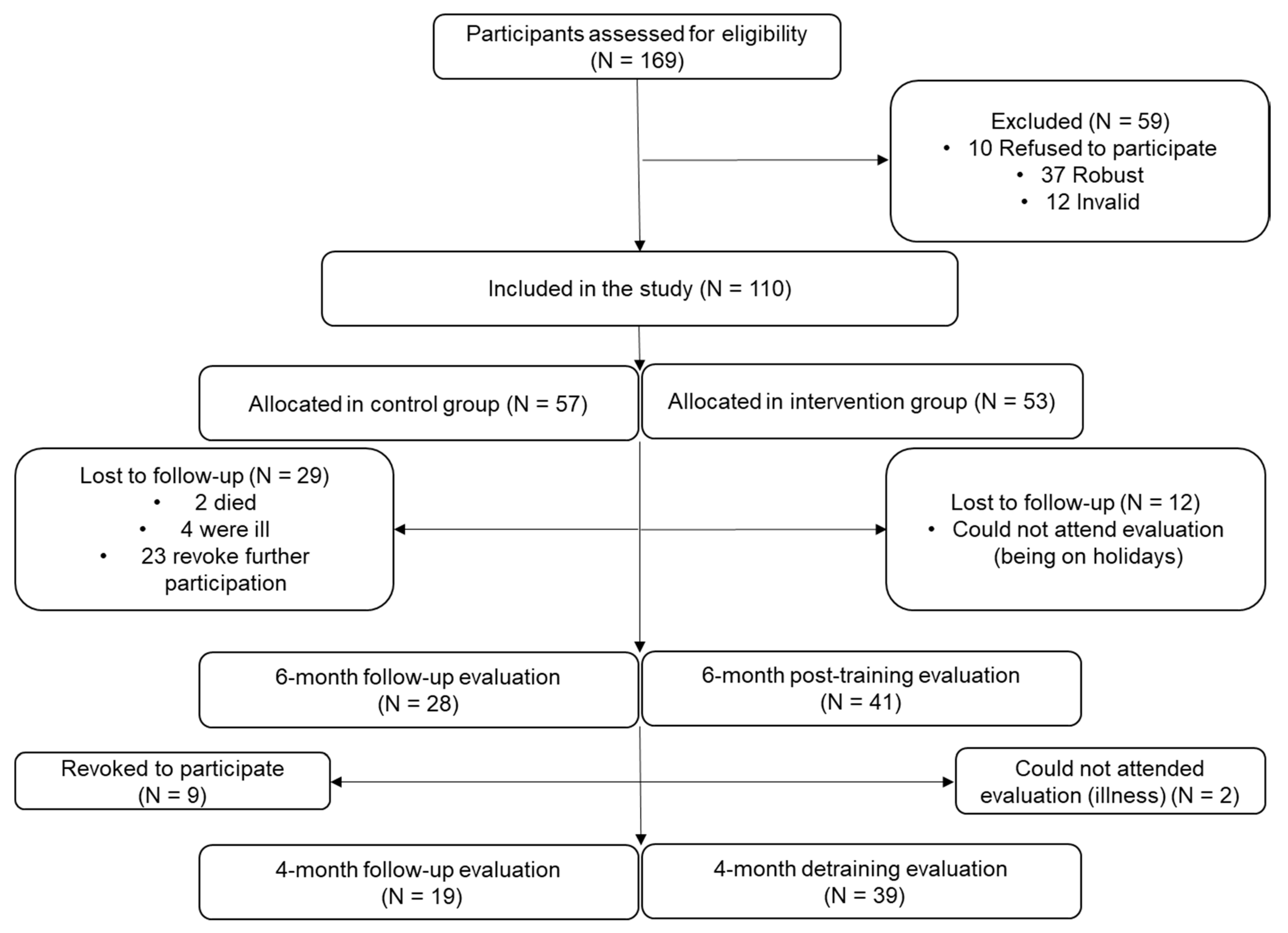
2.1. Study Design and Participants
2.2. The EXERNET Elder 3.0 Multicomponent Exercise Program
2.3. Short Physical Performance Battery (SPPB)
2.4. Anthropometric Measurements
2.4.1. Height
2.4.2. Waist and Hip Circumference
2.5. Body Composition Measurements
2.6. Dietary Intake
2.7. Statistical Analysis
3. Results
Effects of the Exercise Program and the Detraining Period on Body Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gómez-Cabello, A.; Vicente-Rodríguez, G.; Vila-Maldonado, S.; Casajús, J.A.; Ara, I. Aging and body composition: The sarcopenic obesity in Spain. Nutr. Hosp. 2012, 27, 22–30. [Google Scholar] [PubMed]
- Goodpaster, B.H.; Krishnaswami, S.; Harris, T.B.; Katsiaras, A.; Kritchevsky, S.B.; Simonsick, E.M.; Nevitt, M.; Holvoet, P.; Newman, A.B. Obesity, Regional Body Fat Distribution, and the Metabolic Syndrome in Older Men and Women. Arch. Intern. Med. 2005, 165, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajek, A.; Bock, J.-O.; Saum, K.-U.; Matschinger, H.; Brenner, H.; Holleczek, B.; Haefeli, W.E.; Heider, D.; König, H.-H. Frailty and healthcare costs—longitudinal results of a prospective cohort study. Age Ageing 2018, 47, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, Q.-L. The Frailty Syndrome: Definition and Natural History. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Reinders, I.; Visser, M.; Schaap, L. Body weight and body composition in old age and their relationship with frailty. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 11–15. [Google Scholar] [CrossRef] [Green Version]
- São-Romão-Preto, L.; Conceição, M.D.C.D.; Figueiredo, T.M.; Mata, M.A.P.; Preto, P.M.B.; Aguilar, E.M. Frailty, body composition and nutritional status in non-institutionalised elderly. Enfermería Clín. (Engl. Ed.) 2017, 27, 339–345. [Google Scholar] [CrossRef]
- Kelaiditi, E.; van Kan, G.A.; Cesari, M. Frailty: Role of nutrition and exercise. Curr. Opin. Clin. Nutr. Metab. Care. 2014, 17, 32–39. [Google Scholar] [CrossRef]
- Toraman, N.F.; Şahin, G. Age responses to multicomponent training programme in older adults. Disabil. Rehabil. 2004, 26, 448–454. [Google Scholar] [CrossRef]
- Marques, M.C.; Zajac, A.; Pereira, A.; Costa, A.M. Strength Training and Detraining in Different Populations: Case Studies. J. Hum. Kinet. 2011, 29, 7–14. [Google Scholar] [CrossRef]
- Bouaziz, W.; Lang, P.O.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Vogel, T. Health benefits of multicomponent training programmes in seniors: A systematic review. Int. J. Clin. Pr. 2016, 70, 520–536. [Google Scholar] [CrossRef]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy Balance and Obesity. Circuits 2012, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- San-Cristobal, R.; Navas-Carretero, S.; Martínez-González, M.A.; Ordovás, J.M.; Martínez, J.A. Contribution of macronutrients to obesity: Implications for precision nutrition. Nat. Rev. Endocrinol. 2020, 16, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Esain, I.; Rodriguez-Larrad, A.; Bidaurrazaga-Letona, I.; Gil, S.M. Health-related quality of life, handgrip strength and falls during detraining in elderly habitual exercisers. Health Qual. Life Outcomes 2017, 15, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-García, Á.I.; Gómez-Cabello, A.; Moradell, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Ara, I.; Pedrero-Chamizo, R.; Subías-Perié, J.; Muniz-Pardos, B.; Casajús, J.A.; et al. How to Improve the Functional Capacity of Frail and Pre-Frail Elderly People? Health, Nutritional Status and Exercise Intervention. The EXERNET-Elder 3.0 Project. Sustainability 2020, 12, 6246. [Google Scholar] [CrossRef]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef]
- López-Rodríguez, C.; Laguna, M.; Gómez-Cabello, A.; Gusi, N.; Espino, L.; Villa, G.; Pedrero-Chamizo, R.; Casajus, J.; Ara, I.; Aznar, S. Validation of the self-report EXERNET questionnaire for measuring physical activity and sedentary behavior in elderly. Arch. Gerontol. Geriatr. 2017, 69, 156–161. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, A.E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Guigoz, P.Y.; Vellas, M.B.; Garry, P.P.J. Assessing the Nutritional Status of the Elderly: The Mini Nutritional Assessment as Part of the Geriatric Evaluation. Nutr. Rev. 2009, 54, S59–S65. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L.T. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefsroom, South Africa, 2011. [Google Scholar]
- Martín-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ballarth, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.; Salas-Salvado, J.; Martin-Moreno, J. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Los Alimentos. GUÍA de Prácticas; Pirámide, E., Ed.; Piramide: Madrid, Spain, 2015. [Google Scholar]
- Mataix, J. Tabla de Composición de Alimentos, 5th ed.; Universidad de Granada: Granada, Spain, 2009. [Google Scholar]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villareal, D.T.; Smith, G.I.; Sinacore, D.R.; Shah, K.; Mittendorfer, B. Regular Multicomponent Exercise Increases Physical Fitness and Muscle Protein Anabolism in Frail, Obese, Older Adults. Obesity 2011, 19, 312–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Molina, R.; Ruíz-Grao, M.C.; García, A.N.; Reig, M.M.; Víctor, M.E.; Izquierdo, M.; Abizanda, P.; Redín, M.I.; Abizanda, P. Benefits of a multicomponent Falls Unit-based exercise program in older adults with falls in real life. Exp. Gerontol. 2018, 110, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodriguez-Mañas, L.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. AGE 2014, 36, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Sousa, N.; Mendes, R. Effects of Resistance Versus Multicomponent Training on Body Composition and Functional Fitness in Institutionalized Elderly Women. J. Am. Geriatr. Soc. 2013, 61, 1815–1817. [Google Scholar] [CrossRef]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J. Appl. Physiol. 2002, 93, 1318–1326. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Ota, N.; Shimotoyodome, A.; Hase, T.; Hosoi, E.; Yoshida, H. Effects of Exercise and Milk Fat Globule Membrane (MFGM) Supplementation on Body Composition, Physical Function, and Hematological Parameters in Community-Dwelling Frail Japanese Women: A Randomized Double Blind, Placebo-Controlled, Follow-Up Trial. PLoS ONE 2015, 10, e0116256. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L. Strength and Endurance Training Prescription in Healthy and Frail Elderly. Aging Dis. 2014, 5, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Stathokostas, L.; Roland, K.P.; Jakobi, J.M.; Patterson, C.; Vandervoort, A.A.; Jones, G.R. The Effectiveness of Exercise Interventions for the Management of Frailty: A Systematic Review. J. Aging Res. 2011, 2011, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starr, K.N.P.; McDonald, S.R.; Bales, C.W. Obesity and Physical Frailty in Older Adults: A Scoping Review of Lifestyle Intervention Trials. J. Am. Med. Dir. Assoc. 2014, 15, 240–250. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.C.; Harhay, M.O. Appendicular lean mass and mortality among prefrail and frail older adults. J. Nutr. Health Aging 2017, 21, 342–345. [Google Scholar] [CrossRef]
- Kelly, O.J.; Gilman, J.C.; Boschiero, D.; Ilich, J.Z. Osteosarcopenic Obesity: Current Knowledge, Revised Identification Criteria and Treatment Principles. Nutrients 2019, 11, 747. [Google Scholar] [CrossRef] [Green Version]
- Cadore, E.L.; Moneo, A.B.B.; Mensat, M.M.; Muñoz, A.R.; Casas-Herrero, A.; Rodriguez-Mañas, L.; Izquierdo, M. Positive effects of resistance training in frail elderly patients with dementia after long-term physical restraint. AGE 2013, 36, 801–811. [Google Scholar] [CrossRef]
- Ratel, S.; Gryson, C.; Rance, M.; Penando, S.; Bonhomme, C.; Le Ruyet, P.; Duclos, M.; Boirie, Y.; Walrand, S. Detraining-induced alterations in metabolic and fitness markers after a multicomponent exercise-training program in older men. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2012, 37, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Anton, S.D.; Hida, A.; Mankowski, R.; Layne, A.; Solberg, L.M.; Mainous, A.G.; Buford, T. Nutrition and Exercise in Sarcopenia. Curr. Protein Pept. Sci. 2018, 19, 649–667. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef]
- Vergnaud, A.-C.; Norat, T.; Mouw, T.; Romaguera, D.; May, A.M.; Bueno-De-Mesquita, H.B.; Van Der A, D.; Agudo, A.; Wareham, N.; Khaw, K.-T.; et al. Macronutrient Composition of the Diet and Prospective Weight Change in Participants of the EPIC-PANACEA Study. PLoS ONE 2013, 8, e57300. [Google Scholar] [CrossRef] [Green Version]
- Kang, L.; Gao, Y.; Liu, X.; Liang, Y.; Chen, Y.; Liang, Y.; Zhang, L.; Chen, W.; Pang, H.; Peng, L.-N. Effects of whey protein nutritional supplement on muscle function among community-dwelling frail older people: A multicenter study in China. Arch. Gerontol. Geriatr. 2019, 83, 7–12. [Google Scholar] [CrossRef]
- Sun, Y.; You, W.; Almeida, F.A.; Estabrooks, P.; Davy, B.M. The Effectiveness and Cost of Lifestyle Interventions Including Nutrition Education for Diabetes Prevention: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2017, 117, 404–421.e36. [Google Scholar] [CrossRef] [Green Version]
- Safer, U.; Tasci, I.; Safer, V.B.; Doruk, H. Is segmental bioelectrical impedance analysis a valid tool to assess muscle mass in the elderly? Geriatr. Gerontol. Int. 2013, 13, 1085–1086. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Control (n = 57) | Training (n = 53) |
|---|---|---|
| Age (year) | 80.4 ± 5.6 | 80.9 ± 6.1 |
| Sex | ||
| Male | 14 (24.6) | 18 (34.0) |
| Female | 43 (75.4) | 35 (66.0) |
| SPPB-Frailty status | ||
| Frail | 16 (28.1) | 14 (26.4) |
| Pre-frail | 41 (71.9) | 39 (73.6) |
| Walking hours per day | 1.13 ± 0.9 | 1.9 ± 1.4 |
| Sitting hours | 6.3± 2.3 | 6.2± 3.0 |
| Smoke | ||
| Yes | 4 (7.0) | 1 (1.9) |
| No | 51 (89.5) | 52 (98.1) |
| IADL groups | ||
| Moderate dependence | 10 (17.5) | 5 (9.4) |
| Mild dependence | 9 (15.8) | 14 (26.4) |
| Completely autonomy | 38 (66.6) | 34 (64.1) |
| Barthel Index | ||
| Moderate dependent | 1 (1.7) | 0 (0.0) |
| Mild dependent | 28 (49.1) | 20 (37.7) |
| Independent | 28 (49.1) | 33 (62.2) |
| MNA | ||
| Malnourished | 6 (11.3) | 2 (4.0) |
| At risk of malnutrition | 12 (22.6) | 14 (28.0) |
| Normal nutritional status | 35 (66.0) | 34 (68.0) |
| 6 Months Training | 4 Months Detraining | Total 10 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CON (n = 28) | TRAIN (n = 43) | p Value | CON (n = 19) | TRAIN (n = 39) | p Value | CON (n = 17) | TRAIN (n = 43) | p Value | |
| Weight (kg) | −0.03 ± 0.40 | −0.57 ± 0.33 | 0.278 | 0.26 ± 0.35 | 0.14 ± 0.24 | 0.691 | 0.14 ± 0.61 | −0.61 ± 0.39 | 0.309 |
| BMI (kg/m2) | −0.07 ± 0.18 | −0.29 ± 0.14 * | 0.246 | 0.19 ± 0.15 | 0.06 ± 0.10 | 0.570 | 0.01 ± 0.29 | −0.23 ± 0.18 | 0.496 |
| FM (kg) | −0.20 ± 0.42 | −0.86 ± 0.38 * | 0.180 | 0.39 ± 0.53 | 1.07 ± 0.30 * | 0.421 | 0.59 ± 0.53 | 0.11 ± 0.33 | 0.447 |
| FFM (kg) | 0.13 ± 0.38 | 0.43 ± 0.30 | 0.511 | −0.64 ± 0.39 | −0.90 ± 0.30 * | 0.618 | −0.40 ± 0.42 | −0.75 ± 0.26 * | 0.491 |
| BF% | −0.18 ± 0.45 | −0.98 ± 0.36 * | 0.144 | 1.32 ± 0.47 * | 1.43 ± 0.31 * | 0.895 | 0.84 ± 0.56 | 0.50 ± 0.35 | 0.606 |
| Waist Cir (cm) | 3.20 ± 1.41 * | 3.04 ± 1.15 * | 0.787 | 0.51 ± 2.07 | 3.92 ± 1.38 * | 0.184 | 4.08 ± 0.95 | 5.08 ± 1.04 | 0.487 |
| Hip Cir (cm) | 3.06 ± 1.22 * | 1.66 ± 0.85 | 0.252 | −0.50 ± 0.81 | −1.06 ± 0.55 | 0.719 | 1.80 ± 1.38 | 1.26 ± 0.82 | 0.736 |
| CONTROL | TRAINING | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training (n = 28) | Detraining (n = 19) | Training (n = 41) | Detraining (n = 39) | ||||||||||||||
| Total Energy (kcal) | CH (%) | Fat (%) | Prot (%) | Total Energy (kcal) | CH (%) | Fat (%) | Prot (%) | Total Energy (kcal) | CH (%) | Fat (%) | Prot (%) | Total Energy (kcal) | CH (%) | Fat (%) | Prot (%) | ||
| Weigh (kg) | β standardized | −0.081 | 0.127 | −0.122 | 0.046 | −0.048 | −0.377 | 0.321 | 0.022 | −0.005 | −0.104 | 0.149 | −0.166 | 0.108 | 0.074 | −0.220 | 0.269 |
| p value | 0.653 | 0.482 | 0.499 | 0.801 | 0.824 | 0.069 | 0.127 | 0.918 | 0.974 | 0.495 | 0.328 | 0.275 | 0.506 | 0.649 | 0.172 | 0.093 | |
| BMI (kg/m2) | β standardized | −0.058 | 0.166 | −0.166 | 0.012 | −0.063 | −0.513 | 0.395 | 0.166 | 0.108 | −0.116 | 0.178 | −0.190 | 0.029 | 0.090 | −0.300 | 0.461 |
| p value | 0.769 | 0.399 | 0.399 | 0.953 | 0.792 | 0.021 | 0.085 | 0.484 | 0.538 | 0.507 | 0.306 | 0.274 | 0.874 | 0.618 | 0.090 | 0.007 | |
| FM (kg) | β standardized | 0.182 | 0.288 | 0.106 | −0.023 | −0.476 | 0.077 | −0.125 | 0.017 | −0.147 | −0.202 | −0.099 | −0.169 | 0.338 | −0.101 | 0.099 | −0.070 |
| p value | 0.327 | 0.116 | 0.571 | 0.904 | 0.019 | 0.719 | 0.561 | 0.938 | 0.347 | 0.194 | 0.526 | 0.278 | 0.035 | 0.542 | 0.550 | 0.671 | |
| FFM (kg) | β standardized | −0.252 | −0.191 | −0.209 | −0.006 | 0.320 | −0.459 | −0.209 | 0.016 | 0.001 | 0.186 | 0.147 | 0.053 | −0.204 | 0.068 | −0.220 | 0.313 |
| p value | 0.171 | 0.304 | 0.259 | 0.974 | 0.128 | 0.024 | 0.259 | 0.940 | 0.515 | 0.232 | 0.347 | 0.736 | 0.212 | 0.679 | 0.178 | 0.052 | |
| BF% | β standardized | 0.182 | −0.191 | 0.106 | −0.203 | −0.529 | 0.321 | 0.002 | −0.341 | −0.147 | 0.186 | −0.099 | −0.169 | 0.330 | −0.136 | 0.187 | −0.172 |
| p value | 0.327 | 0.304 | 0.571 | 0.904 | 0.008 | 0.126 | 0.991 | 0.103 | 0.347 | 0.232 | 0.526 | 0.278 | 0.040 | 0.408 | 0.262 | 0.294 | |
| Waist Cir (cm) | β standardized | 0.058 | −0.018 | 0.063 | −0.083 | 0.299 | 0.100 | −0.089 | −0.028 | 0.038 | −0.107 | 0.210 | −0.167 | 0.041 | 0.211 | −0.236 | 0.098 |
| p value | 0.780 | 0.930 | 0.761 | 0.688 | 0.166 | 0.649 | 0.687 | 0.901 | 0.832 | 0.533 | 0.242 | 0.353 | 0.798 | 0.184 | 0.138 | 0.543 | |
| Hip Cir (cm) | β standardized | −0.436 | 0.245 | 0.106 | −0.093 | 0.113 | −0.239 | 0.258 | −0.132 | 0.074 | 0.303 | −0.099 | −0.093 | −0.077 | −0.226 | 0.184 | 0.138 |
| p value | 0.048 | 0.284 | 0.571 | 0.688 | 0.617 | 0.285 | 0.245 | 0.557 | 0.670 | 0.072 | 0.526 | 0.590 | 0.643 | 0.166 | 0.262 | 0.401 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moradell, A.; Navarrete-Villanueva, D.; Fernández-García, Á.I.; Sagarra-Romero, L.; Marín-Puyalto, J.; Pérez-Gómez, J.; Gesteiro, E.; Ara, I.; Casajus, J.A.; Gómez-Cabello, A.; et al. Effects of a Multicomponent Exercise Program, a Detraining Period and Dietary Intake Prediction of Body Composition of Frail and Pre-Frail Older Adults from the EXERNET Elder 3.0 Study. Sustainability 2020, 12, 9894. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239894
Moradell A, Navarrete-Villanueva D, Fernández-García ÁI, Sagarra-Romero L, Marín-Puyalto J, Pérez-Gómez J, Gesteiro E, Ara I, Casajus JA, Gómez-Cabello A, et al. Effects of a Multicomponent Exercise Program, a Detraining Period and Dietary Intake Prediction of Body Composition of Frail and Pre-Frail Older Adults from the EXERNET Elder 3.0 Study. Sustainability. 2020; 12(23):9894. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239894
Chicago/Turabian StyleMoradell, Ana, David Navarrete-Villanueva, Ángel Iván Fernández-García, Lucía Sagarra-Romero, Jorge Marín-Puyalto, Jorge Pérez-Gómez, Eva Gesteiro, Ignacio Ara, Jose Antonio Casajus, Alba Gómez-Cabello, and et al. 2020. "Effects of a Multicomponent Exercise Program, a Detraining Period and Dietary Intake Prediction of Body Composition of Frail and Pre-Frail Older Adults from the EXERNET Elder 3.0 Study" Sustainability 12, no. 23: 9894. https://0-doi-org.brum.beds.ac.uk/10.3390/su12239894