1. Introduction
The relationship between built environment and health-related conditions (such as physical activity, obesity, and cardiovascular disease) have been extensively discussed in previous studies [
1,
2,
3]. Although the sustainable built environment is a multidimensional concept, the literature defines it through particular measures including the urban density and intensity of activities, diversity of land use, street network design, aesthetic qualities, and transportation facilities [
4]. Neighborhood walkability, street connectivity, density, and mixed land use are associated with higher walking trips and physical activities [
5,
6,
7] and can reduce the risk of cardiovascular disease [
8,
9]. Built environment attributes including density, diversity of land use, availability of destinations, and distance to transit can explain physical activity-related improvements in mortality and morbidity [
10].
However, the evaluation of built environment attributes on cancer outcomes is a relatively novel arena that has not been extensively discussed in cancer-related research. Notably, a few studies discuss the role of residential neighborhoods on the level of physical activities and body mass of cancer patients [
11,
12,
13,
14], while a majority of literature focuses on the effects of geographical accessibility and distance to cancer care providers on cancer outcomes [
15,
16]. Meanwhile, some studies focus on the spatial cluster analysis of cancer-risk factors and suggest that the number of new cancer incidences is higher in metropolitan areas exposed to a high levels of air pollution when compared to less polluted geographical clusters [
17].
The impact of built environment on primary and secondary cancer prevention can be investigated in four thematic areas of interest, including spatial proximity, transportation, land use, and housing [
18]. Nonetheless, pioneer studies often concentrate on the spatial proximity and centralization of cancer care services in medical centers and large hospitals. This line of research investigates the travel burden to low-income and transit-oriented cancer patients dwelling in remote areas [
19,
20,
21,
22,
23]. The previous studies often have utilized the neighborhood built environments to justify the health-related outcomes between different ethnicities (such as overweight and obesity) among cancer survivors [
24,
25] to mediate the relationships between the cancer risk and the socioeconomic status of the patients [
14,
24,
25]. Access to neighborhood amenities such as recreational facilities, parks, and beaches have been demonstrated to contribute to the physical activity recommended by the American Cancer Society and improve cancer outcomes [
14]. Moreover, a few scholars propose that population density has an influence on cancer mortality [
14,
15,
26,
27]. It seems that living in more densely populated neighborhoods is associated with higher risks of cancer incidents and poorer overall survival.
On the other hand, it is suggested that a supportive built environment can overcome the barriers in the outdoor environment and improve perceived quality of life (QoL) [
28,
29]. Notably, QoL, especially health-related QoL, denotes a broad-ranging concept with complex impacts related to physical health, psychological state, personal beliefs, social relationships, and a person’s relationship to salient features of their environment [
30]. Analyzing cancer survivors indicates that micro-environmental conditions can affect their level of physical exercise and, consequently, the cancer patients’ quality of life [
31]. Although evidence reveals that built environment characteristics promote physical activities, physical wellbeing, social interaction in the community, and mental health, the impacts of built environment on QoL is less recognized. Living in pedestrian-friendly neighborhoods with mixed-land use and well-designed green areas is associated with higher levels of self-reported wellbeing and mental health [
32]. Examining the perceived neighborhood characteristics on health-related quality of life (HRQOL) reveals that perception of diversity, safety, and esthetics are associated with the higher physical and mental wellbeing of residents [
33].
Contrary to the limited numbers of cancer studies investigating QoL and the built environment, several studies have been developed to understand how cancer experiences impact patients’ QoL as a multidimensional construct. Cancer types, pain intensity [
34], and cancer treatment [
35] have been identified as the most significant factors. Sociodemographic features and social supports, on the other hand, are also commonly considered as determinants of cancer patients’ QoL [
36,
37,
38]. Evidence indicates that the QoL in cancer patients can be affected by race [
39], age at diagnosis [
40], access to health providers [
41], and social support [
42]. Some studies suggest that the association between the socioeconomic status of neighborhoods (such as race and ethnicity) and QoL result in health disparities in geographical areas [
43]. It is deemed that performing physical activity such as walking and exercise interventions is significantly related to a higher QoL for patients with cancer history [
44,
45,
46,
47].
To the best of our knowledge, the impact of built environment attributes on cancer patients’ QoL has not been fully explored in the literature, and only a few studies have explored the relationships between neighborhood environments and QoL in urban settings [
48]. Although little effort has been made to understand the effects of physical features such as access to goods and services on cancer survival through physical activities [
14,
25], the literature has not sufficiently explored the associations between built environment and QoL among the cancer patients. To our knowledge, these associations have not been investigated in the literature. Understanding the factors shaping patients’ QoL can help public health planners to recognize vulnerable groups of patients who require further support interventions and provide appropriate services to cancer survivors [
49].
The growing need to develop sustainability in cities points to the importance of health and wellbeing in shaping sustainable communities. Researchers suggest a close association between QoL and environmental sustainability. Accordingly, in addition to measuring sustainability indicators, measuring and tracking the QoL of urban residents could be regarded as a critical goal of city planners and policymakers [
50]. Moreover, the satisfaction of city residents regarding environmental sustainability indicators such as green spaces, air quality, noise level, cleanliness, and climate change can increase city livability and QoL [
51]. Accordingly, investigating the effects of built environment factors on QoL can be regarded as an effort to understand the environmental sustainability concept.
This study aims to identify the factors that contribute to the QoL of people who struggle with cancer while considering a comprehensive set of internal and external factors. Accordingly, we address the following research questions: (1) How do built environment attributes along with health-related and sociodemographics shape the self-reporting QoL of cancer patients? and (2) What are the most influential factors associated with patients’ QoL?
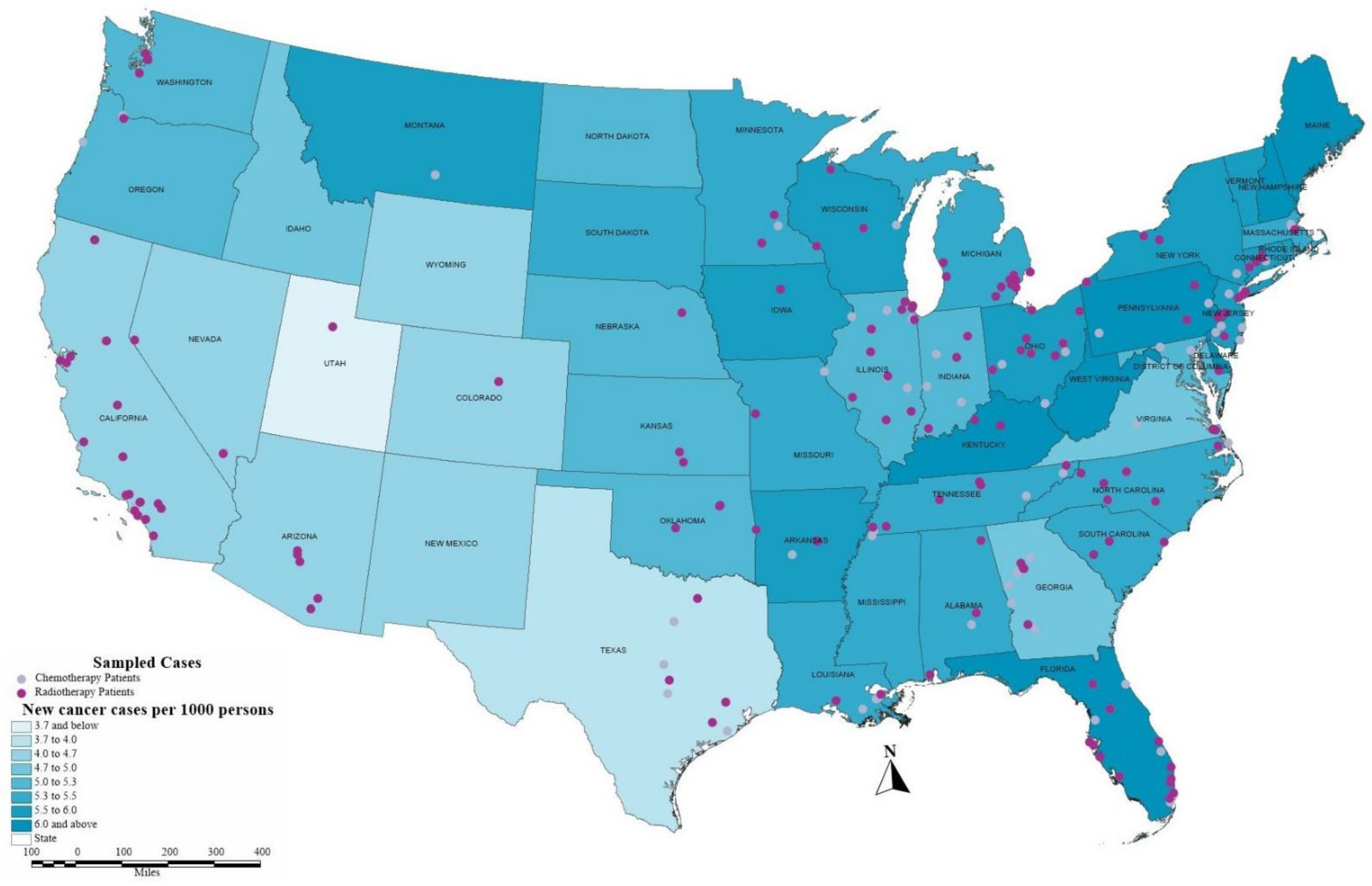
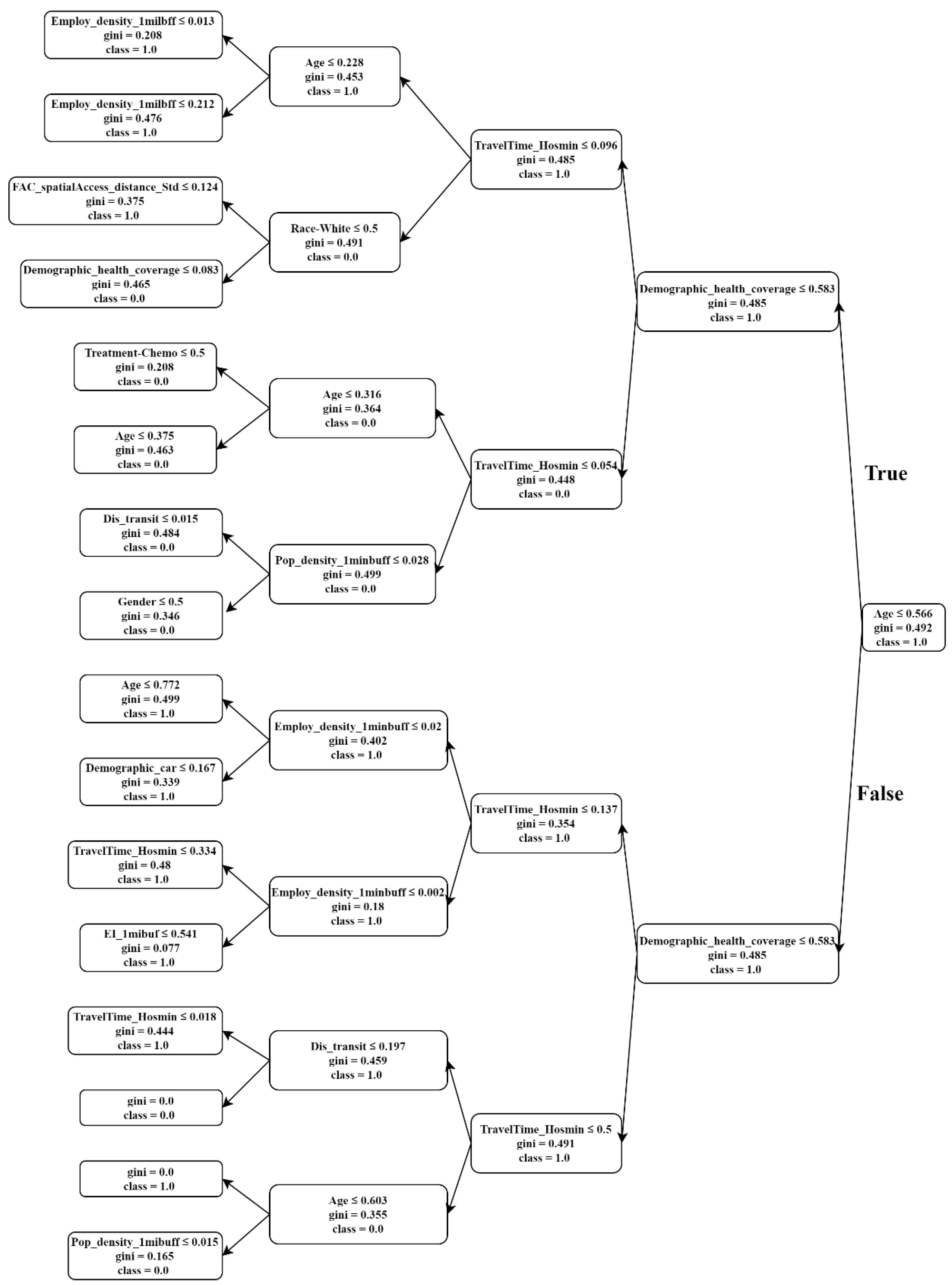
To fulfill the research gap, the present study designs a comprehensive survey to collect data from cancer patients across the US systematically. We explore the effects of built environment attributes by considering objective and actual measures as well as the subjective and perceptional factors. Furthermore, and to conduct a comprehensive framework, we employ the sociodemographic attributes and health-related variables suggested in the literature as the significant internal determinants of cancer patients’ QoL. Although most of the previous studies have focused on simple regression models to examine the linear relationship between QoL and its predictors [
36,
52], we employ machine learning models to analyze the survey data. The application of a broad conceptual model developed based on machine learning algorithms allows us to better understand self-reported QoL in cancer patients. Our study further incorporated machine learning models (i.e., logistic regression, decision tree, random forest, and multilayer perceptron neural network) to delineate the nonlinear patterns underlying the predictor variables with respect to the QoL of cancer patients. Results of this study have a great potential to help urban planners and policymakers design health-oriented neighborhoods that can improve cancer patients’ wellbeing and satisfaction.
4. Discussion
This study employs a cross-section survey to investigate how built environment impacts the quality of life (QoL) of cancer patients.
The random forest’s results demonstrate the top ten most important features that predict the QoL of cancer patients (
Table 4) and the logistic regression indicates associations. Our results demonstrate that the built environment characteristics considerably contribute to predicting the QoL of the participants. According to the scored features in random forest, the travel distance to the closest hospital is one of the most significant predictors of QoL. Previous studies have suggested that the distance from residential neighborhoods to patients’ treating hospital influences cancer outcomes, and consequently, those who reside far from their care provides may have a lower QoL among cancer survivors [
76]. Although travel distance to health facilities can be a barrier for cancer patients [
77,
78,
79,
80], this study considers the distance to the closest hospital and not the treated hospital. Hence, residing in neighborhoods distant from large hospital can be an indicator of living in the low-dense suburbs.
Perceived accessibility is the third predictor of the QoL in random forest [
33]. The perception towards accessibility to the neighborhood local services such as access to schools, public transportation, medical care, and shopping exhibits a significant effect on self-rated health [
81]. Although the logistic regression does not indicate a significant association between the perceived accessibility and QoL, it seems that patients residing with less accessibility (greater values of perceived accessibility), reported lower levels of QoL.
Distance to transit is the fourth important feature in the random forest. These measures are defined as the supportive built environment features that can significantly predict the QoL [
29]. The literature introduces the distance to transit and residential density as two of the objective indicators measuring the quality of urban life [
50]. According to the logistic model, patients residing in areas with more distance to transit declare lower QoL. The association is not statistically significant, but the direction is aligned with the theory.
Population density is another determinant of QoL in the random forest. Despite the lack of a clear understanding of the mechanism under which different urban densities influence QoL, some studies have suggested that high density positively affects life satisfaction [
82]. Higher population density can be positively associated with subjective wellbeing when accompanied by mixed land uses, public transport, limited car traffic, access to green spaces, and social equity [
83]. People who reside in higher density neighborhoods are more likely to perform physical activities [
84] and more able to experience better health conditions and life satisfaction [
85]. On the other hand, some research suggests that living in less dense areas can increase the quality of life while controlling for all the other sociodemographic and somatic health variables [
86]. Accordingly, urban density contributes to QoL in different ways. The results of logistic regression in terms of density and QoL associations indicates an evident paradox. Earlier studies have often reported a positive relationship between population density and health outcomes due to the availability of walkable destinations, and consequently a higher tendency towards walking, biking, or public transit [
87,
88]. In contrast, our results suggest that a higher level of QoL is reported by participants in neighborhoods with lower population density. Research on compact city form states that the negative association between life satisfaction and urban density stems from the emotional response of the residents toward perceived crime and stress in crowded and noisy neighborhoods [
83]. In contrast, residing in low-dense suburbs has positive effects on the wellbeing of individuals through positive emotions and calmness [
89]. In addition, higher levels of anxiety can be found in high-density areas and consequently decrease mental health [
90]. The positive effects of density on wellbeing occur when it brings with it mixed land use, access to public transit, restricted car travel, access to green spaces, and social equity [
83]. Accordingly, the adverse effects of population density on the self-reported QoL in cancer patients can be a result of their negative emotions towards the negative aspects of density, such as traffic congestion, the sense of crime, and lack of green space.
The scored features of the random forest reveal that the entropy index plays a moderate role in defining the level of self-reported QoL in cancer patients. Neighborhoods with mixed land use provide the cancer survivors accessibility to different errands in a walkable distance [
25]. This result is in accordance with some previous studies about the compact city form in which mixed land use has the potential to provide a better quality of life through offering longer, healthier, and safer lives and contributing to the economic wellbeing and health of cities [
91].
Random forest scores show that among all sociodemographic characteristics, respondents’ age has an enormous contribution to the level of QoL among cancer patients. It seems that the process of aging in cancer patients can influence disease adjustment and therefore impact the health-related QoL [
92]. Our results from the regression model reveal that older cancer patients have a higher level of QoL. This finding is in line with similar studies, which suggest that younger patients feel worse than older adults on some quality of life dimensions because they suffer more from psychological symptoms and financial issues [
93,
94].
The random forest score of health insurance shows that this feature can differentiate the QoL experience through different levels. This result is in line with previous studies that demonstrate health insurance status is associated with health-related attributes of cancer patients over time [
95]. Since patients with poorer insurance coverage may have less access to high-quality treatment, this can result in later diagnoses and worse outcomes [
96]. This result confirms empirical evidence, which shows that health insurance can reinforce the health of vulnerable groups, such as senior adults, children, and people with premedical conditions and low-income populations [
97]. Moreover, the associations between health insurance and QoL explain that participants who have private and/or employer-paid insurance health insurance reported a higher QoL levels compared with low-income participants who have government-related insurance. It confirms previous studies that report that cancer-related financial burdens are related to an increased risk of depression and lower health-related QoL levels in cancer patients [
98].
The number of cars in the family is the tenth significant factor in predicting the QoL that has been identified by the random forest. To the best of our knowledge, there is no evidence to identify the effect of vehicle ownership on the QoL of cancer patients. However, the vehicle is the most usual mobility mode particularly for residents of distant and rural areas, so, it can affect a cancer patients’ access to treatment facilities where they might not have access to other mobility modes [
77,
78,
99,
100]. Access to private vehicles and the option of driving with others are among the most crucial treatment-related factors that impose barriers to cancer patients [
101]. Vehicle availability is assumed as a variable that has a positive relationship with the early diagnosis stage [
15] and receiving the first line of treatments [
79]. Patients residing in areas having no access to a private vehicle are less likely to follow cancer screening treatments [
102]. This evidence can support the contribution of access to a car in the QoL of cancer patients.
Furthermore, education is another factor contributing to the QoL of cancer patients. This result supports the studies that propose education improves wellbeing because it develops access to economic devices, enhances a person’s sense of control over life, and increases social support [
103]. The positive association between education and QoL in this study can be justified by the earlier research suggesting that low education along with low neighborhood socioeconomic status result in worse all-kind survival for particular cancers [
24]. The higher score related to the significance of chemotherapy compared with radiotherapy reveals that chemotherapy treatment has a more significant contribution in predicting quality of life [
104]. Chemotherapy treatment appears to have a negative effect on the QoL of patients who received this treatment. Although physicians suggest chemotherapy to improve QoL for patients with end-stage cancer, it cannot reinforce QoL for patients with moderate or poor performance status and worsened QoL close for patients with good performance status [
105]. Gender and race have a small participation in determining the level of QoL. The race of the participants (white versus other races) has a small but notable effect on QoL after treatment [
106].
5. Conclusions
This study brings new insights regarding the impacts of actual and perceived built environment characteristics on the QoL of cancer patients while controlling sociodemographic and health-related factors. To address the first research question regarding the factors explaining the self-reporting QoL, we employed the random forest approach. Results suggested that the QoL of cancer patients can be principally influenced by built environment features, including travel distance to a closest large hospital, perceived accessibility, distance to transit, population density, and sociodemographic factors such as age, health insurance status, and education. Results from the logistic regression fulfill the second research question regarding the most significant determinants of QoL in cancer patients. Population density, age, education, health insurance, and chemotherapy treatment are the most critical determinants of QoL in cancer patients. We point out the main research outcomes in the following areas:
Our findings regarding the effects of built environment features such as density and access to healthcare facilities on the QoL of cancer patients indicate that a supportive built environment can overcome the barriers in the outdoor environment, increase the likelihood of physical activity, and therefore improve perceived quality of life. These results point out that urban design and transportation planning need to become more friendly for this population group with particular needs and requirements.
To improve social equity, it is fundamental to design environments compatible with the needs of all community groups, including people who are struggling with chronic diseases that require ongoing medical attention or limit activities of daily living in the long term.
Understanding the associations between built environment and health-related QoL can help in the development of intervention policies that aim to improve cancer patients’ wellbeing. Hence, there is a need for collaboration between transit agencies, MPOs, and community planners to target the living environment and mobility needs of people who are burdened with chronic disease. To this end, urban and transportation planners and practitioners should be more involved in this field and acquire more knowledge from other disciplines. Integrating transportation planning with public health and social studies could reinforce existing policies and strategies in transportation accessibility and equity and therefore increase wellbeing and QoL.
In addition, there is an inherent need to develop a QoL measurement that comprehensively counts for subjective feelings as well as objective factors in terms of patients’ health condition, transportation, and built environment. This QoL measurement can be used as a policy tool by communities and local governments to evaluate the extent to which the mobility and built environment meet the needs of patients with chronic diseases.
The inverse associations between population density and cancer patients’ QoL indicate that compact development strategies can be fulfilled when policymakers address the side effects of urban density, such as fear of crime, high noise, and traffic congestion. This compact development pattern should concentrate on strategies that increase robust transportation options and improve public health indicators such as air quality while creating safe and secure neighborhoods that preserve more open space.
There is large room for improvement in our understanding of the effects of built environment and transportation accessibility on cancer patients’ QoL in future research. Working with the small sample size in our study can be a principal limitation of our study, which may have caused some failures in identifying more associations between the key variables, particularly in the logistic regression model. Further studies need to be developed to collect data on a large population of cancer patients regarding their mobility needs, their concerns towards residential neighborhoods, and their preferences about the attributes of a supportive neighborhood that can overcome their physical, mental, social, and environmental barriers. The other limitation of this study is related to measuring QoL. Measuring the QoL of the patients through standard EQ-5D-5L or Q-5D-3L criteria can allow future studies to explain the QoL of cancer patients thoroughly. This study also emphasizes the need for collaboration between health policymakers, urban planners, and transportation experts to conduct more research regarding the effects of transportation policies on health outcomes.






{kind=link}
{kind=link}
{kind=link}