
Identifying Psychosocial Risks and Protective Measures for Workers’ Mental Wellbeing at the Time of COVID-19: A Narrative Review

 ,
, 
 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
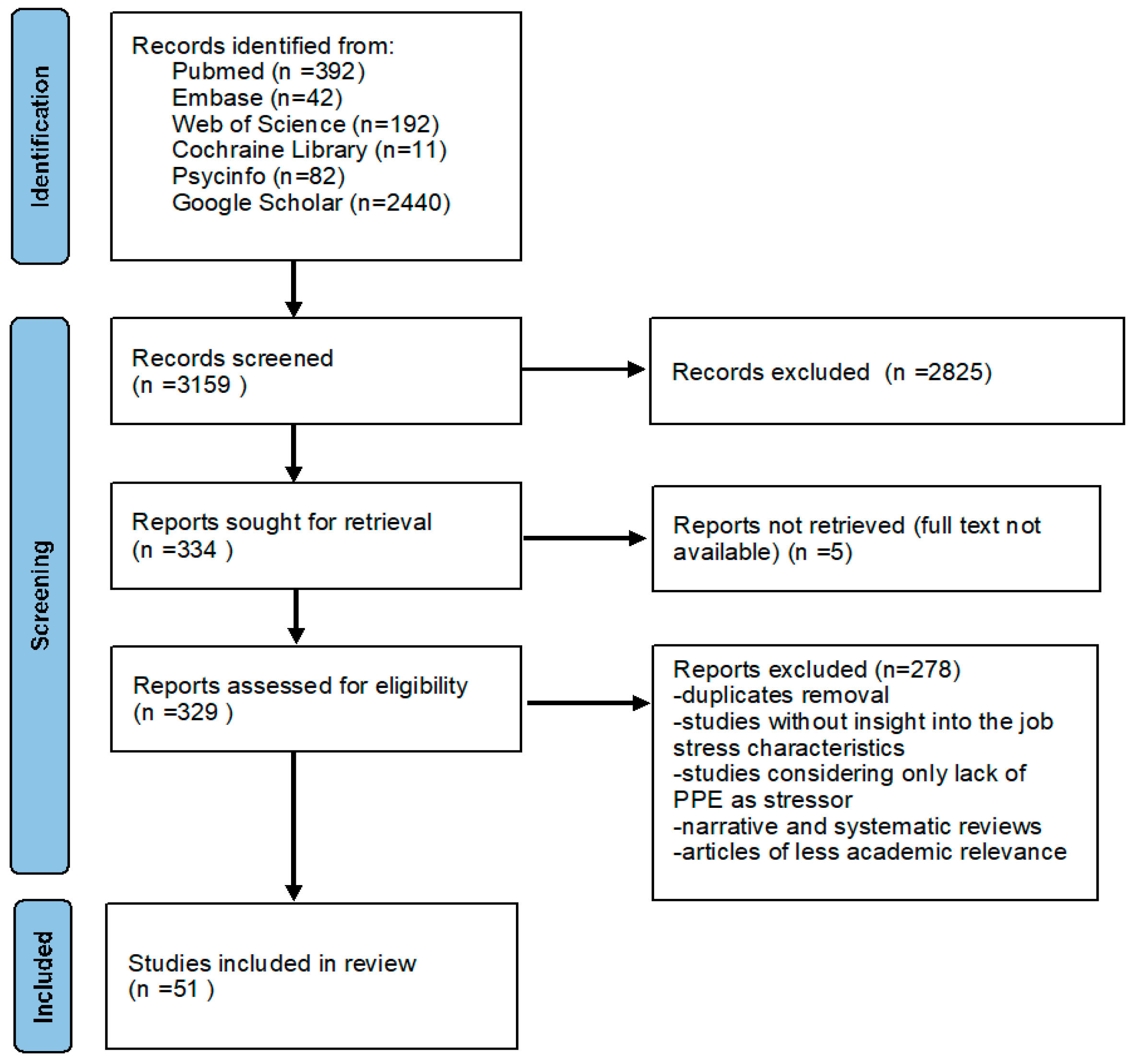
2.1. Literature Research, Selection and Data Extraction
2.2. Inclusion Criteria
2.3. Exclusion Criteria
3. Results
- Support from peers and organizations;
- Home–work interface and balance;
- Changes in workload and job demand;
- Work competence and adequate training;
- Job insecurity and financial stress.
3.1. Support from Peers and Organization
3.2. Home–Work Interface and Balance
3.3. Changes in Workload and Job Demand
3.4. Work Competence and Adequate Training
3.5. Job Insecurity and Financial Stress
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Authors | Sample/ Country/ Study Design | Working Population | Scale Used | Intervention/ Psychosocial Risks Identified | Mental Outcomes | Main Results |
|---|---|---|---|---|---|---|
| Aguiar-Quintana et al. [67] | 353/Spain/Cross-sectional study | Hotel employees | Ad hoc questionnaires | Job insecurity and financial stress | Anxiety and depression | Job insecurity of employees did not significantly influence Task Performance but was positively and significantly associated with Anxiety and Depression |
| Zhou et al. [42] | 107/China/Short-term longitudinal study | Frontline HCW | The Chinese version of Impact Event Scale-Revised (CIES-R), A perceived organizational support scale was developed, ad hoc questionnaires for coping strategies. | Support from peers and organization | PTSD | Perceived organizational support had a significant indirect effect on PTSD symptoms. Problem-focused coping strategies and self-efficacy mediate this effect. |
| Zhang J. et al., [54] | 4850/China/Cross-sectional study | Frontline HCW | ERI questionnaire, the 9-item Patient Health Questionnaire (PHQ-9), 7-item General Anxiety Disorder Scale (GAD-7). | Changes in workload and job demand | work stress, depression, anxiety | Effort and over-commitment were positively associated with depression and anxiety, and negatively associated with reward, through development and job acceptance. |
| Khajuria A. et al. [17] | 2527/Multiple countries (China, UK, USA)/Cross-sectional study | HCWs | Patient Health Questionnaire-2 (PHQ-2); questionnaires ad hoc for workplace factors | Work competence and adequate training/Support from peers and organizations | Depressive symptoms | Poor training and poor support in the workplace, including being redeployed without adequate training, were all highly significant correlated to more depressive symptoms., |
| Gilleen J. et al. [55] | 2773/UK/Cross-sectional study | HCW | Patient Health Questionnaire (PHQ-9), General Anxiety Disorder-7 (GAD-7), 22-item Impact of Event Scale-Revised (IES-R)1; ad hoc questionnaires on work conditions and possible factors of anxiety and depression | Support from peers and organization/Changes in workload and job demand | Anxiety and depression symptoms | Insufficient personal protective equipment availability, workplace preparation, training and communication, and higher workload were associated with anxiety and depression symptoms. Sharing stress, resilience and ethical support were associated with better psychological outcomes. |
| Escudero-Castillo I. et al. [43] | 1050/Spain/Cross-sectional study | Workers not further specified | Ad hoc questionnaires | Home–work interface and balance | Personal wellbeing | The lockdown exerted a greater negative effect on the self-perceived wellbeing of unemployed and furloughed persons than on those in employment. Teleworkers experienced a lesser degree of self-perceived wellbeing post lockdown as compared to those people remaining in the same work location. |
| Babore A. et al. [30] | 595/Italy/Cross-sectional study | HCWs | Perceived Stress Scale (PSS-10); The COPE-New Italian Version (COPE-NVI-25 | Support from peers and organization | Occupational stress | Lower positive attitude, higher social support, working with COVID-19 patients and higher avoidance strategies predicted higher levels of distress. The higher the positive attitude, the lower distress, while social support and avoidance constituted risk factors for work-related stress. |
| Bulinska-Stangrecka H. et al. [24] | 220/Poland/Cross-sectional study | IT employees | Ad hoc questionnaires | Support from peers and organization | Job satisfaction | Employee relations including interpersonal trust support, help building job satisfaction, even in a virtual space and remotely. |
| Afulani P.A. et al. [35] | 414/Ghana/Cross-sectional | HCW | 10-item Cohen perceived stress scale. Burnout was assessed using the 14-item Shirom-Melamed Burnout measure (SMBM), ad hoc questionnaires | Support from peers and organization | Job stress, burnout | Healthcare workers who felt somewhat prepared and appreciated/experienced support from management and support by family had lower stress and burnout scores than those who did not feel prepared. Fear of infection was associated with higher stress and burnout. |
| Charoensukmongkol P. et al. [31] | 300/Thailand/cross-sectional | University employees | Adapted scale for Uncertainty at work, supervisor support was measured using the scale of Cole et al. (2006); Emotional Exhaustion was measured using the scale of Maslach and Jackson; Organizational Intransigence was measured using the scale of Patterson et al. (2005). | Support from peers and organization | Uncertainty at work, emotional exhaustion | Perceived uncertainties were associated with emotional exhaustion. Supervisor support has a negative effect on the perceived uncertainties of employees, however this support can be suppressed by organizational intransigence. |
| Cipolotti L. et al. [25] | 158/UK/cross sectional | Hospital employees (HCW and non HCW) | Ad hoc questionnaire assessing psychological impact of COVID | Changes in workload and job demand/Work competence and adequate training | Psychological distress | Work challenges (performance at work/making mistakes, changes to role/hours worked/shift patterns, discussions with dying patients families, dealing with families), and social change (distancing from family, not doing regular activities) predicted psychological distress |
| Elbay R.Y. et al. [18] | 442/Turkey/cross sectional | HCW on frontline and not | DAS-21; specific questionnaires on working conditions | Support from peers and organization/Changes in workload and job demand/Work competence and adequate training | Depression and anxiety symptoms | Increased weekly working hours, increased number of COVID-19 patients cared for, lower level of support from peers and supervisors, lower logistic support and lower feelings of competence during COVID-19 related tasks were associated with higher DAS-21 total scores. |
| Gómez-Galán J. Et al. [32] | 2182/Spain/cross-sectional | Security workforce | Maslach Burnout Inventory (MBI) scale; ad hoc questionnaire for subjective perceptions about their working conditions and the need for psychological and psychiatric treatment; the Death Anxiety Scale. | Support from peers and organization | Burnout | Stress and anxiety levels increased in work as a result of not having the basic supplies for their personal protection. Most workers reported that they have not felt recognized in their professional activity by their institution. |
| Hines S.E. et al. [41] | 96/USA/longitudinal study | HCW | Impact of Events Scale-Revised (IES-R) Moral Injury Events Scale (MIES); specific questionnaires on occupational factors | Support from peers and organization | Moral injury | A supportive workplace environment was related to lower moral injury, whereas a stressful, less supportive environment was associated with increased moral injury. |
| Kannampalli T. et al. [46] | 393/USA/cross sectional | Physician trainees | DASS-21; Stanford Professional Fulfillment Index (PFI). Specific questionnaires on work–family balance and perceived life stressors | Home–work interface and balance | Burnout, stress | The group exposed to COVID-19 patients experienced moderate to extremely high perceived stress regarding childcare and considerably lower work–family balance. Their job duties interfered with their family life, and they experienced more difficulty in taking time off for attending to personal or family matters. |
| Labrague L. et al. [19] | 325/Philippines/cross-sectional | Nurses | COVID-19 Anxiety Scale, the Brief Resilient Coping Scale (BRCS), the Perceived Social Support Questionnaire (PSSQ) and the Perceived Organizational Support (POS) questionnaire | Support from peers and organization | Anxiety symptoms | Social support, personal resilience and organizational support predicted COVID-19 anxiety. Increased scores in the social support, organizational support and personal resilience measures were associated with lower COVID-19 related anxiety. |
| Magnavita N. et al. [64] | 155/Italy/cross-sectional | Anesthetists | Specific questionnaires on changes in occupation and lifestyles; Effort-Reward Imbalance questionnaire, Colquitt Scale (organizational justice), Goldberg Anxiety and Depression Scale (GADS). | Changes in workload and job demand/Work competence and adequate training | Occupational stress, anxiety symptoms | A significant increase in workload was associated with work-related stress and low perceived levels of organizational justice. Workers experienced little ability to influence and change the outcome of procedures. Levels of anxiety and depression were significantly correlated with work effort. |
| Manzano-Garcia G. et al. [36]. | 771/Spain/cross sectional | Nurses | Questionnaire on socio-demographic data; Spanish Burnout Inventory (CESQT) for burnout, the UNIPSICO Battery for the evaluation of certain psychosocial factors of demand and resources in the context of work; ad hoc scale for perceived threat of COVID-19 | Changes in workload and job demand/Support from peers and organization | Burnout | Work overload, material and human resources and social support at work were significant in explaining burnout. The perceived threat of COVID-19 moderated the relationship between social support at work and burnout. |
| Marco C.A.et al. [48] | 1300/USA/cross-sectional | Emergency Physicians | Life Events Checklist for DSM-5, the PTSD Checklist for DSM-5 | Changes in workload and job demand/Work competence and adequate training/Job insecurity and financial stress | PTSD/work related stress | The major sources of stress identified by participants included disinformation about COVID-19, computer work/electronic medical record, PPE concerns, and workload. Financial stress related to reduced patient volume and concerns about work–home imbalance were present, especially in those caring for homeschooling children. This played a role in the stress perceived. |
| Mattila E.et al. [20] | 1079/Finland/cross-sectional | Hospital staff | Generalized Anxiety Disorder 7-item scale (GAD-7), specific questionnaires on demographic data, changes in work, interaction between co-workers, psychological distress linked to work, fear of contagion. | Support from peers and organization/Changes in workload and job demand | Anxiety symptoms | Anxiety symptoms were associated with: young age, working in a university hospital, problems in cooperation between co-workers, difficulty concentrating at work, a health-threatening physical and psychological workload, and a fear of being infected at work. |
| Moretti A. et al. [44] | 51/Italy/cross-sectional | Home working population (put in remote worker since the beginning of pandemic) | Utrecht Work Engagement Scale (UWES) for job satisfaction, Brief Pain Inventory (BPI) and Fear Avoidance Beliefs Questionnaire (FABQ) for MSK issues; ad hoc questionnaire for structural aspects of the workplace at home | Home–work interface and balance | Perceived job productivity and satisfaction, work-related stress, and musculoskeletal (MSK) issues. | Thirty-nine percent of the subjects working from home self-perceived to be less productive but less stressed, while 51% were equally satisfied. Among mobile working advantages, the most appreciated was saved travel time and the least appreciated was greater autonomy. Impaired interaction with colleagues and distractions in the domestic environment were the worst disadvantages |
| Morgantini L.A.et al. [47] | 2707/Various countries (USA, Italy, Brazil, Sweden, others)/cross sectional | Healthcare workers | Ad hoc questionnaire containing questions covering three major domains of HCPs experience (exposure, perception, and workload) | Home–work interface and balance/Work competence and adequate training | Burnout | Burnout was associated with work impacting household activities, feeling pushed beyond training, exposure to COVID-19 patients and making life prioritizing decisions. Burnout was higher in high-income countries compared to low- and middle-income countries. |
| Portoghese I. et al. [50] | 521/Italy/cross-sectional | Physicians | Ad hoc questionnaire on organizational preparedness, personal preparedness concerns about catching COVID-19; perceived impact on personal job (role and demand) and on personal life, perceived job stress, rumination about the pandemic, crying at work. | Changes in workload and job demand/Home–work interface and balance | Job stress | The risk factors for perceived job stress were concerns about catching COVID-19, perceived impact on job demands, perceived impact on job role and non-working concerns (fear of infecting relatives and friends). |
| Soto-Rubio A. et al. [37] | 125/Spain/cross-sectional | Nurses | Trait Meta-Mood Scale (TMMS-24) for emotional intelligence, UNIPSICO Battery for psychosocial risks, Interpersonal conflicts scale, Lack of organizational justice scale, Role conflict scale, Workload scale Social support scale, Job satisfaction scale, Frankfurt Emotional Work Scale (FEWS), Questionnaire for the Assessment of Workplace Burnout Syndrome (CESQT) | Support from peers and organization | Job stress, burnout | The emotional intelligence of nurses can influence interpersonal conflicts or lack of organizational justice at work. Emotional repair component can be a factor that when enhanced can prevent the possible adverse effects related to burnout and job satisfaction. |
| Tušl M. et al. [45] | 2118/Switzerland, Germany/cross sectional | Employees | Warwick–Edinburgh Mental Well-Being Scale (WEMWBS), ad hoc questionnaires for impact of COVID in life and change in work | Home–work interface and balance/Changes in workload and job demand | Mental wellbeing and self-reported health | Mandatory short-time work was strongly associated with perceived negative impact on work life, while work from home, particularly if experienced for the first time, was strongly associated with a perceived positive impact on work life. Perceived negative impact of the crisis on work and private life and mandatory short-time work were associated with lower mental wellbeing and self-reported health. |
| Yang Y. et al. [21] | 2878/China/cross sectional | HCWs | Chinese version of the Workplace Violence Scale, 9-item Patient Health Questionnaire (PHQ-9). The 7-item General Anxiety Disorder Questionnaire (GAD),The 26-itemWorld Health Organization Quality of Life Questionnaire (WHOQOL-BREF) | Support from peers and organization | Depression, anxiety | Frontline clinicians’ experience of workplace violence directly affected quality of life and emotional disturbances partly mediated the association between workplace violence and the quality of life |
| Zandi G. [38] | 129/Pakistan/cross-sectional | Physicians | Perceived stress scale for job stress, scale for extent of exposure to COVID, scale adapted from Survey of Perceived Organizational Support (SPOS) for organizational support | Support from peers and organization | Job stress | Perceived organizational support moderated the relationship between the extent of exposure and stress. The relationship appeared weaker when organizational support was perceived high; the relationship was stronger with a low level of perceived organizational support. |
| Zerbini G. et al. [65] | 110/Germany/cross sectional | Nurses and physicians | Patient Health Questionnaire(PHQ) the Maslach Burnout INventory (MBI), specific scale for fear of COVID infection and stress at work, open questions. | Changes in workload and job demand/Job insecurity and financial stress | Depression symptoms, burnout | The most common causes for burden were job strain and uncertainty about the future. Psychosocial support as well as leisure time were listed important resources, and a better infrastructure adjustment to COVID-19 at the hospital (e.g., sufficient staff, keeping teams and working schedules stable)as suggestion for improvement. |
| Zhang X. et al. [54] | 524/China/cross sectional | Medical Staff | Generalized Anxiety Disorder Scale, the Patient Health Questionnaire, the Insomnia Severity Index, the Occupational stress Questionnaire. | Changes in workload and job demand | anxiety and depression symptoms, job stress | Working intensity, working time, working difficulty and working risk were correlated positively with mental health symptoms. A significant association was found between occupational stress and mental health symptoms in both frontline and non-frontline medical staff during COVID-19 outbreak. |
| Lee H. et al. [40] | 131/Singapore/cross sectional | Remote workers | Open ended questions for qualitative analysis | Support from peers and organization | Mental status related to emotions perception | The employees’ emotional reactions were elicited from the perceived organizational support, in how the organization cares for their wellbeing and work contributions and, in turn, influence the psychological safety. Anxiety, stress, unfairness, inferiority and vulnerability are triggered by perceived |
| Al-Ghunaim T. et al. [53] | 141/UK/qualitative analysis | Surgeons | Qualitative analysis through two open-ended questions | Changes in workload and job demand/Work competence and adequate training | Stress and burnout; fear anxiety, loss of motivation, low mood. | Surgeons’ mental health during COVID-19 pandemic was affected by substantial emotional and psychological effects particularly in relation to fear and anxiety, loss of motivation, low mood, stress and burnout, highlighting the urgent need for workplace support and mental health interventions. |
| Al-Mansour, K. et al. [26] | 1378/Saudi Arabia/cross sectional | Physicians, nurses, other health professionals and other workers who worked in the primary healthcare centers. | -Perceived Stress Scale (PSS) Rosenberg Self-Esteem Scale (RSES); Multidimensional Scale of Perceived Social Support (MSPSS);-scale for ambiguity at work. | Support from peers and organization | Stress | During the COVID-19 pandemic, higher levels of stress and role conflict and ambiguity were found among HCWs in fever clinics than among HCWs in regular primary healthcare centers in Saudi Arabia. Role conflict and ambiguity, social support and self-esteem were found to be major determinants of stress among HCWs during the pandemics. |
| Digby, R.et al. [22] | 321/Australia/qualitative analysis | Medical, nursing, allied health and non-clinical staff | Qualitative: Free-text questions | Work competence and adequate training/Support from peers and organization | Anxiety, stress | Healthcare staff need both practical and psychological support and regular clear communication to minimize anxiety, promote well-being, foster resilience, and ensure that they are in a strong position to deal with the health crisis |
| Dreher, A.et al. [60] | 2150/Germany/cross sectional | Medical assistants (MA) | Patient Health Questionnaire (PHQ-2); Generalized Anxiety Disorder questionnaire (GAD-2); questions on socio-demographic data, own contraction of SARS-CoV-2, contraction of SARS-CoV-2 among family, friends, and colleagues, and questions on attitudes, stressors, and work-related outcomes during SARS-CoV-2 pandemic. | Support from peers and organization/Work competence and adequate training | Anxiety, depression | A low level of preparedness and high levels of uncertainty affected MAs in Germany regarding the SARS-CoV-2 pandemic. Major stressors were uncertainty about the temporal scope of the pandemic, uncertainty about how to act correctly, a feeling of not being allowed to let patients down and uncertainty about one’s financial situation. |
| Elshami, W. et al. [59] | 385/Middle East, North Africa and India/cross sectional | RWF working at hospitals during the pandemic, such as radiologists, radiographers, advanced practitioners and radiology nurses | The survey consisted of four sections: demographic characteristics, radiology professional practice survey, the Coronavirus Anxiety Scale (CAS), and the Fear of COVID-19 Scale(FCe19S). | Job insecurity and financial stress/Changes in workload and job demand/Work competence and adequate training | Stress, anxiety, fear | Fear was associated with workers younger than 30 years of age and also with temporary staff. Nevertheless, anxiety occurred completely independently of gender, age, experience, country, working environment and work status. Professional support is needed to reduce or prevent fear, stress, and anxiety among HCPs. |
| Yang, Y. et al. [51] | 1208/China, USA/cross sectional | 664 doctors, 246 nurses | DASS (Depression, Anxiety, and Stress Scale); PSS (Perceived Social Support Scale) | Changes in workload and job demand | Anxiety, depression, stress | Stress, anxiety, and depression were positively related to lower levels of social support, longer working hours, discrimination experience and workplace violence. Stress, anxiety, and depression were positively related to lower levels of social support, longer working hours, discrimination experience and workplace violence. |
| Feeley, T. et al. [52] | 408/Ireland/cross sectional qualitative design | Intensive care unit (ICU) staff | Open questions | Changes in workload and job demand/Job insecurity and financial stress/Home–work interface and balance | Occupational stress | The home, work and social environments, the home–work interface and uncertainty about the future were the major themes retrieved. The work environment-team structure, senior staff guidance, social communication, colleague support, altered role, high workload-dictated the emotional and psychological responses of healthcare staff. |
| Gul, S. et al. [63] | 192/Turkey/cross sectional | Operating rooms nurses | Beck Anxiety inventory (BAI) | Support from peers and organization/Changes in workload and job demand | Anxiety | Nurses experienced moderate levels of anxiety as they are inexperienced and must work with patients who pose a serious level of risk; they should be trained in critical patient care in order to reduce their anxiety levels. |
| Havaei, F. et al. [33] | 3676/Canada/cross sectional | Nurses | Post-traumatic Stress Symptoms-14 (PTSS-14); Generalized Anxiety Disorder-7 (GAD-7); Patient Health Questionnaire-9 (PHQ-9); EE subscale of the Maslach Burnout Inventory; Human Services Survey (MBI-HSS) | Support from peers and organization | Anxiety, PTSD, depression, burnout | Negative ratings of workplace relations, organizational support, organizational preparedness, workplace safety, and access to supplies and resources were associated with higher scores on all of the adverse mental health outcomes. Better workplace policies and practices are urgently required to prevent and mitigate nurses’ suboptimal work conditions. |
| Halley, M.C. et al. [49] | 1806/USA/qualitative analysis | Physician mothers | Qualitative approach | Support from peers and organization/Home–work interface and balance/Job insecurity and financial stress | Stress | Leaders within healthcare organizations and the government need a deep understanding of the physician mothers’ challenges in order to ensure robust public health policies, adequate equipment for personal safety and optimal patient care, and support to meet basic personal financial and family needs. |
| Hu, J. et al. [34] | 1:163/2:282/3:210/China/USA/cross sectional | 1: employees of an information technology company 2: Amazon’s Mechanical Turk 3: Amazon’s Mechanical Turk | Ad hoc questionnaires | Support from peers and organization | Anxiety symptoms | COVID-19-triggered mortality salience increases state anxiety. Mortality salience not only triggers anxiety about own deaths but also generates tremendous overall anxiety. Servant leaders who keep employees’ well-being paramount and model compassion can help anxious employees stay engaged at work and help the broader community. |
| Ingusci, E. et al. [57]. | 530/Italy/ | Remote workers | Validated scales for workload, job crafting and behavioral stress | Changes in workload and job demand/Work competence and adequate training | Occupational Stress | The direct effect between work overload and behavioral stress was positive; the indirect, negative effect through the mediation of job crafting was also significant Job crafting can play a crucial role as a protective factor supporting the activation and adjustment of suitable resources; these resources can be useful to deal with the negative effects of work overload, particularly under the condition of heavy remote working and use of technologies. |
| Mekonen, E. et al. [58] | 302/Ethiopia/cross sectional | Nurses | DASS-21 | Changes in workload and job demand/Work competence and adequate training | Anxiety, depression, and stress | Workload, taking training, having a guideline, adequate protective equipment, having children, fear of infecting family members, feedback from families and friends are significantly associated with anxiety, depression and stress. |
| Al-Jumaili, A.A. et al. [27] | 430/Iraq/cross sectional | Healthcare providers (HCPs) | Adopted items of surveys used in previous studies of Severe Acute Respiratory Syndrome (SARS) and Avian Influenza Outbreak | Support from peers and organization | Stress | Working during COVID-19 pandemic has several negative impacts on HCPs including mental and physical health and an overwhelming work environment. Thus, social and emotional support is needed to help HCPs to cope with such stressful conditions |
| Mo, Y., et al. [23] | 200/China/cross sectional | Nurses | Self-rating Anxiety Scale (SAS); Stress Overload Scale (SOS); General Self-efficacy Scale (GSES) | Support from peers and organization | Anxiety, stress, self-efficacy | Nurses’ mental health were affected by, sleep status, stress and self-efficacy. Work stress and self-efficacy were closely correlated with anxiety. Social support plays an important role in alleviating mental stress. Self-efficacy is negatively correlated with anxiety. |
| Nguyen, P. et al. [62] | 761/Vietnam/cross sectional | Healthcare workers | Impact of Event Scale-Revised (IES-R) | Changes in workload and job demand | Stress | It was found that there was a higher risk of having stress among HCWs who were at the frontline, since they perceived their health status as worse as compared with that before the pandemic. Most HCWs were worried about being a potential source of infection to their families. |
| Norful, A. [28] | 55/USA/qualitative analysis | Healthcare workers | Qualitative interviews | Support from peers and organization | Burnout, anxiety, sleep disturbance, stress | Uncertainty of COVID-19 practice guidelines, lack of resources, and risk of transmission to loved ones at home were the primary drivers behind stress. Further, anxiety, physical exhaustion, and sleep disturbances were the predominant manifestations of stress experienced by participants. Psychosocial support and increased teamwork across disciplines emerged as a significant mitigator of stress, yielding less perceived burnout and improved clinician wellbeing. |
| Rodriguez-Lopez, A.M. [39] | 360/Spain/cross sectional | Fashion Retailing Workers | CarMen-Q Mental workload questionnaire (Cognitive Demands, Temporal Demands, Emotional Demands, Performance Demands); MBI Burnout Syndrome Inventory (Emotional Exhaustion, Depersonalization, Personal Accomplishment); Perception of COVID-19 | Changes in workload and job demand/Job insecurity and financial stress | Burnout | Participants exhibited deep concern about the COVID-19 pandemic and its influence in the workplace. Environmental changes, work overload, somatic symptoms, insomnia, negative job expectations, and uncertainty constituted significant mental workload predictors. Insomnia, somatic symptoms, and negative job expectations constituted significant predictors for burnout. |
| Tokac, U. et al. [66] | 83/USA/cross sectional | Nurses | Patient Health Questionnaire (PHQ-9); Generalized Anxiety Disorder (GAD-7) Scale; Insomnia Severity Index (ISI); Impact of Event Scale-Revised (IES-R); Compassion Fatigue and Satisfaction Self-Test (CFS); Work Productivity and Activity Impairment Questionnaire(WPAI:GH) | Work competence and adequate training | Anxiety, depression, burnout, avoidance level | Nurses’ work impairment decreased with greater years of nursing experience and increased with higher anxiety, depression, burnout and avoidance levels. |
| Coulombe, S. et al. [29] | 1122/Canada/cross sectional | Workers not further specified | Perceived Stress Scale (PSS) Patient Crisis; Disaster Preparedness Scale; Depression and Anxiety (PHQ-4); ad hoc questionnaires | Job insecurity and financial stress/Support from peers and organization | Distress and stress | COVID-19 crisis encompasses several stressors related to the virus as well as to its impact on one’s social, occupational, and financial situation, putting workers at risk of lower wellbeing. |
| Moreno-Jiménez, J. et al. [61] | 221/Spain/cross sectional | Health professionals | Nursing Burnout Scale (NBS), Occupational Hardiness Questionnaire, Short Burnout Questionnaire, Secondary Traumatic Stress Scale, ad hoc questionnaires | Changes in workload and job demand | Emotional exhaustion and secondary traumatic stress | The lack of human resources predicted emotional exhaustion through the workload and secondary traumatic stress through fear of contagion, contact with death/suffering, and workload. |
References
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Sheraton, M.; Deo, N.; Dutt, T.; Surani, S.; Hall-Flavin, D.; Kashyap, R. Psychological Effects of the COVID-19 Pandemic on Healthcare Workers Globally: A Systematic Review. Psychiatry Res. 2020, 292, 113360. [Google Scholar] [CrossRef] [PubMed]
- Sigahi, T.F.A.C.; Kawasaki, B.C.; Bolis, I.; Morioka, S.N. A Systematic Review on the Impacts of COVID-19 on Work: Contributions and a Path Forward from the Perspectives of Ergonomics and Psychodynamics of Work. Hum. Factors Ergon. Manuf. 2021, 31, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The Impact of SARS-CoV-2 on the Mental Health of Healthcare Workers in a Hospital Setting—A Systematic Review. J. Occup. Health 2020, 62, e12175. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/10.1002/1348-9585.12175 (accessed on 6 September 2021). [CrossRef]
- Baldassarre, A.; Giorgi, G.; Alessio, F.; Lulli, L.G.; Arcangeli, G.; Mucci, N. Stigma and Discrimination (SAD) at the Time of the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6341. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gomez, M.; Giorgi, G.; Finstad, G.L.; Urbini, F.; Foti, G.; Mucci, N.; Zaffina, S.; León-Perez, J.M. COVID-19 Pandemic as a Traumatic Event and Its Associations with Fear and Mental Health: A Cognitive-Activation Approach. Int. J. Environ. Res. Public Health 2021, 18, 7422. [Google Scholar] [CrossRef] [PubMed]
- De Pablo, G.S.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of Coronavirus Syndromes on Physical and Mental Health of Health Care Workers: Systematic Review and Meta-Analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, Prevention, and Management of the Psychological Effects of Emerging Virus Outbreaks on Healthcare Workers: Rapid Review and Meta-Analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Mhango, M.; Dzobo, M.; Chitungo, I.; Dzinamarira, T. COVID-19 Risk Factors Among Health Workers: A Rapid Review. Saf. Health Work 2020, 11, 262–265. [Google Scholar] [CrossRef]
- Stansfeld, S.; Candy, B. Psychosocial Work Environment and Mental Health—A Meta-Analytic Review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef]
- Posel, D.; Oyenubi, A.; Kollamparambil, U. Job Loss and Mental Health during the COVID-19 Lockdown: Evidence from South Africa. PLoS ONE 2021, 16, e0249352. [Google Scholar] [CrossRef] [PubMed]
- ILO Monitor: COVID-19 and the World of Work. 7th Edition. Available online: http://www.ilo.org/global/topics/coronavirus/impacts-and-responses/WCMS_767028/lang--en/index.htm (accessed on 6 September 2021).
- Barone Gibbs, B.; Kline, C.E.; Huber, K.A.; Paley, J.L.; Perera, S. COVID-19 Shelter-at-Home and Work, Lifestyle and Well-Being in Desk Workers. Occup. Med. 2021, 71, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Galanti, T.; Guidetti, G.; Mazzei, E.; Zappalà, S.; Toscano, F. Work from Home during the COVID-19 Outbreak: The Impact on Employees’ Remote Work Productivity, Engagement, and Stress. J. Occup. Environ. Med. 2021, 63, e426–e432. [Google Scholar] [CrossRef]
- Preparing for the next Pandemic. Nat. Med. 2021, 27, 357. Available online: https://0-doi-org.brum.beds.ac.uk/10.1038/s41591-021-01291-z (accessed on 6 September 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Quintana, T.; Nguyen, T.H.H.; Araujo-Cabrera, Y.; Sanabria-Díaz, J.M. Do Job Insecurity, Anxiety and Depression Caused by the COVID-19 Pandemic Influence Hotel Employees’ Self-Rated Task Performance? The Moderating Role of Employee Resilience. Int. J. Hosp. Manag. 2021, 94, 102868. [Google Scholar] [CrossRef]
- Zhou, T.; Guan, R.; Sun, L. Perceived Organizational Support and PTSD Symptoms of Frontline Healthcare Workers in the Outbreak of COVID-19 in Wuhan: The Mediating Effects of Self-Efficacy and Coping Strategies. Appl. Psychol. Health Well-Being 2021, 13, 745–760. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Xu, J.; You, H.; Li, Y.; Liang, Y.; Li, S.; Ma, L.; Lau, J.T.-F.; Hao, Y.; et al. Prevalence of Mental Health Problems and Associated Factors among Front-Line Public Health Workers during the COVID-19 Pandemic in China: An Effort–Reward Imbalance Model-Informed Study. BMC Psychol. 2021, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Khajuria, A.; Tomaszewski, W.; Liu, Z.; Chen, J.-H.; Mehdian, R.; Fleming, S.; Vig, S.; Crawford, M.J. Workplace Factors Associated with Mental Health of Healthcare Workers during the COVID-19 Pandemic: An International Cross-Sectional Study. BMC Health Serv. Res. 2021, 21, 262. [Google Scholar] [CrossRef] [PubMed]
- Gilleen, J.; Santaolalla, A.; Valdearenas, L.; Salice, C.; Fusté, M. Impact of the COVID-19 Pandemic on the Mental Health and Well-Being of UK Healthcare Workers. BJPsych Open 2021, 7, e88. [Google Scholar] [CrossRef] [PubMed]
- Escudero-Castillo, I.; Mato-Díaz, F.J.; Rodriguez-Alvarez, A. Furloughs, Teleworking and Other Work Situations during the COVID-19 Lockdown: Impact on Mental Well-Being. Int. J. Environ. Res. Public Health 2021, 18, 2898. [Google Scholar] [CrossRef] [PubMed]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological Effects of the COVID-2019 Pandemic: Perceived Stress and Coping Strategies among Healthcare Professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef] [PubMed]
- Bulińska-Stangrecka, H.; Bagieńska, A. The Role of Employee Relations in Shaping Job Satisfaction as an Element Promoting Positive Mental Health at Work in the Era of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 1903. [Google Scholar] [CrossRef]
- Afulani, P.A.; Gyamerah, A.O.; Nutor, J.J.; Laar, A.; Aborigo, R.A.; Malechi, H.; Sterling, M.; Awoonor-Williams, J.K. Inadequate Preparedness for Response to COVID-19 Is Associated with Stress and Burnout among Healthcare Workers in Ghana. PLoS ONE 2021, 16, e0250294. [Google Scholar] [CrossRef] [PubMed]
- Charoensukmongkol, P.; Phungsoonthorn, T. The Effectiveness of Supervisor Support in Lessening Perceived Uncertainties and Emotional Exhaustion of University Employees during the COVID-19 Crisis: The Constraining Role of Organizational Intransigence. J. Gen. Psychol. 2020, 148, 431–450. [Google Scholar] [CrossRef]
- Cipolotti, L.; Chan, E.; Murphy, P.; van Harskamp, N.; Foley, J.A. Factors Contributing to the Distress, Concerns, and Needs of UK Neuroscience Health Care Workers during the COVID-19 Pandemic. Psychol. Psychother. 2021, 94 (Suppl. 2), 536–543. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, Anxiety, Stress Levels of Physicians and Associated Factors in COVID-19 Pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Galán, J.; Lázaro-Pérez, C.; Martínez-López, J.Á.; Fernández-Martínez, M.D.M. Burnout in Spanish Security Forces during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8790. [Google Scholar] [CrossRef] [PubMed]
- Hines, S.E.; Chin, K.H.; Glick, D.R.; Wickwire, E.M. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 488. [Google Scholar] [CrossRef] [PubMed]
- Kannampallil, T.G.; Goss, C.W.; Evanoff, B.A.; Strickland, J.R.; McAlister, R.P.; Duncan, J. Exposure to COVID-19 Patients Increases Physician Trainee Stress and Burnout. PLoS ONE 2020, 15, e0237301. [Google Scholar] [CrossRef]
- Labrague, L.J.; De Los Santos, J.A.A. COVID-19 Anxiety among Front-Line Nurses: Predictive Role of Organisational Support, Personal Resilience and Social Support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Ricciardi, W.; Antonelli, M. Occupational Stress and Mental Health among Anesthetists during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8245. [Google Scholar] [CrossRef] [PubMed]
- Manzano García, G.; Ayala Calvo, J.C. The Threat of COVID-19 and Its Influence on Nursing Staff Burnout. J. Adv. Nurs. 2021, 77, 832–844. [Google Scholar] [CrossRef]
- Marco, C.A.; Larkin, G.L.; Feeser, V.R.; Monti, J.E.; Vearrier, L. For the ACEP Ethics Committee. Post-Traumatic Stress and Stress Disorders during the COVID-19 Pandemic: Survey of Emergency Physicians. JACEP Open 2020, 1, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Mattila, E.; Peltokoski, J.; Neva, M.H.; Kaunonen, M.; Helminen, M.; Parkkila, A.-K. COVID-19: Anxiety among Hospital Staff and Associated Factors. Ann. Med. 2021, 53, 237–246. [Google Scholar] [CrossRef]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef] [PubMed]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M.; et al. Factors Contributing to Healthcare Professional Burnout during the COVID-19 Pandemic: A Rapid Turnaround Global Survey. PLoS ONE 2020, 15, e0238217. [Google Scholar] [CrossRef] [PubMed]
- Portoghese, I.; Meloni, F.; Galletta, M.; Piras, I.; D’Aloja, E.; Finco, G.; Campagna, M. Concerns, Perceived Impact, Preparedness in Coronavirus Disease (COVID-19) Pandemic and Health Outcomes among Italian Physicians: A Cross-Sectional Study. J. Prim. Care Community Health 2021, 12, 21501327211000244. [Google Scholar] [CrossRef]
- Soto-Rubio, A.; Giménez-Espert, M.D.C.; Prado-Gascó, V. Effect of Emotional Intelligence and Psychosocial Risks on Burnout, Job Satisfaction, and Nurses’ Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7998. [Google Scholar] [CrossRef]
- Tušl, M.; Brauchli, R.; Kerksieck, P.; Bauer, G.F. Impact of the COVID-19 Crisis on Work and Private Life, Mental Well-Being and Self-Rated Health in German and Swiss Employees: A Cross-Sectional Online Survey. BMC Public Health 2021, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Y.; An, Y.; Zhao, Y.-J.; Zhang, L.; Cheung, T.; Hall, B.J.; Ungvari, G.S.; An, F.-R.; Xiang, Y.-T. Workplace Violence Against Chinese Frontline Clinicians During the COVID-19 Pandemic and Its Associations with Demographic and Clinical Characteristics and Quality of Life: A Structural Equation Modeling Investigation. Front. Psychiatry 2021, 12, 649989. [Google Scholar] [CrossRef] [PubMed]
- Zandi, G.; Shahzad, I.; Farrukh, M.; Kot, S. Supporting Role of Society and Firms to COVID-19 Management among Medical Practitioners. Int. J. Environ. Res. Public Health 2020, 17, 7961. [Google Scholar] [CrossRef]
- Zerbini, G.; Ebigbo, A.; Reicherts, P.; Kunz, M.; Messman, H. Psychosocial Burden of Healthcare Professionals in Times of COVID-19—A Survey Conducted at the University Hospital Augsburg. Ger. Med. Sci. 2020, 18, Doc05. [Google Scholar] [CrossRef]
- Lee, H. Changes in Workplace Practices during the COVID-19 Pandemic: The Roles of Emotion, Psychological Safety and Organisation Support. J. Organ. Eff. People Perform. 2021, 8, 97–128. [Google Scholar] [CrossRef]
- Al-Ghunaim, T.A.; Johnson, J.; Biyani, C.S.; O’Connor, D. Psychological and Occupational Impact of the COVID-19 Pandemic on UK Surgeons: A Qualitative Investigation. BMJ Open 2021, 11, e045699. [Google Scholar] [CrossRef] [PubMed]
- Al-Mansour, K.; Alfuzan, A.; Alsarheed, D.; Alenezi, M.; Abogazalah, F. Work-Related Challenges among Primary Health Centers Workers during COVID-19 in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 1898. [Google Scholar] [CrossRef]
- Digby, R.; Winton-Brown, T.; Finlayson, F.; Dobson, H.; Bucknall, T. Hospital Staff Well-Being during the First Wave of COVID-19: Staff Perspectives. Int. J. Ment. Health Nurs. 2021, 30, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Dreher, A.; Pietrowsky, R.; Loerbroks, A. Pandemic-Related Attitudes, Stressors and Work Outcomes among Medical Assistants during the SARS-CoV-2 (“Coronavirus”) Pandemic in Germany: A Cross-Sectional Study. PLoS ONE 2021, 16, e0245473. [Google Scholar] [CrossRef]
- Elshami, W.; Akudjedu, T.N.; Abuzaid, M.; David, L.R.; Tekin, H.O.; Cavli, B.; Issa, B. The Radiology Workforce’s Response to the COVID-19 Pandemic in the Middle East, North Africa and India. Radiography 2021, 27, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lu, L.; Chen, T.; Ye, S.; Kelifa, M.O.; Cao, N.; Zhang, Q.; Liang, T.; Wang, W. Healthcare Worker’s Mental Health and Their Associated Predictors during the Epidemic Peak of COVID-19. Psychol. Res. Behav. Manag. 2021, 14, 221–231. [Google Scholar] [CrossRef]
- Feeley, T.; Ffrench-O’Carroll, R.; Tan, M.H.; Magner, C.; L’Estrange, K.; O’Rathallaigh, E.; Whelan, S.; Lyons, B.; O’Connor, E. A Model for Occupational Stress amongst Paediatric and Adult Critical Care Staff during COVID-19 Pandemic. Int. Arch. Occup. Environ. Health 2021, 94, 1721–1737. [Google Scholar] [CrossRef] [PubMed]
- Gül, Ş.; Kılıç, S.T. Determining Anxiety Levels and Related Factors in Operating Room Nurses during the COVID-19 Pandemic: A Descriptive Study. J. Nurs. Manag. 2021, 29, 1934–1945. [Google Scholar] [CrossRef]
- Havaei, F.; Ma, A.; Staempfli, S.; MacPhee, M. Nurses’ Workplace Conditions Impacting Their Mental Health during COVID-19: A Cross-Sectional Survey Study. Healthcare 2021, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Halley, M.C.; Mathews, K.S.; Diamond, L.C.; Linos, E.; Sarkar, U.; Mangurian, C.; Sabry, H.; Goyal, M.K.; Olazo, K.; Miller, E.G.; et al. The Intersection of Work and Home Challenges Faced by Physician Mothers during the Coronavirus Disease 2019 Pandemic: A Mixed-Methods Analysis. J. Women’s Health 2021, 30, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; He, W.; Zhou, K. The Mind, the Heart, and the Leader in Times of Crisis: How and When COVID-19-Triggered Mortality Salience Relates to State Anxiety, Job Engagement, and Prosocial Behavior. J. Appl. Psychol. 2020, 105, 1218–1233. [Google Scholar] [CrossRef]
- Ingusci, E.; Signore, F.; Giancaspro, M.L.; Manuti, A.; Molino, M.; Russo, V.; Zito, M.; Cortese, C.G. Workload, Techno Overload, and Behavioral Stress during COVID-19 Emergency: The Role of Job Crafting in Remote Workers. Front. Psychol. 2021, 12, 655148. [Google Scholar] [CrossRef] [PubMed]
- Mekonen, E.; Shetie, B.; Muluneh, N. The Psychological Impact of COVID-19 Outbreak on Nurses Working in the Northwest of Amhara Regional State Referral Hospitals, Northwest Ethiopia. Psychol. Res. Behav. Manag. 2020, 13, 1353–1364. [Google Scholar] [CrossRef]
- Al-Jumaili, A.A.; Al-Fatlawi, B.G.; Al-Jalehawi, A.K.; Al-Hamadani, F.Y.; Alsawad, O.S. Impact of COVID-19 Pandemic on Healthcare Providers: Save the Frontline Fighters. Int. J. Pharm. Pract. 2021, 29, riab018. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Pang, H.; Liao, C.; Wang, N.; Tao, P.; Huang, H. Anxiety of Nurses to Support Wuhan in Fighting against COVID-19 Epidemic and Its Correlation with Work Stress and Self-Efficacy. J. Clin. Nurs. 2021, 30, 397–405. [Google Scholar] [CrossRef]
- Nguyen, P.T.L.; Nguyen, T.B.L.; Pham, A.G.; Duong, K.N.C.; Gloria, M.A.J.; Vo, T.V.; Vo, B.V.; Phung, T.L. Psychological Stress Risk Factors, Concerns and Mental Health Support Among Health Care Workers in Vietnam during the Coronavirus Disease 2019 (COVID-19) Outbreak. Front. Public Health 2021, 9, 628341. [Google Scholar] [CrossRef]
- Norful, A.A.; Rosenfeld, A.; Schroeder, K.; Travers, J.L.; Aliyu, S. Primary Drivers and Psychological Manifestations of Stress in Frontline Healthcare Workforce during the Initial COVID-19 Outbreak in the United States. Gen. Hosp. Psychiatry 2021, 69, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, A.M.; Rubio-Valdehita, S.; Díaz-Ramiro, E.M. Influence of the COVID-19 Pandemic on Mental Workload and Burnout of Fashion Retailing Workers in Spain. Int. J. Environ. Res. Public Health 2021, 18, 983. [Google Scholar] [CrossRef] [PubMed]
- Tokac, U.; Razon, S. Nursing Professionals’ Mental Well-Being and Workplace Impairment during the COVID-19 Crisis: A Network Analysis. J. Nurs. Manag. 2021, 29, 1653–1659. [Google Scholar] [CrossRef] [PubMed]
- Coulombe, S.; Pacheco, T.; Cox, E.; Khalil, C.; Doucerain, M.M.; Auger, E.; Meunier, S. Risk and Resilience Factors during the COVID-19 Pandemic: A Snapshot of the Experiences of Canadian Workers Early on in the Crisis. Front. Psychol. 2020, 11, 580702. [Google Scholar] [CrossRef]
- Moreno-Jiménez, J.E.; Blanco-Donoso, L.M.; Demerouti, E.; Belda Hofheinz, S.; Chico-Fernández, M.; Moreno-Jiménez, B.; Garrosa, E. The Role of Healthcare Professionals’ Passion in Predicting Secondary Traumatic Stress and Posttraumatic Growth in the Face of COVID-19: A Longitudinal Approach. Int. J. Environ. Res. Public Health 2021, 18, 4453. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, K.; Zhang, G.; Feng, R.; Chen, J.; Xu, D.; Liu, X.; Ngoubene-Atioky, A.J.; Huang, H.; Liu, Y.; et al. Occupational Stress and Mental Health: A Comparison Between Frontline Medical Staff and Non-Frontline Medical Staff during the 2019 Novel Coronavirus Disease Outbreak. Front. Psychiatry 2020, 11, 555703. [Google Scholar] [CrossRef]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A Systematic Review Including Meta-Analysis of Work Environment and Burnout Symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heath, C.; Sommerfield, A.; von Ungern-Sternberg, B.S. Resilience Strategies to Manage Psychological Distress among Healthcare Workers during the COVID-19 Pandemic: A Narrative Review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Lecca, L.I.; Finstad, G.L.; Traversini, V.; Lulli, L.G.; Gualco, B.; Taddei, G. The Role of Job Support as a Target for the Management of Work-Related Stress: The State of Art. Qual.-Access Success 2020, 21, 152–158. Available online: https://0-www-proquest-com.brum.beds.ac.uk/openview/f7f3198c1fdfd682d43d73503460efc3/1?pq-origsite=gscholar&cbl=1046413 (accessed on 11 September 2021).
- Mead, S.; Hilton, D.; Curtis, L. Peer Support: A Theoretical Perspective. Psychiatr. Rehabil. J. 2001, 25, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Hancock, F.; Page, F. Family to Work Conflict and the Usefulness of Workplace Support. Occup. Med. 2013, 63, 373–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, B.; Brooks, S.K.; Greenberg, N. The Role of Peer Support in Managing Occupational Stress: A Qualitative Study of the Sustaining Resilience at Work Intervention. Workplace Health Saf. 2020, 68, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Finstad, G.L.; Giorgi, G.; Lulli, L.G.; Pandolfi, C.; Foti, G.; León-Perez, J.M.; Cantero-Sánchez, F.J.; Mucci, N. Resilience, Coping Strategies and Posttraumatic Growth in the Workplace Following COVID-19: A Narrative Review on the Positive Aspects of Trauma. Int. J. Environ. Res. Public Health 2021, 18, 9453. [Google Scholar] [CrossRef]
- Banerjee, D.; Sathyanarayana Rao, T.S.; Kallivayalil, R.A.; Javed, A. Psychosocial Framework of Resilience: Navigating Needs and Adversities During the Pandemic, A Qualitative Exploration in the Indian Frontline Physicians. Front. Psychol. 2021, 12, 622132. [Google Scholar] [CrossRef]
- Windle, G. What Is Resilience? A Review and Concept Analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- Eisenberger, R.; Huntington, R.; Hutchison, S.; Sowa, D. Perceived Organizational Support. J. Appl. Psychol. 1986, 71, 500–507. Available online: https://doi.apa.org/doiLanding?doi=10.1037%2F0021-9010.71.3.500 (accessed on 4 September 2021). [CrossRef]
- Bowling, N.A.; Alarcon, G.M.; Bragg, C.B.; Hartman, M.J. A Meta-Analytic Examination of the Potential Correlates and Consequences of Workload. Work Stress 2015, 29, 95–113. [Google Scholar] [CrossRef]
- Sommerville, K.L. Hospitality Employee Management and Supervision: Concepts and Practical Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2007; ISBN 978-0-470-07427-5. [Google Scholar]
- Saedpanah, D.; Salehi, S.; Moghaddam, L.F. The Effect of Emotion Regulation Training on Occupational Stress of Critical Care Nurses. J. Clin. Diagn. Res. 2016, 10, VC01–VC04. [Google Scholar] [CrossRef] [PubMed]
- Eilström, P.-E.; Kock, H. Competence Development in the Workplace: Concepts, Strategies and Effects. Asia Pac. Educ. Rev. 2008, 9, 5–20. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job Demands–Resources Theory: Taking Stock and Looking Forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Lee, D.-J.; Sirgy, M.J. What Do People Do to Achieve Work-Life Balance? A Formative Conceptualization to Help Develop a Metric for Large-Scale Quality-of-Life Surveys. Soc. Indic. Res. 2018, 138, 771–791. [Google Scholar] [CrossRef]
- Fuß, I.; Nübling, M.; Hasselhorn, H.M.; Schwappach, D.; Rieger, M.A. Working Conditions and Work-Family Conflict in German Hospital Physicians: Psychosocial and Organisational Predictors and Consequences. BMC Public Health 2008, 8, 353. Available online: https://0-bmcpublichealth-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/1471-2458-8-353 (accessed on 6 September 2021). [CrossRef] [PubMed] [Green Version]
- Langballe, E.M.; Innstrand, S.T.; Aasland, O.G.; Falkum, E. The Predictive Value of Individual Factors, Work-Related Factors, and Work-Home Interaction on Burnout in Female and Male Physicians: A Longitudinal Study. Stress Health 2011, 27, 73–87. [Google Scholar] [CrossRef]
- Sorrentino, E.; Vona, R.; Monterosso, D.; Giammarioli, A.M. Gender Issues on Occupational Safety and Health. Ann. Ist. Super. Sanità 2016, 52, 190–197. [Google Scholar] [CrossRef]
- La Torre, G.; De Leonardis, V.; Chiappetta, M. Technostress: How Does It Affect the Productivity and Life of an Individual? Results of an Observational Study. Public Health 2020, 189, 60–65. Available online: https://0-reader-elsevier-com.brum.beds.ac.uk/reader/sd/pii/S0033350620304200?token=FD099DCCC7326E6FD013476B82EAA4877C33816CB9D99182CC98E4849003A9BFA3F3E67993841D3B2184E8D43EB2C330&originRegion=eu-west-1&originCreation=20210904130142 (accessed on 4 September 2021). [CrossRef] [PubMed]
- Ragu-Nathan, T.S.; Tarafdar, M.; Ragu-Nathan, B.S.; Tu, Q. The Consequences of Technostress for End Users in Organizations: Conceptual Development and Empirical Validation. Inf. Syst. Res. 2008, 19, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Day, A.; Paquet, S.; Scott, N.; Hambley, L. Perceived Information and Communication Technology (ICT) Demands on Employee Outcomes: The Moderating Effect of Organizational ICT Support. J. Occup. Health Psychol. 2012, 17, 473–491. [Google Scholar] [CrossRef] [PubMed]
- Basyouni, S.S.; El Keshky, M.E.S. Job Insecurity, Work-Related Flow, and Financial Anxiety in the Midst of COVID-19 Pandemic and Economic Downturn. Front. Psychol. 2021, 12, 2681. [Google Scholar] [CrossRef] [PubMed]

| Major Findings | Implications | |
|---|---|---|
| Support from peers and organizations | -Most recurrent topic related to workers mental wellbeing in pandemics; -it protects mental health; -it prevents depression, anxiety and burnout among workers; -it has a human and organizational dimension | -Peer support, communication and team building training programs are needed, especially in healthcare settings; -organizational changes can mitigate the impact of the emergency on workers; -clear and effective communication between colleagues and supervisors is a key factor in preventing poor mental outcomes. |
| Home–work interface and balance | -This is affected by long working schedules in HCWs and by the fear of bringing contagion home -It implies difficulty in maintaining work time and home time as separate for remote workers | -Educating employees and supervisors in making clear distinction between free time and work time -Government and organizational measures to support family care can support workers and protect their mental health |
| Changes in workload | -In HCWs, augmented workloads causes anxiety, depression and burnout symptoms; -reduced workloads is associated with loss of economic status and subsequent poor mental outcomes; -for remote workers, it can be configured as technostress and threatens home–work balance. | -Providing adequate resting time is crucial not only for workers’ health but also for patients’ safety; -balancing job demands and requests with the physical and psychological resources of workers is mandatory in every working environment |
| Work competence and adequate training | -This is a major source of stress for HCWs; -the fear of making mistakes is enhanced by the lack of general protocols to treat COVID; -the feeling of being pushed beyond training contributes to the development of burnout symptoms especially in young HCWs. | -Healthcare organizations must provide adequate training programs, especially when a worker is redeployed from one department to another; -supervisors should understand when workers are pushed beyond training -protocols for the management of COVID patients and scientific data sharing are a relevant resource. |
| Job insecurity and financial stress | -The economic crisis linked to the sanitary emergency meant several categories of workers were uncertain of the future; -the job insecurity and the consequent financial stress causes burnout, anxiety and depression symptoms; -this also involved HCWs with a reduction in patient volume. | -Government measures aimed at sustaining certain working categories can have an important impact on mental status of workers; -when possible, companies should provide job stabilization and economic support to workers |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lulli, L.G.; Giorgi, G.; Pandolfi, C.; Foti, G.; Finstad, G.L.; Arcangeli, G.; Mucci, N. Identifying Psychosocial Risks and Protective Measures for Workers’ Mental Wellbeing at the Time of COVID-19: A Narrative Review. Sustainability 2021, 13, 13869. https://0-doi-org.brum.beds.ac.uk/10.3390/su132413869
Lulli LG, Giorgi G, Pandolfi C, Foti G, Finstad GL, Arcangeli G, Mucci N. Identifying Psychosocial Risks and Protective Measures for Workers’ Mental Wellbeing at the Time of COVID-19: A Narrative Review. Sustainability. 2021; 13(24):13869. https://0-doi-org.brum.beds.ac.uk/10.3390/su132413869
Chicago/Turabian StyleLulli, Lucrezia Ginevra, Gabriele Giorgi, Caterina Pandolfi, Giulia Foti, Georgia Libera Finstad, Giulio Arcangeli, and Nicola Mucci. 2021. "Identifying Psychosocial Risks and Protective Measures for Workers’ Mental Wellbeing at the Time of COVID-19: A Narrative Review" Sustainability 13, no. 24: 13869. https://0-doi-org.brum.beds.ac.uk/10.3390/su132413869